

Abstract
The present study aimed to evaluate the perinatal outcomes and influencing factors in twin pregnancies undergoing emergency cervical cerclage. The present retrospective cohort study included clinical data that were recorded between January 2015 and December 2021 at The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University (China). The study included data from 103 pregnancies (26 twin and 77 singleton pregnancies) that underwent emergency cerclage and 17 twin pregnancies that underwent expectant treatment. The median gestational age of twin emergency cerclage was significantly lower than that of singleton emergency cerclage, but higher than that of expectant treatment (28.5, 34.0 and 24.0 weeks, respectively). The median interval to delivery of twin emergency cerclage was significantly lower than that of singleton emergency cerclage, but significantly higher than that of expectantly treated twin pregnancies (37.0, 78.0 and 7.0 days, respectively).
What is already known on this subject? An important cause of premature birth is cervical insufficiency. Cervical cerclage extends the gestational period of women with cervical insufficiency. According to 2019 SOGC's No. 373-Cervical Insufficiency and Cervical Cerclage, both twin and single pregnancies benefit from emergency cerclage. However, there is minimal information about the pregnancy outcomes of emergency cerclage in twin pregnancies.
What the results of this study add? This study shows that the outcomes of pregnancy in twin pregnancies undergoing emergency cerclage were better than that of expectant treatment but worse than that in singleton pregnancies undergoing emergency cerclage.
What the implications are of these findings for clinical practice and/or further research? In this study, pregnant women with cervical insufficiency in twin pregnancies can benefit from emergency cerclage, we should treat those pregnant women as early as possible.
IMPACT STATEMENT
Introduction
Cervical insufficiency is usually characterised by painless cervical dilation in the second or early third trimester resulting in pregnancy loss or preterm birth (McDonald Citation1978), due to a functional or structural defect of the cervix (Vink and Feltovich Citation2016).
An emergency cerclage is usually performed on pregnant women whose cervix is dilated by 1-2 cm on clinical or ultrasound examination without significant uterine contraction (Chatzakis et al. Citation2020). It was reported that emergency cerclage extended the gestation period of a single pregnancy by 8 and 11 weeks, while conservative treatment prolonged the gestation period by <4 weeks (Costa et al. Citation2019, Zeng et al. Citation2022). To the best of our knowledge, there is limited literature on emergency cerclage in twin pregnancies. According to the 2019 SOGC's No. 373-Cervical Insufficiency and Cervical Cerclage guideline, both twin and singleton pregnancies benefit from emergency cerclage. A previous retrospective study (Kawwass and Badell Citation2018) reported that emergency cerclage was as effective in twins as in singleton pregnancies. However, a recent study (Wei et al. Citation2021) showed that twin pregnancies did not benefit as much from emergency cerclage as single pregnancies. Yet, to the best of our knowledge, the number of cases of twin emergency cerclage reported in the literature remains small. The increase in twin pregnancy rate due to in vitro fertilization-embryo transfer (IVF-ET), as well as the rise in the number of pregnant women with twin cervical insufficiency, allows for the collection of more cases of twin emergency cervical cerclage and a more objective evaluation of its outcomes.
To provide a clinical reference for managing twin cervical dysfunction, the present study compared the pregnancy outcomes of twin expectant treatment and emergency cerclage in twin and singleton pregnancies.
Materials and methods
Study population
The present retrospective cohort study included data recorded at The Second Affiliated Hospital of Wenzhou Medical University (Wenzhou, Zhejiang, China) between January 2015 and December 2021. The study protocol was reviewed and approved by the Ethics and Research Committee of The Second Affiliated Hospital of Wenzhou Medical University (approval no. 2022-K-44-01). The study included data from pregnant patients with cervical dilatation ≥1cm and bulging of the amniotic sac who did not feel uterine contractions during the second trimester. The patients were divided into three groups according to treatment: (i) Group A (twin emergency cerclage, n = 26); (ii) group B (singleton emergency cerclage, n = 77); and (iii) group C (twin expectant treatment, n = 17). Informed consent was signed by all patients for emergency cerclage or expectant treatment. The inclusion criteria were as follows: (i) No evidence to suggest a high risk of aneuploidy or foetal malformation; (ii) no obvious lower abdominal pain or heavy vaginal bleeding; (iii) no amniotic membrane rupture; (iv) no evidence of chorioamnionitis, such as fever (>38 °C), abdominal pain, uterine tenderness, malodorous vaginal discharge, maternal tachycardia (>100 times/min), foetal tachycardia (>160 times/min) and increase in white blood cell count (>15×109/l) (Can et al. Citation2022). Patients with pregnancy complications, including cardiac disease, hepatic disease, renal insufficiency and abnormal haematopoietic system, were excluded.
Basic information
Baseline characteristics included maternal age, previous gravidity, parity and previous abortion, history of uterine or cervical surgery, assisted reproductive technology and cervical dilatation. Primary outcomes included gestational age (weeks) at the time of delivery and interval time to delivery. Secondary outcomes included newborn weight at birth, neonatal asphyxia rate, neonatal intensive care unit (NICU) check-in and neonatal survival rate. Neonatal asphyxia was defined as a neonatal first Apgar score ≤7 (Tunç et al. Citation2022).
Emergency cerclage
Emergency cerclage was performed under lumbar anaesthesia by experienced physicians. The surgical position was the bladder lithotomy position. All patients received prophylactic antibiotics, such as cefuroxime, cefazolin and azithromycin, before and 2 days after surgery. Intraoperative exposure of the cervix was performed using a speculum. If the amniotic sac was protruding out of the cervix, a catheter water sac was used to push the amniotic sac back into the uterine cavity, according to the size of the protruding amniotic sac. The anterior and posterior lips of the cervix were clamped with cervical forceps and the cervix was sutured around the circle using the Johnson & Johnson D8438 suture needle and thread [using the McDonald technique (Locatelli et al. Citation1999)]. The catheter balloon was removed before tying the knot. Routine post-operative bed rest, avoidance of strenuous exercise and contraction inhibitors (ritodrine) were administered for 2–5 days to prevent infection. The dosage of contraction suppressants was adjusted according to maternal contractions and discontinued if the contractions could not be suppressed or an intrauterine infection was suspected.
Expectant treatment
Expectant treatment included bed rest, breech elevation, anti-infection and uterine contractions suppression. Antibiotics were not routinely used prophylactically but were administered for at least 3 days to prevent infection if the patient presented with premature rupture of membranes and prolonged vaginal bleeding. Contraction inhibitors, such as ritodrine or atosiban, were used depending on the contractions. At <32 weeks of gestation, magnesium sulphate was used for foetal neuroprotection. At <35 weeks of gestation, dexamethasone was used for foetal lung maturation in patients who were likely to deliver within 1 week.
Statistical analysis
Statistical analysis was performed using SPSS 26.0 (IBM Corp.). Data are expressed as mean ± standard deviation. Normally distributed data were analysed with the Student’s t-test, while non-normally distributed data were analysed with the Mann–Whitney U. Categorical variables were compared using the Chi-square test. The gestational ages at delivery of single and twin pregnancies were compared using the Kaplan-Meier survival analysis. The Cochran-Armitage Trend test was used to identify trends in single and twin pregnancies delivered at different gestational weeks. A stratified Chi-square test was performed to test for confounding factors that might affect pregnancy outcomes.
Results
Basic clinical characteristics of the patients
The age, gravidity or parity, previous early and late miscarriage, as well as history of hysteroscopy, were similar between twin emergency cerclage and expectant treatment. Patients in the twin emergency cerclage group were slightly younger than those in the singleton emergency cerclage group (29.0 vs. 32.0 years; P = 0.004). A proportion of 76.9% of patients in the twin emergency cerclage group was IVF-ET; however, the history of hysteroscopy was similar among all the groups.
Conditions on admission
The conditions on admission of the three groups of patients are shown in . On admission, half of the patients had vaginal bleeding and all underwent physical and laboratory examinations before cervical cerclage or expectant treatment to exclude chorioamnionitis. The white blood cell count, C-reactive protein, neutrophil ratio and vaginal secretions in the twin emergency cerclage group were not significantly different from those in the singleton emergency cerclage and expectant treatment groups. The median cervical dilation was 2.5 cm in the twin emergency cerclage group and it showed no significant difference compared with that in the other two groups (3 and 2.5 in the singleton emergency cerclage and expectant treatment groups, respectively). The cervical dilatation was measured at 21–24 weeks of gestation.
Table 1. Three groups of pregnant women on admission.
Pregnancy outcomes of twin and singleton emergency cerclage and twin expectant treatment
The twin emergency cerclage group showed a significant increase in newborn survival rate, while the 1 and 5 min neonatal asphyxia rates were considerably decreased compared with those in singleton emergency cerclage and expectant treatment groups. The NICU rate in the twin emergency cerclage group was significantly higher than that in the singleton emergency cerclage group (80 vs. 42.4%). The gestational age and weight at birth in the twin emergency cerclage group were lower than those in the singleton emergency cerclage group. The median interval time to delivery in the twin emergency cerclage group was significantly higher than that in the expectant treatment group, but lower than that in the singleton emergency cerclage group (37.0, 7.0 and 78.0 days, respectively; ).
Table 2. Pregnancy outcomes of twin and singleton emergency cerclage and twin expectation treatment.
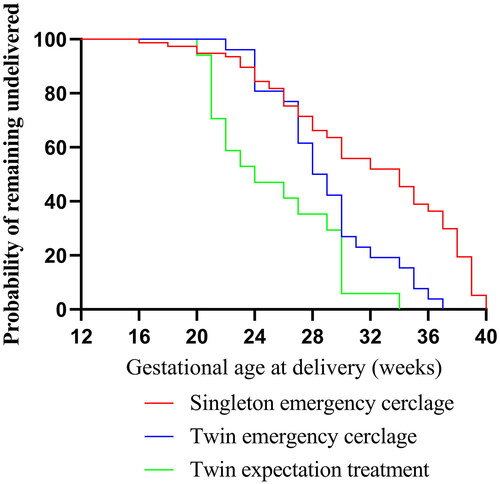
Survival curves of twin and singleton emergency cerclage and twin expectant treatment
The survival curves of the three groups are shown in . The Kaplan–Meier survival curves showed that the gestational age at delivery in the twin emergency cerclage group was increased compared with that in the expectant treatment group (28.5 vs. 24.0 weeks; P = 0.0224), but it was decreased compared with that in the singleton emergency cerclage group (28.5 vs. 34.0 weeks; P = 0.0007).
Figure 1. Survival curves of the three groups.
The proportion of deliveries in different gestational weeks of twin and singleton emergency cerclage and twin expectant treatment groups
The proportions of deliveries in different gestational weeks were statistically different between twin and singleton emergency cerclage groups (P = 0.011; ). At gestational age <26 weeks, twin and singleton emergency cerclage groups accounted for 26.3 and 73.7% of the deliveries, respectively. The proportion of deliveries increased in the twin singleton emergency cerclage group from 26–34 weeks, but it decreased to 3.4% after 37 weeks of gestation (odds ratio, 0.100; 95% CI, 0.011–0.940; P = 0.044). The percentage of patients who delivered before 34 weeks of gestation was significantly higher for twins than for singleton emergency cerclage (80.8 vs. 48.1%; P = 0.004; Table S1). Moreover, 52.9% of patients with twin cervical insufficiency in the expectant treatment group delivered before 26 weeks, while only 19.2% of patients in the emergency cerclage group delivered before 26 weeks.
Table 3. The proportion of deliveries in different gestational weeks of twin and singleton emergency cerclage.
Difference of risk factors between twin and singleton emergency cerclage
Table S2 shows the difference in risk factors between twin and singleton cervical insufficiency groups. When cervical dilation was <3 cm during emergency cerclage or no premature rupture of membranes occurred after emergency cerclage, the risk of foetal preservation failure in twin emergency cerclage was greater than that in singleton emergency cerclage. There was no significant difference in the risk of foetal preservation failure between twin and singleton emergency cerclage when cervical dilation was >3 cm, or premature rupture of membranes occurred after cerclage.
Discussion
The sudden dilation of the cervix in the mid-trimester leads to adverse pregnancy outcomes, such as abortion and premature delivery. The clinal decision-making process during pregnancy can be complex, especially in the presence of twin pregnancies. This must balance perinatal risks, pros and cons of cervical cerclage vs. expectant treatment, and the patient’s values and preferences. Emergency cervical cerclage for a dilated cervix with exposed membranes is effective in singleton pregnancies. In twin pregnancies, several studies also suggested a beneficial effect of emergency cervical cerclage in pregnancy prolongation and neonatal survival. Studies have reported prolongation of pregnancy by 4.4–13 weeks following rescue cerclage, and the neonatal survival rate was 50–83.3% (Rebarber et al. Citation2014, Abbasi et al. Citation2018, Chun et al. Citation2018, Park et al. Citation2018). The present findings were also encouraging, with the median interval to delivery being ∼37 days and the neonatal survival rate being 75%.
Following an emergency cerclage for cervical dilatation, the median gestational age at delivery and the median time from cerclage placement to delivery appeared similar between twin and singleton pregnancy (Rebarber et al. Citation2014, Park et al. Citation2018). A previous study (Miller et al. Citation2014) reported that, although twin pregnancies were more likely to deliver at a slightly earlier median gestation [31.9 weeks; interquartile range (IQR), 24.9–35.1 weeks] than singletons (32.7 weeks; IQR, 24.6–38.3 weeks) (P = 0.015), the frequency of delivery before 28 weeks did not differ between twin and singleton pregnancy (33.7 vs. 35.8%; P = 0.69). The present study found that the median gestational age at delivery of twin emergency cerclage (28.5 weeks; IQR, 27–31 weeks) was significantly lower than that of singleton emergency cerclage (34 weeks; IQR, 27–38 weeks) (P = 0.018), and the prolongation of gestational age of twin emergency cerclage was significantly lower than that of singleton emergency cerclage (37.0 vs. 78 days; P = 0.007). Although the neonatal survival rates were similar (75 vs. 77.6%), the proportion of deliveries in different gestational weeks was different between the two groups, with a significantly higher proportion of twin emergency cerclage pregnancies being delivered before 34 weeks compared with that in the singleton emergency cerclage group (80.8 vs. 48.1%; P = 0.004). Furthermore, twin emergency cerclage had a higher NICU rate and lower birth weight than singleton emergency cerclage.
The present study compared the perinatal outcomes of twin emergency cerclage and expectant treatment to find that women in the cerclage group gave birth at a more advanced median gestational age (28.5 vs. 24.0 weeks), had a longer median interval to delivery (37 vs. 7 days), had a higher neonatal survival rate (75 vs. 35.3%), while 52.9% of women with twin cervical insufficiency who received expectant treatment delivered before 26 weeks. Only 19.2% of the twin emergency cerclage group delivered before 26 weeks. It was reported by two retrospective studies that twin emergency cerclage had improved perinatal outcomes compared with expectant treatment (Roman et al. Citation2016, Abbasi et al. Citation2018). Therefore, the role of emergency cerclage is of potential value in the management of twin gestation when the cervix is dilated and the amniotic membrane is bulging.
Finally, the current study analysed the risk factors for emergency cerclage in twin and singleton pregnancies and found that when cervical dilation was <3 cm or there was no premature rupture of the membranes after emergency cerclage, the delivery risk of twin emergency cerclage was significantly higher than that of singleton emergency cerclage. By contrast, when the cervical dilatation was >3 cm or premature rupture of membranes occurred after emergency cerclage, regardless of the occurrence of abnormal leukorrhoea, both single and twin pregnancies showed a similar increased delivery risk after emergency cerclage.
Limitation
We compared twin and singleton emergency cerclage, and analysed the difference of risk factors between twin and singleton emergency cerclage, so that we can more directly understand the effect of twin emergency cerclage. However, this study has some limitations. First of all, the incidence of cervical insufficiency with twin pregnancy is relatively low, although we have collected all data of pregnant women with cervical dysfunction in the past six years, the number of twin pregnancy is still insufficient. Secondly, this study is a retrospective cohort study, surgeons and the pregnant woman’s desire for treatment can affect the results of the study.
Conclusions
In a word, pregnant women with cervical insufficiency in twin pregnancies can benefit from emergency cerclage. This procedure prolongs the gestational age and improves the survival rate of the newborn. This study provides clinical support for extending the gestational weeks of twin pregnancies and reducing the rate of preterm birth and neonatal mortality.
Supplemental Material
Download MS Word (15.4 KB)Disclosure statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The primary data used to support the results of this study are available on reasonable request to the corresponding author.
Additional information
Funding
References
- Abbasi, N., Barrett, J. and Melamed, N., 2018. Outcomes following rescue cerclage in twin pregnancies. The Journal of Maternal-Fetal & Neonatal Medicine, 31 (16), 2195–2201.
- Can, E., Oğlak, S. C. and Ölmez, F., 2022. Maternal and neonatal outcomes of expectantly managed pregnancies with previable preterm premature rupture of membranes. The Journal of Obstetrics and Gynaecology Research, 48 (7), 1740–1749.
- Chatzakis, C., et al. 2020. Emergency cerclage in singleton pregnancies with painless cervical dil atation: A meta-analysis. Acta Obstetricia et Gynecologica Scandinavica, 99 (11), 1444–1457.
- Chun, S., et al. 2018. Effects of emergency cerclage on the neonatal outcomes of preterm twin pregnancies compared to preterm singleton pregnancies: A neonatal focus. PloS One, 13 (11), e0208136.
- Costa, M. M. F., et al. 2019. Emergency cerclage: gestational and neonatal outcomes. Revista da Associacao Medica Brasileira, 65 (5), 598–602.
- Kawwass, J. and Badell, M., 2018. Maternal and Fetal Risk Associated With Assisted Reproductive Technology. Obstetrics and Gynecology, 132 (3), 763–772.
- Locatelli, A., et al. 1999. Amnioreduction in emergency cerclage with prolapsed membranes: compari son of two methods for reducing the membranes. American Journal of Perinatology, 16 (2), 73–77.
- Mcdonald, I., 1978. Incompetence of the cervix. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 18 (1), 34–37.
- Miller, E., Rajan, P. and Grobman, W., 2014. Outcomes after physical examination-indicated cerclage in twin gestations. American Journal of Obstetrics and Gynecology, 211 (1), 46.e1-5–46.e5.
- Park, J., et al. 2018. Outcomes of physical examination-indicated cerclage in twin pregnancies with acute cervical insufficiency compared to singleton pregnancies. Journal of Perinatal Medicine, 46 (8), 845–852.
- Rebarber, A., et al. 2014. Outcomes of emergency or physical examination-indicated cerclage in twin pregnancies compared to singleton pregnancies. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 173, 43–47.
- Roman, A., et al. 2016. Cerclage in twin pregnancy with dilated cervix between 16 to 24 weeks of gestation: retrospective cohort study. American Journal of Obstetrics and Gynecology, 215 (1), 98.e1–98.e11.
- TUNç, Ş., et al. 2022. The evaluation of the antepartum and intrapartum risk factors in predi cting the risk of birth asphyxia. The Journal of Obstetrics and Gynaecology Research, 48 (6), 1370–1378.
- Vink, J. and Feltovich, H., 2016. Cervical etiology of spontaneous preterm birth. Seminars in Fetal & Neonatal Medicine, 21 (2), 106–112.
- Wei, M., et al. 2021. A comparison of pregnancy outcome of emergency modified transvaginal c ervicoisthmic cerclage performed in twin and singleton pregnancies. Archives of Gynecology and Obstetrics, 303 (5), 1197–1205.
- Zeng, C., et al. 2022. Pregnancy outcomes and factors affecting the clinical effects of emerg ency cerclage in twin pregnancies with cervical dilation and prolapsed membranes. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics, 157 (2), 313–321.