
Abstract
Implants are commonly used as a replacement for damaged tissue. Many implants, such as pacemakers, chronic electrode implants, bone screws, and prosthetic joints, are made of or contain metal. Infections are one of the difficult to treat complications associated with metal implants due to the formation of biofilm, a thick aggregate of extracellular polymeric substances (EPS) produced by the bacteria. In this study, we treated a metal prosthesis infection model using a combination of ciprofloxacin-loaded temperature-sensitive liposomes (TSL) and alternating magnetic fields (AMF). AMF heating is used to disrupt the biofilm and release the ciprofloxacin-loaded TSL. The three main objectives of this study were to (1) investigate low- and high-temperature-sensitive liposomes (LTSLs and HTSLs) containing the antimicrobial agent ciprofloxacin for temperature-mediated antibiotic release, (2) characterise in vitro ciprofloxacin release and stability and (3) study the efficacy of combining liposomal ciprofloxacin with AMF against Pseudomonas aeruginosa biofilms grown on metal washers. The release of ciprofloxacin from LTSL and HTSL was assessed in physiological buffers. Results demonstrated a lower transition temperature for both LTSL and HTSL formulations when incubated in serum as compared with PBS, with a more pronounced impact on the HTSLs. Upon combining AMF with temperature-sensitive liposomal ciprofloxacin, a 3 log reduction in CFU of Pseudomonas aeruginosa in biofilm was observed. Our initial studies suggest that AMF exposure on metal implants can trigger release of antibiotic from temperature sensitive liposomes for a potent bactericidal effect on biofilm.
Introduction
Metallic implants have been used extensively in orthopaedic procedures and infections of these implants are a tremendous burden for individual patients as well as for the global health care system. For example, every year in the US, hundreds of thousands prosthetic joint replacement procedures are performed due to degenerative joint disease. Unfortunately, approximately 1–2% of all prosthetic joint replacements become infected [Citation1,Citation2]. The rapidly increasing number of joint replacements that are projected due to population trends is expected to translate into hundreds of thousands of infected joints per year by 2030 [Citation1]. The projected total annual cost to treat patients with PJIs in the US in 2020 is about $1.6 billion [Citation3,Citation4]. Multiple surgeries are usually required including replacement of the infected joint along with prolonged antibiotic administration, adding significant costs to the healthcare system [Citation5]. Antibiotic therapy in patients with infected metal implants is often challenging because the efficacy of antibiotics is severely hampered by the formation of biofilm on the surface of the metal implant. Biofilm is comprised of aggregates of bacteria bound within extracellular polymeric substances (EPS) which protect these pathogens from both antimicrobial agents and the host immune response, rendering them much more resistant to antimicrobial killing than planktonic bacteria [Citation6]. In the case of infected prosthetic joints, biofilm-associated infections can typically only be treated by additional surgery [Citation5] including replacement of the affected implant [Citation7]. Different treatment methods have been studied for combating biofilms include electrical current [Citation8], shock waves [Citation9], photodynamic therapy [Citation10] and magnetic field exposure [Citation11]. Richardson et al. [Citation12] studied heat treatment of infected haemodialysis catheters and showed that treating with heat in the presence of antibiotics led to additive killing of Staphylococcus epidermidis, Staphylococcus aureus and Klebsiella pneumoniae. Kim et al. [Citation13] has developed antimicrobial magnetic thermotherapy to treat Staphylococcus aureus biofilms. Pavlovsky et al. [Citation14] has shown that exposure of the Staphylococcus epidermidis bacterial biofilm to local temperature treatment can weaken the mechanical integrity of the biofilm. O’Toole et al. [Citation15] studied the thermal mitigation of Pseudomonas aeruginosa biofilms and found the thermal shock can reduce the populations of Pseudomonas aeruginosa biofilms by six orders of magnitude at temperatures not exceeding 80 °C.
A non-invasive approach for the treatment of biofilm on metal implants can be achieved through the use of high-frequency (>100 kHz) alternating magnetic fields (AMF). When metals are exposed to high-frequency AMF, electrical currents induced on their outer surface, result in rapid heating which can destroy the biofilm. Since this method of treatment is highly selective to biofilms, it would likely be most effective when combined with traditional antimicrobials to achieve complete treatment. AMF heating has been investigated previously as a means to treat tumours through direct injection of magnetic nanoparticles [Citation16], as a means of direct tissue heating [Citation17] or as a means of triggering a change in the shape of a shape-memory alloy within the body [Citation18]. Recently, Coffel et al. [Citation19] described the possibility of using AMF exposures on implants coated with a ferromagnetic nanoparticle to generate heating to treat biofilms, although direct heating of metals may not need these coatings. In a recent study, we reported the safety of using AMF exposure to eradicate biofilm on a metal surface, methods to achieve uniform heating of a prosthetic joint and in vivo methods to assess the extent of thermal damage to surrounding tissues after an AMF exposure [Citation4].
Our recent study also shows the successful treatment in vitro of Pseudomonas aeruginosa (PAO1) and Staphylococcus aureus biofilms grown on metals using high-frequency alternating magnetic fields (AMF) [Citation4]. It was observed that a 4–5 log reduction in bacterial count (measured as colony forming units (CFU)) could be achieved within 5–7 min of heat treatment (20 W of power) when Pseudomonas aeruginosa or Staphylococcus aureus biofilms were grown on metal washers [Citation4]. This study also revealed a potential synergistic relationship between the antimicrobial ciprofloxacin and AMF exposures in the treatment of P. aeruginosa biofilms. In this study, we explored the potential of achieving local delivery of ciprofloxacin to the site of infection using a temperature-sensitive liposome (TSL) carrier. Previously developed TSLs encapsulating the chemotherapeutic agent doxorubicin have been shown to be capable of circulating in the bloodstream and locally releasing their contents when passing through a region of elevated temperature [Citation20–25]. Needham et al. reported the new lipid formulation containing doxorubicin and optimised for both mild hyperthermic temperatures (39–40 °C) [Citation26]. This liposome system was found to be significantly more effective than free drug or current liposome formulations in combination with mild hyperthermia [Citation26]. This group further studied and explained the effect of lipid composition on the thermal transition and doxorubicin release [Citation27].
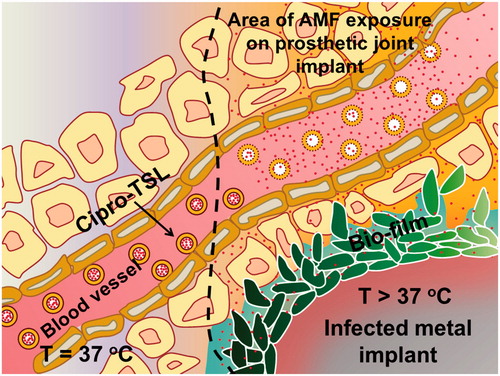
Since the proposed use of AMF exposures generates heating in the vicinity of an infected metal implant, a combined nanoparticle strategy might enable local delivery of high concentrations of ciprofloxacin directly at the site of infection, where a joint is heated using AMF (). Further, since the magnitude and gradient of temperatures achieved on metal implants exposed to AMF are quite distinct from soft-tissue hyperthermia, an opportunity exists to customise the lipid formulation of TSL to this type of heating. In this research, the release kinetics, serum stability and bacterial activity of ciprofloxacin-loaded TSLs in vitro with and without AMF exposure were characterised. Our initial studies can allow further development and optimisation of TSLs in combination with AMF exposures for localised treatment of infected metal implants.
Figure 1. Schematic of ciprofloxacin release from temperature sensitive liposomes (TSL) in the vicinity of an infected metal implant heated by exposure to alternating magnetic field (AMF).
Materials and methods
Chemicals
1,2-Dipalmitoyl-sn-glycerol-3-phosphocholine (DPPC), 1-stearoyl-2-hydroxyl-sn-glycero-3-phosphocholine (MSPC), N-(Carbonyl-methoxypolyethyleneglylcol-2000)–1,2-distearoyl-sn-glycerol-3-phosphoethanolamine sodium salt (DSPE-MPEG 2000) were purchased from Corden Pharma (Boulder, CO). Cholesterol was purchased from Sigma Aldrich. Ciprofloxacin HCl was obtained from Alfa Aesar. Pseudomonas aeruginosa (PAO1, ATCC BAA-47) was provided by the Greenberg Lab at UT Southwestern (Dallas, TX).
Synthesis of ciprofloxacin-loaded low temperature-sensitive liposomes (cipro-LTSL), high temperature-sensitive liposomes (cipro-HTSL) and PEGylated high temperature-sensitive liposomes (cipro-PEG-HTSL)
LTSL and HTSLs were prepared by hydration of phospholipid films followed by extrusion through a 400 and 200 nm pore size polycarbonate membrane filter. LTSL phospholipids films were prepared by dissolving DPPC, MSPC and DSPE-PEG in chloroform (2 ml) at a molar ratio of 85.3:9.7:5.0 (DPPC:MSPC:DSPE-PEG) [Citation28]. The total mass of the dried LTSL was 50 mg per lipid film. The HTSL lipid films were prepared by dissolving the cholesterol and DPPC in chloroform (2 ml) at a molar ratio of 2:8 (20% Chol DPPC). The total mass of lipids in dried HTSL was 20 mg per lipid film. The chloroform solvent was evaporated using a rotary evaporator at 40 °C and the resulting thin lipid films were kept overnight in a vacuum desiccator. Each of the dried LTSL and HTSL lipid films were hydrated using a 250 mM ammonium sulphate buffer (2 ml) at pH 2.5 (at 55 °C) and 600 mM ammonium sulphate buffer at pH 2.5 (at 55 °C), respectively. The hydrated lipid mixtures were extruded five times through 400 and 200 nm pore size polycarbonate filters, respectively, to yield unilamellar vesicles of liposome nanoparticles. Encapsulation of ciprofloxacin into LTSLs and HTSLs (1 mg of ciprofloxacin per 50 mg of lipids, concentration of ciprofloxacin solution 1 mg/ml, pH of the ciprofloxacin solution 4.2) was carried out actively using a pH gradient method described by Oh et al. [Citation29]. Samples were incubated at 37 °C for 1 h. Unencapsulated ciprofloxacin was removed using a PD-10 size exclusion column (eluted using phosphate buffer solution) and by dialysis using 100 kDa membrane (0.9% sodium chloride dialysis buffer) in the LTSL and HTSL solutions, respectively.
A similar method was used to developed new cipro PEG-HTSL and it comprises DPPC, Cholesterol and DSPE-MPEG 2000 in a 56:36:5.07 molar ratio. The PEG-HTSL lipid films were prepared by dissolving the cholesterol, DSPE-MPEG and DPPC in chloroform (2 ml). The total mass of lipids in dried PEG-HT was 20 mg per lipid film. The chloroform solvent was evaporated using a rotary evaporator at 40 °C and the resulting thin lipid films were kept overnight in a vacuum desiccator. Dried lipid films were hydrated using a 600 mM ammonium sulphate buffer at pH 2.5 (at 55 °C). The hydrated lipid mixture was extruded five times through 400 and 200 nm pore size polycarbonate filters respectively to yield unilamellar vesicles of liposome nanoparticles. Encapsulation of ciprofloxacin into PEG-HTSL (1 mg of ciprofloxacin per 50 mg of lipids) was carried out actively using a pH gradient method. Samples were incubated at 37 °C for 1 h. Unencapsulated ciprofloxacin was removed by dialysis using 100 kDa membrane (0.9% sodium chloride dialysis buffer).
LTSL and HTSL size, zeta potential and ciprofloxacin loading analysis
LTSL and HTSL nanoparticles were characterised for size and zeta potential using a dynamic light scattering (DLS) instrument (Zetasizer Nano ZS, Malvern, UK). Electron microscopy analysis was performed on a transmission electron microscope (Tecnai G2 Spirit, FEI, Hillsboro, OR) equipped with a Gatan camera operating at 120 kV with Digital Micrograph software to determine the morphology and the size of the aqueous dispersion of liposome nanoparticles. Ciprofloxacin concentrations were determined by using a filter-based multi-mode microplate reader (FLUOstar Omega, BMG LABTECH, Germany) employing an excitation wavelength of 355 nm and an emission wavelength of 460 nm. Encapsulation efficiency was measured using a total phosphorus assay [Citation29], by computing the ratio of drug:phospholipds in pre- and post-column-purified samples as given below.
Ciprofloxacin concentration was determined by using fluorometry.
Where C1 is ciprofloxacin concentration of ciprofloxacin-loaded liposome after being passed through the column/dialysis and C2 is ciprofloxacin concentration of ciprofloxacin-loaded liposome before passed through the column/dialysis. P1 and P2 are phospholipid concentrations after and before passed through the column/dialysis [Citation29].
Ciprofloxacin release from LTSLs and HTSLs
The stability of liposome solutions was assessed by measuring release of encapsulated ciprofloxacin from LTSLs and HTSLs as a function of temperature (25–45 °C) and time in vitro in phosphate buffered saline (PBS) and 10% Fetal Bovine Serum (FBS). For the ciprofloxacin release measurements, samples were diluted 300-fold in PBS and FBS, and placed in a quartz cuvette equipped with a magnetic stirrer. A Cary Eclipse Fluorescence Spectrometer (Agilent Technologies, Santa Clara, CA) equipped with an external temperature controller (Cary Temperature Controller) and a temperature probe (Cary Temperature Probe Series II) that sat inside the cuvette, in contact with the sample, was used to measure ciprofloxacin release from the LTSLs and HTSLs. Ciprofloxacin release was assessed by excitation at 320 nm and fluorescence emission was monitored at 420 nm at a heating rate of 1 °C per minute from 25 to 42 °C for LTSL and 37–80 °C for HTSL.
Ciprofloxacin release kinetics
To measure ciprofloxacin release as a function of time at a constant temperature, kinetic experiments were performed. For fluorescence measurements, samples were equilibrated to the desired temperature for 2 min. Baseline fluorescence measurements for each sample were taken at 25 °C and complete release was determined by adding 1% Triton X-100 to each sample using Cary Eclipse Fluorescence Spectrometer. Drug release based on fluorescence quantification at a given time (t) under constant temperature exposure was determined using the equation below:
where Fo represented the initial fluorescence intensity of the sample at 25 °C, and Ft is its intensity at time (t) at a predetermined temperature. Fm represented the fluorescence intensity of completely released ciprofloxacin with Triton X-100. Data were obtained as percentage release of encapsulated ciprofloxacin at a given temperature.
In vitro studies
Biofilms were grown on stainless steel washers (Alloy 316, P/N 91525A107, McMaster-Carr, Elmhurst, IL) with the gram-negative pathogen Pseudomonas aeruginosa (PAO1, ATCC BAA-47) P. aeruginosa is the most prevalent cause of PJI among gram-negative bacteria [Citation30]. An isolated colony of PAO1 was inoculated into 3 ml of cation adjusted Mueller Hinton II (MH II) media (212322, Becton Dickinson, Franklin Lakes, NJ). The culture was incubated for 18 h at 37 °C in a shaking incubator operating at 220 RPM. After 18 h, a working solution was created by adding 20 μl of the starting culture into 50 ml of MH II to obtain an approximate bacterial concentration of 5 × 105 CFU/ml. A biofilm was produced by placing an autoclaved stainless steel washer in a 50 ml centrifuge tube along with 4 ml of the working solution, and incubating in a shaking incubator at 110 RPM for 18 h at 37 °C. Then the infected metal washers were transferred into 50 ml centrifuge tubes containing 4 ml PBS. 0.01 mg/ml liposomal ciprofloxacin LTSL and HTSL (1600 µl: 8 × MIC (MIC =0.5 µg/ml)) and 1600 µl of 0.01 mg/ml ciprofloxacin (control) were added into above centrifuge tubes. Two tubes were used as control samples without adding any ciprofloxacin. Next, the tubes were placed in the centre of a solenoid coil and exposed to 20 W AMF for 3 and 5 min for LTSL and HTSL, respectively. The exposure times were chosen to achieve complete release from each TSL formulation. Control LTSL and HTSL samples were kept without any AMF exposure. The resulting control and exposed samples were maintained at room temperature for 2 h. Then, the exposed and other control washers were transferred into another 50 ml centrifuge tube containing 4 ml PBS and sonicated for 10 min in order to dislodge bacteria into suspension. Finally, serial dilutions (10−6) were done for all the bacterial solutions in the above steps and plating was performed for all samples and incubated for 18 h at 37 °C to quantify colony forming units (CFU).
Scanning electron microscopy (SEM) analysis of biofilms
The surface of the stainless steel washers with P. aeruginosa biofilms was imaged with SEM to evaluate the effect of cipro-LTSL and AMF exposures on bacteria and biofilm. Imaging was performed on washers treated with cipro-LTSL and AMF exposures. A control washer with biofilm but no treatment of cipro-LTSL and AMF exposure, a control washer with biofilm with treatment of cipro-LTSL and a blank washer with no biofilm were also imaged for comparison. Biofilm was grown on the washers and then the washers were carefully transferred from their growth media into a 4 ml solution of PBS, and were rinsed in 4 ml of 0.1 M sodium cacodylate buffer three times, and fixed for 22 h in a 4 ml solution comprised of 2% glutaraldehyde, 2% paraformaldehyde in a 0.1 M sodium cacodylate buffer (pH 7.4). After three rinse steps, the samples were then fixed in 4 ml of 2% osmium tetroxide in 0.1 M sodium cacodylate buffer for 2 h. The fixed washers were rinsed with 4 ml of deionised water five times and dehydrated at room temperature in seven steps by placing the washers for 5 min in 4 ml of 50, 70 (twice), 85, 95 (twice) and 100% ethanol, respectively. The washers were then transferred into 4 ml of 25, 50, 75 and 100% (twice) hexamethyldisilazane (HMDS) in ethanol, respectively for 15 min. Finally, the samples were left to dry for 24 h in a fume cupboard. This sample preparation protocol has been described previously for SEM imaging of biofilms [Citation31]. The dried specimens were mounted on aluminium stubs, sputter coated with gold/palladium and examined using the scanning electron microscope operating at 5 kV (Zeiss ΣIGMA VP Field Emission Scanning Electron Microscope, Carl Zeiss Microscopy Ltd., Cambridge, UK) [Citation4].
Results
Size, stability and encapsulation efficiency of ciprofloxacin loaded LTSL and HTSL
) shows the large unilamellar vesicles of ciprofloxacin loaded LTSL and HTSL nanoparticles (arrow indicates liposomes). The hydrodynamic diameter of LTSL and HTSL nanoparticles measured using DLS in MQ water was 153.00 ± 56.50 nm (n = 3) and 185.00 ± 64.00 nm (n = 3) respectively (, ). The polydispersity index of LTSL and HTSL nanoparticles in MQ water was 0.13 ± 0.03 and 0.07 ± 0.03, respectively, and indicates homogeneous liposome nanoparticle suspension (). The stability of LTSL and HTSL was checked in Milli-Q (MQ) water by measuring the zeta potential and the values were −40.22 ± 1.96 and −43.03 ± 2.46 mV, respectively (). The magnitude of the zeta potential indicates the degree of electrostatic repulsion between adjacent, similarly charged particles in dispersion. Higher negative value indicates that original ciprofloxacin loaded nanoparticle dispersions are highly stable in the medium and electrically stabilised. Active loading of ciprofloxacin by a transmembrane pH gradient yielded a maximum encapsulation efficiency of ∼95% in LTSLs and HTSLs. Encapsulation efficiencies were calculated as the ciprofloxacin/phospholipid ratio after passing through the PD-10 column (or dialysis) divided by the ciprofloxacin/phospholipid ratio before passing through the PD-10 column (or dialysis). The efficiency of ciprofloxacin encapsulation by remote loading was observed to be dependent on the pH of the bulk external medium. shows that the fraction of encapsulated ciprofloxacin increased from pH 5.5 to 7.0. The highest loading efficiency achieved was 97% of the added drug and was observed when the external pH was adjusted to pH 7.0. When the external pH was adjusted greater than 7.5, precipitation of ciprofloxacin was observed, and encapsulation efficiency dropped by 30%. The pH 7.0 medium was used for ciprofloxacin loading into both LTSL and HTSL.
Figure 2. TEM images of (A) LTSL and (B) HTSL nanoparticles loaded with ciprofloxacin (arrow indicates liposomes) and size distribution curve of (C) LTSL and (D) HTSL measured with MQ water and (E) pH dependence of ciprofloxacin encapsulation by remote loading in LTSL nanoparticle in PBS.
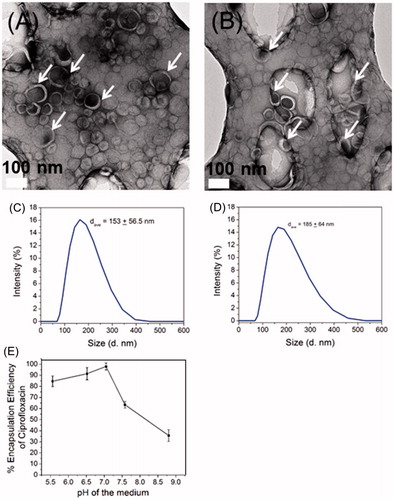
Table 1. Composition, drug/lipid ratio, size (in MQ water and ammonium sulphate buffer), polydispersity index and zeta potential (in MQ water) of ciprofloxacin loaded LTSL, HTSL and PEG-HTSL (n = 3).
Thermoscan and kinetics of ciprofloxacin release from LTSLs
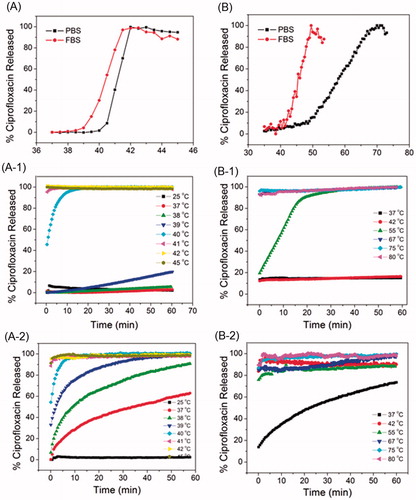
shows the percentage of ciprofloxacin released from LTSL in PBS and FBS as a function of temperature. Ciprofloxacin release was very minimal (<5%) at 37–40 °C in PBS and 37–39 °C in FBS. LTSLs begin to exhibit release of ciprofloxacin above 40 °C in PBS and 39 °C in FBS. In both media, complete ciprofloxacin release (> 95%) from the LTSL is achieved by 41–42 °C. Overall, ciprofloxacin release was greater in FBS between 39 and 41 °C compared to the ciprofloxacin release from LTSL in PBS (). Ciprofloxacin LTSL release as a function of time (for different fixed temperature levels) is shown in . represents the ciprofloxacin release from LTSL in PBS and FBS, respectively. In general, between 37–39 °C release was <10%, and up to 20% release was observed at 39 °C for samples in PBS after 60 min. The thermal scans also show ciprofloxacin release is greater when LTSL nanoparticles are incubated in FBS as compared with PBS, and significant leakage of ciprofloxacin from LTSL was observed at body temperature in FBS. Rapid release of ciprofloxacin from LTSL was observed in FBS at 37–39 °C compared to the PBS and approximately 60, 90 and 95% of ciprofloxacin had been released after 60 min. Within 10 min of incubation in FBS, most of the trapped ciprofloxacin (>90%) was released at 41 °C in both PBS and FBS. More interestingly within the first 5 min, complete release of ciprofloxacin was observed for ciprofloxacin loaded LTSL in PBS and FBS after 42 °C.
Figure 3. Thermoscan assay of ciprofloxacin loaded (A) LTSL (B) HTSL in PBS and FBS, ciprofloxacin release kinetics of LTSL in (A-1) PBS and (A-2) FBS and ciprofloxacin release kinetics of HTSL in (B-1) PBS and (B-2) FBS.
Thermoscan and kinetics of ciprofloxacin release from HTSLs
shows the percentage of ciprofloxacin release from HTSL in PBS and FBS as a function of temperature. Ciprofloxacin release was minimal (<20%) at 37–45 °C in PBS and FBS (). HTSLs show more rapid release of ciprofloxacin in FBS as compared to PBS. Similar trends were observed for ciprofloxacin LTSL samples in FBS. A greater rate of leakage of ciprofloxacin from HTSL was observed at body temperature in FBS. In FBS, maximum ciprofloxacin release from HTSL is observed (>95%) at 50 °C (). But the same HTSLs show a maximum release of ciprofloxacin at 68 °C in PBS, representing a much higher difference compared with the LTSL described above. This release difference in FBS and PBS for same HTSL is due to the interaction of serum components with HTSL nanoparticles [Citation32,Citation33]. A similar ciprofloxacin release trend was observed in a time-release kinetic study (. represents the ciprofloxacin release from HTSL in PBS and FBS, respectively. In general, between 37–42 °C release was <20% for HTSL until 60 min in PBS. HTSL shows rapid release of ciprofloxacin in PBS above 55 °C. In contrast significant leakage of ciprofloxacin from the HTSL was observed at body temperature in FBS with release >60% after 60 min. As observed in the release kinetics of LTSLs, the stability of ciprofloxacin HTSLs is dependent on the medium it is incubated in, however, this formulation showed a greater sensitivity.
Size and stability of ciprofloxacin loaded LTSL, HTSL and PEG-HTSL in 10% FBS
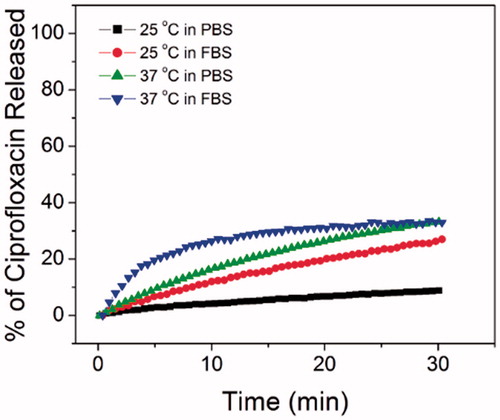
In this study, 10% FBS diluted in PBS was used for thermoscan and kinetic studies of liposomal ciprofloxacin. The size of the LTSL and HTSL nanoparticles in 10% FBS medium was 90.89 ± 4.13 and 105.72 ± 5.17 nm, respectively. Here we observed the shrinkage of the liposomal ciprofloxacin nanoparticles in 10% FBS compared to the original size of nanoparticles. In addition, changes in zeta potential were observed upon exposing liposomes to serum. Zeta potential values of serum exposed LTSL and HTSL was 6.89 ± 8.64 and −8.27 ± 5.75 mV, respectively. Serum induced change in liposome size and stability was studied before and it is due to the protein corona surrounding the particles [Citation34]. Osmotic pressure is generated by proteins that are impermeable to liposome membrane and cause water to escape from the liposome core and subsequent shrinking of the vesicle [Citation34]. Hioki et al. [Citation35] studied the in vitro doxorubicin release assay of PEGylated liposome using bovine serum albumin (BSA) at high temperature and compared with non-PEGylated liposome. They observed more stability in drug release for PEGylated formulation in serum compared to non-PEGylated liposome. PEG molecules immobilised on the surface of PEGylated liposomes can prevent the direct interaction of BSA with liposomes. Therefore, we have formulated a new cipro-HTSL (PEG-HTSL) lipid composition by incorporating PEG molecules in to HTSL and in vitro serum stability was checked at 25 and 37 °C. The hydrodynamic diameter of PEG-HTSL nanoparticles measured using DLS in MQ water was 192.81 ± 2.88 nm (n = 7). The polydispersity index of nanoparticles in MQ water was 0.11 ± 0.04 and indicates homogeneous liposome nanoparticle suspension. The size of the PEG-HTSL nanoparticles in 10% FBS medium was 150.73 ± 1.50 nm. The stability of the new HTSL was checked in MQ water by measuring the zeta potential and the value is −34.69 ± 2.78 mV. Zeta potential value of serum exposed PEG-HTSL was −4.15 ± 3.81 mV which is due to interaction of liposome nanoparticles with serum components. PEG-HTSL still shows () leakage of ciprofloxacin in both PBS and FBS at 37 °C, but a reduced rate compared to the HTSL. In 30 min, ciprofloxacin release was 30% for both medium at 37 °C. HTSL shows about 55% ciprofloxacin release at 30 min in FBS and less than 20% release in PBS at 37 °C. Incorporating PEG into HTSL lipid somewhat improved the serum stability at 37 °C compared to the non-PEG-HTSL.
Figure 4. Ciprofloxacin release kinetics of PEG-HTSL in PBS and FBS at 25 and 37 °C.
Temperature and ciprofloxacin release kinetics study during AMF exposure
An experimental apparatus comprised of a solenoid coil with the capability to expose biofilm-coated metal washers to an AMF was developed as a model system for the concept of treating infected metal implants through induction heating [Citation4]. A schematic and photograph of the experimental solenoid coil is shown in . For the setup, the maximum power delivered to the coil was 20 W. The 50 ml centrifuge tubes containing stainless steel washers in PBS (4 ml) were inserted into the solenoid such that the washers were located at the centre of the coil. The AMF inside the coil generated eddy currents on the washer, which in turn resulted in heating across its surface. In our previous study, the fibre optic temperature measurements were performed to characterise the magnitude and rate of heating of the washers when 20 W of power was delivered to the solenoid [Citation4]. The washer was placed in a 50 ml centrifuge tube with 4 ml of Dulbecco’s phosphate-buffered saline (DPBS, D8537, Sigma Aldrich) at room temperature, and the tube was inserted into the coil. The temperature of the washer was recorded at a rate of 1 Hz during a 10 min AMF exposure during heating and cooling back to room temperature. The measurements were repeated three times to evaluate the repeatability of the heating with the solenoid. Results of AMF exposures show a steady increase in the surface temperature until about 6 min, after which a steady state temperature of around 80 °C was reached [Citation4].
Figure 5. (A) Experimental solenoid coil, (B) ciprofloxacin release vs. time for LTSL and HTSL under 20 W AMF exposure, (C) ciprofloxacin release vs. washer temperature for LTSL and HTSL during AMF exposure (20 W). [A fibre optic temperature sensor (Neoptix Inc., Quebec, Canada) was attached to the top surface of a metal washer using a thermally conductive epoxy (ASTA, Arctic Silver Inc., Visalia, CA).] (D) The bactericidal effect of alternating magnetic field (AMF) exposures on biofilm-associated bacteria associated with a metal washer for cipro-LTSL and cipro-HTSL. This assay demonstrates that the cipro-LTSL and HTSL keeps the antibiotic encapsulated until activated with heat from AMF.
![Figure 5. (A) Experimental solenoid coil, (B) ciprofloxacin release vs. time for LTSL and HTSL under 20 W AMF exposure, (C) ciprofloxacin release vs. washer temperature for LTSL and HTSL during AMF exposure (20 W). [A fibre optic temperature sensor (Neoptix Inc., Quebec, Canada) was attached to the top surface of a metal washer using a thermally conductive epoxy (ASTA, Arctic Silver Inc., Visalia, CA).] (D) The bactericidal effect of alternating magnetic field (AMF) exposures on biofilm-associated bacteria associated with a metal washer for cipro-LTSL and cipro-HTSL. This assay demonstrates that the cipro-LTSL and HTSL keeps the antibiotic encapsulated until activated with heat from AMF.](/cms/asset/af7c024a-227a-4a52-8a72-56cc2b60fdef/ihyt_a_1422028_f0005_c.jpg)
According to , LTSL and HTSL completely release ciprofloxacin at 42 and 67 °C, respectively in PBS. An experiment was conducted to measure ciprofloxacin release kinetics in PBS with a 20 W AMF exposure. Complete release of ciprofloxacin was observed after 3 and 5 min for LTSL and HTSLs respectively (). shows the percentage of ciprofloxacin released vs. washer temperature and demonstrates that the rate of ciprofloxacin release from the LTSL is greater than for the HTSL as expected. This is due to the rigid lipid membrane formed by cholesterol in HTSL. About 90% and 70% of ciprofloxacin was released from LTSL and HTSL, respectively, when the washer temperature is 60 °C. This demonstrates that washers need to be heated more than the phase transition temperature of TSL in order to get complete release of ciprofloxacin, likely due to the fact that there was a temperature gradient between the washer and the PBS in the setup.
In vitro studies
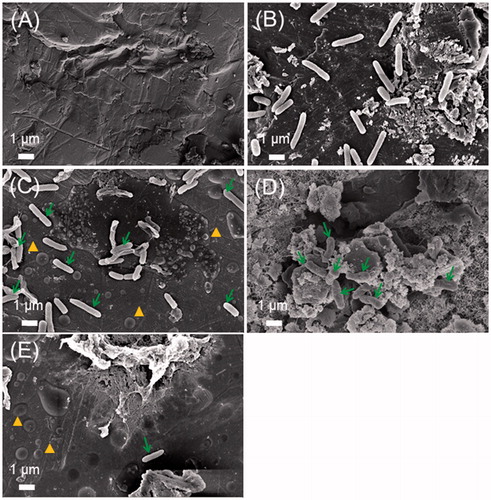
shows the CFU reduction across different treatment groups for Pseudomonas aeruginosa biofilm. The in vitro studies under the AMF exposure were performed at 3 and 5 min for LTSL and HTSL samples respectively, in order to achieve complete release of ciprofloxacin from the liposomes. When the control group is compared to the LTSL/HTSL groups with no exposure, the liposomes keep the antibiotic encapsulated resulting in only a minor reduction (p > 0.05) in CFU (probably due to remaining small fraction of free ciprofloxacin that wasn’t removed by dialysis in the preparation of the nanoparticles). The addition of free ciprofloxacin resulted in a 2–3 log reduction in CFU. The AMF exposure alone also resulted in a similar reduction in CFU. When the LTSL or HTSL nanoparticles were added to the sample and exposed to an AMF, a similar reduction in CFU was observed as compared to free ciprofloxacin (p > 0.05) indicating that the contents of the liposomes were fully released by the exposure. depicts scanning electron microscopy (SEM) images of biofilms on washers with and without cipro-LTSL and AMF treatment. Accumulation of liposomal ciprofloxacin on biofilm is very clear in compared to the control samples in (bare washer) and (18 h biofilm). Once activated, the liposome degrades and the ciprofloxacin is bioavailable and capable of achieving close to equivalent reduction in viable bacteria compared with free ciprofloxacin. Treatment of P. aeruginosa biofilm with encapsulated ciprofloxacin that was activated using AMF resulted in about 3-log reduction in bacterial biofilm, consistent with the effects of treating biofilm with unencapsulated antibiotic. shows the SEM image of biofilm treated with AMF. shows the SEM image of biofilm treated with both liposomal ciprofloxacin (LTSL) and AMF. It was difficult to detect any viable bacteria on this washer, and aggregates of biofilm material were visible on the washer surface. The unactivated LTSL and HTSL showed only a small reduction in viable bacteria compared to the untreated control. The implications for this observation are that the systemic circulation could be spared from unwanted exposure to high levels of ciprofloxacin if toxicity was a concern.
Figure 6. Scanning electron microscopy (SEM) images of the surface of a stainless steel washer showing the influence of both cipro-LTSL and AMF exposures on bacteria and biofilms. (A) a negative control sample – washer with no bacteria, (B) a positive control sample – washer with biofilm but no treatment of cipro-LTSL and AMF exposure, (C) a control sample – washer with biofilm but treatment of cipro-LTSL and no AMF exposure, (D) sample – washer with biofilm with treatment of AMF exposure and (E) sample – washer with biofilm with treatment of both cipro-LTSL and AMF exposure. It was difficult to find any viable bacteria on the washer (E), and aggregates of material were visible on the washer surface. (Arrow indicates bacteria and arrow head indicates cipro-LTSL).
Discussion
The objective of this study was to treat a metal implant infection model using a combination of ciprofloxacin-loaded temperature-sensitive liposomes (TSL) and alternating magnetic fields (AMF). AMF heating is used to disrupt the biofilm and release the ciprofloxacin-loaded TSL. In this study, we characterised the ability to trigger release of ciprofloxacin from TSL in the vicinity of a metal heated using an AMF. Temperature-triggered drug targeting by TSL has the advantage of being able to externally control drug release spatially and temporally by steering both heating focus and power [Citation20,Citation21]. Previously, ciprofloxacin loaded temperature sensitive liposomes were reported for the first time by Wardlow et al. [Citation28] and they demonstrated the triggered release of ciprofloxacin in vivo in muscle using mild heating generated with magnetic resonance-guided high-intensity focussed ultrasound (MR-HIFU). Ciprofloxacin loaded liposomes have also been widely studied for pulmonary administration [Citation36–40]. Previous in vitro and in vivo studies of antibiotic pharmacokinetics in bacterial biofilms have indicated that, biofilm bacteria are significantly more resistant than planktonic bacteria to antibiotic treatment and therefore, require a higher dose for a longer period of time [Citation7]. However, data on efficacy and toxicity with long-term antibiotic therapy for biofilm eradication are lacking [Citation41]. Encapsulation of ciprofloxacin in liposomes results in a prolonged circulation time and greatly increases the ciprofloxacin area under the concentration–time curve over conventional ciprofloxacin [Citation42]. The effect of TSL-encapsulated antimicrobials on biofilms has not been studied.
The thermal sensitivity of PAO1 appears to be higher than eukaryotic cells [Citation15]. Therefore, higher temperatures are likely required to achieve thermal eradication of bacteria residing on metal implants. Therefore, the optimal TSL formulation may require a higher transition temperature, which might also result in better serum stability. A more stable TSL with higher transition temperature (high temperature sensitive liposomes – HTSL) may provide improved systemic stability relative to LTSL as previously demonstrated [Citation28], and achieve better localisation in the body. One of the aims of this study was to develop more stable liposomes with higher transition temperatures and check its stability and release properties compared to low-temperature sensitive liposomes. Cholesterol is a hydrophobic molecule and preferentially interacts with the core of the membrane, thus stabilising it and stretching the transition temperature to higher values [Citation43]. Therefore, HTSL lipid formulation was developed using cholesterol.
The preliminary data for liposome nanoparticle characterisation suggest that the successfully synthesis of ciprofloxacin loaded LTSL, HTSL and PEG-HTSL below 200 nm with ∼95% encapsulation efficiency. Similar encapsulation efficiency was reported for ciprofloxacin loaded temperature sensitive liposomes using the pH gradient method [Citation28,Citation29]. We have studied the stability and release kinetics of LTSL and HTSL in both PBS and FBS. HTSL nanoparticles exhibited a high leakage rate in FBS compared with PBS, with a slight reduction in leakage when PEG was incorporated into the liposome. Serum-induced drug leakage from doxorubicin loaded liposomes has also been reported by Yang et al. [Citation32]. They observed the serum components accelerate the doxorubicin release from several different kinds of DOX-liposomes. This is due to the interaction between the liposomes and serum components, which caused leakage of the contents entrapped in the liposome. Also, the physical characteristics of drug loaded liposome particles are affected by serum and serum proteins. Serum proteins adsorb onto the surface of the liposomes and reduce the size of the liposome particles, which destabilise larger particles and lead to a rapid release of the internal contents [Citation32]. Hossann et al. also studied the influence of serum on TSL to identify the serum components which are responsible for increasing drug release [Citation33]. They have concluded that the use of plasma or serum is still inevitable to investigate stability and release properties of TSL formulations until all serum components have been identified that alter TSL integrity [Citation33].
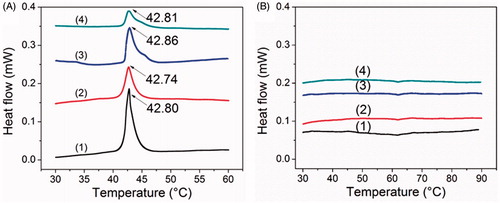
Differential scanning calorimetry studies (DSC) of LTSL and HTSL were performed in both PBS and 10% FBS using Differential Scanning Calorimeter (TA instruments, New Castle, DE). The LTSL formulations showed a distinct transition temperature (Tm) () in both PBS and 10% FBS. The Tm of LTSLs in PBS and 10% FBS had a similar sharp phase transition peaks around 42 °C. These results are comparable with Needham et al data. We have not observed considerable Tm change in LTSL due to the FBS. The HTSL formulations (20 mol% of cholesterol) did not show any sharp peak of transition around the Tm of DPPC (). The data seems to be in agreement with previous reports on DSC of DPPC-Cholesterol liposomes in which the sharp component of transition peak of DPPC was decreasing and a broad component instead of a sharp peak was observed with increasing cholesterol concentrations due to the transition of cholesterol-lipid units. The sharp peak of DPPC disappeared at 20 mol% of cholesterol [Citation44]. The co-operative gel to liquid crystalline phase transition also got eliminated with increasing cholesterol concentrations [Citation45]. De Smet et al. has developed Traditional Temperature-sensitive Liposomes (TTSL) with lipid composition DPPC:HSPC:Chol: DPPE-PEG (50:25:15:3) with ∼16 mol% of cholesterol and which shows Tm around 40.9 °C [Citation46]. This lipid composition is different compared to what we have prepared. Genz et al. further shows the broadening of DPPC-Cholesterol liposomes as the % of cholesterol increases in the lipid formulation [Citation44]. Therefore we will expect similar broadening for PEG-HTSL formulation since it contains 37 mol% of cholesterol and DSC was not performed for this formulation. Gaber et al. [Citation47] showed the effect of cholesterol on liposomes stability in both bovine serum and human plasma depend on the physical state of the lipid membranes. They have reported that addition of cholesterol to gel phase lipids destabilises the liposomes and increases the leakage of DOX in the presence of both bovine serum and human plasma [Citation47]. We have also observed the leakage of Cipro form cholesterol liposomes in the presence of FBS. However, DSC data of LTSL and HTSL in PBS and 10% FBS do not give clear scientific idea why this formulations show leakage of Cipro in FBS. Overall the stability of liposomal ciprofloxacin is dependent on the incubation medium.
Figure 7. DSC thermograms of (A-1) LTSL in PBS, (A-2) LTSL in FBS, (A-3) Cipro-LTSL in PBS, (A-4) Cipro-LTSL in FBS, (B-1) HTSL in PBS, (B-2) HTSL in FBS, (B-3) Cipro-HTSL in PBS and (B-4) Cipro-HTSL in FBS.
In vitro data demonstrates the 3 log reduction in CFU of Pseudomonas aeruginosa in biofilm upon combining AMF with temperature-sensitive liposomal ciprofloxacin. SEM images further support our objective of successfully eradication of biofilm using both AMF and Cipro-TSL nanoparticles.
Finally, some consideration must be paid to the safety and practicality of heating metal implants in the body using AMF. The magnitude and duration of heating will influence TSL release, but also potential thermal damage to surrounding soft tissues and bone. In the case of prosthetic joints, the integrity of the cement used to bond the implant to bone could be impacted by prolonged heating due to AMF. Further, the metal composition, surface finish and geometry of the implant will impact the extent to which it responds to AMF exposures. Some of these factors were explored in our recent paper [Citation4]. Pilot in vivo experiments suggest that short duration high temperature AMF exposures can be delivered safely. The release of cipro from TSLs under these types of exposures is a topic for future studies.
Overall, in this study, both HTSL and LTSL demonstrated equivalent bactericidal activity compared to free ciprofloxacin in in vitro biofilm studies. Serum-induced drug leakage from ciprofloxacin loaded LTSL and HTSL was greater at 37 °C compared to the ciprofloxacin release in PBS. The HTSL formulation exhibited less stability in serum compared to the LTSL. Incorporating PEG into HTSL lipid somewhat improved the serum stability at 37 °C compared to the non-PEG-HTSL. If HTSL/PEG-HTSL had more stability in serum, then this formulation could have some advantages related to the therapeutic index between heated and unheated tissues. Future research will assess the serum stability of LTSL and HTSL by changing the lipid composition and release kinetics and AMF exposure studies will be performed for biofilms on metal implants.
Conclusions
Initial in vitro data demonstrate that AMF exposure combined with temperature-sensitive liposomal ciprofloxacin can eradicate the bacteria in a biofilm. HTSL formulations exhibited a higher transition temperature upon the addition of cholesterol in the lipid membrane as compared with an LTSL formulation in PBS, but the transition temperature dropped significantly in more complex medium like serum. Furthermore, the CFU reduction offered by the LTSL and HTSL were similar to that of free ciprofloxacin indicating the ability to trigger free drug from the nanoparticle in a bioavailable format.
Acknowledgements
The authors acknowledge support from NIH 1R01CA199937 (Chopra) and the Oklahoma Center for the Advancement of Science & Technology (#HR17–060-1; Ranjan) for the personnel and supplies involved in this project. The authors also acknowledge the advice and guidance provided by the Electron Microscopy core facility at UT Southwestern Medical Center in acquiring the results presented in this manuscript.
Disclosure statement
The authors report no conflicts of interest.
References
- Tande AJ, Patel R. (2014). Prosthetic joint infection. Clin Microbiol Rev 27:302–45.
- Anguita-Alonso P, Hanssen AD, Patel R. (2005). Prosthetic joint infection. Expert Rev Anti Infect Ther 3:797–804.
- Kurtz SM, Lau E, Watson H, et al. (2012). Economic burden of periprosthetic joint infection in the United States. J Arthroplasty 27:61–5.e1.
- Chopra R, Shaikh S, Chatzinoff Y, et al. (2017). Employing high-frequency alternating magnetic fields for the non-invasive treatment of prosthetic joint infections. Sci Rep 7:7520.
- McConoughey SJ, Howlin R, Granger JF, et al. (2014). Biofilms in periprosthetic orthopedic infections. Future Microbiol 9:987–1007.
- Kasimanickam RK, Ranjan A, Asokan GV, et al. (2013). Prevention and treatment of biofilms by hybrid- and nanotechnologies. Int J Nanomed 8:2809–19.
- Song Z, Borgwardt L, Høiby N, et al. (2013). Prosthesis infections after orthopedic joint replacement: the possible role of bacterial biofilms. Orthop Rev (Pavia) 5:14.
- Del Pozo JL, Rouse MS, Patel R. (2008). Bioelectric effect and bacterial biofilms. A systematic review. Int J Artif Organs 31:786–95.
- Gnanadhas DP, Elango M, Janardhanraj S, et al. (2015). Successful treatment of biofilm infections using shock waves combined with antibiotic therapy. Sci Rep 5:17440.
- Biel MA, Photodynamic therapy of bacterial and fungal biofilm infections. In: Gomer JC, editor. Photodynamic therapy: methods and protocols. Totowa (NJ): Humana Press; 2010. p. 175–194.
- Bandara HMHN, Nguyen D, Mogarala S, et al. (2015). Magnetic fields suppress Pseudomonas aeruginosa biofilms and enhance ciprofloxacin activity. Biofouling 31:443–57.
- Richardson IP, Sturtevant R, Heung M, et al. (2016). Hemodialysis catheter heat transfer for biofilm prevention and treatment. ASAIO J 62:92–9.
- Kim MH, Yamayoshi I, Mathew S, et al. (2013). Magnetic nanoparticle targeted hyperthermia of cutaneous Staphylococcus aureus infection. Ann Biomed Eng 41:598–609.
- Pavlovsky L, Sturtevant RA, Younger JG, et al. (2015). Effects of temperature on the morphological, polymeric, and mechanical properties of Staphylococcus epidermidis bacterial biofilms. Langmuir 31:2036–42.
- O’Toole A, Ricker EB, Nuxoll E. (2015). Thermal mitigation of Pseudomonas aeruginosa biofilms. Biofouling 31:665–75.
- Giustini AJ, Petryk AA, Cassim SM, et al. (2010). Magnetic nanoparticle hyperthermia in cancer treatment. Nano Life 1.doi: 10.1142/S1793984410000067.
- Stauffer PR, Cetas TC, Jones RC. (1984). Magnetic induction heating of ferromagnetic implants for inducing localized hyperthermia in deep-seated tumors. IEEE Trans Biomed Eng 31:235–51.
- Buckley PR, Mckinley GH, Wilson TS, et al. (2006). Inductively heated shape memory polymer for the magnetic actuation of medical devices. IEEE Trans Biomed Eng 53:2075–83.
- Coffel J, Nuxoll E. (2015). Magnetic nanoparticle/polymer composites for medical implant infection control. J Mater Chem B 3:7538–45.
- Staruch R, Chopra R, Hynynen K. (2011). Localised drug release using MRI-controlled focused ultrasound hyperthermia. Int J Hyperthermia 27:156–71.
- Staruch RM, Hynynen K, Chopra R. (2015). Hyperthermia-mediated doxorubicin release from thermosensitive liposomes using MR-HIFU: therapeutic effect in rabbit Vx2 tumours. Int J Hyperthermia 31:118–33.
- Lokerse WJM, Kneepkens ECM, ten Hagen TLM, et al. (2016). In depth study on thermosensitive liposomes: optimizing formulations for tumor specific therapy and in vitro to in vivo relations. Biomaterials 82:138–50.
- Yeo SY, de Smet M, Langereis S, et al. (2014). Temperature-sensitive paramagnetic liposomes for image-guided drug delivery: Mn2+ versus [Gd(HPDO3A)(H2O)]. Biochim Biophys Acta 1838:2807–16.
- De Smet M, Heijman E, Langereis S, et al. (2011). Magnetic resonance imaging of high intensity focused ultrasound mediated drug delivery from temperature-sensitive liposomes: an in vivo proof-of-concept study. J Control Release 150:102–10.
- Grüll H, Langereis S. (2012). Hyperthermia-triggered drug delivery from temperature-sensitive liposomes using MRI-guided high intensity focused ultrasound. J Control Release 161:317–27.
- Needham D, Anyarambhatla G, Kong G, et al. (2000). A new temperature-sensitive liposome for use with mild hyperthermia: characterization and testing in a human tumor xenograft model. Cancer Res 60:1197–201.
- Needham D, Park JY, Wright AM, et al. (2013). Materials characterization of the low temperature sensitive liposome (LTSL): effects of the lipid composition (lysolipid and DSPE-PEG2000) on the thermal transition and release of doxorubicin. Faraday Discuss 161:515–34.
- Wardlow R, Bing C, VanOsdol J, et al. (2016). Targeted antibiotic delivery using low temperature-sensitive liposomes and magnetic resonance-guided high-intensity focused ultrasound hyperthermia. Int J Hyperthermia 32:254–64.
- Oh YK, Nix DE, Straubinger RM. (1995). Formulation and efficacy of liposome-encapsulated antibiotics for therapy of intracellular Mycobacterium avium infection. Antimicrob Agents Chemother 39:2104–11.
- Hsieh PH, Lee MS, Hsu KY, et al. (2009). Gram-negative prosthetic joint infections: risk factors and outcome of treatment. Clin Infect Dis 49:1036–43.
- Busetti A, Shaw G, Megaw J, et al. (2015). Marine-derived quorum-sensing inhibitory activities enhance the antibacterial efficacy of Tobramycin against Pseudomonas aeruginosa. Mar Drugs 13:1–28.
- Yang B, Geng SY, Wang JY. Physical stability of cholesterol derivatives combined with liposomes and their in vitro behavior. 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); 2013. p. 4114–17.
- Hossann M, Syunyaeva Z, Schmidt R, et al. (2012). Proteins and cholesterol lipid vesicles are mediators of drug release from thermosensitive liposomes. J Control Release 162:400–6.
- Wolfram J, Suri K, Yang Y, et al. (2014). Shrinkage of PEGylated and non-PEGylated liposomes in serum. Colloids Surf B Biointerfaces 114:294–300.
- Hioki A, Wakasugi A, Kawano K, et al. (2010). Development of an in vitro drug release assay of PEGylated liposome using bovine serum albumin and high temperature. Biol Pharm Bull 33:1466–70.
- Cipolla D, Wu H, Gonda I, et al. (2015). Aerosol performance and stability of liposomes containing ciprofloxacin nanocrystals. J Aerosol Med Pulm Drug Deliv 28:411–22.
- Serisier DJ, Bilton D, De Soyza A, et al. (2013). Inhaled, dual release liposomal ciprofloxacin in non-cystic fibrosis bronchiectasis (ORBIT-2): a randomised, double-blind, placebo-controlled trial. Thorax 68:812–7.
- Luiz B, Jim B, Igor G, et al. Treatment of Mycobacterium avium subsp hominissuis (MAH) lung infection with liposome-encapsulated ciprofloxacin resulted in significant decrease in bacterial load in the lung. New York (NY): American Thoracic Society; 2015. p. A6293.
- Norville IH, Hatch GJ, Bewley KR, et al. (2014). Efficacy of liposome-encapsulated ciprofloxacin in a murine model of Q fever. Antimicrob Agents Chemother 58:5510–18.
- Ong HX, Traini D, Cipolla D, et al. (2012). Liposomal nanoparticles control the uptake of ciprofloxacin across respiratory epithelia. Pharm Res 29:3335–46.
- Zimmerli W, Trampuz APE. (2004). Ochsner prosthetic-joint infections. N Engl J Med 351:1645–54.
- Ellbogen MH, Olsen KM, Gentry-Nielsen MJ, Preheim LC. (2003). Efficacy of liposome-encapsulated ciprofloxacin compared with ciprofloxacin and ceftriaxone in a rat model of pneumococcal pneumonia. J Antimicrob Chemother 51:83–91.
- Bozzuto G, Molinari A. (2015). Liposomes as nanomedical devices. Int J Nanomedicine 10:975–99.
- Genz A, Holzwarth JF, Tsong TY. (1986). The influence of cholesterol on the main phase transition of unilamellar dipalmytoylphosphatidylcholine vesicles. A differential scanning calorimetry and iodine laser T-jump study. Biophys J 50:1043–51.
- Bolean M, Simão AMS, Favarin BZ, et al. (2010). The effect of cholesterol on the reconstitution of alkaline phosphatase into liposomes. Biophys Chem 152:74–9.
- de Smet M, Langereis S, den Bosch SV, et al. (2010). Temperature-sensitive liposomes for doxorubicin delivery under MRI guidance. J Control Release 143:120–7.
- Gaber MH, Hong K, Huang SK, et al. (1995). Thermosensitive sterically stabilized liposomes: formulation and in vitro studies on mechanism of doxorubicin release by bovine serum and human plasma. Pharm Res 12:1407–16.