

Abstract
The aim of this study was to elucidate the application of ultrasound examination of umbilical artery (UA) hemodynamics with urine microalbumin (UmA) determination in evaluating the outcomes of sPE patients. Altogether 80 sPE patients and 75 healthy pregnant women were recruited. UmA, RI (resistance index) and PI (pulsatility index) were separately measured by ELISA and the ultrasonic Doppler flow detector. The correlation between parameters was analysed using Pearson’s coefficient method. The independent risk factors of sPE were identified using the Logistic regression model. sPE patients had increased UmA, RI and PI (all p < 0.05). UmA level was positively correlated with RI and PI in sPE patients. RI, PI and UmA were independent risk factors of sPE (all p < 0.05). sPE can predict adverse pregnancy outcomes. High UmA levels may increase the risk of poor prognosis. Overall, ultrasound examination of UA hemodynamics with UmA determination can predict the adverse pregnancy outcomes of sPE patients.
What is already known on this subject? Doppler ultrasound and urine microalbumin (UmA) measurement are important tools in assessing the clinical severity of severe preeclampsia (sPE).
What do the results of this study add? This study aims to unravel the application of ultrasound examination of hemodynamics in the umbilical artery (UA) combined with the determination of UmA in evaluating the outcomes of sPE patients.
What are the implications of these findings for clinical practice and/or further research? Ultrasound examination of hemodynamics in UA combined with the determination of UmA can predict the adverse pregnancy outcomes of sPE patients.
IMPACT STATEMENT
Introduction
Preeclampsia (PE) refers to a pregnancy-specific syndrome affecting 3–5% of pregnancies, whose traditional diagnostic basis is elevated blood pressure and proteinuria (Ananth et al. Citation2013, Mol et al. Citation2016). In low and middle-income countries, PE is a chief contributor to maternal, foetal and neonatal deaths (Saleem et al. Citation2014). The clinical significance of severe preeclampsia (sPE) lies in its association with maternal and neonatal mortality and morbidity (Sibai Citation2003). If not treated in time, pregnant women suffering from PE may encounter serious complications such as eclampsia, hepatic rupture, stroke, pulmonary edoema, or kidney failure, all of which might lead to life-threatening conditions (Souza et al. Citation2013). Meanwhile, PE is inextricably linked with foetal growth restriction and premature delivery, and the risks of bronchopulmonary dysplasia and cerebral palsy are relatively higher in children born to mothers with PE (Hansen et al. Citation2010; Strand et al. Citation2013). All in all, PE reduces the life quality of pregnant women and increases the risk of postpartum depression (Blom et al. Citation2010; Prick et al. Citation2015). Therefore, it’s imperative to explore and develop effective methods to evaluate the pregnancy outcomes of sPE patients.
In response to the hypoxia triggered by impaired uterine and placental perfusion, various substantial hemodynamic changes occur in the foetus (Goldman-Wohl and Yagel, Citation2002). In foetal hypoxia, blood flow to the kidney, intestines, and lower limbs was reduced to protect blood circulation in the foetal brain, adrenal gland, and myocardium (Dubiel et al. Citation1997, Gunenc et al. Citation2002), the process of which is a compensatory mechanism called brain sparing effect that has been confirmed by researchers in human and animal experiments (Peeters et al. Citation1979). The peak value of the brain sparing effect emerges 2 or 3 weeks before the appearance of late decelerations on an electrocardiogram (Arduini and Rizzo, Citation1992). Evaluation of the hemodynamic changes in the foetus is of great importance to the outcomes of the neonates (Pruetz et al. Citation2015). Given that several studies have proved the association between the Doppler method of hemodynamic assessment and the poor prognosis of neonates (Yalti et al. Citation2004, Ebrashy et al. Citation2005, Simanaviciute and Gudmundsson, Citation2006), the correlation between the Doppler method of hemodynamic assessment and the prognosis of sPE patients deserves to be studied as well.
PE is defined as blood pressure ≥140/90 mmHg at two-time points with an interval of at least 6 h, and proteinuria ≥300 mg/24 h after 20 weeks of gestation (Jeyabalan, Citation2013). Endothelial cell injury belongs to the early pathological characteristics of PE (Young et al. Citation2010). Urine microalbumin (UmA) is an indicator of endothelial dysfunction relating to hypertension, obesity, diabetes, and kidney diseases (Yuyun et al. Citation2004). There is evidence that persistent UmA represents a high possibility of impaired glomerular filtration capacity of the kidney and confers pivotal diagnostic significance in pregnancy as a potential predictor of PE (Hasslacher, Citation1993). Although both the Doppler method of hemodynamic assessment and measurement of UmA are in effect with clear results on diagnosis and prognosis of patients with PE, their combined use in the evaluation of adverse pregnancy outcomes of sPE patients has been ignored in the past. This study intended to investigate the application of ultrasound examination of hemodynamics in the umbilical artery (UA) combined with the measurement of UmA in assessing the adverse pregnancy outcomes of sPE patients.
Materials and methods
Ethics statement
The study protocol was approved by the Ethics Committee of Maternal and Child Health Hospital of Hubei Province. All participants voluntarily signed the informed consent.
Study subjects
All 80 sPE patients aged 26–32 years at the gestational week of 36–39 (average age: 29.19 ± 1.61 years, mean gestational week: 37.71 ± 0.80) were diagnosed and treated in Maternal and Child Health Hospital of Hubei Province from January 2020 to June 2021 were recruited, and patients with other pregnancy complications were excluded by clinical examination. The inclusion criteria were as follows: (1) accorded with the diagnosis criteria of PE; (2) singleton pregnancies; (3) no history of essential hypertension, kidney disease, and diabetes; (4) with complete information, including test results of proteinuria.
Meanwhile, 75 normal pregnant women aged 26–32 years at the gestational week of 37–39 (average age: 29.53 ± 1.65 years, mean gestational week: 38.24 ± 0.54) undergoing physical examination were randomly selected as controls. There were no distinct differences in age and gestational week between these two groups (p > 0.05). Exclusion criteria for all participants were as follows: (1) multiple pregnancies; (2) essential hypertension, kidney disease, and diabetes; (3) chronic infectious disease, autoimmune disease; (4) a history of treatment using the assisted reproduction technology; (5) spontaneous discharge or no record of delivery due to loss of follow-up; (6) incomplete laboratory and auxiliary examination data.
The diagnostic criteria of sPE were as follows: the diagnostic criteria of mild PE refer to the definition of PE put forward by the International Society for the Study of Hypertension in Pregnancy (ISSHP) (Poon et al. Citation2019): systolic blood pressure (SBP) ≥140 mmHg and (or) diastolic blood pressure (DBP) ≥ 90 mmHg after 20 weeks of gestation in women with normal blood pressure, accompanied by any of the following: (1) proteinuria (24-h urine protein ≥300 mg/d or spot urine protein/creatinine ratio ≥0.30 mg/d or urine dipstick testing ≥1+); (2) other maternal organ dysfunction, including acute kidney injury (AKI) (creatinine ≥ 90 μmol/L; 1 mg/dL), liver involvement [increased transaminases such as alanine aminotransferase (ALT) or aspartate aminotransferase (AST) >40 IU/L] with or without right upper quadrant or epigastric abdominal pain, neurological complications (eclampsia, altered mental status, blindness, stroke, clonus, severe headache, persistent visual scotomata), hematological complications [thrombocytopenia-platelet count less than 150,000/μL, disseminated intravascular coagulation (DIC), hemolysis]; (3) uteroplacental dysfunction (including foetal growth restriction, abnormal UA Doppler wave form analysis or stillbirth). sPE was defined when maternal SBP was ≥160 mmHg and (or) DBP was ≥110 mmHg, accompanied by minimal proteinuria, or mild hypertension was accompanied by severe proteinuria (≥2 g/24 h or random urine protein ≥2+).
All pregnant women need to stay in bed after admission. The treatment methods include spasmolysis, hypotension, sedation and diuresis. In case of maternal and foetal complications, pregnancy should be ended in time.
The adverse pregnancy outcome refers to the severe complication of patients with PE that endangers the life of pregnant women and foetuses (Bouzari et al. Citation2014). In this study, adverse pregnancy outcome was defined when asphyxia neonatorum, low birth weight, foetal stress, and foetal growth restriction occurred.
Enzyme-linked immunosorbent assay
First, 5 mL of midstream urine was collected from each pregnant woman in the morning. A 96-well microplate coated with an anti-human albumin polyclonal antibody was used to capture UmA. At the beginning of Enzyme-linked immunosorbent assay (ELISA), the calibrator and the urine samples were pre-diluted 100-fold with 1% phosphate buffer containing bovine serum albumin (BSA-PBS) and 0.1% Tween 20. Then, 10 μL pre-diluted calibrator or sample was added to each antibody-coated well, gently mixed, and incubated at 30 °C for 30 min. After three washes with washing buffer, 100 μL pre-diluted enzyme labelling detecting antibody was added and incubated for 1 h at 30 °C under a gentle stir. Following three washes with washing buffer, the enzyme-substrate K-Blue was added for incubation for 10 min, followed by the addition of 100 μL H2SO4 (1 mol/L) to end the reaction. The absorbance at 450 nm and 620 nm was measured separately.
Colour Doppler ultrasonography
After admission, the Doppler UA blood flow parameters of foetuses were determined using Philips iU22 (Philips, Amsterdam, Netherlands) and Madison H60 colour Doppler ultrasound diagnostic instrument (Samsung, Seoul, Korea) with an abdominal probe frequency of 1-5 MHz. The free-floating segment of the UA was selected (sample volume: 2 mm), at the angle between the ultrasonic beam and the long axis of the UA reaching 0° as much as possible (≤30°), and detection was carried out when foetal movements were less frequent or no breathing movements were observed for the time being. At least 4–6 neat and clear images with the same shape were captured to measure the blood flow parameters. The foetal UA hemodynamic parameters, pulsatility index (PI), and resistance index (RI) were observed, and the difference in the incidence of foetal UA hemodynamic abnormalities between groups was compared. The value of RI >0.8 was considered abnormal in UA blood flow dynamics.
Statistical analysis
Data were subjected to analysis and plotting utilising SPSS21.0 statistical software (IBM Corp., Armonk, NY, USA) and GraphPad Prism 6.0 software (GraphPad Software Inc., San Diego, CA, USA). Normal distribution was verified by Shapiro–Wilk test. Normally distributed measurement data were depicted in the form of mean ± standard deviation. The independent sample t-test was adopted for pairwise comparisons. Non-normally distributed measurement data were described as quartiles. Pairwise comparison was implemented utilising Mann–Whitney U test. Count data were expressed as the number of cases, and the difference between groups was compared using Chi-square test. Logistics multivariate regression analysis was conducted to analyse the risk factors of sPE. The p value was derived from two-sided tests. The difference was regarded as statistically significant when p < 0.05.
Results
Clinical baseline characteristics
A total of 80 sPE patients and 75 healthy participants were enrolled as study subjects. sPE patients (age: 29.19 ± 1.61 years) had a gestational age of 37.71 ± 0.80 weeks at delivery and healthy controls (age: 29.53 ± 1.65 years) had a gestational age of 38.24 ± 0.54 weeks at delivery. The clinical baseline characteristics are illustrated in Table S1. There were no significant differences in age, gestational age at delivery, number of pregnancies, blood urea nitrogen, and placental weight between groups (all p > 0.05), yet obvious differences in alanine aminotransferase, blood platelets and infant birth weight existed between groups (all p < 0.05). Meanwhile, compared with the control group, values of PI and RI were considerably elevated in the sPE group (all p < 0.001).
UmA is highly expressed in sPE patients
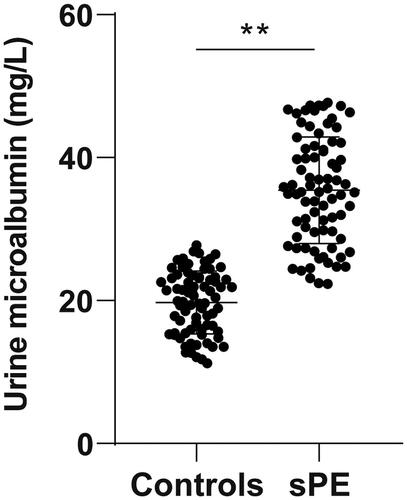
UmA has been indicated as a possible predictor of PE during pregnancy (Mishra et al. Citation2017). Thereafter, we measured UmA in urine samples of sPE patients and healthy controls by ELISA, which revealed higher UmA levels in sPE patients (35.42 ± 7.47 mg/L) than that in healthy controls (19.74 ± 4.39 mg/L) (p < 0.01, ).
Figure 1. UmA level is increased in sPE patients. UmA level in urine samples of sPE patients and healthy controls was measured by means of ELISA. Data were described as mean ± standard deviation. The independent sample t test was applied to compare the difference between groups. **p < 0.01.
UmA level is positively correlated with ultrasonic parameters of UA PI and RI in urine of sPE patients
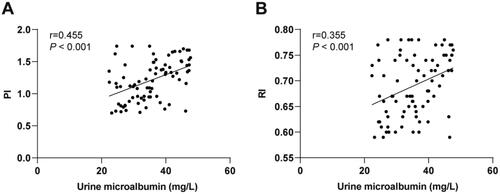
We subsequently analysed the correlation between ultrasonic parameters of UA and UmA levels in sPE patients by Pearson’s co-efficient analysis, which demonstrated that UmA level was positively associated with the values of PI (r = 0.455, p < 0.001) and RI (r = 0.355, p < 0.001) in urine samples of sPE patients ().
Figure 2. UmA level is positively correlated with ultrasonic parameters of UA PI and RI in the urine of sPE patients. The correlation between (A) PI and UmA levels and between (B) RI and UmA levels in sPE patients was analysed by Pearson’s co-efficient analysis.
sPE patients have more adverse pregnancy outcomes
Next, we compared the adverse pregnancy outcomes between groups and found that sPE patients had more total cases of adverse pregnancy outcomes, including asphyxia neonatorum, low birth weight, foetal stress, foetal growth restriction than the healthy controls (p < 0.05, ), suggesting that sPE can predict the adverse pregnancy outcomes of pregnant women. Evidence suggests that persistent UmA signifies a high probability of impaired glomerular filtration capacity of the kidney and therefore can be used as a potential predictor of PE (Mishra et al. Citation2017). To further dig into the relationship between UmA in the urine samples of sPE patients and adverse pregnancy outcomes, we divided sPE patients into the high UmA expression group (N = 40) and low UmA expression group (N = 40) based on the median value of UmA expression. The total number of cases of adverse pregnancy outcomes, including asphyxia neonatorum, low birth weight, foetal stress and foetal growth restriction, were increased in the high UmA expression group relative to those in the low UmA expression group (p < 0.05, ), illustrating that high UmA expression may increase the probability of poor prognosis of sPE patients.
Table 1. Adverse pregnancy outcomes of sPE patients and healthy controls.
Table 2. Comparison of adverse pregnancy outcomes between the high UmA expression group and low UmA expression group.
Values of PI and RI and UmA level are independent risk factors of adverse pregnancy outcomes in sPE patients
Finally, to precisely confirm the influence of ultrasonic parameters of UA and UmA level on adverse pregnancy outcomes of sPE patients, we conducted multivariate analysis to analyse the relationship between adverse pregnancy outcomes and alanine aminotransferase, blood platelets, infant birth weight, values of PI and RI and UmA level. The Logistics regression analysis unravelled that values of PI and RI and UmA level were independent risk factors for adverse pregnancy outcomes in sPE patients (all p < 0.05, ).
Table 3. Logistics multivariate regression analysis of adverse pregnancy outcomes of sPE patients.
Discussion
Unfortunately, PE and its complications remain one of the most devastating causes of death of mothers, foetuses, and neonates, and delivery of the baby and placenta seems the only effective treatment option (Dymara-Konopka et al. Citation2018). UA PI and RI have high specificity and sensitivity for the detection of adverse perinatal outcomes in patients with PE (El-Demiry et al. Citation2020). UmA plays a contributory role in providing a subclinical diagnostic instrument for the prediction of PE (Shaarawy and Salem, Citation2001). In the present study, we pointed out that the combined use of ultrasound examination of UA hemodynamics and determination of UmA can predict adverse pregnancy outcomes in sPE patients.
Measurement of alanine aminotransferase is one of the routine investigations of PE (Kasraeian et al. Citation2018). Uncontrolled activation of platelet in the artery and increment of platelet destruction are common events in PE (Temur et al. Citation2021). The occurrence of PE is independently correlated with low birth weight (Spracklen et al. Citation2015). In the enrolled population, sPE patients exhibited remarkable differences in alanine aminotransferase, blood platelet, and infant birth weight from healthy people. PI/RI ratios in the middle cerebral artery and UA and RI in the UA manifest the highest specificity in predicting adverse perinatal outcomes (Rani et al. Citation2016). After Doppler detection of UA blood flow, we discovered remarkably elevated values of PI and RI in sPE patients, further confirming their indicative values in the examination of sPE patients.
AKI is one of the diagnostic criteria for PE (Poon et al. Citation2019). UmA is recognised as a marker of early AKI (Shatat et al. Citation2016) and an early predictive factor of PE patients with pre-gestational diabetes (Zen et al. Citation2019). Persistent UmA represents high probability of impaired glomerular filtration capacity in the kidney and is of paramount diagnostic significance in pregnancy as a potential predictive factor for PE development (Mishra et al. Citation2017). By means of ELISA, we measured UmA levels in sPE patients and a healthy population and revealed a noticeably raised UmA level in the urine of sPE patients. Therefore, we speculated that the UmA levels in sPE patients might correlate with the UA hemodynamic indexes PI and RI. Pearson’s co-efficient analysis indicated that the UmA level in the urine of sPE patients was positively correlated with UA hemodynamic parameters PI and RI, indicating their consistency in the examination of PE. Furthermore, UmA can effectively reflect renal injury in patients with pregnancy-induced hypertension syndrome (Zhang et al. Citation2019). High levels of UmA in neonates with intrauterine growth restriction reflect subclinical kidney damage after growth restriction (Montaldo et al. Citation2022). We found that the total number of adverse foetal outcomes was increased in sPE patients with high UmA levels. Therefore, it could be inferred that high UmA expression may increase the probability of poor prognosis of sPE patients.
Women with previous PE are prone to higher risks for adverse maternal and foetal outcomes such as foetal growth restriction in subsequent pregnancies (Giannubilo et al. Citation2014). In our study, adverse neonatal events including asphyxia neonatorum, low birth weight, foetal distress, and foetal growth restriction appeared more frequently in infants born to mothers with sPE. Thus, it’s reasonable to conjecture that sPE could predict adverse pregnancy outcomes in pregnant women. Existing evidence suggests that the adoption of Doppler ultrasound on the UA in high-risk pregnant women might help prevent serious illness and death by detecting changes in blood flow patterns in neonates (Alfirevic et al. Citation2017). Increased UmA plays an essential role in the prediction of adverse outcomes, PE included, in high-risk pregnant women (Jayaballa et al. Citation2015; Jin, Citation2020). At present, it has been reported that colour Doppler ultrasound can accurately detect the changes of PI and RI in foetal uterine artery, middle cerebral artery and UA and thus provide references for the judgement of foetal intrauterine state and prediction of adverse pregnancy outcomes, especially the parameters in the late trimester of pregnancy, which have especially high diagnostic values on the adverse pregnancy outcomes (Zhou et al. Citation2022). Nevertheless, this study further probed into the value of colour Doppler ultrasonic examination combined with UmA on the assessment of pregnancy outcomes of sPE patients. Intriguingly, UmA was highly expressed in sPE patients, and the levels of UmA in the urine samples of sPE patients were positively correlated with UA hemodynamic parameters PI and RI. High levels of UmA might increase the risk of poor prognosis in sPE patients. Additionally, we further confirmed that values of PI and RI in UA ultrasound and the level of UmA were independent risk factors of adverse pregnancy outcomes in sPE patients. Hence, UmA can be used as a key monitoring index to evaluate the pregnancy outcomes of sPE patients.
In this retrospective study, by evaluating PI and RI with UA Doppler and measuring UmA, we analysed the correlation between UA hemodynamic parameters (PI and RI) and UmA level in sPE patients using Pearson’s co-efficient analysis and their influence on the adverse pregnancy outcomes in sPE patients using Logistics regression analysis, thus providing a breakthrough point for the clinical judgement of sPE. Despite this, the time span of sample collection was relatively short, and the enrolled population was relatively young, which may cause bias in the UmA level. In addition, the number of case and ultrasonic UA parameters selected for analysis was limited. It’s necessary to expand the sample size and carry out in-depth research to further clarify the prognostic ability of ultrasonic UA quantitative parameters combined with UmA. In the future, a multi-center prospective study will be performed and the sample size will be expanded to increase the persuasiveness of the results and to further analyse their diagnostic and prognostic values in the early stage of the disease.
Supplemental Material
Download MS Word (18.1 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Anon 2013. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol, 122 (5), 1122–1131.
- Alfirevic, Z., et al. 2017. Fetal and umbilical Doppler ultrasound in high-risk pregnancies. Cochrane Database Syst Rev, 6, CD007529.
- Ananth, C.V., et al. 2013. Pre-eclampsia rates in the United States, 1980–2010: age-period-cohort analysis. BMJ, 347, f6564.
- Arduini, D., and Rizzo G. 1992. Prediction of fetal outcome in small for gestational age fetuses: comparison of Doppler measurements obtained from different fetal vessels. Journal of Perinatal Medicine, 20 (1), 29–38.
- Blom, E.A., et al. 2010. Perinatal complications increase the risk of postpartum depression. The Generation R Study. BJOG : An International Journal of Obstetrics and Gynaecology, 117 (11), 1390–1398.
- Bouzari, Z., et al. 2014. Does proteinura in preeclampsia have enough value to predict pregnancy outcome? Clinical and Experimental Obstetrics & Gynecology, 41 (2), 163–168.
- Dubiel, M., et al. 1997. Middle cerebral artery velocimetry as a predictor of hypoxemia in fetuses with increased resistance to blood flow in the umbilical artery. Early Human Development, 47 (2), 177–184.
- Dymara-Konopka, W., et al. 2018. Preeclampsia – current management and future approach. Current Pharmaceutical Biotechnology, 19 (10), 786–796.
- Ebrashy, A., et al. 2005. Middle cerebral/umbilical artery resistance index ratio as sensitive parameter for fetal well-being and neonatal outcome in patients with preeclampsia: case-control study. Croatian Medical Journal, 46 (5), 821–825.
- El-Demiry, N.M., et al. 2020. The value of fetal Doppler indices as predictors of perinatal outcome in women with preeclampsia with severe features. Hypertension in Pregnancy, 39 (2), 95–102.
- Giannubilo, S.R., et al. 2014. Preeclampsia: what could happen in a subsequent pregnancy? Obstetrical & Gynecological Survey, 69 (12), 747–762.
- Goldman-Wohl, D., and Yagel S 2002. Regulation of trophoblast invasion: from normal implantation to pre-eclampsia. Molecular and Cellular Endocrinology, 187 (1-2), 233–238.
- Gunenc, O., et al. 2002. The effect of methyldopa treatment on uterine, umblical and fetal middle cerebral artery blood flows in preeclamptic patients. Archives of Gynecology and Obstetrics, 266 (3), 141–144.
- Hansen, A.R., et al. 2010. Maternal preeclampsia predicts the development of bronchopulmonary dysplasia. The Journal of Pediatrics, 156 (4), 532–536.
- Hasslacher, C., 1993. Clinical significance of microalbuminuria and evaluation of the Micral-Test. Clinical Biochemistry, 26 (4), 283–287.
- Jayaballa, M., et al. 2015. Microalbuminuria is a predictor of adverse pregnancy outcomes including preeclampsia. Pregnancy Hypertension, 5 (4), 303–307.
- Jeyabalan, A., 2013. Epidemiology of preeclampsia: impact of obesity. Nutrition Reviews, 71 Suppl 1 (0 1), S18–S25.
- Jin, H., 2020. Increased levels of glycosylated hemoglobin, microalbuminuria and serum cystatin C predict adverse outcomes in high-risk pregnancies with gestational diabetes mellitus. Experimental and Therapeutic Medicine, 19 (2), 1281–1287.
- Kasraeian, M., et al. 2018. Evaluation of serum biomarkers for detection of preeclampsia severity in pregnant women. Pakistan Journal of Medical Sciences, 34 (4), 869–873.
- Mishra, V.V., et al. 2017. Evaluation of spot urinary albumin-creatinine ratio as screening tool in prediction of pre-eclampsia in early pregnancy. Journal of Obstetrics and Gynaecology of India, 67 (6), 405–408.
- Mol, B.W.J., et al. 2016. Pre-eclampsia. Lancet, 387 (10022), 999–1011.
- Montaldo, P., et al. 2022. Impact of intrauterine growth restriction on cerebral and renal oxygenation and perfusion during the first 3 days after birth. Scientific Reports, 12 (1), 5067.
- Peeters, L.L., et al. 1979. Blood flow to fetal organs as a function of arterial oxygen content. American Journal of Obstetrics and Gynecology, 135 (5), 637–646.
- Poon, L.C., et al. 2019. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: A pragmatic guide for first-trimester screening and prevention. International Journal of Gynaecology and Obstetrics, 145 Suppl 1 (Suppl 1), 1–33.
- Prick, B.W., et al. 2015. Determinants of health-related quality of life in the postpartum period after obstetric complications. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 185, 88–95.
- Pruetz, J.D., et al. 2015. Clinical relevance of fetal hemodynamic monitoring: perinatal implications. Seminars in Fetal & Neonatal Medicine, 20 (4), 217–224.
- Rani, S., et al. 2016. Prediction of perinatal outcome in preeclampsia using middle cerebral artery and umbilical artery pulsatility and resistance indices. Hypertension in Pregnancy, 35 (2), 210–216.
- Saleem, S., et al. 2014. A prospective study of maternal, fetal and neonatal deaths in low- and middle-income countries. Bulletin of the World Health Organization, 92 (8), 605–612.
- Shaarawy, M., Salem M.E. 2001. The clinical value of microtransferrinuria and microalbuminuria in the prediction of pre-eclampsia. Clinical Chemistry and Laboratory Medicine., 39 (1), 29–34.
- Shatat, I.F., et al. 2016. Changes in urine microalbumin-to-creatinine ratio in children with sickle cell disease over time. Frontiers in Pediatrics, 4, 106.
- Sibai, B.M., 2003. Diagnosis and management of gestational hypertension and preeclampsia. Obstetrics and Gynecology, 102 (1), 181–192.
- Simanaviciute, D., and Gudmundsson S., 2006. Fetal middle cerebral to uterine artery pulsatility index ratios in normal and pre-eclamptic pregnancies. Ultrasound in Obstetrics & Gynecology, 28 (6), 794–801.
- Souza, J.P., et al. 2013. Moving beyond essential interventions for reduction of maternal mortality (the WHO Multicountry Survey on Maternal and Newborn Health): a cross-sectional study. Lancet, 381 (9879), 1747–1755.
- Spracklen, C.N., et al. 2015. Effects of smoking and preeclampsia on birth weight for gestational age. The Journal of Maternal-Fetal & Neonatal Medicine, 28 (6), 679–684.
- Strand, K.M., et al. 2013. Mediators of the association between pre-eclampsia and cerebral palsy: population based cohort study. BMJ, 347, f4089.
- Temur, M., et al. 2021. Role of platelet indices in prediction of preeclampsia. Ginekologia Polska, 92 (11), 792–796.
- Yalti, S., et al. 2004. Ratio of middle cerebral to umbilical artery blood velocity in preeclamptic & hypertensive women in the prediction of poor perinatal outcome. Indian J Med Res, 120 (1), 44–50.
- Young, B.C., et al. 2010. Pathogenesis of preeclampsia. Annual Review of Pathology, 5, 173–192.
- Yuyun, M.F., et al. 2004. Microalbuminuria independently predicts all-cause and cardiovascular mortality in a British population: The European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) population study. International Journal of Epidemiology, 33 (1), 189–198.
- Zen, M., et al. 2019. Microalbuminuria as an early predictor of preeclampsia in the pre-gestational diabetic population: A prospective cohort study. Pregnancy Hypertension, 15, 182–188.
- Zhang, L., et al. 2019. The significance of combined detection of CysC, urinary mAlb and beta(2)-MG in diagnosis of the early renal injury in pregnancy-induced hypertension syndrome. Saudi Journal of Biological Sciences, 26 (8), 1982–1985.
- Zhou, P., et al. 2022. Fetal and neonatal middle cerebral artery hemodynamic changes and significance under ultrasound detection in hypertensive disorder complicating pregnancy patients with different severities. Computational and Mathematical Methods in Medicine, 2022, 6110228.