

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Microblood perfusion of isolated single umbilical artery (ISUA) foetus placenta was evaluated using three-dimensional power Doppler ultrasound (3D-PDU). Vascular endothelial growth factor (VEGF) protein expression in the placenta was also semi-quantitative and qualitatively analysed. Differences between ISUA and control groups were compared. 3D-PDU was used to detect placental blood flow parameters, including vascularity index (VI), flow index, and vascularity flow index (VFI), in 58 foetuses in the ISUA group and 77 normal foetuses in the control group. Immunohistochemistry and polymerase chain reaction were employed to analyse the VEGF expression in placental tissues of 26 foetuses in the ISUA group and 26 foetuses in the control group. The control group exhibited higher VI and VFI than the ISUA group (p < 0.05). Meanwhile, the ISUA group showed a higher positivity rate of VEGF protein expression than the control group (χ2=28.013, p˂0.001). The ISUA group also presented a higher VEGF mRNA protein expression than the control group (p˂0.001). 3D-PDU can be used to quantitatively analyse microblood perfusion of the placenta and provide an objective assessment of ISUA foetuses.
What is already known on this subject? Colour Doppler flow can be used to evaluate placental and maternal circulation and remains an ideal method for evaluating high-risk placental function. Three-dimensional power Doppler ultrasound (3D-PDU) can be used to quantify blood vessels and blood flow in placental parenchyma via the measurement of the amplitude of blood vessels and blood flow in normal foetuses, respectively.
What do the results of this study add? 3D-PDU can be used to quantitatively analyse micro blood perfusion of the placenta and conduct an objective assessment of isolated single umbilical artery foetuses. The isolated single umbilical artery foetuses exhibited a higher positivity rate of vascular endothelial growth factor (VEGF) protein expression and higher VEGF mRNA protein expression than the normal foetuses.
What are the implication of these findings for clinical practice and/or further research? The study provides a reliable basis for maternal-foetal monitoring during pregnancy in the isolated single umbilical artery foetuses. Objective assessment of the occurrence and development of foetuses with isolated single umbilical artery was performed.
Impact statement
Background
Single umbilical artery (SUA) is one of the most common prenatally diagnosed foetal abnormalities and is a soft indicator of congenital structural deformity, chromosome abnormality, premature birth and low birth weight (Bugatto et al. Citation2010; Dagklis et al. Citation2010; Araujo et al. Citation2015; Wang et al. Citation2019). SUA can be divided into two categories, namely, non-isolated and isolated SUA (ISUA), based on the presence of other structural deformities or chromosome abnormalities. Approximately 65% of SUA cases present isolated findings (Chetty-John et al. Citation2010; Li et al. Citation2019). Most ISUA cases are not associated with the presence of other malformations and chromosomal alterations. ISUA cases often give rise to the development of certain obstetric complications, such as foetal growth restriction and increased perinatal mortality (Horton et al. Citation2010; Murphy-Kaulbeck et al. Citation2010; Shen et al. Citation2016).
The placenta connects a pregnant woman and her foetus; given that SUA foetuses lack an umbilical artery, haemodynamic changes in placental parenchyma may further affect foetal growth and development. The quantitative study of blood flow parameters of ISUA foetal placenta using three-dimensional power Doppler ultrasound (3D-PDU) can provide an objective basis for the prompt identification of changes in the placental parenchyma of ISUA foetus. Vascular endothelial growth factor (VEGF) is an important regulatory factor of angiogenesis and effectively promotes the proliferation of vascular endothelial cells in tissues or organs. Hypoxia can stimulate VEGF to increase its positive expression rate (Anteby et al. Citation2004; Keshavarzi et al. Citation2017; Ali et al. Citation2019). In this study, VEGF expression in placental tissues of the ISUA and control groups was measured by immunohistochemistry and polymerase chain reaction (PCR) to analyse the blood supply of the placental cycle during the growth and development of ISUA foetuses.
Methods
Study subjects
This study included 58 pregnant women in the third trimester and diagnosed by prenatal ultrasound in our hospital between December 2018 and April 2020 as the ISUA group. Meanwhile, the control group comprised 77 randomly selected pregnant women in their third trimester during the same period (except for those showing foetal structural malformation and chromosomal abnormality). No significant difference in age was found between the two groups. The hospital ethics committee approved the study protocol, and the pregnant mothers provided their written informed consent. Basic clinical data, including age, weight, height, body mass index and parity, were collected from the 58 and 77 pregnant women in the ISUA and control groups, respectively. Gestational age was calculated based on the last menstruation or by ultrasonic measurement of crown-rump length in the early pregnancy of women with irregular menstrual cycles. In all cases, ISUA diagnosis was confirmed by postnatal pathological examination, and all newborns were determined to be anatomically normal at delivery. The small-for-gestational-age (SGA) newborns were diagnosed as those with a birth weight below the 10th percentile for gestational age. The exclusion criteria were as follows: (1) placenta located in posterior and lateral walls, (2) abnormal placental morphology, (3) polyhydramnios or oligohydramnios, (4) foetuses with other structural abnormalities, (5) multiple pregnancies; (6) pregnancy complications.
Instruments and methods
For 3D-PDU, the blood flow of the placenta was measured using an E10 (GE Healthcare, USA) ultrasound system with an abdominal volume probe. The Doppler energy was set to <100 mW/cm2. Foetal biometric measurements were performed on each scan. The instrument parameters were adjusted, and the insertion point from the placenta to the umbilical cord was detected to fill the blood flow in the placental parenchyma. With the use of the energy Doppler, the umbilical cord inserted into the placental parenchyma was considered the region of interest, and complete microvessels were scanned from the basal surface of the placenta to the foetal surface. The pregnant women were instructed to hold their breath or breathe calmly, and the 3D-PDU mode was selected when their foetus was in a quiet state. With the incident angle set at 60° and the umbilical cord inserted into the placenta as the initial scanning section, 3D scanning was quickly completed, and volume data were stored. Computer-aided analysis software was used to measure the volume of the region of interest and the following 3D-PDU blood flow parameters: vascularity index (VI), which represents the number of blood vessels in the region of interest and is expressed as a percentage; flow index (FI), which denotes blood flow intensity in tissues; vascularity flow index (VFI), which is also called tissue perfusion and represents the sum of blood flow intensity and blood vessel number.
In this study, 26 cases of ISUA and 26 cases of normal foetal placental tissues were selected. Placental tissues were collected from the foetal placenta surface area, which was approximately 1 cm away from the central umbilical cord insertion point of the placenta. The sample with 1.5 × 1.5 × 1.5 cm3 size was fixed in the prepared conventional formaldehyde, dehydrated for 24 h, embedded with conventional paraffin and sectioned. The immunohistochemical VEGF kit and VEGF monoclonal antibody (Fuzhou Maixin Biotechnology Co., Ltd.) were used for analysis. Routine dewaxing was conducted on tissue slices. The samples were subjected to antigen repair at high temperature in a microwave oven, added with H2O2 to block endogenous peroxidase activity, dropwise added with the primary antibody and allowed to stand overnight at 4 °C. Secondary antibodies were added in accordance with the detailed operation procedure and dosage of the kits. Counterstaining with haematoxylin was performed after DAB development. The samples were dehydrated with different concentrations of ethanol and sealed with xylene. The primary antibody was replaced with a phosphate-buffered saline solution as the negative control. Five representative high-power visual fields were selected from each slice to observe the VEGF protein expression in the placenta and umbilical cord of the two groups.
In this study, 26 ISUA cases and 26 cases of normal foetal placenta were selected, and 0.5 × 0.5 × 0.5 cm3 placental tissues were obtained from the foetal surface of the placenta area, which was 1 cm away from the central umbilical cord insertion point of the placenta. Fresh umbilical cord tissues were also collected at 0.5 cm away from the placenta, repeatedly washed with normal saline and preserved at −80 °C for later use after being fixed in RNAlaterTM (protein fixative solution). mRNA extraction was carried out as follows: (1) extraction of total RNA from the umbilical cord and placenta, (2) RNA reverse transcription and (3) real-time PCR (the primers used in real-time experimental PCR were synthesised using Huada gene).
Statistical analysis
Data analysis was performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, N.Y., USA). Continuous variables were presented as mean ± standard deviation or median (interquartile range) as appropriate. The positivity rate was expressed in percentage (n%). The χ2 test was used for the comparison of VEGF positivity rates between the two groups, and the T-test of two independent samples was used for the comparison of VEGF mRNA expressions. p < 0.05 indicated a statistical difference.
Results
A 3D vascular tree structure was observed in the 3D-PDU blood flow images at the insertion point of the umbilical cord and placenta for both groups (). The comparison of 3D-PDU blood flow parameters revealed significantly higher VI and VFI in the control group compared with those in the ISUA group (p < 0.05) ( and ). No significant difference was observed in the FI and volume of the region of interest between the two groups (p > 0.05) (). Meanwhile, 58 foetuses in the ISUA group and 77 foetuses in the control group were followed up until birth, and the general condition of newborns in both was analysed. The results showed 10 and 3 cases of SGA in the ISUA and normal control groups, respectively. Compared with that in the normal control group, the incidence of SGA in the ISUA group was higher (13.0 vs. 3.9%; p < 0.01). Neonatal and placental weights also significantly differed between the two groups (p < 0.05) (). However, no significant difference was observed in the maternal age, maternal weight, body mass index and gestational age at delivery between the two groups (p > 0.05) ().
Figure 1. 3D-PDU image of the foetal placenta in the isolated single umbilical artery (ISUA) group and control group; (a, b) 3D-PDU blood flow images at the insertion point of umbilical cord and placenta in the ISUA group showing a 3D vascular tree structure.

Figure 2. Measurement of 3D-PDU blood flow parameters vascularity index (VI), flow index (FI) and vascularity flow index (VFI) at the umbilical cord insertion point of the foetal placenta in the isolated single umbilical artery (ISUA) group and control group.
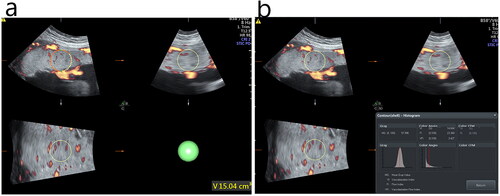
Table 1. Comparison of the 3D-PDU blood flow parameters of foetal placenta between the ISUA and control groups (±SD).
Table 2. Clinical data of pregnant women and newborns in the ISUA and control groups (±SD).
Immunohistochemistry slices of the placenta from both groups were individually observed. Five typical fields were selected for each slice, with 130 visual fields observed in each group. The ISUA group exhibited a significantly higher positivity rate of VEGF expression than the control group (p < 0.05) ( and ).
Figure 3. VEGF expression in placenta by immunohistochemistry (x 400); a: Control group (-); b: ISUA group (+++).
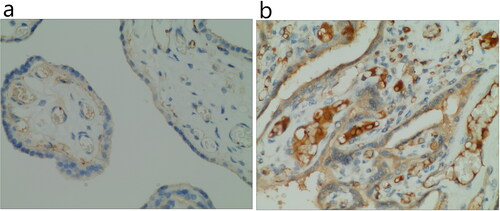
Table 3. Immunohistochemical expression intensity of VEGF in the foetal placenta of the ISUA and control groups.
PCR was used to detect the mRNA protein expression of VEGF in the placental tissues of the two groups. The ISUA group showed a higher VEGF mRNA protein expression in placental tissues compared with the control group (0.38 ± 0.27 vs. 0.94 ± 0.44, p˂0.001).
Discussion
Colour Doppler flow can be used to evaluate placental and maternal circulation and is an ideal method for evaluating high-risk placental function (Moran and McAuliffe Citation2011). However, this method can only indirectly assess placental function and cannot objectively reflect the placental parenchymal blood supply because of many factors affecting the blood vessel spectrum. In addition, the observation of placental parenchymal blood flow by colour Doppler by visually counting placental blood vessels is greatly influenced by subjective factors and lacks accurate and objective quantitative detection indicators. Therefore, describing foetal placental blood perfusion in different degrees is difficult. In our study, 3D-PDU and transabdominal volume probes can be used to significantly improve the definition of 2D imaging of the placenta and the sensitivity of internal blood flow to evaluate placental morphology and observe the distribution of vascular beds in placental parenchyma (Noguchi et al. Citation2009; Rizzo et al. Citation2009). 3D-PDU can also be applied to quantify blood vessels and blood flow in placental parenchyma by measuring the amplitude of blood vessels and blood flow in ISUA and normal foetuses and quantitatively measuring blood vessel volume in the placental parenchyma of ISUA foetuses to calculate the density of blood vessels per unit placental volume. Our study revealed the high VI and VFI of the foetal placenta in the ISUA group, which indicated placental insufficiency and low blood flow signal in placental parenchyma. This finding also explained why ISUA foetuses merge with SGA infants easily, which is a phenomenon related to the small amount of blood in the placental parenchyma. In this study, newborns in the ISUA group had lower weight and placental quality than those in the control group. Meanwhile, the ISUA group manifested a higher incidence of SGA than the control group. This result indicated that at birth, the ISUA foetus may be lighter than a normal foetus due to the lack of an umbilical artery in the former. SUA may result in a series of changes in the foetal circulatory system, thus changing the vascular resistance of the umbilical artery and the blood supply of the placenta.
VEGF is an important angiogenic factor, and it can promote the proliferation of endothelium in tissues and organs and the formation and remodelling of new blood vessels in the placenta and umbilical cord during pregnancy. This condition further enhances tissue vascular permeability, which causes the exudation of plasma proteins and the formation of clotting substances, which eventually lead to a decline in placental function. The placenta is an important structure connecting a pregnant woman and her foetus. Abnormal VEGF expression in the placenta often manifests as a disorder of placental circulation and oxygen exchange in placental parenchyma, and it consequently affects intrauterine growth and foetal development (Rajakumar and Conrad Citation2000). In our study, the ISUA foetal placental tissues showed a significantly higher positivity rate of VEGF expression than the control group due to the disorder of placental circulation, decreased blood and oxygen supply in placental parenchyma and hypoxic environment that promoted the compensatory increase in VEGF expression. In addition, the possible hypoperfusion and hypoxia in the placental circulation of the ISUA foetus were reported, and these findings are consistent with the blood perfusion results of 3D-PDU for the placental tissues of the ISUA foetus. The ISUA group presented higher VI and VFI than the control group, which suggests possible hypoperfusion in the placenta of ISUA foetuses. Placental hypoperfusion can stimulate placental tissues to counteractively increase VEGF expression, which is beneficial to the formation of new blood vessels in the placenta. A high VEGF expression can further reduce placental circulation resistance, which can further improve placental circulation and microvascular blood oxygen perfusion.
The ISUA group showed a higher VEGF mRNA expression than the control group. Thus, VEGF can be up-regulated in vascular endothelial cells through a certain mechanism that promotes the formation of new blood vessels in placental tissues and further improves the hypoxic state of the placenta. However, no clear conclusion was obtained regarding the mechanism of VEGF stimulation in a hypoxic environment and the mechanism that mediates the function of VEGF and its downstream genes. Therefore, further studies are warranted. In this study, the expression of VEGF protein in the placentas of the two groups was detected by immunohistochemistry, which can only be used for semi-quantitative diagnosis, and mRNA quantitative method, which can be utilised for quantitative evaluation of VEGF and is thus more accurate and reliable than immunohistochemistry.
However, the present study also encountered some limitations. Firstly, with the increase in gestational age, a complete image of the placenta in the third trimester cannot be obtained because the placenta is located in the posterior wall. Therefore, the posterior placenta in the third trimester was excluded from this study to ensure the reliability of measurement data. Secondly, although placental microperfusion in ISUA foetuses can be quantitatively evaluated by 3D-CPU, given the small sample size used in this study (58 ISUA foetuses), larger prospective research should be conducted in the future. The small sample size used in semi-quantitative and mRNA quantitative analyses of placental tissue by immunohistochemical and PCR must be further enlarged in future works, and 3D-PDU imaging of foetal placenta of ISUA in the second trimester must be performed. Finally, the breathing movement of a pregnant woman and foetal movement can cause motion artefacts, such as distortion and deformation in the 3D images of the placental region of interest, leading to a large deviation in the results. Therefore, the pregnant women were instructed to hold their breath, and images were collected while the foetus was in a quiet state during 3D scanning. In this study, only the foetal placenta of ISUA in the third trimester was measured using 3D-PDU, and the foetal placenta in the second trimester was not studied. The expression of VEGF protein in the placental tissues in both groups was quantified by PCR but not Western blot, which reduced the accuracy of results.
Conclusions
The 3D-PDU of ISUA foetuses revealed lower blood flow parameters (VI and VFI) compared with those of normal foetuses, and this finding may be one of the reasons why ISUA foetuses are prone to be associated with SGA. 3D-PDU can be used to quantitatively analyse microblood perfusion of the placenta and provide an objective assessment of ISUA foetuses. VEGF protein expression in ISUA placentas can be detected by immunohistochemistry and PCR. The ISUA group exhibited a higher VEGF protein expression than the control group. This study provides an objective basis for clarifying the pathology of ISUA foetal placenta. With this technology, microblood flow perfusion of the foetal placenta of ISUA cases can be observed as early as possible. This work provides an objective basis for the clinical guarantee of maternal and infant safety.
Ethical approval
The study protocol was approved by the Medical Ethics Committee of Gansu Provincial Maternity and Child-care Hospital (Approval number 2017-14).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data and material in the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Ali, Z., et al., 2019. Altered expression of vascular endothelial growth factor, vascular endothelial growth factor receptor-1, vascular endothelial growth factor receptor-2, and Soluble Fms-like Tyrosine Kinase-1 in peripheral blood mononuclear cells from normal and preeclamptic pregnancies. Chinese Journal of Physiology, 62 (3), 117–122.
- Anteby, E.Y., et al., 2004. Vascular endothelial growth factor, epidermal growth factor and fibroblast growth factor-4 and -10 stimulate trophoblast plasminogen activator system and metalloproteinase-9. Molecular Human Reproduction, 10 (4), 229–235.
- Araujo, J.E., et al., 2015. Congenital heart disease and adverse perinatal outcome in fetuses with confirmed isolated single functioning umbilical artery. Journal of Obstetrics and Gynaecology, 35 (1), 85–87.
- Bugatto, F., et al., 2010. Ultrasound predictors of birth weight in euploid fetuses with isolated single umbilical artery. Ultrasound in Obstetrics and Gynecology, 36 (6), 724–727.
- Chetty-John, S., et al., 2010. Long-term physical and neurologic development in newborn infants with isolated single umbilical artery. American Journal of Obstetrics and Gynecology, 203 (4), 361–368.
- Dagklis, T., et al., 2010. Isolated single umbilical artery and fetal karyotype. Ultrasound in Obstetrics and Gynecology, 36 (3), 291–295.
- Horton, A. L., Barroilhet, L. and Wolfe, H. M., 2010. Perinatal outcomes in isolated single umbilical artery. American Journal of Perinatology, 27 (4), 321–324.
- Keshavarzi, F., et al., 2017. The placental vascular endothelial growth factor polymorphisms and preeclampsia/preeclampsia severity. Clinical and Experimental Hypertension, 39 (7), 606–611.
- Li, T.G., et al., 2019. Evaluation of right ventricular function in fetuses with isolated single umbilical artery using spatiotemporal image correlation M-mode. Cardiovascular Ultrasound, 17 (1), 14.
- Moran, M. and McAuliffe, F.M., 2011. Imaging and assessment of placental function. Journal of Clinical Ultrasound., 39 (7), 390–398.
- Murphy-Kaulbeck, L., et al., 2010. Single umbilical artery risk factors and pregnancy outcomes. Obstetrics and Gynecology, 116 (4), 843–850.
- Noguchi, J., et al., 2009. Placental vascular sonobiopsy using three-dimensional power Doppler ultrasound in normal and growth restricted fetuses. Placenta, 30 (5), 391–397.
- Rajakumar, A. and Conrad, K.P., 2000. Expression, ontogeny, and regulation of hypoxia-inducible transcription factors in the human placenta. Biological Reproduction, 63 (2), 559–569.
- Rizzo, G., et al., 2009. First-trimester placental volume and vascularization measured by 3-dimensional power Doppler sonography in pregnancies with low serum pregnancy-associated plasma protein a levels. Journal of Ultrasound in Medicine., 28 (12), 1615–1622.
- Shen, N., Zhang, W. and Li, G., 2016. Impact of isolated single umbilical artery on pregnancy outcome and delivery in full-term births. Journal of Obstetrics and Gynecology Research, 42 (4), 399–403.
- Wang, J., et al., 2019. Is echocardiography necessary for all single umbilical artery fetuses? A retrospective study in a selected Chinese population. Journal of Obstetrics and Gynaecology Research, 45 (4), 803–809.