
ABSTRACT
This study assessed the lead and trail arm peak and average extensor carpi ulnaris (ECU) muscle activity in association with tri-planar angular velocities of the lead and trail wrists during the golf swing. Fifteen sub-elite, male right-handed golfers (Mage = 34.7 years ±13.3, Mhandicap = 1.5 ± 2.2) were recruited to execute five shots each with their pitching wedge, 7-iron and driver clubs in an indoor golf simulator. Surface electromyography (EMG) sensors were placed over the ECU muscle belly and inertial measurement unit sensors were placed bi-laterally on the distal forearm and dorsum of the hand. There was a statistically greater recruitment of the trail ECU muscle during the downswing (p < 0.001) for all clubs. The lead ECU muscle was recruited more during the backswing (p < 0.001) and follow through (p < 0.024) phases. There were statistically different tri-planar movement patterns between the lead and trail wrist throughout all three phases of the golf swing. No significant relationships were found between downswing EMG data and clubhead kinematics at impact. In conclusion, differing wrist kinematics and associated muscle activity may contribute to the asymmetrical injury pattern seen clinically.
Introduction
Wrist injuries are the second most common injury reported in sub-elite and elite level golfers (Robinson et al., Citation2019). The lead wrist (left wrist in right-handed golfers) accounts for 67% of all wrist injuries, of which 52% relate to pathology of the extensor carpi ulnaris (ECU) muscle/tendon/sheath (Hawkes et al., Citation2013; Robinson et al., Citation2019). Pathologies of this tendon typically concern tendinopathy, tenosynovitis or tendon instability with subluxation and can lead to golfers reducing their practice for 5–24 weeks and missing 3–12 tournaments per year (Hawkes et al., Citation2013). It is hypothesised that the reason for a higher incidence of wrist injuries in elite level golfers compared to amateurs is due to high practice volumes, higher swing velocities and the downward striking action at ball contact (i.e., striking the ground with the clubhead). However, factors that may predispose towards ECU injury in the lead wrist have not yet been explored through biomechanical and electromyographical studies.
ECU is comparable in activation during supination and pronation and is one of the most active muscles within the forearm in both positions (Bader et al., Citation2018). In supination, the tendon exits the sixth compartment at approximately 30° to the long axis of the radius, placing maximal tension on the ECU retinaculum and sub-sheath. The position of forearm rotation influences the action of ECU. In supination, the tendon assumes a dorsal location and acts as a pure extensor whereas with the wrist neutrally positioned, ECU is most active in the combined movement of extension and ulnar deviation (Shah et al., Citation2017). Shin et al. performed a fine-wire electromyography (EMG) analysis in the lead and trail arms of both amateur and professional golfers with tennis elbow and found that extensor carpi radialis brevis (ECRB) EMG activity peaked in the lead arm in the downswing and gradually diminished throughout the remainder of the swing (Farber et al., Citation2009). In the trail arm, ECRB was recruited to a greater extent in the takeaway and less in the downswing, compared to the lead side (Farber et al., Citation2009). These data suggest that ECU may have different EMG behaviours, despite its proximity (in location and action) to ECRB, as it is involved in ulnar deviation in addition to extension.
The golf swing is typically divided into three phases; backswing, downswing and follow through. Three studies have previously examined EMG of the forearm muscles during the golf swing (Farber et al., Citation2009; Glazebrook et al., Citation1994; Sorbie et al., Citation2016). Despite ECU being the most frequently injured structure in the wrist/forearm of elite and sub-elite golfers, none of the aforementioned studies have captured its activity. It is unknown when ECU is most active in the golf swing and whether it is more active overall in the lead or trail wrist. The type of activity of this muscle may, in some part, be responsible for the incidence of tendinopathy/tenosynovitis. A greater understanding of the angular velocity dynamics with respect to the phase, magnitude and type of contraction may yield greater insights into potential injury mechanisms and performance markers.
Recently, statistical parametric mapping (SPM) has been used to investigate time-series data including joint kinematics and EMG (Pataky et al., Citation2013; Robinson et al., Citation2015). This offers the advantage over discrete parameter analysis because it takes the amplitude and timing over the whole time series into consideration. This approach can be used to investigate movement patterns, as well as the contribution and timing of muscle activity during dynamic movements, which may help to improve observations of potential injury risks, particularly when considering the timing of muscle activity and joint velocities. Therefore, the purpose of this study was to assess the peak enveloped and average rectified ECU muscle activity in the lead and trail arm in association with the tri-planar angular velocities of the lead and trail wrists during the golf swing in sub-elite golfers. The hypotheses were that a greater ECU peak enveloped and average rectified muscle activity with a different sequence of muscle activation would be seen in the lead side when compared to the trail, and these responses would be consistent across a range of clubs used by golfers.
Method
Participants
Fifteen male, sub-elite right-handed golfers (Mage = 34.7 years ±13.3, Mexperience = 25.9 years ±14.5) were recruited for this study. Golfers were classified as “sub-elite”, which meant that they had an official Council of National Golf Unions (CONGU) handicap of ≤ 5 (M = 1.5 ± 2.2) (Murray et al., Citation2020) or were a qualified PGA Professional golf coach. Golfers were excluded if they had a history of a previous wrist injury. Each golfer was consulted and examined by an orthopaedic clinician to rule out any existing wrist pathology. In addition, golfers were excluded if, despite being right-handed, they ordinarily played golf with the right hand as their leading hand. Prior to data collection, the study received ethical approval from the Moray House School of Education and Sport ethics committee at The University of Edinburgh and all participants provided signed informed consent. Testing was conducted in accordance with NHS and Scottish government guidelines for research (NHS Scotland NHS Inform, Citation2020).
Data collection
To ensure consistency of the task for all participants, data were collected at a golf club in Edinburgh (UK) utilising an indoor swing studio on an artificial turf mat with a simulator set to “driving range” mode, which includes no wind and standard ground conditions. Golfers wore their own golf shoes, wore a glove if they preferred, used their own clubs and hit provided new golf balls (Titleist Pro V1). Previous studies have shown no difference in forearm muscle activity during the golf swing with or without wearing a glove (Sorbie et al., Citation2017). Prior to commencing data collection, participants were advised and permitted to perform a self-conducted warm-up as they normally would prior to play. This consisted of stretching exercises, practice swings and shots into the simulator until each participant reported that they were ready to begin.
Test conditions consisted of five full golf swings with each of a driver (from a tee at a height determined by each participant’s preference), 7-iron and pitching wedge (15 shots in total), with the latter two being struck from an artificial grass mat. Specifically, the order of trials across these clubs were balanced to ensure that participants maintained adequate focus during each trial and to remove any possibility of an order-effect that could still be possible with randomisation. Trials were conducted in blocks of five shots with a break of 30 s between each trial and 1 min between each block to prevent fatigue. Each trial required hitting towards a target on the driving range positioned in a straight line from the starting position, with the instruction to hit the ball as close to the target line as possible. Participants were instructed to swing using their most usual and well-established technique and not to try and alter their shot shape away from the natural ball-flight, as evidence has shown this can disrupt the motor control strategy in this level of golfer (Carson et al., Citation2014, Citation2016).
To record muscle activity, two wireless EMG sensors (TrignoTM Avanti mini sensors, Delsys, USA) recording at 1000 Hz and band passed 20–450 Hz were fixed using double-sided tape directly over the muscle belly of the ECU on the lead and trail forearm with the sensor electrodes aligned perpendicular to the muscle fibre direction. EMG sensor placement was identified as halfway between the lateral epicondyle and the base of the little finger metacarpal bone, immediately dorsal to the bony ulnar ridge (Burkhart & Andrews, Citation2010; Mogk & Keir, Citation2003). To reduce the skin impedance, all participants had the identified area of forearm shaved and prepared with alcohol wipes in accordance with the SENIAM guidelines (Hermens & Workshop, Citation1998). Inertial measurement unit (IMU) sensors (TrignoTM Avanti, Delsys, USA) recording at 148 Hz were fixed in the same way but positioned at the distal end of the lead and trail forearms and on the dorsal surface of both hands. IMU data allowed the key swing events to be determined in order to define the different golf swing phases and the wrist angular velocities.
Data processing
Raw EMG and IMU data were exported to c3d file format and processed using Visual3D software (version v2022.10.2, USA). The direct current offset was removed and the EMG data were then high pass filtered at 20 Hz to reduce any movement artefacts, then rectified and low pass filtered at 15 Hz (Bonifacio et al., Citation2018; Richards et al., Citation2008). All EMG data were normalised to the maximal observed signal seen across all trials for all clubs for each participant.
The swing was divided into three phases (backswing, downswing and follow-through). Events were defined by utilising the IMU sensors (see ) and each phase was normalised to 101 points. Swing Onset was defined by the angular velocity of the lead hand IMU crossing a threshold of 20 °/s in the local transverse plane. The Top of the Swing event was defined by the angular velocity of the lead distal forearm IMU with a threshold of − 20 °/s on descent in the transverse plane following Swing Onset. Impact was defined by calculating the first derivative of the lead hand acceleration in the proximal-distal direction and identifying the moment that this crossed −200 m/s3 on descent. Swing End was defined as the angular velocity of the lead hand IMU crossing a threshold of 20 °/s in the local transverse axis following the impact event. Swing phases were created using the Swing Onset to Top to define the “backswing”, the Top of the Swing to Impact to define the “downswing” and Impact to Swing End to define the “Follow Through”.
Figure 1. Swing events identified using IMU kinematic signals. (a) “Swing Onset” defined using the angular velocity of the lead hand IMU crossing a threshold of 20 °/s in the local transverse plane, “Swing End” defined in the same way following the impact event. (b) “Top of Swing” defined by the angular velocity of the lead distal forearm IMU with a threshold of − 20 °/s on descent in the transverse plane following Swing Onset. “Impact” defined by calculating the first derivative of the lead hand acceleration (c) in the proximal-distal direction and identifying the moment that this crossed −200 m/s3 on descent (d). All events are identified on each graph by a vertical dotted line, with event labels provided when pertaining to the specific kinematic data presented.
The three-dimensional angular velocities were time normalised for each swing phase and were calculated by considering the hand segment rotational velocities with respect to the distal forearm. The methods used to describe the relationship between IMU sensors at the distal forearm and the dorsum of the wrist have previously been validated (Manivasagam & Yang, Citation2022). The hand segment rotation velocities were equivalent to the forearm rotation velocity given pronation and supination of the wrist occurs at the radiocapitellar joint. For the EMG data, average rectified and peak low pass filtered signals within the different phases were exported for statistical analysis. Performance variables were collected for analysis using the TrackManTM launch monitor (TrackMan A/S, Denmark) (Turner et al., Citation2020). Variables collected were: angle of attack (°), swing direction (°) and swing speed (mph). Negative values reflect a downward and positive values reflect an upward angle of attack. Negatives values for swing direction reflect a movement towards the left of the target (out-to-in path), while positive values reflect a movement towards the right of the target (in-to-out path).
Data analysis
Statistical analysis of the different phases was performed using Statistical Package for Social Sciences (SPSS) software (v.28, IBM Inc., USA). The distribution of the data was assessed using Kolmogorov–Smirnov tests and all data were found to be suitable for parametric testing. Three-factor (club, lead/trail, phase) repeated measures analysis of variance (RM ANOVA) tests were performed on the enveloped EMG data and any interactions were then further explored using statistical parametric mapping (SPM; Python software, v. 3.9.4) (Robinson et al., Citation2015). Time series (SPM) analysis of the entire swing for enveloped EMG data and three dimensional wrist angular velocities was then used to assess for differences in peak amplitude and timing between the lead and trail sides. Pearson’s product moment correlations were used to assess the relationships between performance variables and EMG measures. A p-value of < 0.05 was considered statistically significant and effect sizes were calculated using partial eta squared (ƞp2), with 0.02 denoting a weak effect, 0.13 denoting a medium effect and 0.26 denoting a strong effect (Barrio Minton & Lenz, Citation2019).
Results
The average and peak EMG data for each golf club for each phase of the swing for the trail and lead sides can be seen in . There were significant main effects for side, club and phase for both the average and peak data. Post-hoc pairwise within subject comparisons of each club and each phase for both average rectified and peak enveloped data can be seen in . However, significant interactions were found between side and phase for both the average (p < 0.001, ƞp2 = 0.564) and peak EMG data (p = 0.008, ƞp2 = 0.293), therefore, further exploration of the differences between the lead and trail side over the entire swing using SPM was performed for each club separately.
Table 1. Mean rectified and enveloped EMG data including effect sizes for lead and trail ECU with each club during each phase of the golf swing.
Table 2. Rectified and enveloped post-hoc pairwise within subject comparisons of each club and each phase.
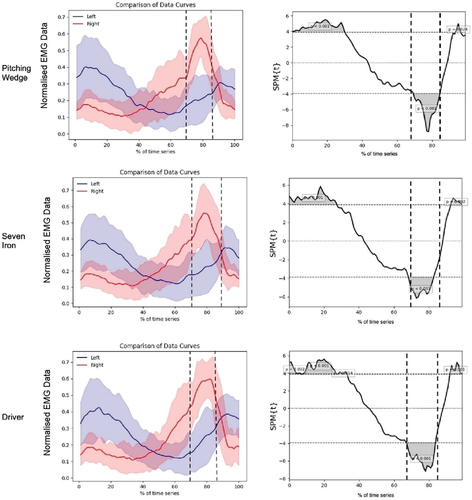
The mean time during the swing for backswing to downswing transition for pitching wedge, 7-iron and driver was 68%, 70% and 68%, respectively (p = 0.979). The mean time during the swing for downswing to follow through transition for pitching wedge, 7-iron and driver was 84%, 87% and 86% respectively (p = 0.919).
shows the comparison data curves and SPM analysis for the peak enveloped EMG data over the whole of the golf swing for the pitching wedge, 7-iron and driver. Significantly greater activity was seen in the trail ECU during the downswing (p < 0.001) for all clubs, with the lead ECU being recruited more during the backswing (p < 0.001) and the follow through (p < 0.024).
Figure 2. Comparison of the data curves as a percentage of time (left) and SPM analysis (right) for enveloped EMG for the lead and trail side during the whole of the golf swing. “Swing Onset” occurs at 0, the first vertical dotted line indicates the “Top of Swing” event, the second vertical dotted line indicates the “Impact” event and “Swing End” occurs at 100.
Wrist kinematics
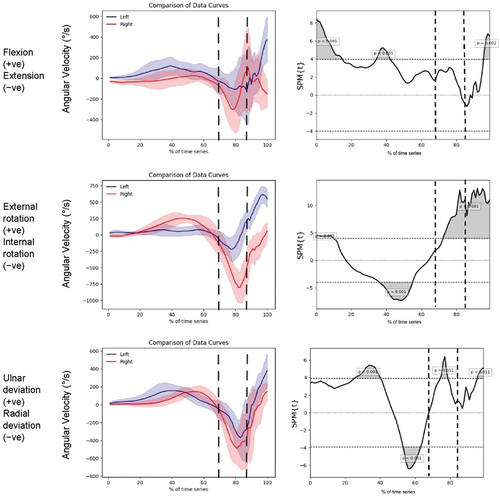
show the comparison data curves and SPM analysis for the angular velocity data over the whole of the golf swing for the pitching wedge, 7-iron and driver. There were statistically different movement patterns in flexion/extension, external/internal rotation and radial/ulnar deviation between the lead and trail wrist throughout all three phases of the golf swing.
Figure 3. Tri-planar IMU kinematic data for the pitching wedge with corresponding statistical parametric analysis “Swing Onset” occurs at 0, the first vertical dotted line indicates the “Top of Swing” event, the second vertical dotted line indicates the “Impact” event and“ Swing End” occurs at 100.
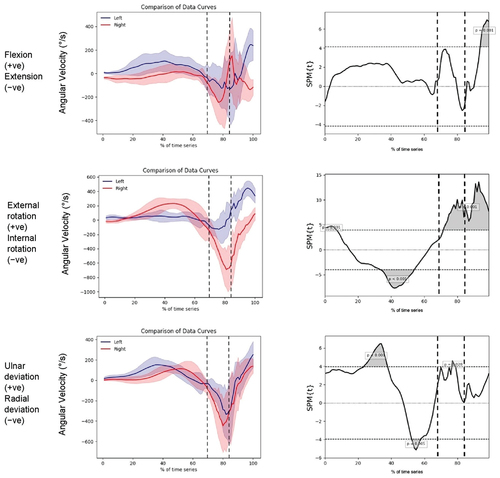
Figure 4. Tri-planar IMU kinematic data for the 7-iron with corresponding statistical parametric analysis “Swing Onset” occurs at 0, the first vertical dotted line indicates the “Top of Swing” event, the second vertical dotted line indicates the “Impact” event and “Swing End” occurs at 100.
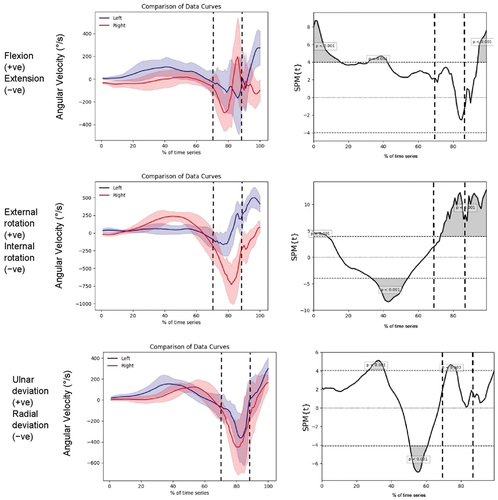
Figure 5. Tri-planar IMU kinematic data for the driver with corresponding statistical parametric analysis “Swing Onset” occurs at 0, the first vertical dotted line indicates the “Top of Swing” event, the second vertical dotted line indicates the “Impact” event and “Swing End” occurs at 100.
Performance characteristics
There was no significant relationship found between the angle of attack, club path or clubhead speed with lead or trail sided downswing EMG data (p > 0.05; ).
Table 3. Correlation between performance characteristics and downswing EMG data.
Discussion
The purpose of this study was to assess the peak enveloped and average rectified ECU muscle activity in the lead and trail arm in association with the tri-planar angular velocities of the lead and trail wrists during the golf swing in sub-elite golfers. The hypotheses were that a greater ECU peak and average muscle activity with a different sequence of muscle activation would be seen in the lead side when compared to the trail, and these responses would be consistent across a range of clubs used by golfers. The key findings were that 1) ECU is activated to varying degrees in the lead and trail arm and 2) at different times of sub-elite level golfers. The differing kinematics demonstrated in each wrist and the associated muscle activity may contribute to the asymmetrical injury pattern seen clinically. Golfing performance metrics in the downswing had no correlation with the magnitude of ECU muscle activity in either arm. These findings confirmed our hypothesis that muscle activity sequencing differed between the trail and lead wrists during each phase of the swing and this was consistent across all clubs.
ECU injuries are a common problem for skilled golfers (Hawkes et al., Citation2013). Understanding the causative factors associated with the injury and subsequently providing treatment, rehabilitative and preventative strategies are all important roles for healthcare and sport science practitioners. Most ECU injuries do not happen after a single discrete incident but occur secondary to tissue overload due to force being repeatedly channelled through tissues. This mechanism can lead to tendinopathy or tenosynovitis (Hawkes et al., Citation2013). Less common are traumatic injuries, which can include the tendon being torn out of its sub-sheath leading to ECU instability. Despite the prevalence of ECU injuries, the causative factors associated with it are yet to be studied. The asymmetrical loads exerted via the tendon during the swing via muscle contraction and the complex kinematics occurring at each wrist joint during the swing may be associated with the asymmetrical injuries phenotypes clinically seen in elite golf.
Studies have found that more skilled golfers have less lead wrist radial deviation at impact (Fedorcik et al., Citation2012) while there have been several biomechanical studies describing increased distal ulna loading with progressive increase in ulnar deviation (af Ekenstam et al., Citation1984; Markolf et al., Citation1998, Citation2000). This finding would be expected to be compounded when the forearm rotates into pronation because this movement results in relative ulnar lengthening. Carson et al. studied the kinematics of the wrist in professional golfers and found greater internal/external rotation range of motion in the lead compared to the trail side when referencing the hand to the distal forearm segment (Carson et al., Citation2019). Furthermore, the authors found the positioning of the hands while gripping the golf club played a role in changing the kinematics and clubface angle relative to the target at impact. Shin et al. demonstrated ECRB EMG activity peaking in the lead arm in the downswing and gradually diminishing throughout the remainder of the swing. In the trail arm, ECRB decreased during the downswing, increased before impact and then gradually diminished throughout the remainder of the swing (Farber et al., Citation2009). These findings are in contrast to our data for ECU where the trail ECU activity was greater than the lead wrist in the downswing. ECU’s role in active ulnar deviation (in addition to wrist extension) and resisting radial deviation compared to ECRB may explain this.
This study is the first to analyse the EMG activity of ECU in the golf swing. Despite lead sided injuries being more common, it would appear that the trail side has greater peak activity during the downswing and at impact, which is when the club is at its highest velocity. Additional analysis of the lead and trail wrist kinematics demonstrated statistically different movement patterns in all three phases of the swing. With consideration of the ECU musculotendinous function, there appears to be a lower speed of movement of the lead wrist in both extension/flexion and ulnar/radial deviation compared to the trail wrist during the downswing and around the time of impact. It is possible that this movement pattern represents more isometric/eccentric ECU tendon load in comparison to the trail wrist and therefore may partially explain the asymmetrical injury pattern seen clinically. Other movement pattern factors such as the position and movement of forearm rotation (pronation/supination) that are permitted or prevented by the position of the elbow may also influence ECU activity. Previous studies have demonstrated that the lead wrist goes through a greater range of movement in the ulnar/radial deviation direction throughout the golf swing compared to the trail wrist (Sweeney et al., Citation2012). This is likely to play an additive role in the asymmetrical nature of ECU tendon injury seen in elite golfers.
There was no correlation between the performance characteristics of the golf swing (i.e., clubhead speed, angle of attack or swing direction) and the work done by the ECU muscle on either the trail or lead arm. Expert clinical opinion has previously suggested that steep angles of attack may be related to wrist injuries, particularly in the lead wrist (Golf Fitness Magazine, Citation2008; Hand Surgery Specialists of Texas, Citation2019). If we consider ECU muscle activity as a surrogate marker of force through the ulnar side of the wrist, the findings from the present study may suggest that swing mechanics alone are not the only risk factor for injury to ECU during the golf swing. This EMG data builds on previous understanding of kinematics of the wrist during the swing. This study gives researchers a strong base by which to explore additional variables to understand injury patterns in the ECU tendon.
Despite the novel data that this study has provided, it must be interpreted in light of certain limitations. Firstly, the EMG sensors were placed transcutaneously and therefore not intramuscularly. This can affect the quality and variability of the EMG readings when considering body fat levels, body hair and sweat. However, shaving and meticulous cleaning of each participant’s skin was performed in this study in line with established protocols in an attempt to minimise these variabilities. Secondly, understanding wrist biomechanics in the golf swing can be challenging given the influence a golfer’s grip type (i.e. the way they hold the club) can have (Carson et al., Citation2019). Significant differences in wrist extension/flexion and internal/external rotation can be seen depending on how “strong” or “weak” one’s grip is. Such variations in grip may have led to influences in the EMG data gathered. Further, this data may not be generalisable to the entire golfing community as we have specifically looked at skilled “sub-elite” golfers. It is unlikely to be applicable to recreational, high handicap golfers given differences in technical variables in the golf swing being more likely to be relevant to other skilled players such as professional golfers.
In conclusion, lead and trail forearm ECU muscles have different levels of muscle activity during each phase of the swing. The differing wrist kinematics and associated muscle activity may contribute to the asymmetrical injury pattern seen clinically. Performance characteristics showed no relationship with muscle activity.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- af Ekenstam F. W., Palmer, A. K., & Glisson, R. R. (1984). The load on the radius and ulna in different positions of the wrist and forearm. A cadaver study. Acta orthopaedica Scandinavica, 55(3), 363–365. https://doi.org/10.3109/17453678408992375
- Bader, J., Boland, M. R., Greybe, D., Nitz, A., Uhl, T., & Pienkowski, D. (2018). Muscle activity during maximal isometric forearm rotation using a power grip. Journal of Biomechanics, 68, 24–32. https://doi.org/10.1016/j.jbiomech.2017.12.011
- Barrio Minton, C. A., & Lenz, A. S. (2019). Practical approachesto applied research and program evaluation for helping professions. Routledge.
- Bonifacio, D., Richards, J., Selfe, J., Curran, S., & Trede, R. (2018). Influence and benefits of foot orthoses on kinematics, kinetics and muscle activation during step descent task. Gait & Posture, 65, 106–111. https://doi.org/10.1016/j.gaitpost.2018.07.041
- Burkhart, T. A., & Andrews, D. M. (2010). Activation level of extensor carpi ulnaris affects wrist and elbow acceleration responses following simulated forward falls. Journal of Electromyography and Kinesiology: Official Journal of the International Society of Electrophysiological Kinesiology, 20(6), 1203–1210. https://doi.org/10.1016/j.jelekin.2010.07.008
- Carson, H. J., Collins, D., & Richards, J. (2014). Intra-individual movement variability during skill transitions: A useful marker? European Journal of Sport Science, 14(4), 327–336. https://doi.org/10.1080/17461391.2013.814714
- Carson, H. J., Collins, D., & Richards, J. (2016). Initiating technical refinements in high-level golfers: Evidence for contradictory procedures. European Journal of Sport Science, 16(4), 473–482. https://doi.org/10.1080/17461391.2015.1092586
- Carson, H. J., Richards, J., & Mazuquin, B. (2019). Examining the influence of grip type on wrist and club head kinematics during the golf swing: Benefits of a local co-ordinate system. European Journal of Sport Science, 19(3), 327–335. https://doi.org/10.1080/17461391.2018.1508504
- Farber, A. J., Smith, J. S., Kvitne, R. S., Mohr, K. J., & Shin, S. S. (2009). Electromyographic analysis of forearm muscles in professional and amateur golfers. The American Journal of Sports Medicine, 37(2), 396–401. https://doi.org/10.1177/0363546508325154
- Fedorcik, G. G., Queen, R. M., Abbey, A. N., Moorman III, C. T., & Ruch, D. S. (2012). Differences in wrist mechanics during the golf swing based on golf handicap. Journal of Science & Medicine in Sport / Sports Medicine Australia, 15(3), 250–254. https://doi.org/10.1016/j.jsams.2011.10.006
- Glazebrook, M. A., Curwin, S., Islam, M. N., Kozey, J., & Stanish, W. D. (1994). Medial epicondylitis. An electromyographic analysis and an investigation of intervention strategies. The American Journal of Sports Medicine, 22(5), 674–679. https://doi.org/10.1177/036354659402200516
- Golf Fitness Magazine. Getting a grip on wrist injuries: Golf channel. 2008 Available from: https://www.golfchannel.com/article/golf-fitness-magazine/getting-grip-wrist-injuries#:~:text=A%20steep%20angle%20of%20attack,damage%20the%20tendons%20and%20muscles.
- Hand Surgery Specialists of Texas. Golf injuries to the hand and wrist. 2019 [ Available from: https://carpaltunnelpros.com/2019/10/23/golf-injuries/.
- Hawkes, R., Connor, P., & Campbell, D. (2013). The prevalence, variety and impact of wrist problems in elite professional golfers on the European Tour. Bri Journal Sports Medicine, 47(17), 1075. https://doi.org/10.1136/bjsports-2012-091917
- Hermens, H. J., & Workshop, G. S. (1998). Surface electromyography: Application areas and parameters. Proceedings of the Third General SENIAM Workshop, Aachen, Germany.
- Manivasagam, K., & Yang, L. (2022). Evaluation of a New simplified inertial sensor method against electrogoniometer for measuring wrist motion in occupational studies. Sensors (Basel), 22(4), 1690. https://doi.org/10.3390/s22041690
- Markolf, K. L., Dunbar, A. M., & Hannani, K. (2000). Mechanisms of load transfer in the cadaver forearm: Role of the interosseous membrane. The Journal of Hand Surgery, 25(4), 674–682. https://doi.org/10.1053/jhsu.2000.8640
- Markolf, K. L., Lamey, D., Yang, S., Meals, R., & Hotchkiss, R. (1998). Radioulnar load-sharing in the forearm. A study in cadavera. The Journal of Bone and Joint Surgery American Volume, 80(6), 879–888. https://doi.org/10.2106/00004623-199806000-00012
- Mogk, J. P., & Keir, P. J. (2003). The effects of posture on forearm muscle loading during gripping. Ergonomics, 46(9), 956–975. https://doi.org/10.1080/0014013031000107595
- Murray, A., Junge, A., Robinson, P. G., Bizzini, M., Bossert, A., Clarsen, B., Coughlan, D., Cunningham, C., Drobny, T., Gazzano, F., Gill, L., Hawkes, R., Hospel, T., Neal, R., Lavelle, J., Scanlon, A., Schamash, P., Thomas, B., Voight, M., … Dvorak, J. (2020). International consensus statement: Methods for recording and reporting of epidemiological data on injuries and illnesses in golf. British Journal of Sports Medicine, 54(19), 1136–1141. https://doi.org/10.1136/bjsports-2020-102380
- NHS Scotland. NHS Inform. Self-help guide: Coronavirus (COVID-19). 2020 [ Available from: https://www.nhsinform.scot/self-help-guides/self-help-guide-coronavirus-covid-19.
- Pataky, T. C., Robinson, M. A., & Vanrenterghem, J. (2013). Vector field statistical analysis of kinematic and force trajectories. Journal of Biomechanics, 46(14), 2394–2401. https://doi.org/10.1016/j.jbiomech.2013.07.031
- Richards, J., Thewlis, D., Selfe, J., Cunningham, A., & Hayes, C. (2008). A biomechanical investigation of a single-limb squat: Implications for lower extremity rehabilitation exercise. Journal of Athletic Training, 43(5), 477–482. https://doi.org/10.4085/1062-6050-43.5.477
- Robinson, P. G., Murray, I. R., & Duckworth, A. D. (2019). Systematic review of musculoskeletal injuries in professional golfers. British Journal of Sports Medicine, 53(1), 13–18. https://doi.org/10.1136/bjsports-2018-099572
- Robinson, M. A., Vanrenterghem, J., & Pataky, T. C. (2015). Statistical parametric mapping (SPM) for alpha-based statistical analyses of multi-muscle EMG time-series. Journal of Electromyography and Kinesiology: Official Journal of the International Society of Electrophysiological Kinesiology, 25(1), 14–19. https://doi.org/10.1016/j.jelekin.2014.10.018
- Shah, D. S., Middleton, C., Gurdezi, S., Horwitz, M. D., & Kedgley, A. E. (2017). The effects of wrist motion and hand orientation on muscle forces: A physiologic wrist simulator study. Journal of Biomechanics, 60, 232–237. https://doi.org/10.1016/j.jbiomech.2017.06.017
- Sorbie, G. G., Darroch, P., Grace, F. M., Gu, Y., Baker, J. S., & Ugbolue, U. C. (2017). Commercial golf glove effects on golf performance and forearm muscle activity. Research in Sports Medicine, 25(4), 451–461. https://doi.org/10.1080/15438627.2017.1365291
- Sorbie, G. G., Hunter, H. H., Grace, F. M., Gu, Y., Baker, J. S., & Ugbolue, U. C. (2016). An electromyographic study of the effect of hand grip sizes on forearm muscle activity and golf performance. Research in Sports Medicine, 24(3), 222–233. https://doi.org/10.1080/15438627.2016.1191492
- Sweeney, M., Mills, P., & Mankad, A. (2012). Wrist kinematics during the golf drive from a bilaterally anatomical perspective. Proceedings of the 30th Conference of the International Society of Biomechanics in Sport, Melbourne, Australia.
- Turner, J., Forrester, S. E., Mears, A. C., & Roberts, J. R. (2020). Reliability of repeat golf club testing sessions with modified club moment of inertia. Sports Engineering, 23(1), 8. https://doi.org/10.1007/s12283-020-0320-7