
ABSTRACT
To describe all health problems (injuries and illnesses) in relation to type, location, incidence, prevalence, time loss, severity, and burden, in competitive adolescent distance runners in England. Prospective observational study: 136 competitive adolescent distance runners (73 female athletes) self-reported all health problems for 24-weeks between May and October 2019. Athletes self-reported health problems using the Oslo Sports Trauma Research Centre Questionnaire on Health Problems. The incidence of running-related injury per 1,000 hours of exposure was markedly higher, compared to previous research. At any time, 24% [95% Confidence Intervals (CI): 21–26%] of athletes reported a health problem, with 11% [95% CI: 9–12%] having experienced a health problem that had substantial negative impact on training and performance. Female athletes reported noticeably more illnesses, compared to male athletes, including higher prevalence, incidence, time loss, and severity. The most burdensome health problems, irrespective of sex, included lower leg, knee, and foot/toes injuries, alongside upper respiratory illnesses. The mean weekly prevalence of time loss was relatively low, regardless of health problem type or sex. Competitive adolescent distance runners are likely to be training and competing whilst concurrently experiencing health problems. These findings will support the development of injury and illness prevention measures.
Introduction
Distance running is one of the most popular sports among children and adolescents around the world (Hulteen et al., Citation2017). In England, distance running has been reported to be the second most prevalent sport among adolescents (Sport England, Citation2019). Although distance running is associated with multiple health benefits in later life (Pedisic et al., Citation2019), adult-based research indicates that participation is also associated with negative health outcomes, such as injury (Van Gent et al., Citation2007). In adolescent distance runners, there is a lack of research that has investigated such outcomes (Steffen & Engebretsen, Citation2010). This population is often included as a sub-group within larger multi-sport samples of adolescent athletes (Carragher et al., Citation2019; Jacobsson et al., Citation2012; Moseid et al., Citation2018; Pierpoint et al., Citation2016; Von Rosen et al., Citation2017; Von Rosen et al., Citation2018), whereby sex differences have been investigated within a heterogeneous population rather than at sport-specific levels (Jacobsson et al., Citation2012; Moseid et al., Citation2018; Pierpoint et al., Citation2016; Von Rosen et al., Citation2018). Regardless, in those studies that include adolescent distance runners, the reported running-related injury (RRI) incidence ranges from 0.84 to 17.0 per 1,000 hours of exposure (Pierpoint et al., Citation2016; Rauh et al., Citation2006, Citation2000; Von Rosen et al., Citation2017; Von Rosen et al., Citation2018), and injury prevalence ranges from 15% to 32% (Carragher et al., Citation2019; Jacobsson et al., Citation2012; Moseid et al., Citation2018). While these studies used different methodologies, which may account for these differences (Tabben et al., Citation2020), data suggest that the most frequently injured anatomical body region is the lower limb, with the knee (Jacobsson et al., Citation2012; Von Rosen et al., Citation2017; Huxley et al., Citation2014), lower leg (Carragher et al., Citation2019; Huxley et al., Citation2014; Jacobsson et al., Citation2012; Von Rosen et al., Citation2017; Von Rosen et al., Citation2018), and ankle (Huxley et al., Citation2014; Jacobsson et al., Citation2012; Pierpoint et al., Citation2016; Rauh et al., Citation2006, Citation2000) being the most commonly affected body areas. However, due to small sample sizes and narrow age ranges, there is limited opportunity to generalise these findings to other distance running populations.
Another limitation of the existing distance running literature (adult and paediatric populations) is that numerous epidemiological studies use a time loss or medical attention injury definition, and often do not account for illness within their study design (Bahr et al., Citation2020). Therefore, these studies may have underestimated the total number of health problems (injuries and illnesses; Bahr et al., Citation2020; Clarsen & Bahr, Citation2014; Clarsen et al., Citation2013; Tabben et al., Citation2020), while ignoring the potential impact of illnesses. For example, injuries that do not result in time loss, and allow athletes to continue to participate regardless of the injury, may be missed. This “loss of detail” is exacerbated when studying adolescent athletes and not examining sex differences within sub-groups of broader sporting populations (i.e., focusing upon track and field athletes, instead of distance runners). This is an important consideration given that the growth and maturation of adolescent athletes differ according to sex (Bergeron et al., Citation2015; Wik et al., Citation2020). Therefore, any sex differences related to the burden of health problems, defined as the cross-product of severity and incidence (Bahr et al., Citation2018), may require further attention, with the possibility of developing sex- and event-specific injury and illness prevention measures.
The purpose of this study was to describe the prevalence, incidence, severity, and burden of health problems within a population of competitive adolescent distance runners in England, using a prospective cohort study design. Specifically, the study aimed to (1) describe all health problems in relation to type, location, incidence, prevalence, time loss, severity, and burden, and (2) describe sex differences related to these outcomes.
Methods
Study design
This was a 24-week prospective cohort study based on weekly completion of an online questionnaire. Data collection took place between May and October 2019. This timeframe was chosen to reflect the international and domestic outdoor track and field season (approx. April until September) and the start of the cross-country season (approx. October to March).
Participants
A total of 644 distance runners (athletes) from 210 England Athletics affiliated athletics clubs, aged between 13 and 18 years, were invited to participate in this study. These athletes were selected to take part based on achieving a Top-50 performance in their given age-group during 2018, according to the publicly available Power of 10 database, for all distance running events from 800 m up to 10,000 m, including the steeplechase (Power of 10, Citation2020). The Top-50 performances for each distance running event were collated according to the age-groups used in the Power of 10 database: 13–14 years (U15), 15–16 years (U17), and 17–19 years (U20). Data extracted from the Power of 10 database included: event ranking, performance time, name of athlete, year in age-group, name of coach, and name of athletics club. These data were not retained for analysis. Athletes that had achieved a Top-50 performance in their third year as a U20 were excluded due to being over the age of 18 years. Once exported, any duplicate data were identified (i.e., the same athlete achieving a Top 50 performance for multiple distance running events) and athletes were grouped according to their athletics club affiliation. Once collated, each athletics club was contacted by letter and email with study information and which athletes were eligible to take part. Each athletics club was actively encouraged to share this study information with eligible athletes, their coach, and guardians. If interested, these athletes were able to enrol onto the study by contacting the primary author (RM) via email or telephone. Athletes were excluded from the study if they were injured at the time of study enrolment, not aged between 13 and 18 years old, unable to fully understand the study procedure, and/or failed to complete the consent/assent forms and/or baseline questionnaire. Both consent and assent were obtained before an athlete completed the baseline questionnaire. A flow diagram of the recruitment process is presented in . Ethics approval was granted by the institutional ethics committee (180801/B/02).
Figure 1. Study flow chart illustrating participant recruitment, enrolment, and dropout. N.B. Due to the nature of data collection, it is not possible to confirm whether all 443 athletes received study information. Only the athletics clubs confirmed receipt of this information
Athletes provided data on a rolling basis. During the first 4 weeks, the sample size (n) increased by the following amount: 98 (week 1), 16 (week 2), 19 (week 3), and 3 (week 4). The final study sample consisted of 136 athletes (73 females). Regardless of the athletes’ given week of enrolment, data were collected up to week 24. In relation to internal validity, the sex split within this study sample was 54% female, compared with 46% male. Within the total available sample (n = 644), the sex split was 48% female, compared with 52% male.
Data collection procedures
Baseline questionnaire
Before starting weekly data collection, each athlete completed a baseline questionnaire via Qualtrics XM (Provo, Utah, USA), an online platform that is compatible with computers and mobile devices. The questionnaire included sections on background demographics (e.g., date of birth), performance history (e.g., event preferences), training practices (e.g., sessions per week), and medical information (e.g., injury history). This questionnaire was based on previous research (Huxley et al., Citation2014; Jacobsson et al., Citation2012; Woollings et al., Citation2015), and developed for a prior study (unpublished). Key stakeholders were involved in the development of this questionnaire to ensure that it was appropriate for the target audience (face validity). This included adolescent distance runners, parents, athletics coaches, and sports physiotherapists (n = 12). Please see supplementary material for a copy of this questionnaire.
Participant characteristics were calculated from these questionnaire responses. Chronological age (decimal age) was calculated, before being categorised according to age-group: 13–14 years (U15), 15–16 years (U17), and 17–18 years (U19). Training ages (i.e., number of years participating in distance running); stature (cm), body mass (kg), current performance level (i.e., club, county, regional, national, or international), and injury history were all self-reported. Each athlete’s age at peak height velocity (PHV) was determined by applying sex-specific maturity offset equations (Moore et al., Citation2015), and used to estimate maturity timing and tempo (Baxter-Jones et al., Citation2005).
Weekly data collection
Injury and illness data were collected using the Oslo Sports Trauma Research Centre questionnaire on health problems (OSTRC-H) (Clarsen et al., Citation2020, Citation2013, Citation2014). The questionnaire has demonstrated good validity and reliability in samples including runners (Clarsen et al., Citation2014). It consists of four questions about athlete participation in sport, training volume, sports performance, and symptoms of health problems during the previous 7 days (Clarsen et al., Citation2013). The response to each of these questions is given a value between 0 and 25, with 0 (minimum value) representing “no problems” and 25 (maximum value) representing “severe problems”. The four values were summed to calculate a severity score from 0 to 100 for each recorded health problem. If the athlete answered all four questions with the minimum value (full participation without health problems, no reduction in training volume or sports performance, and no symptoms), the OSTRC-H was completed for that week. If athletes reported a health problem, they were asked to self-report whether it was an injury or an illness. Athletes were asked to record the anatomical location of all reported injuries, and the main symptoms experienced for all reported illnesses. For all recorded health problems, athletes were asked to record the number of days of complete time loss from training and competition, whether the health problem had previously been recorded, and who the health problem had been reported to (i.e., nobody, medical doctor, or physiotherapist). Athletes were able to report multiple health problems per week. Alongside the OSTRC-H, athletes were also asked to self-report a weekly training diary, having been encouraged to record this throughout the week. Each weekly training diary allowed athletes to detail the type, total duration, distance covered, and rating of perceived exertion related to all of their running-related training sessions or competitions. Athletes also completed the adolescent version of the Profile of Mood States (Terry et al., Citation1999).
The OSTRC-H was sent to athletes on a weekly basis (every Sunday) by email from 5th May until 13 October 2019 (24 weeks) and was completed via Qualtrics XM. If athletes did not complete the questionnaire, email reminders were sent on the following day (Monday), after two days (Wednesday), and after four days (Friday). The athlete’s parents or legal guardians were copied into the email reminders after two and four days, respectively. If a response had still not been received after five days (Saturday), the principal investigator would send an SMS reminder to non-responders. If the questionnaire remained unanswered by the time the subsequent weekly questionnaire was distributed, the athlete was categorised as a “non-responder” for that specific week and recorded as missing data.
Definition and classification of health problems
Aligned with recent consensus statements (Bahr et al., Citation2020; Schwellnus et al., Citation2016; Soligard et al., Citation2016; Timpka et al., Citation2014), a “broad” definition of health problems was used, recording all health problems regardless of time loss and/or the need for medical attention. Health problems were classified as an injury if they affected the musculoskeletal system and were classified as an illness if they affected a specific organ system or represented general symptoms. Athletes did not classify injuries as having an acute or overuse mechanism. Instead, the primary author (RM) classified injury onset as gradual or sudden. Health problems were defined as “substantial” if they caused moderate or severe reductions in training volume, moderate or severe reductions in performance, or complete inability to participate in distance running, according to the OSTRC-H scoring guide (Clarsen et al., Citation2013, Citation2014). Health problems were classified as having caused time loss if the injury or illness led to the athlete being unable to participate fully in distance running training and competition the day after the incident occurred (Bahr et al., Citation2020; Timpka et al., Citation2014).
Prevalence calculations
The following prevalence measures were calculated on a weekly basis: all health problems, substantial health problems, time loss health problems, all injuries, substantial injuries, time loss injuries, all illnesses, substantial illnesses, and time loss illnesses. The mean prevalence and 95% confidence intervals (CI) were calculated for the entire study period and stratified by sex. To avoid potential overreporting of health problems, each athlete’s first week of data were excluded from analyses (Clarsen et al., Citation2013).
Incidence and relative burden of health problems
After reviewing each athlete’s questionnaire responses for the entire season, a list of cases was compiled that included the following details: type of health problem, body region and area (for injuries) or main organ system affected (for illnesses), number of weeks reported, cumulative time loss days, and cumulative severity score. To identify the main organ system affected for illnesses, the athletes’ self-reported symptoms were independently reviewed and classified by the first author and a medical doctor, using recommended categories (Bahr et al., Citation2020). Once classified, differences were discussed and the main affected organ system was subsequently agreed upon (percentage agreement = 89%). The severity of each case was also based on its cumulative time loss, reported as: none (0 days), slight (1 day), minimal (2–3 days), mild (4–7 days), moderately serious (8–28 days), serious (>28 days-6 months), or long term (>6 months) (Timpka et al., Citation2014). The incidence of each type of health problem was expressed as both the number of cases per athlete per year (52 weeks) and per 1,000 hours of exposure. Exposure was calculated from the weekly training diary data.
To reflect the relative burden of injuries and illnesses as a proportion of the total health burden, severity scores for each health problem were summed and divided by the cumulative severity score for all health problems (Bahr et al., Citation2018). A risk matrix was created based on the severity and incidence of health problems in all affected injury body areas and illness organ systems, stratified by sex.
Statistical analysis
For the participant characteristics, the statistical software SPSS (version 26.0; IBM., Chicago, USA) was used to calculate means and standard deviations (SD) for continuous variables. Also, solely in relation to participant characteristics, percentages (%) were calculated for categorical variables, while sex differences were analysed using independent samples t-tests for continuous variables and Chi-squared tests (X2) for categorical variables. Statistical significance was set at an alpha level of 0.05 and effect sizes (ES) for mean comparisons were described using Cohen’s thresholds (small = 0.2, medium = 0.5, large = 0.8; Cohen, Citation1992). For the incidence and prevalence data, the statistical software R was used (version 3.6.1; The R Foundation for Statistical Computing., Vienna, Austria). 95% confidence intervals reported for incidence and prevalence data were used to indirectly infer differences between male and female athletes.
Results
Response rate and participant characteristics
A total of 136 (73 female) adolescent distance runners participated in this study. Participant characteristics are shown in . Throughout the study, a total of 2969 questionnaires were distributed, and 2774 responses were received (mean weekly response rate, 91% (range: 85–99%)). During the follow-up period, 97 of the 136 (71%) athletes enrolled in the study completed every weekly questionnaire, while seven athletes dropped out of the study (). The data collected for these athletes until the time they dropped out were included in the analysis. Responses to the questionnaire were generally received on the Sunday (47%) or Monday (30%) and the median questionnaire completion time was 8 min.
Table 1. Participant characteristics (data presented as mean and SD, unless otherwise stated)
Number, incidence, and severity of health problems
In total, 136 athletes reported 213 injuries and 150 illnesses. This translated to 4.0 new injuries and 2.8 new illnesses/athlete/year. The incidence of all health problems (both sexes combined) was 42.6 per 1,000 hours (95% CI, 38.4–47.1). The mean time loss was 4 days/athlete/year (95% CI, 3–5 days), with a mean of five days for injuries (95% CI, 3–7 days) and three days for illnesses (95% CI, 2–4 days) ().
Table 2. Incidence, total time loss, and cumulative severity score of all health problems, all injuries, and all illnesses (split by sex)
The most frequent injury locations were the lower leg (27%), knee (19%), and foot/toes (13%). For illnesses, the most frequently affected organ systems were upper respiratory (65%), lower respiratory (11%), and non-specific illness (10%). The number and severity of injuries (body region and area) and illnesses (organ system) are summarised in . 61% of injuries had a gradual onset and 39% had a sudden onset. The most frequent injury locations for gradual onset injuries were the lower leg (38%), knee (17%), and thigh (13%). In comparison, the most frequent injury locations for sudden onset injuries were the knee (22%), foot/toes (20%), lower leg (11%), and ankle (11%).
Table 3. Severity of time loss of all health problems, all injuries (body region and area), and all illnesses (organ system)
Prevalence of health problems
The weekly mean prevalence of all health problems, substantial health problems, and time loss health problems are presented in . When compared to all health problems, the mean weekly prevalence was reduced for substantial health problems (approx. 50%), and again for time loss health problems (approx. 33%) across the sample.
Table 4. Weekly prevalence of all health problems, substantial health problems, and time loss health problems (in percentages)
Burden of health problems
Using the total number of time loss days as the basis for injury severity when calculating relative burden (), injuries represented 80% of the total burden of health problems, with illnesses representing 20%. This was 66% and 34% for female athletes, compared to 85% and 15% for male athletes, respectively. Using cumulative severity score as the basis for injury severity (), injuries represented 70% of the total burden of health problems, with illnesses representing 30%. This was 61% and 39%, and 82% and 18% for female and male athletes, respectively.
illustrates the relationship between severity and incidence for the five most commonly affected body areas (injuries) and organ systems (illnesses), stratified by sex, with supplementary data provided for all other health problems.
Figure 2. Risk matrices illustrating the relationship between severity (consequence) and incidence (likelihood) of all injuries (areas) and illnesses (systems) with three or more reported cases in a population of competitive adolescent distance runners, stratified by sex. The five most commonly affected health problems are labelled. Shading illustrates the relative importance of each health problem; the darker the colour, the greater the overall burden, and the greater the priority should be given to prevention. A supplementary file can be downloaded for access to original data, excluding means and 95% confidence intervals for health problems with less than three cases
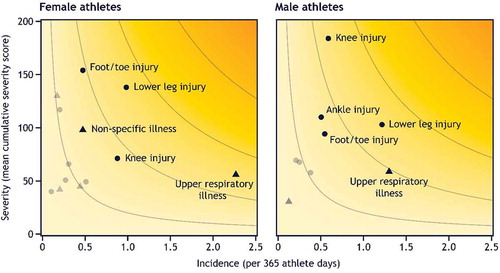
Regardless of sex differences, the body areas representing the highest burden of injuries were the lower leg, knee, and foot/toes. For affected organ systems, the highest burden of illnesses was caused by upper respiratory illness, non-specific illness, and lower respiratory illnesses.
Discussion
To the authors’ knowledge, this is the first study to record all injuries and illnesses, including those that did not result in time loss and/or medical attention, exclusively in a population of competitive adolescent distance runners. The key findings were that: (1) the incidence of RRI per 1,000 hours of exposure was markedly higher when compared to previous research; (2) at any time, 24% of athletes reported a health problem, with 11% having experienced a health problem that had substantial negative impact on training and performance; (3) female athletes reported noticeably more illnesses compared with male athletes, including higher prevalence, incidence, time loss, and severity; (4) the most burdensome health problems, regardless of sex, included lower leg, knee, and foot/toes injuries, alongside upper respiratory illnesses; and (5) the mean weekly prevalence of time loss was relatively low, regardless of health problem type or sex.
The first key finding was that the incidence of RRI per 1,000 hours of exposure was markedly higher when compared to previous research. For example, the reported RRI per 1,000 hours for all injuries, including male and female athletes, within this study (25.0) was higher than that reported in similar cohorts of adolescent endurance athletes (range: 4.0–13.1), when using a prospective study design (Rauh et al., Citation2000; Von Rosen et al., Citation2017; Von Rosen et al., Citation2018). These differences remain apparent when sex-specific analyses are made. The data from the present study are also higher than that previously reported in novice adult distance runners (Videbaek et al., Citation2015). Differences between the aforementioned studies may be explained by the fact that the present study included data from the outdoor Track and Field season, whereby athletes regularly reduced their training volume in order to perform to their best ability in races. Likewise, a period of rest (i.e., training break) was usually taken following athletes’ final track race of the season, before transitioning into the cross-country season. When combined, this highlights that the reported exposure may have been lower than if the study had captured data throughout an entire calendar year. Further to this, the use of a broad definition of recordable health problems, capturing “all health problems,” may inflate the reported incidence per 1,000 of exposure.
The mean weekly prevalence of all health problems reported within this study (24%) was lower than that reported in cohorts of adolescent endurance athletes (range: 32.7–38%), as part of sub-group analyses in studies that used similar methods (Carragher et al., Citation2019; Moseid et al., Citation2018). Likewise, the reported mean weekly prevalence of substantial health problems within this study (11%) was lower than that reported in comparable cohorts (range: 17.6–22%; Carragher et al., Citation2019; Moseid et al., Citation2018). These studies (Carragher et al., Citation2019; Moseid et al., Citation2018), as well as the current study, demonstrate a pattern that approximately half of all health problems are substantial. When only focussing on injuries, the mean weekly prevalence reported within this study (16%) is both similar to (range: 15–19.4%) (Moseid et al., Citation2018; Von Rosen et al., Citation2018), and lower than (range: 25.9–32.4%) (Carragher et al., Citation2019; Von Rosen et al., Citation2017), that reported in similar cohorts of adolescent endurance athletes. For illnesses, the mean weekly prevalence reported within this study (8%) is predominantly lower than that reported in the comparable studies (range: 14–23%) (Moseid et al., Citation2018; Von Rosen et al., Citation2017; Von Rosen et al., Citation2018), with the exception being a cohort of elite Irish adolescent endurance athletes (6.9%) (Carragher et al., Citation2019). Differences between these studies may be explained by the longer follow-up period (52-weeks) used in two of the studies (Von Rosen et al., Citation2017; Von Rosen et al., Citation2018), thus being representative of a full calendar year, in addition to the possibility that the smaller sample sizes (range: 25 to 76) used in these studies overestimate the prevalence of these health problems (Carragher et al., Citation2019; Moseid et al., Citation2018; Von Rosen et al., Citation2017; Von Rosen et al., Citation2018). The fundamental methodological differences between other studies make any further comparison difficult.
The third key finding was that female athletes reported more illnesses (109 illnesses, 73 participants), compared to male athletes (41 illnesses, 63 participants). They also reported more injuries (118 injuries, 73 participants) than male athletes (95 injuries, 63 participants) too, although this is a less noticeable difference compared to illnesses. In this study, this resulted in higher prevalence, incidence, time loss, and severity data relating to illnesses in female athletes. In the two available studies that report sex differences specific to adolescent distance runners (Carragher et al., Citation2019; Von Rosen et al., Citation2017), this pattern is consistent. However, in studies that combine sport sub-samples when analysing sex-differences (Moseid et al., Citation2018; Von Rosen et al., Citation2018), this pattern is not identified. Also, the difference between female and male athletes, in relation to weekly illness prevalence data (8%), is more pronounced in the present study, when compared to others (~3-4%) (Carragher et al., Citation2019; Von Rosen et al., Citation2017). Nonetheless, this identified sex difference in self-reported illness (and wider health problems) is consistent across general adolescent populations in Europe and North America (Torsheim et al., Citation2006), and elite adult athletes (Schwellnus et al., Citation2016). When trying to explain this sex difference, it is apparent that female athletes self-report upper and lower respiratory illnesses, and non-specific illnesses, more often than male athletes do. While the data related to respiratory illnesses are contrary to those sex differences reported in non-athletic populations, including adults and adolescents (Falagas et al., Citation2007), it does align with research in adult endurance athletes (He et al., Citation2014). In relation to non-specific illnesses, the higher number self-reported by female athletes is difficult to explain without aetiological information, derived from medical diagnoses. Therefore, future research should look to describe and analyse this sex difference according to specific diagnosis and aetiology (Bahr et al., Citation2020).
In relation to the burden of health problems (), results were similar regardless of sex. For example, the body region resulting in the greatest burden from injuries was the lower limb, with the greatest burden according to body area being to the lower leg, knee, and foot/toes. Although comparison to previous research is problematic, these reported body areas are largely consistent with previous adult- and adolescent-based research, irrespective of mode of onset (Jacobsson et al., Citation2012; Van Gent et al., Citation2007; Von Rosen et al., Citation2017 Huxley et al., Citation2014). When combined with the prevalence and incidence data, these results indicate that injury and illness prevention measures for competitive adolescent distance runners should focus on reducing the risk of these specific injuries. Also, as overuse is the usual mode of onset within distance running, any measures should attempt to address this problem. In relation to illnesses, the greatest burden was related to upper respiratory illnesses, in both male and female athletes. While this finding is consistent across the majority of sports (Walsh, Citation2018), the development of prevention measures within this population may also want to consider this illness system. When combined, these findings demonstrate that a holistic approach to injury and illness prevention is required, whereby a range of different prevention strategies may need to be applied.
As a pattern identified in the data, the mean weekly prevalence of time loss health problems, regardless of type or sex, was relatively low. For example, the mean weekly prevalence of all health problems was 24%, compared to 4% when employing a time loss definition. This means that a large proportion of self-reported health problems did not cause athletes to miss training and competition. Although this could be interpreted as a positive finding in relation to athlete availability, it also worryingly highlights that competitive adolescent distance runners are likely to be training and competing whilst also experiencing a health problem. The potentially adverse consequences of this practice are concerning, representing a “silent issue” in the sport that is largely overlooked by youth sport consensus statements (Bergeron et al., Citation2015; DiFiori et al., Citation2014; Mountjoy et al., Citation2015) and long-term athlete development models (Lloyd & Oliver, Citation2012). However, this finding may be aligned to the nature of endurance sports, whereby athletes are required to sustain consistent and monotonous training intensities, durations, and frequencies (Seiler, Citation2010), regardless of health problems. Therefore, the potentially negative consequences of training and competing when concurrently experiencing a health problem warrants further investigation, while improved access to medical support at the time of initial injury may act to limit this pattern.
Methodological considerations
Data collection was reliant on athlete self-report outcomes, without any dedicated support from medical professionals. Although this is normal for adolescent distance running in England, it means that recording specific diagnoses for injuries and illnesses was not possible (Bahr et al., Citation2020) and, as discussed elsewhere (Clarsen et al., Citation2013), using an “all health problems” definition can result in overreporting of minor and transient problems (i.e., non-specific symptoms). However, within a homogenous population of distance runners, it is more likely that differences in reporting introduce “random noise,” rather than systematic bias into the results, whereby some athletes may under-report and others may over-report. Nonetheless, to account for the potential issue of over-reporting, the “substantial health problems” definition provides additional information on the full impact of injuries and illnesses in this population of adolescent athletes. Also, injuries were not classified based on their mechanism (Bahr et al., Citation2020). However, based on previous studies (Carragher et al., Citation2019; DiFiori et al., Citation2014; Huxley et al., Citation2014; Jacobsson et al., Citation2012; Moseid et al., Citation2018; Pierpoint et al., Citation2016), and the nature of the sport, it is likely that most injuries in this population have a repetitive mechanism, irrespective of whether the onset was sudden or gradual.
An additional study limitation is the extent to which these findings are generalisable to more recreational adolescent distance runners and different periods of the calendar year. With the emphasis being on competitive athletes, future studies may wish to focus their attention on the wider population of distance runners, allowing for comparison to these data. Likewise, a longer follow-up period (i.e., one year) may better capture seasonal variations related to the incidence, prevalence, and burden of health problems within this population. As internal validity is a prerequisite for generalisability, (Rothman et al., Citation2008) it is also important to highlight that the proportionately low sample size (representing 22% of the total possible sample), coupled with the rolling enrolment of participants, may have unintentionally made the potential for bias greater. However, this form of baseline self-selection resulted in a group of highly motivated participants, evidenced by the high mean weekly response rate (91%) and small number of participants who dropped out of the study (n = 7). This can be upheld as a methodological strength of this study and, in turn, can be seen to decrease selection bias.
Practical implications
Future injury and illness prevention measures within this population should be aimed at reducing the risk of lower limb injuries, with an emphasis on the lower leg, knee, and foot/toes – supported by previous research (Huxley et al., Citation2014; Jacobsson et al., Citation2012; Von Rosen et al., Citation2017). The development of prevention measures should also consider how to address the possibility that adolescent distance runners are training and competing whilst concurrently experiencing health problems, including attempting to improve initial access to medical support. This is important to consider in relation to safeguarding the long-term health and wellbeing of these athletes, whereby excelling as an adolescent athlete is unlikely to be necessary for, nor a guarantee of, success as a senior athlete (Kearney & Hayes, Citation2018). An additional practical implication is that sex differences in the self-reporting of respiratory and non-specific illnesses should be incorporated into the debate surrounding youth athletic development (Bergeron et al., Citation2015), with further evidence required to explain this difference. Based on the findings of this study, future descriptive epidemiological studies including adolescent athletes should present data for male and female athletes separately.
From a methodological perspective, it is important to reiterate that the response rate during the study was high (91%), with a large proportion of athletes (71%) responding to every weekly questionnaire. Therefore, this study indicates that prospective self-report surveillance methods are feasible in this population, while the questionnaire distribution method can also be advocated for future studies. Finally, the application of the OSTRC-H questionnaire can be recommended, based on its simplicity and capacity to record all health problems (Clarsen et al., Citation2013, Citation2014). However, future studies should adopt the updated questionnaire (Clarsen et al., Citation2020) include medical diagnoses, and, where appropriate, extend the length of follow-up.
Perspectives
This study provides an important insight into the extent of health problems within a population of competitive adolescent distance runners. The incidence of RRI per 1,000 hours of exposure was markedly higher when compared to previous research. At any time throughout the follow-up period, 24% of athletes had a health problem, with 11% having a substantial problem with a negative impact on their training and performance. Regardless of sex, lower leg, knee, and foot/toes injuries were the most burdensome health problems, alongside upper respiratory illnesses, which were a particular problem for female athletes. This study also shows that competitive adolescent distance runners are likely to be training and competing whilst concurrently experiencing health problems, whereby initial access to medical support needs to be improved. Therefore, appropriate management strategies for athletes and coaches should be developed (i.e., return-to-play decision making) for when health problems do occur. These data also support the development of holistic injury and illness prevention measures, that should aim to safeguard the long-term health and wellbeing of competitive adolescent distance runners.
Supplemental Material
Download PDF (152.4 KB)Supplemental Material
Download PDF (86.4 KB)Acknowledgement
The authors acknowledge the athletics clubs, coaches, and athletes who made this research possible. Daniel Razey is acknowledged for supporting with participant recruitment.
Disclosure statement
No competing interests (financial or otherwise) declared.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Supplementary material
Supplemental data for this article can be accessed online https://doi.org/10.1080/02640414.2021.1874160.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Bahr, R., Clarsen, B., Derman, W., Dvorak, J., Emery, C. A., Finch, C. F., Hägglund, M., Junge, A., Kemp, S., Khan, K. M., Marshall, S. W., Meeuwisse, W., Mountjoy, M., Orchard, J. W., Pluim, B., Quarrie, K. L., Reider, B., Schwellnus, M., Soligard, T., Stokes, K. A., & Chamari, K. (2020). International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). British Journal of Sports Medicine, 54(7), 372–389. https://doi.org/10.1136/bjsports-2019-101969
- Bahr, R., Clarsen, B., & Ekstrand, J. (2018). Why we should focus on the burden of injuries and illnesses, not just their incidence. British Journal of Sports Medicine, 52(16), 1018–1021. https://doi.org/10.1136/bjsports-2017-098160
- Baxter-Jones, A. D. G., Eisenmann, J. C., & Sherar, L. B. (2005). Controlling for maturation in pediatric exercise science. Pediatric Exercise Science, 17(1), 18–30. https://doi.org/10.1123/pes.17.1.18
- Bergeron, M. F., Mountjoy, M., Armstrong, N., Chia, M., Côté, J., Emery, C. A., ... Engebretsen, L.. (2015). International Olympic Committee consensus statement on youth athletic development. British Journal of Sports Medicine, 49(13), 843–851. https://doi.org/10.1136/bjsports-2015-094962
- Carragher, P., Rankin, A., & Edouard, P. (2019). A one-season prospective study of illnesses, acute, and overuse injuries in elite youth and junior Track and Field athletes. Frontiers in Sports and Active Living, 1(13). https://doi.org/10.3389/fspor.2019.00013
- Clarsen, B., & Bahr, R. (2014). Matching the choice of injury/illness definition to study setting, purpose and design: One size does not fit all! British Journal of Sports Medicine, 48(7), 510–512. [published Online First: 2014/03/13]. https://doi.org/10.1136/bjsports-2013-093297
- Clarsen, B., Bahr, R., Myklebust, G., Andersson, S. H., Docking, S. I., Drew, M., Finch, C. F., Fortington, L. V., Harøy, J., Khan, K. M., Moreau, B., Moore, I. S., Møller, M., Nabhan, D., Nielsen, R. O., Pasanen, K., Schwellnus, M., Soligard, T., & Verhagen, E. (2020). Improved reporting of overuse injuries and health problems in sport: An update of the Oslo Sport Trauma Research Center questionnaires. British Journal of Sports Medicine, 54(7), 390–396. https://doi.org/10.1136/bjsports-2019-101337
- Clarsen, B., Myklebust, G., & Bahr, R. (2013). Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. British Journal of Sports Medicine, 47(8), 495–502. [published Online First: 2012/10/06]. https://doi.org/10.1136/bjsports-2012-091524
- Clarsen, B., Ronsen, O., Myklebust, G., Flørenes, T. W., & Bahr, R. (2014). The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. British Journal of Sports Medicine, 48(9), 754–760. [published Online First: 2013/02/23]. https://doi.org/10.1136/bjsports-2012-092087
- Cohen, J. (1992). A power primer. Psychological Bulletin Journal, 112(1), 155–159. [published Online First: 1992/07/01]. https://doi.org/10.1037//0033-2909.112.1.155
- DiFiori, J. P., Benjamin, H. J., Brenner, J. S., Gregory, A., Jayanthi, N., Landry, G. L., & Luke, A. (2014). Overuse injuries and burnout in youth sports: A position statement from the American Medical Society for Sports Medicine. British Journal of Sports Medicine, 48(4), 287–288. https://doi.org/10.1136/bjsports-2013-093299
- Falagas, M. E., Mourtzoukou, E. G., & Vardakas, K. Z. (2007). Sex differences in the incidence and severity of respiratory tract infections. Respiratory Medicine, 101(9), 1845–1863. [published Online First: 2007/06/05]. https://doi.org/10.1016/j.rmed.2007.04.011
- He, C. S., Bishop, N. C., Handzlik, M. K., Muhamad, A. S., & Gleeson, M. (2014). Sex differences in upper respiratory symptoms prevalence and oral-respiratory mucosal immunity in endurance athletes. Exercise Immunology Review, 20, 8–22. [published Online First: 2014/07/01].
- Hulteen, R. M., Smith, J. J., Morgan, P. J., Barnett, L. M., Hallal, P. C., Colyvas, K., & Lubans, D. R. (2017). Global participation in sport and leisure-time physical activities: A systematic review and meta-analysis. Preventive Medicine, 95, 14–25. https://doi.org/10.1016/j.ypmed.2016.11.027
- Huxley, D. J., O’Connor, D., & Healey, P. A. (2014). An examination of the training profiles and injuries in elite youth track and field athletes. European Journal of Sport Science, 14(2), 185–192. [published Online First: 2013/06/20]. https://doi.org/10.1080/17461391.2013.809153
- Jacobsson, J., Timpka, T., Kowalski, J., Nilsson, S., Ekberg, J., & Renström, P. (2012). Prevalence of musculoskeletal injuries in Swedish elite track and field athletes. American Journal of Sports Medicine, 40(1), 163–169. [published Online First: 2011/11/05]. https://doi.org/10.1177/0363546511425467
- Kearney, P. E., & Hayes, P. R. (2018). Excelling at youth level in competitive track and field athletics is not a prerequisite for later success. Journal of Sport Sciences, 36(21), 2502–2509. https://doi.org/10.1080/02640414.2018.1465724
- Lloyd, R. S., & Oliver, J. L. (2012). The youth physical development model: A new approach to long-term athletic development. Strength and Conditioning Journal, 34(3), 61–72. https://doi.org/10.1519/SSC.0b013e31825760ea
- Moore, S. A., McKay, H. A., Macdonald, H., Nettlefold, L., Baxter-Jones, A. D. G., Cameron, N., & Brasher, P. M. A. (2015). Enhancing a somatic maturity prediction model. Medicine and Science in Sports and Exercise, 47(8), 1755–1764. [published Online First: 2014/11/26]. https://doi.org/10.1249/mss.0000000000000588
- Moseid, C. H., Myklebust, G., Fagerland, M. W., Clarsen, B., & Bahr, R. (2018). The prevalence and severity of health problems in youth elite sports: A 6-month prospective cohort study of 320 athletes. Scandinavian Journal of Medicine & Science in Sports, 28(4), 1412–1423. https://doi.org/10.1111/sms.13047
- Mountjoy, M., Rhind, D. J. A., Tiivas, A., & Leglise, M. (2015). Safeguarding the child athlete in sport: A review, a framework and recommendations for the IOC youth athlete development model. British Journal of Sports Medicine, 49(13), 883–886. https://doi.org/10.1136/bjsports-2015-094619
- Pedisic, Z., Shrestha, N., Kovalchik, S., Stamatakis, E., Liangruenrom, N., Grgic, J., Titze, S., Biddle, S. J., Bauman, A. E., & Oja, P. (2019). Is running associated with a lower risk of all-cause, cardiovascular and cancer mortality, and is the more the better? A systematic review and meta-analysis. British Journal of Sports Medicine, 54(15), 898–905. https://doi.org/10.1136/bjsports-2018-100493
- Pierpoint, L. A., Williams, C. M., Fields, S. K., & Comstock, R. D. (2016). Epidemiology of injuries in United States High School track and field: 2008-2009 through 2013-2014. American Journal of Sports Medicine, 44(6), 1463–1468. [published Online First: 2016/02/28]. https://doi.org/10.1177/0363546516629950
- Power of 10. (2020). Power of 10: Rankings https://www.thepowerof10.info/rankings/2020
- Rauh, M. J., Koepsell, T. D., Rivara, F. P., Margherita, A. J., & Rice, S. G. (2006). Epidemiology of musculoskeletal injuries among high school cross-country runners. American Journal of Epidemiology, 163(2), 151–159. [published Online First: 2005/11/25]. https://doi.org/10.1093/aje/kwj022
- Rauh, M. J., Margherita, A. J., Rice, S. G., Koepsell, T. D., & Rivara, F. P. (2000). High school cross country running injuries: A longitudinal study. Clinical Journal of Sport Medicine, 10(2), 110–116. [published Online First: 2000/05/08]. https://doi.org/10.1097/00042752-200004000-00005
- Rothman, K. J., Greenland, S., & Lash, T. L. (2008). Validity in epidemiological studies. In K. J. Rothman, S. Greenland, & T. L. Lash (Eds.), Modern epidemiology (3rd ed., pp. 128–147). Lippincott Williams & Wilkins.
- Schwellnus, M., Soligard, T., Alonso, J. M., Bahr, R., Clarsen, B., Dijkstra, H. P., Gabbett, T. J., Gleeson, M., Hägglund, M., Hutchinson, M. R., Janse Van Rensburg, C., Meeusen, R., Orchard, J. W., Pluim, B. M., Raftery, M., Budgett, R., & Engebretsen, L. (2016). How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. British Journal of Sports Medicine, 50(17), 1043–1052. [published Online First: 2016/08/19]. https://doi.org/10.1136/bjsports-2016-096572
- Seiler, S. (2010). What is best practice for training intensity and duration distribution in endurance athletes? International Journal of Sports Physiology and Performance, 5(3), 276–291. [published Online First: 2010/09/24]. https://doi.org/10.1123/ijspp.5.3.276
- Soligard, T., Schwellnus, M., Alonso, J. M., Bahr, R., Clarsen, B., Dijkstra, H. P., Gabbett, T., Gleeson, M., Hägglund, M., Hutchinson, M. R., Janse van Rensburg, C., Khan, K. M., Meeusen, R., Orchard, J. W., Pluim, B. M., Raftery, M., Budgett, R., & Engebretsen, L. (2016). How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. British Journal of Sports Medicine, 50(17), 1030–1041. [published Online First: 2016/08/19]. https://doi.org/10.1136/bjsports-2016-096581
- Sport England. (2019). Active Lives Survey Data Tables London. https://www.sportengland.org/know-your-audience/data/active-lives/active-lives-data-tables#children_and_young_people_surveys2020
- Steffen, K., & Engebretsen, L. (2010). More data needed on injury risk among young elite athletes. British Journal of Sports Medicine, 44(7), 485–489. https://doi.org/10.1136/bjsm.2010.073833
- Tabben, M., Whiteley, R., Wik, E., Bahr, R., & Chamari, K. (2020). Methods may matter in injury surveillance: “How” may be more important than “what, when or why”. Biology of Sport, 37(1), 3–5. https://doi.org/10.5114/biolsport.2020.89935
- Terry, P. C., Lane, A. M., Lane, H. J., & Keohane, L. (1999). Development and validation of a mood measure for adolescents. Journal of Sports Sciences, 17(11), 861–872. https://doi.org/10.1080/026404199365425
- Timpka, T., Alonso, J. M., Jacobsson, J., Junge, A., Branco, P., Clarsen, B., Kowalski, J., Mountjoy, M., Nilsson, S., Pluim, B., Renström, P., Rønsen, O., Steffen, K., & Edouard, P. (2014). Injury and illness definitions and data collection procedures for use in epidemiological studies in Athletics (track and field): Consensus statement. British Journal of Sports Medicine, 48(7), 483–490. [published Online First: 2014/03/13]. https://doi.org/10.1136/bjsports-2013-093241
- Torsheim, T., Ravens-Sieberer, U., Hetland, J., Välimaa, R., Danielson, M., & Overpeck, M. (2006). Cross-national variation of gender differences in adolescent subjective health in Europe and North America. Social Science & Medicine, 62(4), 815–827. https://doi.org/10.1016/j.socscimed.2005.06.047
- Van Gent, R. N., Siem, D., Van Middelkoop, M., van Os, A. G., Bierma-Zeinstra, S. M. A., Koes, B. W., & Taunton, J. E. (2007). Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. British Journal of Sports Medicine, 41(8), 469–480. https://doi.org/10.1136/bjsm.2006.033548
- Videbaek, S., Bueno, A. M., Nielsen, R. O., & Rasmussen, S. (2015). Incidence of running-related injuries per 1000 h of running in different types of runners: A systematic review and meta-analysis. Sports Medicine, 45(7), 1017–1026. [published Online First: 2015/05/09]. https://doi.org/10.1007/s40279-015-0333-8
- von Rosen, P., Floström, F., Frohm, A., & Heijne, A. (2017). Injury patterns in adolescent elite endurance athletes participating in running, orienteering, and cross-country skiing. International Journal of Sports Physical Therapy, 12(5), 822–832. https://doi.org/10.26603/ijspt20170822
- Von Rosen, P., Heijne, A., Frohm, A., Fridén, C., & Kottorp, A. (2018). High injury burden in elite adolescent athletes: A 52-week prospective study. Journal of Athletic Training, 53(3), 262–270. https://doi.org/10.4085/1062-6050-251-16
- Walsh, N. P. (2018). Recommendations to maintain immune health in athletes. European Journal of Sport Science, 18(6), 820–831. https://doi.org/10.1080/17461391.2018.1449895
- Wik, E. H., Martinez-Silvan, D., Farooq, A., Cardinale, M., Johnson, A., & Bahr, R. (2020). Skeletal maturation and growth rates are related to bone and growth plate injuries in adolescent athletics. Scandinavian Journal of Medicine & Science in Sports, 30(5), 894–903. [published Online First: 2020/02/09]. https://doi.org/10.1111/sms.13635
- Woollings, K. Y., McKay, C. D., Kang, J., Meeuwisse, W. H., & Emery, C. A. (2015). Incidence, mechanism and risk factors for injury in youth rock climbers. British Journal of Sports Medicine, 49(1), 44–50. [published Online First: 2014/11/12]. https://doi.org/10.1136/bjsports-2014-094067