
ABSTRACT
The purpose of para sport classification systems is to minimize the impact of impairment on competition outcome. Currently, athletes with intellectual impairment (II) compete in one class, regardless of the extent of activity limitation resulting from their impairment. Consequently, athletes with II that cause relatively minor difficulty in sport have a competitive advantage over athletes who have intellectual impairments that cause more significant advantage. This research investigated the efficacy of a measure of health-related functional impairment, derived from the World Health Organization International Classification of Functioning, Disability, and Health (ICF), as a tool to classify athletes with intellectual impairments (II) into groups with impairments that cause similar activity limitation. The first study used a Delphi technique to identify the most relevant codes within the ICF from which a measure of impairment presence and severity was derived. The second study investigated whether the measure could discriminate between groups of II athletes organized into three competition groups, and whether these groups could be predicted by ICF score. The ICF-based questionnaire shows promise as a conceptual approach and as a tool in this context, but this is a preliminary step before establishing a sport-specific approach to classification.
Introduction
Athletes with intellectual impairments (II) compete in only one class within the three sports of swimming, athletics and table tennis currently included in Paralympic competition. Eligible impairment criteria concerns establishing that the athlete has the eligible impairment, in this case II. This is the first step in Paralympic classification and is managed by Virtus World Intellectual Impairment Sport (previously INAS). Virtus holds the status of an International Organization of Sports for the Disabled (IOSD), one of four such independent organizations recognized by the International Paralympics Committee (IPC). As well as managing eligible impairment criteria processes Virtus organizes and promotes competitions within 16 sports through a network of five regions and 86 member nations. Since 2009 Virtus has had a rigorous system to ensure that athletes meet the diagnostic criteria of II. This system is endorsed by the IPC and once an athlete appears on the Virtus master list they are deemed as meeting the eligible impairment criteria for IPC competition. The definition of II adopted by both Virtus and the IPC is that of the World Health Organization (WHO) International Classification of Diseases, version 10 (ICD-10; World Health Organisation, Citation2016)Footnote1 which requires that athletes “have a restriction in intellectual functioning and adaptive behaviour which affects the conceptual, social and practical adaptive skills required for everyday life. This impairment must be present before the age of 18.” (p6 IPC International Standard for Eligible Impairments, 2016). Intellectual functioning is measured by a formal assessment of IQ, and adaptive behaviour is measured either by clinical observation or completion of a culturally appropriate assessment. The age restriction is to ensure that impairment has occurred during the developmental period and to distinguish between other conditions, such as acquired brain injury later in life.
Once an athlete has been deemed, via Virtus, to meet the eligible impairment criteria a second step is required to compete in IPC sanctioned events, this is to establish that the athlete’s eligible impairment “meets the minimum disability criteria of the sport” (IPC Athlete Classification Code, Citation2015). This process is managed by the International Sport Federation for each sport and is required to be an evidence-based system consistent with the conceptual model underpinning the IPC approach to classification (Tweedy & Vanlandewijck, Citation2011). These IPC classification procedures for II athletes in the three included sports are now well evidenced and described (e.g., Van Biesen et al., Citation2016, Citation2014) and the conceptual approach is described in the paper by Van Biesen et al. (Citation2021) in this volume. The third step within classification is to categorize an athlete into a sports class which describes the athlete’s limitations most accurately. This is to ensure that athletes are competing against each other fairly, with similar levels of activity limitation. Within Physical Impairment (PI) classification a sport may have multiple classes representing the level of functional activity limitation, for example, 10 classes in swimming (S1-S10), and likewise for Visual Impairment (VI), which has three classes, (S11-S13). However, within II there is currently only one sports class in all the three included sports, swimming (S14), athletics (T/F20) and table tennis (TT11).
The reasons for this are multifactorial and include the need to grow competition to ensure there is enough high-level competition to fill more than one class, the practical and financial constraints of running multiple classes in qualifying and international events, and importantly, the current lack of any system to classify athletes with II into distinct classes which is evidence based and is consistent with the IPC conceptual approach. However, that there is only one class for II does represent an equality and inclusion issue, and unless there are additional competition classes it is unlikely that competition will grow. In 2016 the Virtus general assembly passed a motion to grow II sport by developing additional competition classes within Virtus events. To enable this a research project was established to investigate what an evidenced-based classification system to categorize levels of activity limitation in athletes with II would look like. This paper sets out the Virtus conceptual approach and initial findings of this project.
It is acknowledged that whilst keeping broadly to IPC-based principles this is a Virtus-based approach, with the purposes of including a more representative range of athletes with II in Virtus competitions, to test the ICF conceptual approach, and grow this competition group. This will facilitate further research and refinement of the approach, which would be required before being applicable within the context of IPC classification. As such this might be described as a staged approach to facilitating athletes with a greater range of impairment severity to compete within Virtus, which will not only expand the opportunities available for II athletes, but will also provide a pool of competitors to facilitate further research to develop IPC compatible sport-specific classification systems. Such a class, called within Virtus II2, differs from the IPC approach in that at this stage it would be a unified class across sports, but as competition and research develops a more sports-specific approach is anticipated. As Tweedy has previously suggested that a unified approach to classification could be implemented through the application of the International Classification of Functioning, Disability, and Health (ICF: World Health Organization, Citation2001) framework, taking this approach within this context appears an appropriate conceptual starting position (Tweedy, Citation2002). Furthermore, common to the context of both Virtus and the IPC is the need for a sports classification system to have a clear conceptual framework, a “sound scientific and taxonomic basis” and be “articulated using language and definitions that are unambiguous and internationally recognized.” (Tweedy, Citation2002).
Taxonomy and II
Statistically around 0.05 to 1.55% of the world’s population have II (McKenzie et al., Citation2016). This differs across countries, dependent upon factors such as poverty and education, but generally it represents one of the largest types of disability grouping (World Health Organisation, Citation2011). As such it is unsurprising that within this group there is significant variation in causation, level and types of impairment and ultimately functional capacity. The challenge is to have a taxonomy of II that represents this diversity. One approach, adopted by the ICD-10 (World Health Organisation, Citation2004) and the Diagnostic and Statistical Manual for Mental Disorders (DSM; American Psychiatric Association, Citation2015) (the two most commonly used taxonomic frameworks in this area) is by differentiating functioning in terms of level of IQ. Four categories are usually described: mild (IQ 50–69), moderate (IQ 35–49) severe (IQ 20–34) and profound (IQ <20). This approach has been much criticized on several fronts, including; IQ being just one element of II diagnosis; reliability of measures, especially with more severe impairments; and overall IQ scores being a flawed concept (Bertelli et al., Citation2018; Whitaker, Citation2015).
Many studies demonstrate the independence of specific cognitive functions from a single, global IQ score (Johnson et al., Citation2008). Indeed, this has been demonstrated in the development of the sport-specific classification process in II, where not only has there been shown to be a lack of correlation between overall IQ score and sports performance, but that specific types of cognitive skill are implicated in performance (Gilderthorp et al., Citation2018; Van Biesen et al., Citation2016). Recent revisions of DSM-5 and ICD-11 have recognized this problem and both suggest that IQ profiles based on neuropsychological testing across a range of domains are more useful than a single IQ score.
A second serious criticism to this approach concerns the level of multi-morbidity in the population of II. In a recent large cohort study (n = 1,023) it was found that 99.2% of the sample had at least one additional physical health condition, as defined using the International Statistical Classification of Diseases and Related Health Problems, 10th revision (World Health Organisation, Citation2016) and 98.7% had two or more conditions. In addition, the average number of additional health conditions measured was 11, the highest number being 28 (Kinnear et al., Citation2018). Hence, multi-morbidity is the norm within II, not the exception, and is present across the lifespan, unlike the general population where it increases over the age of 50 (Kinnear et al., Citation2018). Many of the most common conditions found in Kinnear et al.’s (Citation2018) study would have a significant impact upon functionality, and specifically sports performance, for example, musculoskeletal (incidence 48.2%), circulatory (28.7%) and respiratory (27.9%) problems. Given that II includes many sub-populations with specific syndromes which contain a constellation of intellectual, sensory and physical health deficits (e.g., Down Syndrome, Fragile X), such multi-morbidity should not be a surprise. For those without a specific genetic causation, that trauma to the central nervous system, no matter what the aetiology, has a wider impact than just cognitively also makes logical sense. However, what is perhaps not as well acknowledged is the extent of this multi-morbidity, and consequently the need to consider the reciprocal nature of these conditions during development. It is recognized within the research literature that multiple deficits will have an additive, iterative and cumulative impact upon the overall functioning of the individual (Karmiloff-Smith, Citation2009, Citation2018). Hence, the limitations an adult with II faces are not just a product of cognitive deficits, but a product of the iterative combination of intellectual, sensory and physical deficits over the developmental period. Indeed, the concept of “intellectual impairment” as previously envisaged is coming under increasing criticism (Misheva, Citation2018; Nakken & Vlaskamp, Citation2007).
A reading of the complex area of taxonomy within II, together with the clear disconnection between unitary measures of IQ and sports performance, makes it clear that a simple approach to sports classification of assuming a causal, linear relationship between IQ and sport performance (i.e. classes based on IQ cut-off points) is flawed and inoperable. A more holistic approach is required which considers the composite of factors which may lead to limited functional capacity.
Conceptual approach
Consistent with sports classification, corresponding calls within educational and clinical contexts have been made to make greater use of the international and comprehensive nature of the ICF taxonomy when trying to characterize individuals with II (Simeonsson, Citation2009; Vale et al., Citation2017). Given that the ICF taxonomy fits conceptually with sports classification and the growing awareness of the complexities of assessment in II, in addition to the resources being freely available, downloadable, recognized internationally and available in several languages, the ICF framework was adopted as the underpinning model to develop further competition classes within the Virtus research programme.
As an initial exploration of this conceptual approach a previous study in the Virtus research programme used the ICF checklist with different groups of II athletes to investigate the relationship between IQ and functional impairment in athletes with II (Gilderthorp et al., Citation2018). The ICF checklist is a short, generic measure recording both presence of the impairment and severity in terms of impact on functioning (World Health Organisation, Citation2003). The finding that IQ was not related to sporting performance found in previous studies (Van Biesen et al., Citation2016) was replicated. The study also replicated that, even within an II population engaged in sporting activity, the number of additional health impairments present was related to IQ, such that the lower the IQ the higher the number of comorbid conditions (Kinnear et al., Citation2018). However, the ICF checklist lacks sensitivity, considers only broad level domains and does not include many of the health conditions experienced by people with II. A more sensitive instrument is required to meet the requirements of Virtus sport classification. Fortunately, the ICF taxonomy offers this opportunity by being able to select from the 1,400 ICF codes those most relevant to describe the condition under investigation.
Aims and hypotheses
The Gilderthorp et al. (Citation2018) study provided “proof of concept” suggesting this ICF-based approach has merit and further work was justified. Hence the aim of the research reported here was to refine the approach to measuring global functional impairment using a wider selection of ICF codes and further explore the relationships between impairment, IQ and competition groups, related to levels of performance. The full ICF taxonomy is available in eight different languages and allows relevant codes, up to four levels of specificity, to be downloaded into a bespoke questionnaire, more nuanced to the impairments relevant to II. Impairments are coded as present or not, but importantly the degree to which it is perceived they impact on functioning (severity) is also recorded. The Delphi study reported here focussed on selection of the most appropriate codes to form an ICF questionnaire, which will measure the presence and severity of the most common health conditions experienced by people with II, for use as a possible tool in Virtus classification.
It is estimated that 20% of the ICF codes will explain 80% of the variance observed in practice, and for this reason “core sets” have been developed (Ustun et al., Citation2004). Core sets are a group of codes which have gone through a rigorous, testing and selection process to be able to efficiently describe an individual’s level of functioning within a specific health condition e.g., stroke, spinal cord injury. However, currently there is no core set which refers specifically to II, hence we needed to select from the 1,400 codes the most relevant to describe this group. A Delphi approach was taken as it uses an expert panel to identify fundamental elements of a phenomenon, through a process of consensus agreement (Brady, Citation2015).
Athletes with II are likely to lie on a continuum, with at one end the Virtus athletes, performing at the highest standard and at the lower end those with the greatest physical impairment demonstrating significantly lower performance. Below Virtus athletes will be athletes with Down Syndrome (DS) who will also be spread along this continuum, but at a lower range than Virtus athletes. The aim of study two was to field test the devised ICF questionnaire and examine if it was able to discriminate between three groups of athletes: Virtus athletes, presumed to be performing at the highest level and hypothesized to have the least additional health impairments; DS athletes, presumed to be competing at the lowest level and hypothesized to have the most additional health impairments; and a group of athletes competing at regional level, hypothesized to fall between the other two groups.
Athletes with DS very rarely compete in the original II class at Virtus events, their world record times are lower across a range of events and they are known to have a range of comorbid health conditions likely to affect athletic performance, such as respiratory and muscular limitations. Given that 15–20% of all people with II have DS, it makes sense that in this first step of developing a second competition class Virtus wants to make sure it includes athletes with DS. However, a measure of equivalence is required to include other athletes with a similar level of functional impairment into this class, such that it is a class for those with more significant impairment, who can compete at a similar level, and not be based on medical diagnosis. To examine this a third comparative group was selected who do not have DS, who train and compete, but not at the international level. It was considered that this group would have the differing levels of impairment ranging from within the range of Virtus athletes to overlapping with the DS group. However, it might not be expected that their impairment level would be worse than those with DS, as DS carries with it significant associated health conditions. These three groups are named respectively Virtus, Regional and DS with regard to their competition grouping and presumed sports performance level. If found to have discriminant validity the questionnaire will be used in further research examining ICF scores in relation to sporting performance, and to investigate if cut-off scores can be used reliably as a component of Virtus competition classification.
Due to their highly interlinked nature, two studies are reported in this paper. The first was a Delphi study to determine the choice of items to include in the bespoke ICF questionnaire, the second was to field test this questionnaire, to establish its sensitivity and discriminant validity, and address the following hypotheses:
1. The hierarchy of competition grouping would be replicated in relation to levels of impairment, such that athletes in the Virtus group would have relatively low level of impairment, compared to the Regional and DS groups, and the DS group have the highest level of impairment.
2. ICF scores would be a better predictor of group membership than IQ.
Materials and methods
Study 1- Delphi study to select relevant ICF codes
Participants
The inclusion criteria for the expert panel were: experience of caring for, or working with people with II (preferably athletes); good spoken and written English; and experience across the three groups of athletes included in study 2. Thirteen people were approached via email to complete the questionnaire, and eleven responded (), representing six different nations. These were people known through Virtus, the Special Olympics and research networks.
Table 1. Details of the expert panel
Measures
To gather feedback from the expert panel, an online questionnaire was developed using Qualtrics (version January 2017). The 114 level 1 Body Functions categories in the ICF were reviewed and reduced to 31 selected from the research literature as most relevant (those most likely to have an impact on athletic performance) for athletes with II. This excluded categories under: voice and speech functions; genitourinary and reproductive functions; and functions of the skin and related structures, as these tend to be less relevant when considering the functional impact on sport. Mental health codes were also excluded as they related to mental health issues or intellectual functions already covered by a diagnosis of II. Whilst this reduction in codes was completed in advance of presentation to the Delphi panel, given the content of the excluded codes, not already covered by a diagnosis of II, their lack of significant impact on sports was felt not to be controversial, and assessing all the codes was too large a task for the panel to complete. The validity of this approach was checked by providing the panel the opportunity to identify areas not covered.
Procedure
This procedure was based on the initial stages used to develop ICF Core Sets (Selb et al., Citation2015). The expert panel were emailed the Qualtrics questionnaire and asked to rate the commonality of each problem area from zero (very rare) to 100 (very common). They were also asked how easy they found it to answer each question, from one (extremely easy) to five (extremely difficult) to get a measure of how accessible the items were. The panel were invited to comment on any additional health issues they thought were missing. Following analysis of the findings from round one, the questionnaire was reviewed and sent back to the expert panel for further comment. Final consensus on the inclusion of items was reached without the need for a further Delphi round.
Results
The lowest reported item was, “Problems relating to sensing temperature and other stimuli” (M = 14.00, SD = 8.72), and the highest was, “Problems with joint mobility” (M = 43.50, SD = 33.69). The panel judged all items to be common to more than 10% of people with II and so all items were included to maximize the comprehensiveness of the measure. None of the results suggested any items were difficult to answer. The items fell into three ICF domains; senses and pain; the heart, lungs and immune system; and movement and mobility. Following comments from the panel, a further three questions were added to cover issues with obesity and epilepsy. This included energy and drive (b130), weight maintenance (b530), taken from the ICF Core Set on Obesity (Stucki et al., Citation2004) and consciousness (b110) taken from previous research on epilepsy using the ICF (Cerniauskaite et al., Citation2012). The complete questionnaire consisted of 35 items.
Study 2 – field testing the ICF questionnaire
Participants
Inclusion criteria for participants across all three groups included: being over age 18; participation in a sport event in the last 12 months; being able to provide informed consent; being accompanied by an English-speaking supporter, familiar with the athlete and their medical history and able to act as translator if required; and meeting the Virtus IQ eligibility criteria of a full scale IQ of 75 or below. Inclusion in the Virtus group was by merit of being a Virtus athlete (i.e. qualified to compete at Virtus sanctioned international events). Inclusion in the Regional group was by having competed no higher than regionally in any II sporting event, were not Virtus registered athletes and recruited through Special Olympic and MencapFootnote2 events. Inclusion in the DS group was through a diagnosis of DS.
Overall, 116 athletes agreed to take part in the study. Fourteen athletes were excluded: three who were under 18; seven who scored above 75 on the WASI-II IQ screening assessment; one when it became apparent they did not have II (they were at university); one who did not complete the interview as they were upset about losing their match; and two who completed the WASI-II but did not respond to follow-up. This gave a sample size of 102. Details on the demographics of the athletes are included in . The majority of interviews took place in person, with eight Virtus athletes interviewed remotely. The DS group consisted of 23 athletes with trisomy 21 (72%), one athlete with mosaicism (3%) and one with translocation (3%). Information on the type of DS was unknown for seven (22%).
Table 2. Characteristics of participating athletes
Measures
Functional impairment
The ICF-based questionnaire as developed in study one was used to measure functional impairment. Where necessary, given that the questionnaire was to be administered to athletes with II and those caring or working with them, the wording of the questions was adapted from the ICF to provide prompts in simpler language. The item was given in its simple format first e.g., do you have any heart problems, and if an issue was found to be present this was then explored in more depth using both accessible and technical language (e.g., does your heart beat too fast sometimes (tachycardia)?). An interview protocol was developed so that the questionnaire was administered in a standardized way and providing standard ways of explaining some health conditions. If the athlete identified that they experienced the health problem they were asked to gauge the extent of the problem (severity), using an accessible scale adapted from the ICF Checklist (World Health Organisation, Citation2003). “No problem” was scored as zero, going up to a score of four for “Complete problem”, giving the possible range of scores as 0–140. Relevant demographic information was also collected.
Versions of the ICF-based questionnaire were created in German, French, Spanish and Finnish using the WHO online tool (http://www.icf-core-sets.org/en/page0.php). Whilst these used the original ICF language, they proved to be a useful reference for athletes and their supporters to check any medical terms they did not recognize. Further minor revisions were made in the early stages of data collection following feedback from interviews, involving changing some minor additions to the prompts, e.g., control of voluntary movement was broken down further to include fine motor skills. The athlete was interviewed in the presence of a supporter, which was often their coach or a family member, who assisted the athlete to understand the questions being asked and provided additional information if required.
Intellectual impairment
The Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II) was used to help ensure that the athlete met the criteria of having an IQ of 75 or below. It is a brief screening tool which can be used for research, but not for diagnostic purposes (Wechsler, Citation2011). It is a well validated and reliable tool based on the Wechsler family of IQ assessments. The two-subtest version was used in this study consisting of the Vocabulary and Matric Reasoning subtests. This provides a Full-Scale IQ (FSIQ) estimate, where the average score in the general population is 100. As Virtus athletes are required to pass the rigorous eligibility procedure, their FSIQ data was accessed through the Virtus records so it was not necessary to administer the WASI-II to this group.
Post-questionnaire interview
As part of the field testing to evaluate the ICF-based questionnaire, a short post-questionnaire was administered generating information about the ease of use of the questionnaire.
Procedure
Event organizers through Virtus, the Special Olympics and Mencap were approached for permission to attend events and were sent details about the research and what would be required. Nine sporting events were attended, including a European event in the Czech Republic and the Virtus Global Games in Brisbane. In addition, 10 clubs and training events were visited in England, France and Hong Kong. Coaches, parents and athletes were approached prior to, and at the events, and given information sheets. If they were interested in taking part a suitable time was arranged to meet them in a private space. After reviewing the information sheet, answering any questions about the research and seeking consent, the athletes were verbally administered the ICF-based questionnaire, followed by the post-interview questionnaire. Non-Virtus athletes were also asked to complete the WASI-II, which they could choose to complete before or after the ICF-based questionnaire. If athletes wanted to participate but were not able to at an event the opportunity to conduct the interview virtually was offered. The WASI-II was always conducted face-to-face, with a translator present if required.
Data analysis
Data analysis was conducted using SPSS statistical analysis software, version 23 (IBM Corp, Citation2015). Additional effect sizes were calculated using formulas in Field (Citation2013). An initial analysis was conducted on the demographic data to check for differences between the three groups. For the categorical variables (gender; health problems; medication; assistive devices) a Pearson Chi-Square was used. For the others (age; years competing) a one-way independent analysis of variance (ANOVA) was used. Where significant results were found, post-hoc pairwise comparisons were conducted to look for differences between the groups. Given the number of potential comparisons, the Bonferroni adjustment was chosen to control for Type 1 errors.
The reliability of the ICF-based questionnaire was analysed using Cronbach’s alpha. The ICF scores were treated as ordinal data, as the difference between the values may not have been equal. Due to this, and the positive skew to the ICF scores, the non-parametric Kruskal-Wallis test was used to analyse the ICF scores by group to test the hypothesis that impairment would vary by group. Pairwise comparisons were conducted on significant effects, to identity what group difference(s) were driving this. Following Field (Citation2013), Bonferroni-adjusted p-values were reported.
To establish whether there was a difference in IQ between the groups, and therefore whether it should be controlled for, a one-way between participants ANOVA was conducted. Due to the differences in sample sizes, post-hoc comparisons were conducted using Gabriel’s procedure (Field, Citation2013). A multinomial logistic regression was then conducted, with groups as the outcome variable. A power calculation was conducted to determine the necessary sample size, giving a target of 31 athletes in each of the three groups (Field, Citation2013; N = , p. 92). This was calculated using a medium effect size and five potential predictors (IQ, ICF-based questionnaire score, age, gender, and number of years competing). To more directly test the hypothesis that a measure that considers functional impairment (i.e. the ICF-based questionnaire) will be able to better predict group membership than IQ alone, the multinomial logistic regression was conducted using just IQ and ICF score as variables. As the multinomial logistic regression did not include all three possible pairwise comparisons between the groups it was followed by three binary logistic regressions, in which the dependent variable of group was respectively “Virtus vs. DS”, “Regional vs. DS”, and “Virtus vs. DS”. In each of these regressions, IQ was entered as the sole predictor in the first model, while IQ and ICF score were both predictors in the second model, such that a significant improvement in model fit from the first to second models would indicate that ICF and IQ together better predicted group membership than IQ alone.
Results
Qualitative feedback on the ICF-based questionnaire
All athletes completed the full ICF-based questionnaire and post-interview questionnaire The results of the post-interview questionnaire showed that in terms of accessibility and the respondent experience, the ICF-based questionnaire seemed to work well, and despite the medical terminology attached to some of the items, with the additional supporting material, most respondents demonstrated a good understanding of the questions. The combination of the interviewer aided by the supporter was positive and was inclusive of the athlete with II which was appreciated by them.
Group homogeneity
IQ information was missing for four of the Regional athletes and three of the DS athletes. There was no significant difference in gender balance across the three groups (X2 (2, N = 102) = 2.25, p = .325) or across the groups for age (F(2,99) = 1.57, p = .219), number of years competing in their current sport (F(2,99) = 1.21, p = .304), and years competing overall (F(2,99) = .80, p = .452), suggesting the three groups are comparable on these variables.
The use of assistive devices (glasses and hearing aids) significantly differed across the groups, and whether the device could be worn during sport. Post-hoc comparisons found significant results on these variables between the Virtus and other groups for assistive devices. These comparisons also highlighted a greater similarity between the Regional and DS groups when compared with the Virtus group, indicating less reliance on such devices for the Virtus group. Athletes were also asked if they were currently suffering any health problems. Whilst there was a trend for less issues reported in the Virtus group Bonferroni-adjusted post-hoc comparisons showed no significant differences between the groups.Footnote3
Testing hypothesis 1: The hierarchy of competition grouping would be replicated in relation to levels of impairment, such that athletes in the Virtus group would have relatively low level of impairment, compared to the Regional and DS groups.
Using all 35 problem-related items on the ICF-based questionnaire gave an acceptable internal consistency, Cronbach’s ɑ = .75 (Field, Citation2013). This suggested a sum of all the individual item scores (the “ICF score”) could be used in the analysis related to hypothesis 1. As shown in , the DS group had the largest mean ICF score, and the Virtus group the lowest. The ICF score significantly differed across the groups. Post-hoc comparisons showed a significant difference between the Virtus and DS groups, but no other significant group differences (see and ). It should be noted that the effect sizes indicate a medium to large effect for the Virtus-DS group comparison, but a small effect for the others.
Figure 1. ICF scores across the three groups
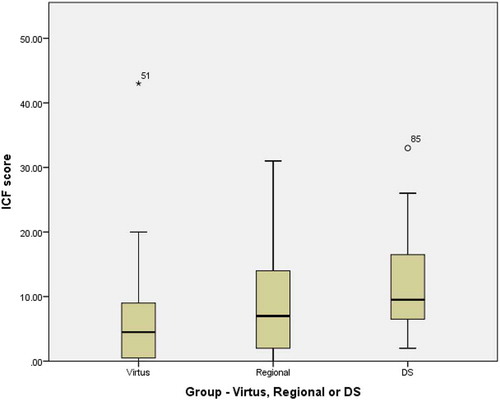
Table 3. Comparisons between the three groups of athletes on the ICF-based questionnaire total score, using an independent samples Kruskal-Wallis test, and the effect size (r) of post-hoc comparisons
Testing hypothesis 2: ICF scores would be a better predictor of group membership than IQ
As shown in , IQ significantly differed across groups, with post-hoc comparisons revealing that the DS group had significantly lower IQ than both the Virtus and Regional groups (both p < .001), while the Virtus and Regional groups did not significantly differ (p = .868).
Table 4. One-way ANOVA comparisons between the three groups of athletes on IQ
A multinomial logistic regression was conducted with IQ and ICF score as the predictors and group (Virtus, Regional and DS) as the dependent variable (). This revealed that, even when IQ was included in the model, ICF score was a significant predictor of group membership, at least with respect to discriminating between the Virtus and DS groups. A significant improvement in fit was found for the binary logistic regressions predicting “Virtus vs. DS” (X2(1) = 5.05, p = .025) and “Regional vs. DS” (X2(1) = 3.86, p = .049), but not for the regression predicting “Virtus vs. Regional ” (X2(1) = 0.90, p = .342).
Table 5. Multinomial logistic regression predicting group membership, with Virtus as the reference group
Discussion
The purpose of the two studies was to a) compose an ICF-based questionnaire that represents health impairments commonly associated with II which may impact on sports performance and b) to test the sensitivity and discriminant validity of this new ICF questionnaire, and its ability to predict group membership of three levels of sport competition. The Delphi study suggested a good level of agreement between the expert panel in relation to the health issues to be included. In terms of the administration of the test, involving both the athlete, an informed supporter and, where necessary, a translator, this worked well and feedback from the participants was positive. Despite the quite medical nature of some of the terminology used in the items, the protocol of having standardized, simplified explanations, and the questionnaire being available in several languages certainly facilitated the administration and suggests face validity. The internal robustness of the questionnaire met the required standards to use a total score and the range of scores demonstrated no floor or ceiling effects.
The hypothesis that the hierarchy of competition grouping would be replicated in relation to levels of impairment, such that athletes in the Virtus group would have relatively low level of impairment, compared to the Regional and DS groups was supported. However, the findings regarding the ICF score discriminating between specific pairs of groups are worth treating somewhat tentatively at this stage, both because the significant findings may be a Type 1 error, as the chances of this have been inflated by multiple comparisons, and because the non-significant finding may be a Type 2 error, arising from the relatively small sample size. Nevertheless, the finding of a distinction between the DS group and Virtus group does seem to be a robust finding and replicates that of Gilderthorp et al. (Citation2018), using the less refined ICF checklist. Whilst significant differences are not proven between all three groups, the order of level of impairment associated with the three competition groupings and likely hierarchy of performance levels is promising.
In order to re-test the assumption that IQ is not related to competition group membership differences in IQ scores between the three groups were examined and there was no significant difference in IQ between the Virtus and the Regional groups, confirming this assumption. That IQ was significantly lower in the DS group is not surprising given that other studies have reported similar findings when comparing participants with DS to those with II and unknown aetiology (e.g., Memisevic & Sinanovic, Citation2014; Patterson et al., Citation2013). Research into the early development and cognitive profile of children with DS also suggests that primary cognitive deficits lead to impaired secondary cognitive gains and deterioration in IQ over the developmental timeline (Karmiloff-Smith et al., Citation2016). As hypothesized ICF total score was found to be a better predictor of group membership than IQ for the Virtus and DS groups. We would also suggest that the overall finding that ICF score is useful in predicting group membership even when IQ is accounted for is robust, and certainty sufficient to justify further research examining the ability of ICF scores to predict the performance of athletes with II.
Conceptually, it is encouraging that the questionnaire distinguishes between the three groups as hypothesized, albeit reliability needs to be improved. Most important is that the questionnaire reliably distinguishes between the Virtus and the DS groups, as it is equivalence to those athletes with DS which is currently being sought so that athletes with a similar level of functional impairment are grouped with DS athletes in Virtus competitions. In relation to the lack of contrast between the Virtus and Regional groups it is acknowledged that assumptions exist about the membership of those in the Regional group, such as they could not perform at an elite level, which might be an artefact of opportunity and training and not related to their actual potential and related health impairments. In addition, assumptions were made about contextual issues, such that the athlete in the Regional group may have elite potential, but through their financial or cultural situation advancement to international competition was not possible. This is a limitation which could have been better controlled for by applying stricter entry criteria into this group in relation to time engaged in sport and training history, to screen out athletes who may be early in their careers and their full potential not tested. Future research might concentrate on developing a comparator group of II athletes whose optimal performance levels are known not to reach international standards. Greater variety might also be expected from a non-matched sample and greater control over the selection into this group might have provided a sharper contrast in level of impairment and validity of the implied performance level.
Further work needs to be completed before a Virtus classification structure can be implemented and cut-off figures confirmed. In terms of the fit with the conceptual model it would be helpful to examine the relationship between the ICF questionnaire and actual sporting performance, as it is expected that there should be a negative correlation between questionnaire scores and sporting performance. Likewise, as another form of construct validity, one might expect a positive relationship between reliable adaptive behaviour measures and the ICF questionnaire, as impaired overall functioning should impact on adaptive behaviour, which also may account for some of the variability found between the association between IQ and adaptive behaviour (Murray et al., Citation2014).
Once the reliability of the questionnaire is established and it is judged “fit for purpose” from a research perspective, various operational hurdles must be surmounted in terms of how it is used in practice. Within Virtus it is expected that all those applying to II2 will come through the II1 eligibility procedures, to confirm the presence of II, and then apply to enter the II2 class, to demonstrate additional significant impairment. One issue is how to safeguard against intentional misrepresentation. One approach, given that the questionnaire aims to identify increased functional impairment through the presence of additional health issues, is to use it as a screening questionnaire, and a confirmatory step of requiring medical proof for those issues identified is included. This could be further enhanced through research using in-competition observation, previous performance records and use of the Virtus eligibility data which all Virtus competitors will have as a consequence of going through II1 eligibility, i.e. IQ and adaptive behaviour data. Other operational challenges lie in the training and quality assurance of assessors and the infrastructure required to operate the system.
Research is in progress to advance the development of the questionnaire to further test its validity and relationship with sports performance, with the aim of setting cut-off scores to enable the piloting of a wider II2 Virtus class, and as a result invite a wider range of athletes with II to participate in international sport. Once such competition classes are established it will be possible to embark upon the work to establish sport-specific classification procedures consistent with the IPC requirements. As set out in the IPC position statement process-focussed research must develop “objective, reliable methods for measuring both of the core constructs – impairment and activity limitation” (Tweedy, & Vanlandewijck, Citation2011, p267). This paper has set out a conceptual approach to measuring impairment within the context of developing an additional Virtus competition class, further research will look at the utility of this approach in measuring activity limitation. These are incremental steps in a programme of work to establish additional competition classes in Virtus, and in the longer term develop sport-specific approaches to classification suitable for the further expansion of international competition opportunities for athletes with II both within Virtus and IPC sanctioned events.
Supplemental Material
Download MS Word (24.5 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed online https://doi.org/10.1080/02640414.2021.1881302.
Notes
1 ICD-11 was published in 2018 and the new terminology to be adopted is “Disorders of Intellectual Development”. This will not come into full effect until 2022.
2 A UK charity providing sports events for athletes with II.
3 Please refer to Figshare for full analysis.
References
- American Psychiatric Association 2015. Diagnostic and statistical manual of mental disorders. (5th ed. update ed).
- Bertelli, M. O., Cooper, S., & Salvador-Carulla, L. (2018). Intelligence and specific cognitive functions in intellectual disability: Implications for assessment and classification. Current Opinion in Psychiatry, 31(2), 88–95. https://doi.org/10.1097/YCO.0000000000000387
- Brady, S. R. (2015). Utilizing and adapting the delphi method for use in qualitative research. International Journal of Qualitative Methods, 14(5), 1609406915621381. https://doi.org/10.1177/1609406915621381
- Cerniauskaite, M., Ajovalasit, D., Quintas, R., Alvarez, A., Franceschetti, S., Casazza, M., … Leonardi, M. (2012). Functioning and disability in persons with epilepsy. American Journal of Physical Medicine & Rehabilitation, 91(13), S22–S30. https://doi.org/10.1097/PHM.0b013e31823d4d6f
- Field, A. (2013). Discovering statistics using IBM SPSS statistics. Sage.
- Gilderthorp, R., Burns, J., & Jones, F. (2018). Classification and intellectual disabilities: An investigation of the factors that predict the performance of athletes with intellectual disability. Journal of Clinical Sport Psychology, 12(3), 285–301. https://doi.org/10.1123/jcsp.2017-0018
- IBM Corp. (2015). IBM SPSS Statistics for Windows. Armonk, NY: IBM Corp.
- IPC. (2015). Athlete Classification Code. https://www.paralympic.org/classification-code
- Johnson, W., Jung, R. E., Colom, R., & Haier, R. J. (2008). Cognitive abilities independent of IQ correlate with regional brain structure. Intelligence, 36(1), 18–28. https://doi.org/10.1016/j.intell.2007.01.005
- Karmiloff-Smith, A. (2009). Nativism versus neuroconstructivism: Rethinking the study of developmental disorders. Developmental Psychology, 45(1), 56. https://doi.org/10.1037/a0014506
- Karmiloff-Smith, A. (2018). Development itself is the key to understanding developmental disorders. In Karmilloff-Smith, A., Thomas, M.S. & Johnson, M.H. (Eds), Thinking developmentally from constructivism to neuroconstructivism (pp. 97–117). Routledge.
- Karmiloff-Smith, A., Al-Janabi, T., D’Souza, H., Groet, J., Massand, E., Mok, K., … Nizetic, D. (2016). The importance of understanding individual differences in down syndrome. F1000Research, 5. https://doi.org/10.12688/f1000research.7506.1
- Kinnear, D., Morrison, J., Allan, L., Henderson, A., Smiley, E., & Cooper, S. (2018). Prevalence of physical conditions and multimorbidity in a cohort of adults with intellectual disabilities with and without down syndrome: Cross-sectional study. BMJ Open, 8(2), e018292. https://doi.org/10.1136/bmjopen-2017-018292
- McKenzie, K., Milton, M., Smith, G., & Ouellette-Kuntz, H. (2016). Systematic review of the prevalence and incidence of intellectual disabilities: Current trends and issues. Current Developmental Disorders Reports, 3(2), 104–115. https://doi.org/10.1007/s40474-016-0085-7
- Memisevic, H., & Sinanovic, O. (2014). Executive function in children with intellectual disability–the effects of sex, level and aetiology of intellectual disability. Journal of Intellectual Disability Research, 58(9), 830–837. https://doi.org/10.1111/jir.12098
- Misheva, E. (2018). Are neurodevelopmental disorders discrete conditions? Psychologist, 31, 34–37. https://thepsychologistbps.org.uk/volume-31/august-2018/are-neurodevelopmental-disorders-discrete-conditions
- Murray, A., McKenzie, K., & Murray, G. (2014). To what extent does g impact on conceptual, practical and social adaptive functioning in clinically referred children? Journal of Intellectual Disability Research, 58(8), 777–785. https://doi.org/10.1111/jir.12092
- Nakken, H., & Vlaskamp, C. (2007). A need for a taxonomy for profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, 4(2), 83–87. https://doi.org/10.1111/j.1741-1130.2007.00104.x
- Patterson, T., Rapsey, C. M., & Glue, P. (2013). Systematic review of cognitive development across childhood in down syndrome: Implications for treatment interventions. Journal of Intellectual Disability Research, 57(4), 306–318. https://doi.org/10.1111/j.1365-2788.2012.01536.x
- Selb, M., Escorpizo, R., Kostanjsek, N., Stucki, G., ÜSTüN, B., & Cieza, A. (2015). A guide on how to develop an international classification of functioning, disability and health core set. European Journal of Physical and Rehabilitation Medicine, 51(1), 105–117. http://pub,ed.ncbi.nlm.nih.gov/24686893/6893
- Simeonsson, R. J. (2009). ICF‐CY: A universal tool for documentation of disability. Journal of Policy and Practice in Intellectual Disabilities, 6(2), 70–72. https://doi.org/10.1111/j.1741-1130.2009.00215.x
- Stucki, A., Daansen, P., Fuessl, M., Cieza, A., Huber, E., Atkinson, R., … Ruof, J. (2004). ICF core sets for obesity. Journal of Rehabilitation Medicine, 36, 107–113. https://doi.org/10.1080/16501960410016064
- Tweedy, S. M. (2002). Taxonomic theory and the ICF: Foundations for a unified disability athletics classification. Adapted Physical Activity Quarterly, 19(2), 220–237. https://doi.org/10.1123/apaq.19.2.220
- Tweedy, S. M., & Vanlandewijck, Y. C. (2011). International Paralympic Committee position stand--background and scientific principles of classification in Paralympic sport. British Journal of Sports Medicine, 45(4), 259–269. https://doi.org/10.1136/bjsm.2009.065060
- Ustun, B., Chatterji, S., & Kostanjsek, N. (2004). Comments from WHO for the journal of rehabilitation medicine special supplement on ICF core sets. Journal of Rehabilitation Medicine-Supplements, (44 Suppl), 7–8. https://doi.org/10.1080/16501960410015344
- Vale, M. D. C., Pereira-da-Silva, L., Pimentel, M. J., Marques, T. N., Rodrigues, H., Cunha, G., … Simeonsson, R. J. (2017). Classifying functioning of children and adolescents with intellectual disability: The utility of the international classification of functioning, disability and health for children and youth. Journal of Policy and Practice in Intellectual Disabilities, 14(4), 285–292. https://doi.org/10.1111/jppi.12199
- Van Biesen, D., Burns, J., Mactavish, J. J., Van de Vliet, P., & Vanlandewijck, Y. C. (2021). Conceptual model of sport-specific classification for para-athletes with intellectual impairment. Journal of Sports Sciences. https://doi.org/10.1080/02640414.2021.1881280
- Van Biesen, D., Mactavish, J., Kerremans, J., & Vanlandewijck, Y. C. (2016). Cognitive predictors of performance in well-trained table tennis players with intellectual disability. Adapted Physical Activity Quarterly, 33(4), 324–337. https://doi.org/10.1123/APAQ.2015-0122
- Van Biesen, D., Mactavish, J. J., & Vanlandewijck, Y. C. (2014). Comparing technical proficiency of elite table tennis players with intellectual disability: Simulation testing versus game play 1. Perceptual and Motor Skills, 118(2), 608–621. https://doi.org/10.2466/15.30.PMS.118k21w5
- Wechsler, D. (2011). WASI-II: Wechsler abbreviated scale of intelligence. PsychCorp.
- Whitaker, S. (2015). How accurate are modern IQ tests at categorising people as ID or non ID? Clinical Psychology Forum, 260, 49–53.
- World Health Organisation. (2001). ICF: International classification of functioning, disability and health. https://www.who.int/classifications/international-classification-of-functioning-disability-and-health
- World Health Organisation. (2003). ICF checklist version 2.1a, clinical form for international classification of functioning, disability and health. World Health Organisation, Geneva. Retrieved July, 2020, from https://www.who.int/classifications/icf/icfchecklist.pdf?ua=1#:~:text=The%20ICF%20Checklist%20is%20a,ICF%20or%20ICF%20Pocket%20version.
- World Health Organisation. (2004). ICD-10: International statistical classification of diseases and related health problems: Tenth revision (2nd ed.).
- World Health Organisation. (2011). World report on disability 2011.
- World Health Organisation. (2016). ICD-10: The ICD-10 classification of mental and behavioral disorders: Clinical descriptions and diagnostic guidelines (5th ed.).