

Abstract
Background
The Menstrual Distress Questionnaire (MDQ) is a commonly used questionnaire that assesses various symptoms and distress associated with the menstrual cycle in women. However, the questionnaire has not been completely translated into Chinese with rigorous reliability and validity testing.
Methods
This study translated the Menstrual Distress Questionnaire Form Cycle (MDQC) from English into Chinese: MDQCC in two stages. First, it was translated forward and backward using Jones’ model; second, to test the validity and reliability, 210 Chinese-speaking women were recruited through online announcements and posters posted between June 2019 and May 2020. Expert validity, construct validity, convergent validity, and factorial validity were determined using content validity index (CVI), intraclass correlation coefficient (ICC), composite reliability (CR), and exploratory factor analysis, respectively. For concurrent criterion validity, MDQCC score was compared with three existing pain scales. Reliability was evaluated using internal consistency across items and two-week test-retest reliability over time.
Results
The CVI for content validity was .92. Item-CVI for expert validities among the 46 items ranged from .50 − 1; scale-CVI for the eight subscales, from .87 − 1; ICC, from .650 − .897; and CRs, from .303 − .881. Pearson correlation coefficients between MDQCC and short-form McGill pain questionnaire, present pain intensity, and visual analog scale scores were .640, .519, and .575, respectively. Cronbach’s α for internal consistency was satisfactory (.932). ICC for test-retest reliability was .852 for the entire MDQCC.
Conclusion
MDQCC was valid and reliable for Mandarin Chinese-speaking women. It can be used to evaluate female psychiatric symptoms related to the menstrual cycle in future work.
PLAIN LANGUAGE SUMMARY
The Menstrual Distress Questionnaire has been used to evaluate menstrual distress, including dysmenorrhoea and premenstrual syndrome. This questionnaire has been translated into Persian, Korean, Japanese, and Cantonese, rendering it to be used more and more widely all over the world. The study translated all 46 items of the Menstrual Distress Questionnaire from English to Mandarin Chinese using a two-stage strategy. The Chinese version of this questionnaire developed by the present study was found to be a valid and reliable tool in Chinese Mandarin-speaking female populations. It could be used to evaluate women’s physical and psychiatric symptoms related to the menstrual cycle in future works.
1. Introduction
The Menstrual Distress Questionnaire (MDQ) is a self-administered inventory for assessing subjective symptoms related to the menstrual cycle (Moos Citation1968). In English-speaking societies, the MDQ is commonly used in clinical approaches and research for measuring primary dysmenorrhoea and premenstrual symptoms (PMS) (Nillni et al. Citation2013; Nguyen et al. Citation2017; Shirwaikar Thomas et al. Citation2020), both of which are extremely bothersome illnesses for women of reproductive age (Wong et al. Citation2018). The MDQ quantises subjective symptoms that identify dysmenorrhoea and PMS (Freeman Citation2003; Ferries-Rowe et al. Citation2020). These symptoms are associated not only with pain and miscellaneous physical symptoms but also with psychological ailments that occur during certain phases of the menstrual cycle (Freeman Citation2003; Hofmeister and Bodden Citation2016). Menstruation has become one of the life stressors that impact mental the health of women (Demir et al. Citation2021; Yilmaz et al. Citation2021).
The MDQ is used to assess physical, psychological, and behavioural symptoms during the menstrual, premenstrual, and intermenstrual phases of the menstrual cycle (Moos Citation2010), with good validity and reliability (Thys-Jacobs et al. Citation1995; Sigmon et al. Citation2000; Moos Citation2010). A total of 46 related items that reflect eight subscales were included in the MDQ. The eight subscales include three subscales for somatic symptoms (pain, water retention, and autonomic reactions); three subscales for mood and behavioural changes (negative affect, impaired concentration, and behaviour change); one subscale for arousal; and one for instrument control. Each of the eight subscales is composed of an interrelated set of items, and each item is scored on a 5-point Likert scale (see Supplemental Material 1). In the original design by Rudolf H. Moos, there are two forms of MDQ: the MDQ Form Cycle (MDQC) and MDQ Form Today. Among them, the MDQ Form Today is used to record daily symptoms, whereas the MDQC is used to screen for menstrual cycle-related illnesses by describing their symptoms and reactions during the three phases of their most recent menstrual cycle (Choi Citation2017).
The MDQC has been translated into several languages, including Persian (Mohamadirizi and Kordi Citation2015; Asgari et al. Citation2020), Korean (Kim et al. Citation2016), Japanese (Ueno et al. Citation2016), and Cantonese (Chang et al. Citation1999). Several groups of researchers have attempted to translate partially the MDQC into Chinese Mandarin. Wang (Citation1991) and Chung et al. (2013) translated 14 items and 22 items, respectively, among the 46 items of the MDQ. Chou et al. (2009) translated all 46 MDQC items and applied them in research, but the reliability and validity of the instrument were not tested. So far, the whole questionnaire has not been completely translated into Chinese with rigorous reliability and validity testing. Because of the increasing use of MDQC in the world, our work will make it possible to measure menstrual-related symptoms and to compare measurement results between Chinese-speaking populations and other areas of the world in future works. This study aimed to completely translate the MDQC using Jones’ model and conduct reliability and validity tests among Chinese Mandarin-speaking women.
2. Materials and methods
2.1. Study design
The translation process was designed based on current measurement principles, which adopted a two-stage designed translation process of Jones’ translation model (Jones et al. Citation2001). Using this model, the systematic forward-backward translation was in the first stage, and the validity and reliability tests were in the second stage.
2.2. Translation
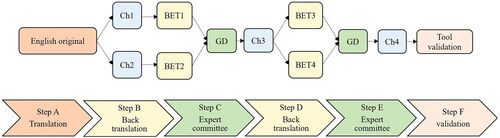
Permission to translate the MDQ was obtained from the original author, Professor Rudolf H. Moos (see Supplemental Material 2), and from the current publisher of the instrument, Mind Garden Inc. The first stage of the two-stage design model included the translation of the MDQC. To retain the equivalency of meanings across the original instrument and the translation, the translation process adopted a decentred translation strategy developed by Brislin and Jones for cross-cultural and cross-language adaptation of self-report measures (Jones et al. Citation2001; Yeh Citation2002) (). Six bilingual experts, who were familiar with both cultures and spoke both languages, were involved in the translation process. Two of them conducted the forward translation from English into Chinese, and two others translated the forward-translated Chinese version back into English independently. Backward translators were blinded to the original English MDQC. According to the suggestion of the “translating instruction for cross-cultural studies” (Peters and Passchier Citation2006), the above four bilingual experts were then involved in the first meeting with the investigator to review the backward translations. The first meeting discussed the discrepancies and achieved the most appropriate culturally equivalent translation. The new Chinese version was then independently back-translated into English by two bilingual experts. The second meeting of bilingual experts was held to review the new backward translations. All of the remaining discrepancies were resolved through thorough discussions to assure semantic, idiomatic, experiential, and conceptual equivalence with the original version of the MDQC. The back-translated English questionnaire was sent to the original author, Professor Rudolf H. Moos, to confirm that words in the backward-translated English version were the same as in the original one (see Supplemental Material 3). The final MDQC Chinese (MDQCC) version (Supplementary Table S1) was accepted by Mind Garden Inc. to become one of the questionnaires of the publisher (see Supplemental Material 4, and link to https://www.mindgarden.com/119-menstrual-distress-questionnaire#horizontalTab4).
Figure 1. Translation process following Jones’ Translation Model. Ch1: Chinese version 1; Ch2: Chinese version 2; Ch3: Chinese version 3; Ch4: Chinese version 4; BET1: first backward English translation; BET2: second backward English translation; BET3: third backward English translation; BET4: fourth backward English translation; GD: group discussion.
2.3. Participants for tool validation
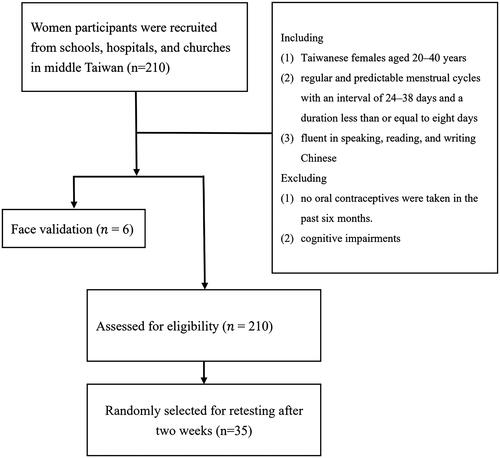
The inclusion criteria for subject enrolment were as follows: (1) Taiwanese females aged 20–40 years; (2) regular and predictable menstrual cycles, with an interval of 24–38 days and a duration less than or equal to eight days (Sun et al. Citation2018); (3) fluent in speaking, reading, and writing Chinese; and (4) no oral contraceptives were taken in the past six months. Those with cognitive impairments were excluded from the study. A total of 210 subjects were recruited. Their occupations were student, office worker, teaching staff, etc. Participants were invited to fill out a demographic information sheet, the MDQCC, the short-form McGill pain questionnaire (SF-MPQ), the present pain intensity (PPI), and the visual analog scale (VAS). Among the 210 volunteers (Comrey Citation1988; Mundfrom et al. Citation2005), 35 randomly selected participants (Wu Citation2006; Castellanos et al. Citation2018; Beykmirza et al. Citation2022) completed the MDQCC twice at an interval of two weeks (Anthoine et al. Citation2014; Lin et al. Citation2017). shows the participants recruitment flowchart. Data for this study were collected between June 2019 and May 2020.
Figure 2. Flow diagram for recruitment of participants to test for validity and reliability of the Chinese version of the Menstrual Distress Questionnaire Form Cycle.
2.4. Compliance with ethical standards
Study approval was obtained from the research ethics committee of the China Medical University Hospital with reference number CMUH108-REC3-052 (see Supplemental Material 5). Written informed consent was obtained after a detailed explanation of the purpose and procedures of this study. Oral and written information about the study was provided to all participants. The information provided to prospective participants included the purpose of the study, the possibility to withdraw at any time point, and the assurance that data would be presented only at the group level and that all individual data would be anonymized.
2.5. Tool validation
Validities included content validity, construct validity, and concurrent criterion validity. Content validity was tested using expert and face validities. Construct validity was tested using intraclass correlation, convergent validity, and factorial validity. Concurrent criterion validity was tested via Pearson correlation analysis between the MDQCC and three existing dysmenorrhoea scales.
The expert validity was measured according to the item-objective relevance to the content validity index (CVI), including both item-CVI (I-CVI) and subscale-CVI (S-CVI). Six specialists, including two gynaecologists, one traditional Chinese medicine gynaecologist, one psychiatrist, one associate professor of nursing, and one epidemiologist, rated the clarity of each item on a 5-point Likert scale. For each item, the I-CVI was computed as the number of experts giving a rating of “very relevant” divided by the total number of experts, resulting in a value between 0 and 1. The average S-CVI was calculated by dividing the sum of the I-CVIs by the total number of items (Rodrigues et al. Citation2017). To test the face validity, six Taiwanese women took part in the pilot (Wild et al. Citation2005; Marmarà et al. Citation2017). All 46 items were completely understood after reading. The average time taken to complete the questionnaire was nine minutes.
The construct validity was measured using the intraclass correlation coefficient (ICC); the convergent validity was measured using the composite reliability (CR), and the factorial validity was measured using the exploratory factor analysis (EFA) (Ross et al. Citation2003; Adawi et al. Citation2018; Rawy et al. Citation2021). The ICC value was obtained from a two-way random-effects model (Koo and Li Citation2016). Intercorrelations between subscales were evaluated using Pearson’s correlation analysis (Vambheim et al. Citation2017). The concurrent criterion validity was assessed using the Pearson correlation analysis between scores of the MDQCC and of three existing self-reporting pain scales commonly used to assess dysmenorrhoea, including the SF-MPQ, the PPI, and the VAS (Asgari et al. Citation2020; Yu et al. Citation2020).
Reliability was evaluated using internal consistency and a two-week test-retest reliability. The internal consistency reliability was assessed using Cronbach’s α (Taber Citation2018). The test-retest reliability was measured using the ICC analysis (Lin et al. Citation2017).
Data analyses were conducted using IBM SPSS Statistics 24 for Windows (IBM Inc., Armonk, NY, USA). A p-value of less than .05 was considered statistically significant in all analyses of this study.
3. Results
3.1. Participants and scores of the MDQCC
A total of 210 healthy women were recruited to complete the questionnaire. The demographic characteristics revealed that they were generally young, with a mean age of 25.7 ± 4.8 years. Participants were well-educated, with a mean education of 16.6 ± 2.1 years. A majority of the participants were unmarried (93.8%) and without children (95.2%). The length of their menstrual cycle was 30.3 ± 2.9 days and the duration of menstrual flow was 5.8 ± 1.1 days (). Among the scores of the eight subscales of the MDQCC for the premenstrual, menstrual, and intermenstrual phases, the pain subscale in the menstrual phase gained the highest score: 1.18 ± 0.81 score/item. The menstrual phase had the highest score on the subscales of pain; the premenstrual phase had the highest score on the subscale of water retention; and the intermenstrual phase had the highest score on the subscale of arousal (Supplementary Table S2).
Table 1. Demographic characteristics of the 210 subjects.
3.2. Content validity
The I-CVI levels for the expert validity for the 46 items ranged from 0.5 to 1 (see Supplementary Table S3). Item 37, “orderliness” had the lowest I-CVI: 0.5. The S-CVI levels ranged from 0.87 to 1. The arousal subscale, which included Item 37, had the lowest S-CVI (0.87).
3.3. Construct validity
The construct validity of the MDQCC was evaluated using the ICC, the convergent validity, and the factorial validity. The ICCs for the construct validity of the eight subscales varied from .650 for control to .897 for negative affect. The CRs for convergent validity ranged from .303 to .881 among the eight subscales (see ).
Table 2. Validity of the MDQCC (N = 210).
The factorial validity of the MDQCC was measured using the EFA in the menstrual phase. The KMO measure of sampling adequacy recorded a value of 0.786, and Bartlett’s sphericity test resulted in a χ2 of 6248.9 (df = 1035, p < 0.001). The contribution of the eight factors to the total variance was 61.2%. The factor loadings ranged from .118 to .864. These factors are generally consistent with the original conceptual model. Items that fell into different factors from the original MDQC were as follows: Item 1 (muscle stiffness), Item 2 (headache), Item 3 (cramp), Item 4 (backache), Item 5 (fatigue), Item 6 (general aches and pains), Item 23 (insomnia), Item 43 (ringing in the ears), and Item 46 (blind spots, fuzzy vision) (see Supplementary Table S4).
3.4. Subscale intercorrelation
Intercorrelations between the average scores of any two of the eight subscales across the three phases of the menstrual cycle were significant, except for the intercorrelation between water retention and arousal. Positive correlations were found among all the subscales (Supplementary Table S5).
3.5. Concurrent criterion validity
In the test of the concurrent criterion validity, Pearson correlation analyses revealed that the MDQCC score was positively correlated with the SF-MPQ, the PPI, and the VAS, with correlation coefficients of .597, .442, and .463, respectively (p < 0.01) (Supplementary Table S6).
3.6. Internal consistency reliability and test-retest reliability
Cronbach’s α for the internal consistency reliability was .932 for the entire MDQCC. The reliabilities ranged from .653 to .913 for the individual subscales. The overall ICC for the two-week test-retest reliability in the menstrual phase was .852. The ICC values for the individual subscales ranged from .637 to .906. The arousal subscale had the lowest ICC of .637 ().
Table 3. Reliabilities including internal consistency and test-retest reliability of the MDQCC (N = 210).
4. Discussion
The two-stage strategy adopted in the present study is the most commonly used method for achieving the quality of translation used in cross-cultural social research (Wu Citation2006). In the first stage, backward translation is necessary for improving translation quality, which usually refers to the equivalence between the target and source languages (Lin et al. Citation2017). Group meetings played an important role in the first stage. During the forward and backward translations, the diversity of translators plays an important role. A group discussion, therefore, allows bilingual experts to discuss and choose the most appropriate words.
The MDQCC had relevant I-CVI and excellent S-CVI scores in terms of clarity, representing satisfactory content validity. However, the ICCs for construct validity varied from .650 for control to .897 for the negative affect subscale. Low ICC for the control subscale indicated that item similarity in the control subscale was not as high as that in the other subscales (Koo and Li Citation2016). The MDQCC has acceptable convergent and concurrent criterion validities. In the EFA, Items 3 (cramps), 4 (backache), 5 (fatigue), and 6 (general aches and pains) were not categorised as Items 1 (muscle stiffness) and 2 (headache) of the original categorisation of the MDQ. This might be because the symptoms of the original pain subscale were caused by different aetiologies, although all of them manifested pain. Item 23 (insomnia) was originally designed in the subscale of impaired concentration; however, in the EFA, it went with the items of negative affect. Clinically, insomnia may be related more to negative affect than to impaired concentration (Reeve et al. Citation2018). The intercorrelation analysis revealed that except for water retention and arousal, any two of the subscales in the MDQCC positively correlated with each other. The low intercorrelations between water retention and arousal subscales were speculated because arousal and water retention are the most difficult subscales to correctly measure in the MDQCC. Measurement of arousal in Eastern people is considered difficult because they are usually hesitant to discuss it and, therefore, tend to report low arousal emotions (Lim Citation2016). This may also explain why all the correlation coefficients between the arousal subscale and the other subscales are low. Water retention is difficult to measure because symptoms in this subscale require a physical examination for diagnosis. This study also found that the control subscale was positively correlated with all of the other scales, indicating that women who reported symptoms frequently associated with the menstrual cycle also tended to endorse symptoms that were not menstrual cycle-related. This result was consistent with that of the original MDQC questionnaire (Moos Citation2010). The Pearson correlation coefficients between the MDQCC and the SF-MPQ, the PPI, and the VAS were moderately relevant, indicating that the MDQCC was comparable to the commonly used tools (Akoglu Citation2018).
In reliability tests, the MDQCC had excellent overall internal consistency reliability. For individual subscales, a Cronbach’s α value of 0.913 for negative affect showed excellent internal consistency reliability. The Cronbach’s α values showed acceptable and good internal consistency reliability for pain, autonomic reactions, impaired concentration, behaviour change, and arousal. Cronbach’s α values of 0.686 for water retention and 0.653 for control showed poor internal consistency reliability in these two subscales. The result of consistency reliability in the present study was similar to that in the original MDQ, which had Cronbach’s α values of 0.92 for negative affect, 0.63 for water retention, and 0.64 for control (Moos Citation2010). The low Cronbach’s α in the water retention subscale might be because there are only four items in this subscale, which cannot generate a large Cronbach’s α. In this case of a small item number, a Cronbach’s α of more than 0.6 for a subscale is considered acceptable (van Griethuijsen et al. Citation2015; Zeugfang et al. Citation2018).
The two-week test-retest reliability was good for the overall MDQCC and varied from moderate to excellent for the subscales based on ICC values.
Compared with the original MDQ English version, and Cantonese version, the Cronbach’s α for internal consistency of subscales of MDQCC were quite similar to the above two questionnaires. All three have the highest Cronbach’s α higher than 0.9 for the negative affect subscale, and have the lowest Cronbach’s α around 0.65 for the water retention subscale (Chang et al. Citation1999; Ross et al. Citation2003). The ICC value for test-retest reliability of MDQCC was also similar to that of the original English version, both were around 0.8. In both questionnaires, the subscale that had the highest test-retest reliability was the pain subscale, and the subscale that had the lowest test-retest reliability was the control (Markum Citation1976).
In the present study, subjects took 9 min to complete the MDQCC—4 min more than that reported by Moos (Citation1968). This may be attributed to the fact that the average saccade size when reading Chinese is about 2.6 characters compared to roughly 7–8 letters for English (Yan et al. Citation2006), rendering the Chinese version time-consuming. The subject characteristics recruited in the present study were similar to those of the original English MDQC study. Subjects in both studies were young (25.2 vs. 25.7 years) and generally possessed high education (about 90% were educated beyond the high-school level). The length and flow of menstrual cycles were similar in both studies. In the original study, the average length of the cycle was 30.3 days and days of menstrual flow were 5.5 days (Moos Citation1968), comparable to 30.3 and 5.8 days, respectively in the present study. The main difference, however, between the study subjects in the two studies is that only half of the participants in the original study were unmarried and did not have children, but more than 90% of the subjects were unmarried and did not have children in our study.
In this study, the feature of scores among the three phases was similar to that of the original English MDQC. Generally, women had the highest score in the menstrual phase, followed by the premenstrual phase in both studies. The only difference was the negative affect subscale. In Moos’ study, the negative affect subscale, which had the highest score in the premenstrual phase, followed by that in the menstrual phase, coincides with research in the U.S. (Woods et al. Citation1982). However, our study showed that the score of negative affect was highest in the menstrual phase, followed by that in the premenstrual phase. The present result is consistent with a study conducted in Japan (Nagata et al. Citation2004). We speculated that Eastern women experience more negative effects during the menstrual phase than Western women—this speculation requires further investigation.
Two limitations of this study must be considered. First, the first limitation included the absence of cross-cultural validity testing, in which both the MDQCC and the original MDQC needed to be filled by the same bilingual participants. As bilingual participants are difficult to recruit—and that would reduce the sample size—we decided to have a large sample size and adopt Jones’ model to achieve cross-cultural equivalency. Second, although Taiwanese is a region where Mandarin Chinese is the primary language, the idiomatic usage of words is slightly different from that of other regions. If MDQCC is planned to be used in Chinese-speaking areas outside of Taiwan, further validation is needed.
In conclusion, the cross-cultural translation was completed, and the MDQCC demonstrated similar psychometric properties to the original English MDQC. Therefore, the results supported that the MDQCC is eligible for assessing self-reported menstrual distress and is valid and reliable when applied to Chinese Mandarin-speaking women.
Supplemental Material
Download Zip (586.8 KB)Acknowledgments
We sincerely thank Professor Rudolf H. Moos for permitting us to translate the instrument. Furthermore, we thank all the experts and the participants in the study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Adawi, M., et al., 2018. Translation and validation of the nomophobia questionnaire in the Italian language: Exploratory factor analysis. JMIR mHealth and uHealth, 6 (1), 1.
- Akoglu, H., 2018. User’s guide to correlation coefficients. Turkish Journal of Emergency Medicine, 18 (3), 91–7.
- Anthoine, E., et al., 2014. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health and Quality of Life Outcomes, 12 (1), 2.
- Asgari, S., et al., 2020. The effect of psychoeducational intervention, based on a self-regulation model on menstrual distress in adolescents: a protocol of a randomized controlled trial. Trials, 21 (1), 747.
- Beykmirza, R., et al., 2022. Development and validation of an instrument to measure pediatric nurses’ adherence to ethical codes. BMC Medical Ethics, 23 (1), 14.
- Castellanos, I., Kronenberger, W.G. and Pisoni, D.B., 2018. Questionnaire-based assessment of executive functioning: Psychometrics. Applied Neuropsychology. Child, 7 (2), 93–109.
- Chang, A.M., Chau, J.P. and Holroyd, E., 1999. Translation of questionnaires and issues of equivalence. Journal of Advanced Nursing, 29 (2), 316–322.
- Choi, J.H., 2017. Effects of kinesio taping and hot packs on premenstrual syndrome in females. Journal of Physical Therapy Science, 29 (9), 1514–1517.
- Chou, Y.C., Lu, J.Z. and Pu, C.Y., 2009. Prevalence and severity of menstrual symptoms among institutionalised women with an intellectual disability. Journal of Intellectual & Developmental Disability, 34 (1), 36–44.
- Chung, M.H., et al., 2013. Selected neurophysiological, psychological, and behavioral influences on subjective sleep quality in nurses: a structure equation model. PLoS One, 8 (11), e79529.
- Comrey, A.L., 1988. Factor-analytic methods of scale development in personality and clinical psychology. Journal of Consulting and Clinical Psychology, 56 (5), 754–761.
- Demir, O., Sal, H. and Comba, C., 2021. Triangle of COVID, anxiety and menstrual cycle. Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology, 41 (8), 1257–1261.
- Ferries-Rowe, E., Corey, E. and Archer, J.S., 2020. Primary dysmenorrhea: Diagnosis and therapy. Obstetrics and Gynecology, 136 (5), 1047–1058.
- Freeman, E.W., 2003. Premenstrual syndrome and premenstrual dysphoric disorder: definitions and diagnosis. Psychoneuroendocrinology, 28 Suppl 3, 25–37.
- Hofmeister, S. and Bodden, S., 2016. Premenstrual syndrome and premenstrual dysphoric disorder. American Family Physician, 94 (3), 236–240. Epub 2016/08/02. PubMed PMID: 27479626
- Jones, P.S., et al., 2001. An adaptation of Brislin’s translation model for cross-cultural research. Nursing Research, 50 (5), 300–304.
- Kim, M.J., Baek, I.H. and Goo, B.O., 2016. The relationship between pelvic alignment and dysmenorrhea. Journal of Physical Therapy Science, 28 (3), 757–760.
- Koo, T.K. and Li, M. Y., 2016. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15 (2), 155–163.
- Lim, N., 2016. Cultural differences in emotion: differences in emotional arousal level between the East and the West. Integrative Medicine Research, 5 (2), 105–109.
- Lin, F.L., et al., 2017. Translation and psychometric testing of the Chinese version of the multidimensional assessment of interoceptive awareness. The Journal of Nursing Research: JNR, 25 (1), 76–84.
- Markum, R.A., 1976. Assessment of the reliability of and the effect of neutral instructions on the symptom ratings on the Moos Menstrual Distress Questionnaire. Psychosomatic Medicine, 38 (3), 163–172.
- Marmarà, D., Marmarà, V. and Hubbard, G., 2017. Maltese translation and adaptation of champion’s health belief model scale and the revised illness perception questionnaire for breast screening among Maltese women. Journal of Nursing Measurement, 25 (3), 486–503.
- Mohamadirizi, S. and Kordi, M., 2015. The relationship between food frequency and menstrual distress in high school females. Iranian Journal of Nursing and Midwifery Research, 20 (6), 689–693.
- Moos, R.H., 1968. The development of a menstrual distress questionnaire. Psychosomatic Medicine, 30 (6), 853–867. https://pubmed.ncbi.nlm.nih.gov/5749738/
- Moos, R.H., 2010. Menstrual distress questionnaire manual. Menlo Park, CA: Mind Garden, Inc.
- Mundfrom, D.J., Shaw, D.G. and Ke, T.L., 2005. Minimum sample size recommendations for conducting factor analyses. International Journal of Testing, 5 (2), 159–168.
- Nagata, C., et al., 2004. Soy, fat and other dietary factors in relation to premenstrual symptoms in Japanese women. BJOG: An International Journal of Obstetrics and Gynaecology, 111 (6), 594–599.
- Nguyen, A.M., et al., 2017. Psychometric validation of the dysmenorrhea daily diary (DysDD): a patient-reported outcome for dysmenorrhea. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 26 (8), 2041–2055.
- Nillni, Y.I., et al., 2013. The role of anxiety sensitivity in the experience of menstrual-related symptoms reported via daily diary. Psychiatry Research, 210 (2), 564–569.
- Peters, M. and Passchier, J., 2006. Translating instruments for cross-cultural studies in headache research. Headache, 46 (1), 82–91.
- Rawy, M., et al., 2021. Development and validation of a theory-based instrument to predict community pharmacists’ intention to provide pharmaceutical care services. Research in Social & Administrative Pharmacy: RSAP, 17 (4), 664–676.
- Reeve, S., et al., 2018. Insomnia, negative affect, and psychotic experiences: Modelling pathways over time in a clinical observational study. Psychiatry Research, 269, 673–680.
- Rodrigues, I.B., et al., 2017. Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMC Musculoskeletal Disorders, 18 (1), 540.
- Ross, C., Coleman, G. and Stojanovska, C., 2003. Factor structure of the modified Moos Menstrual Distress Questionnaire: assessment of prospectively reported follicular, menstrual and premenstrual symptomatology. Journal of Psychosomatic Obstetrics and Gynaecology, 24 (3), 163–174.
- Shirwaikar Thomas, A., Duran, A. and Abraham, B.P., 2020. Correlation of menstrual distress to severity of gastrointestinal symptoms in inflammatory bowel disease patients. Indian Journal of Gastroenterology: Official Journal of the Indian Society of Gastroenterology, 39 (5), 514–520.
- Sigmon, S.T., et al., 2000. The impact of anxiety sensitivity, bodily expectations, and cultural beliefs on menstrual symptom reporting: a test of the menstrual reactivity hypothesis. Journal of Anxiety Disorders, 14 (6), 615–633.
- Sun, Y., et al., 2018. Prevalence of abnormal uterine bleeding according to new International Federation of Gynecology and Obstetrics classification in Chinese women of reproductive age: A cross-sectional study. Medicine, 97 (31), e11457–e57.
- Taber, K.S., 2018. The use of cronbach’s alpha when developing and reporting research instruments in science education. Research in Science Education, 48 (6), 1273–1296.
- Thys-Jacobs, S., Alvir, J.M. and Fratarcangelo, P., 1995. Comparative analysis of three PMS assessment instruments--the identification of premenstrual syndrome with core symptoms. Psychopharmacology Bulletin, 31, 389–396. Epub 1995/01/01. PubMed PMID: 7491397
- Ueno, H.M., et al., 2016. Effects of a bovine lactoferrin formulation from cow’s milk on menstrual distress in volunteers: A randomized, crossover study. International Journal of Molecular Sciences, 17 (6), 845.
- Vambheim, S., et al., 2017. The fear of pain questionnaire-III and the fear of pain questionnaire-short form: a confirmatory factor analysis. Journal of Pain Research, 10, 1871–1878.
- van Griethuijsen, R.A.L.F., et al., 2015. Global patterns in students’ views of science and interest in science. Research in Science Education, 45 (4), 581–603.
- Wang, H., 1991. Study on the related factors of menstrual physilogical distress of junior and senior high schools of female students in Hsin-Chu city [M.S. thesis]. National Yang-Ming Medical College Institute of Public Health. 136.
- Wild, D., et al., 2005. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 8 (2), 94–104.
- Wong, J.J., Laframboise, M. and Mior, S., 2018. Multimodal therapy combining spinal manipulation, transcutaneous electrical nerve stimulation, and heat for primary dysmenorrhea: A prospective case study. Journal of Chiropractic Medicine, 17 (3), 190–197.
- Woods, N.F., Most, A. and Dery, G.K., 1982. Prevalene of perimenstrual symptoms. American Journal of Public Health, 72 (11), 1257–1264.
- Wu, S.F., 2006. A two-stage translation and test the validity and reliability of a foreign instrument. Hu Li Za Zhi, 53, 65–71.
- Yan, G., et al., 2006. The effect of word and character frequency on the eye movements of Chinese readers. British Journal of Psychology (London, England: 1953), 97 (Pt 2), 259–268.
- Yeh, M.L., 2002. Assessing the reliability and validity of the Chinese version of the California Critical Thinking Disposition Inventory. International Journal of Nursing Studies, 39 (2), 123–132.
- Yilmaz, S.K., Bohara, A.K. and Thapa, S., 2021. The stressor in adolescence of menstruation: coping strategies, emotional stress & impacts on school absences among young women in Nepal. International Journal of Environmental Research and Public Health, 18 (17), 8894.
- Yu, L., et al., 2020. Manual acupuncture versus sham acupuncture and usual care for the prevention of primary dysmenorrhea (PD): study protocol for a randomized controlled trial. Trials, 21 (1), 818.
- Zeugfang, D., et al., 2018. Translation and validation of the PACIC + questionnaire: the Thai version. BMC Family Practice, 19 (1), 123.