
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
There is debate within the literature as to whether emotion dysregulation (ED) in Attention-Deficit Hyperactivity Disorder (ADHD) reflects deviant attentional mechanisms or atypical perceptual emotion processing. Previous reviews have reliably examined the nature of facial, but not vocal, emotion recognition accuracy in ADHD. The present meta-analysis quantified vocal emotion recognition (VER) accuracy scores in ADHD and controls using robust variance estimation, gathered from 21 published and unpublished papers. Additional moderator analyses were carried out to determine whether the nature of VER accuracy in ADHD varied depending on emotion type. Findings revealed a medium effect size for the presence of VER deficits in ADHD, and moderator analyses showed VER accuracy in ADHD did not differ due to emotion type. These results support the theories which implicate the role of attentional mechanisms in driving VER deficits in ADHD. However, there is insufficient data within the behavioural VER literature to support the presence of emotion processing atypicalities in ADHD. Future neuro-imaging research could explore the interaction between attention and emotion processing in ADHD, taking into consideration ADHD subtypes and comorbidities.
Attention-deficit / hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterised by persistent and developmentally inappropriate levels of inattention, hyperactivity, and impulsivity (APA, Citation2013). When clinically diagnosed, individuals with ADHD display impaired functioning at school/ work, home and in social situations. The prevalence of a clinical ADHD diagnosis lies between 5 and 8% in children and adolescents (Polanczyk et al., Citation2014; Thomas et al., Citation2015), and 2.8% in adults (Fayyad et al., Citation2017). Although not included in the diagnostic criteria for ADHD, Emotion dysregulation (ED) is proposed to be a clinical feature of the disorder (Bunford et al., Citation2015; Graziano & Garcia, Citation2016; Shaw et al., Citation2014). ED is defined as an impaired ability to regulate an internal emotional state appropriately (D’Agostino et al., Citation2017), and is often conveyed through reactive anger, irritability, outbursts, and inordinate positive emotion (Bunford et al., Citation2015; Drechsler et al., Citation2020; Shaw et al., Citation2014). Evidence suggests ED is present in 25–45% of children, and 30–70% of adults diagnosed with ADHD (Shaw et al., Citation2014), a rate which is significantly higher than healthy adult controls (Barkley & Fischer, Citation2010). Furthermore, ED in ADHD is associated with increases in academic and social impairments (Bunford et al., Citation2015; Wehmeier et al., Citation2010), and an increased risk for the development of comorbidities, such as conduct disorder and depression (Steinberg & Drabick, Citation2015). Therefore, it is important to consider the underlying causes of ED in ADHD, and their implications for treatment.
Emotion dysregulation (ED) in ADHD is thought to arise from deficits in recognising and/or allocating attention to emotions (e.g. anger, happiness, sadness and fear), such as those from the face and voice (Shaw et al., Citation2014; Uekermann et al., Citation2010). However, there is debate in the literature as to the neurodevelopmental pathways which underpin these deficits (Shaw et al., Citation2014). Cognitive behavioural models of ADHD suggest ED stems from generic difficulties in allocating attention towards emotional expressions (Barkley, Citation1997; Nigg et al., Citation2005). Thus, these theories imply emotion recognition deficits and ED are secondary symptoms of core attention deficits in ADHD. Support for this view comes from research linking cognitive deficits in individuals with ADHD directly with emotion regulation difficulties (Fantozzi et al., Citation2021; Groves et al., Citation2020; Sjowall et al., Citation2013). Alternatively, socio-cognitive (Crick & Dodge, Citation1994), and motivational (Sonuga-Barke, Citation2005) theories of ADHD state ED may arise from specific deficits in interpreting emotions at a perceptual level (Borhani & Nejati, Citation2018). These theories suggest impaired perception of emotions may arise due to atypicalities in the bottom-up processes, which are necessary to perceive emotions. These bottom-up emotion processing atypicalities may be manifested behaviourally if an individual misinterprets emotional expressions or fails to understand the emotional significance of an expression. For example, incorrectly perceiving specific types of emotions, such as anger, in an emotional expression may lead to inappropriate hostile responses in social situations (Crick & Dodge, Citation1994). Similarly, not recognising the emotional significance of an incentive may result in a lack of motivation to behave appropriately (Sonuga-Barke, Citation2005). Finally, it is also possible that attentional and socio-cognitive mechanisms are not mutually exclusive, as perceptual processes, including attention, may be influenced by motivation-related processes (Crick & Dodge, Citation1994; Lemerise & Arsenio, Citation2000).
To add to the debate on the underpinnings of ED in ADHD, research can explore the nature of emotion recognition accuracy in ADHD using emotion recognition tasks. Typically, in emotion recognition tasks, participants with ADHD, and a typically developing (TD) control group are presented with facial and/or vocal expressions and are asked to label each expression with the correct emotion. Emotion types incorporated within emotion recognition tasks typically include at least anger and happiness, and several other emotions which consist of some or all of the other six basic emotion types (i.e. fearful, disgust, sadness and surprise), and a neutral expression. If participants with ADHD perform significantly worse on emotion recognition tasks, compared to TD participants, it can be concluded that individuals with ADHD present with emotion recognition deficits. In addition, research can explore the nature of emotion recognition deficits by analysing the pattern of errors participants display during emotion recognition tasks. A generic deficit is defined as a reduced ability to recognise all types of emotions in a random pattern, thought to arise from a general deviancy to allocate attention to emotional expressions. An emotion-specific deficit is defined as a consistent pattern of error towards one or several types of emotions. For example, an anger-specific deficit would arise if participants with ADHD consistently failed to recognise angry emotional expressions more than other emotion types (i.e. happiness) included in the task. Emotion-specific deficits may be indicative of an atypicality at the perceptual processing stage of emotion recognition, in support of socio-cognitive (Crick & Dodge, Citation1994) and motivational accounts (Sonuga-Barke, Citation2005), as a consistent pattern of error towards a specific emotion cannot be due to inattention alone.
To date, reviews have provided reliable evidence for the presence and nature of facial emotion recognition (FER), but not vocal emotion recognition (VER), deficits in individuals with ADHD (Bora & Pantelis, Citation2016; Borhani & Nejati, Citation2018; Collin et al., Citation2013; Cooper et al., Citation2020). For example, Bora and Pantelis (Citation2016) reported a reliable synthesised effect for the presence of FER deficits in ADHD, and further provided support for an emotion-specific deficit for negative facial expressions, such as anger and fear, in ADHD. This result is supported in various other reviews focusing only on FER deficits in ADHD (Borhani & Nejati, Citation2018; Collin et al., Citation2013; Cooper et al., Citation2020). However, thus far no reviews have reliably synthesised an effect for the presence of VER deficits in ADHD. Bora and Pantelis (Citation2016) aimed to synthesise VER deficits in ADHD, however this meta-analysis only included VER effects from six studies, which is a low number of studies to reliably interpret a synthesised effect size. Moreover, there was not enough emotion-specific data included within these six studies to explore whether VER deficits were generic or emotion-specific in nature. It is important to explore the nature of VER accuracy in ADHD to the same rigour as FER accuracy because understanding vocal expressions requires interpreting how the intensity, pitch and loudness of a voice change over time, whereas facial stimuli do not have to be dynamic to be interpreted correctly (Schirmer & Adolphs, Citation2017). Thus, facial and vocal emotions activate different areas of the brain (Schirmer & Adolphs, Citation2017), and need to be examined separately.
There are mixed findings within the literature relating to the nature of VER accuracy in ADHD. Studies employing VER tasks, such as the Diagnostic Analysis of Nonverbal Accuracy (DANVA; Nowicki & Duke, Citation1994) reported significantly more generic errors across happy, sad, angry, fearful and neutral vocal expressions in children with ADHD compared to typically developing children (Cadesky et al., Citation2000; Chronaki, Garner, et al., Citation2015; Corbett & Glidden, Citation2000). Similar findings have also been shown in adults (Bisch et al., Citation2016; Zuberer et al., Citation2020). In contrast, several VER studies have reported that children and adults with ADHD have a specific deficit to recognise negative vocal emotions, such as anger (Kis et al., Citation2017; Plećević et al., Citation2021). A specific emotion processing atypicality for vocal anger has been supported by evidence from Functional Magnetic Resonance Imaging data (Kochel et al., Citation2015) and Event-Related Potentials (Chronaki, Benikos, et al., Citation2015). For example, the finding of an enhanced N1 response to vocal anger in children with ADHD compared to controls is thought to reflect a pre-attentive hypervigilance to anger in ADHD (Chronaki, Benikos, et al., Citation2015). Finally, there is some evidence that the nature of VER accuracy changes depending on the subtype of ADHD or comorbid conduct disorder. For example, ADHD-inattentive subtype is associated with more VER errors overall, whilst hyperactive/impulsive symptoms are associated with greater difficulties to recognise negative (e.g. sad) vocal emotions (Miller et al., Citation2011). Moreover, a bias to recognise vocal anger in individuals with ADHD has been associated with comorbid conduct disorder (Cadesky et al., Citation2000). Findings from a number of studies are limited (Egan et al., Citation1998; Hall et al., Citation1999; Manassis et al., Citation2007; Rapport et al., Citation2002; Waddington et al., Citation2018) as they did not report accuracy scores for specific emotions, so it is inconclusive whether the VER deficits reported in these articles are reflective of a generic or an emotion-specific deficit in ADHD.
The present meta-analysis aims to provide robust evidence for the presence of VER deficits in ADHD by gathering and synthesising effects from all up-to-date literature, both published and unpublished, which measures the difference in accuracy scores between participants with ADHD and TD controls when completing an explicit VER task. Our primary prediction is that VER deficits will be present in ADHD, in accordance with previous reviews demonstrating the presence of FER deficits in ADHD (Bora & Pantelis, Citation2016; Borhani & Nejati, Citation2018; Collin et al., Citation2013; Cooper et al., Citation2020). Secondly, we aim to explore the nature of VER deficits in ADHD by quantifying the moderating effect of emotion type (e.g. happiness and anger) and valence (i.e. positive and negative) on VER accuracy in ADHD. There are two possible outcomes to this exploratory aim. If emotion does not have a moderating effect on VER accuracy in ADHD, this would suggest individuals with ADHD make random errors when recognising vocal emotions, due to general attention deviancies. If, however, emotion type has a moderating effect on VER accuracy in ADHD, this would suggest individuals with ADHD present with a consistent pattern of error towards a specific emotion type (e.g. anger), as found in FER research (Bora & Pantelis, Citation2016). This would reflect a distinct emotion processing atypicality in ADHD.
Method
Search strategy
The databases utilised to conduct searches for relevant studies published until 14 April 2022 included PsychINFO and PsychArticles, Pubmed and ProQuest Central. To address publication bias, ProQuest Dissertations and Theses Global databases were searched and authors were contacted for unpublished work. The Boolean expression used for the literature search was:
(ADHD OR “attention-deficit hyperactivity disorder” OR “attention-deficit/ hyperactivity disorder” OR “externalising behaviour*” OR “externalizing behavior*” OR “externalising problems” OR “externalizing problems” OR hyperact* OR inattent* OR impuls* OR “attention problem*” OR “hyperkinetic disorder”) AND (emotion* OR affect* OR ang* OR happ* OR joy OR sad* OR surprise* OR fear* OR disgust* OR fright*) AND (prosod* OR voice* OR speech OR vocal* OR auditory OR paralanguage OR nonverbal) AND (recogni* OR percept* OR decod* OR identify* OR process* OR naming OR detect* OR match* OR interpret* OR understand*).
The asterisk on some terms allowed for different possible endings e.g. processing, identifying. We formulated our search expression based on terms included in the titles of a list of pre-collected studies exploring associations between vocal emotion recognition and ADHD. Most searches were limited to title and/or abstracts for most terms, apart from words similar to “vocal”, which were searched throughout the whole text. This was because some studies which measured emotion recognition in different modalities do not specify the vocal modality in the title or abstract. To identify additional studies, we searched the reference lists of all included studies, and we searched (via google scholar) for any papers we had missed which had cited one key and most cited paper (Cadesky et al., Citation2000).
Inclusion and exclusion criteria
For a study to be included in the meta-analysis, it was required to meet a number of criteria. First, the study had to include a task which measured VER accuracy. We included tasks which presented vocally emotive stimuli to the participant and instructed the participant to explicitly identify the emotion in the voice. Tasks were labelled as explicit if the experimenter instructed the participant to recognise and label the emotion, and thus, the participant was aware they were recognising emotions. Participants could respond by pressing a corresponding button on a computer, verbally naming the emotion, or pointing to the corresponding emotion word. Generally, VER tasks (i.e. the DANVA) are valid to employ with both adults (Miller et al., Citation2011) and children (Chronaki, Garner, et al., Citation2015), so studies which employed various ages of participants, from childhood to adulthood, were included in this meta-analysis. The literature search yielded some studies with tasks instructing participants to match the vocal expression with a facial expression, or to detect whether the semantic content of the vocal expression matched the prosody (e.g. the MNTAP; Greenbaum et al., Citation2009), as well as dichotic listening tasks (Manassis et al., Citation2000). Although face matching tasks and dichotic listening tasks included elements of recognising emotions from voices, these studies were excluded from the meta-analysis because they were not a direct measure of VER. One study was excluded because participants were selected due to having difficulties recognising emotions as reported by parents or a professional, therefore this measure was biased (Loytomaki et al., Citation2020). Second, the emotions presented in the task needed to include at least two basic emotions, portraying happiness, anger, sadness, fear, disgust, or surprise. Third, all studies had to include a measure of ADHD, either defined as a categorical or a continuous variable. We included studies which employed only community samples and studies which compared clinical cases of ADHD and controls. These latter studies needed to include a sample of clinically diagnosed individuals with ADHD who met the criteria of the Diagnostic and Statistical Manual (DSM) or Diagnostic Interview Schedule for Children (DISC). Studies which included ADHD as a comorbid diagnosis alongside one other disorder, apart from Conduct Disorder (CD) and Oppositional Defiant Disorder (ODD), were excluded. Studies in which ADHD participants were on medication for ADHD symptoms were not excluded due to the ambiguity of medication status in some studies. However, we coded for variations in medication status as an exploratory variable. Fourth, studies which defined ADHD as a categorical variable had to include a TD group of individuals with no diagnosis of ADHD or other psychiatric disorder. Finally, studies that defined ADHD as a continuous variable and recruited only community samples had to include a measure of ADHD-related behaviours (i.e. inattention, and/or hyperactivity/impulsivity) on a dimensional scale by including a questionnaire measure consistent with the diagnostic criteria of ADHD.
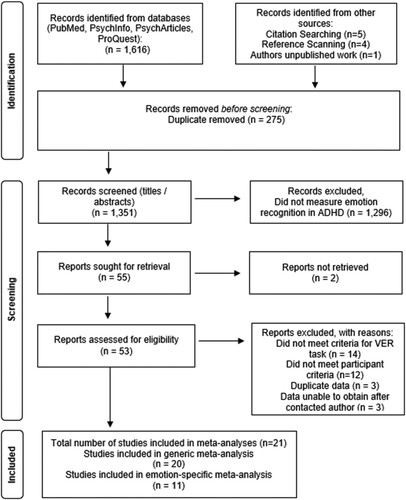
The literature search produced 1,626 published and unpublished research reports. After removing duplicates (n = 275), titles and abstracts were assessed for inclusion. 1,296 were removed on the basis they did not include an emotion recognition task, or a measure of ADHD or ADHD-related behaviour. Two articles were removed as the full-text version could not be retrieved. Finally, based on full-text examination of 53 potentially relevant articles, 26 articles were excluded because they did not measure VER in ADHD and TD participants. Three articles were excluded because they included duplicate data. Finally, we contacted 17 authors regarding missing emotion-specific accuracy scores. Six of these authors provided us with the missing emotion-specific data and five responded but could not access the data due to it being deleted in line with ethics guidelines. A total of six authors did not respond despite being contacted multiple times. Two authors could not be contacted (e.g. due to no forwarding email). Due to the lack of relevant statistics provided to calculate effect sizes for either a generic or emotion-specific vocal emotion recognition score, three papers were excluded (Bisch et al., Citation2016; Egan et al., Citation1998; Manassis et al., Citation2000). We were left with a final number of 21 studies which met our inclusion criteria. See for a flowchart of the literature search, which followed PRISMA guidelines for reporting systematic reviews and meta-analyses (Page et al., Citation2021).
Figure 1. PRISMA flowchart of literature search.
Study coding
All studies were double coded by two independent raters. Any coding disagreements were resolved by discussion. To assess intercoder reliability, intraclass coefficient and kappa coefficient were calculated for continuous and categorical characteristics, respectively (Orwin & Vevea, Citation2009). The mean reliability coefficient was 0.95, and the mean percentage agreement was 95% on coded study characteristics.
Theoretical moderator variables
When articles reported a VER accuracy score for all included emotions, this was coded as an overall VER score. When articles reported several VER accuracy scores for separate emotions, these were coded as emotion-specific VER scores. Twenty studies provided relevant statistics for an overall VER score, and 11 for emotion-specific VER scores. Emotion type and valence of emotion-specific VER scores were coded to assess the effect of emotion as a moderator variable. All 11 studies included scores for happy and angry vocal emotions, eight for sad, six for fearful and six for neutral expressions. Only one study provided scores for disgust and erotic vocal emotions (Zuberer et al., Citation2020), so these emotion types were excluded from the moderator analyses. Surprise was not coded as it was not included in any papers. In regard to valence, anger, sadness, and fear were classified as negative emotions. Happiness was classified as the only positive emotion.
Exploratory moderator variables
Participant characteristics coded for included the sample size, mean age, age range, and the percentage of female participants in each sample. Within the included 21 studies, there was a total of 763 participants with ADHD (32% female) and 888 control participants (42% female). Ages ranged from 3 to 65. Samples with mean ages from 3 to 11 were coded as children, and 12 to 18 as adolescents. This was based on the definition of the start of adolescence being the onset of puberty, which on average starts around 12 years (Blakemore, Citation2008). Those aged 18 and upwards were classified as adults, as the ability to recognise vocal emotions reaches adult levels by 18 years (Chronaki, Hadwin, et al., Citation2015; Grosbras et al., Citation2018). Based on this criterion, there were eight adult, nine child, and four adolescent samples included.
Within each study, it was noted whether ADHD was defined as a continuous or categorical variable. Within the 19 studies which defined ADHD as a categorical variable, participants were generally recruited due to being previously diagnosed. The diagnosis was confirmed with a mix of interview and questionnaire measures. The ADHD diagnosis was based on the DSM criteria (APA, Citation2013), apart from one study (Chronaki, Benikos, et al., Citation2015), which used the DISC-IV (Shaffer et al., Citation2000). Only two papers defined ADHD as a continuous variable. To measure ADHD traits, both continuous studies used the Strengths and Difficulties Questionnaire (Goodman, Citation1997), which maps onto the DSM criteria of ADHD (see b for all continuous measures of ADHD employed by each included study).
For the purpose of this meta-analysis, we defined ADHD as a categorical variable, and therefore we coded the subtypes of ADHD to fit this definition. The categorical subtypes of ADHD included a) ADHD-predominantly inattentive, b) ADHD-predominantly hyperactive/impulsive, and c) ADHD-combined subtype. If the outcome variable included a mix of different subtypes, we coded it as “ADHD-Combined type” but noted the number of ADHD participants with each subtype included in the sample, if reported. If ADHD was defined as a continuous variable in the included paper, then we coded the subscale used to gain a score of ADHD symptoms (i.e. inattentive-subscale, or hyperactive/ impulsive-subscale from the SDQ) under the respective subtype category outlined above. For example, if the inattentive subscale was used to quantify a score for ADHD symptoms, the outcome variable was coded as “ADHD-predominantly inattentive”. If both inattentive and hyperactive/impulsive subscales were combined to give one overall score for ADHD symptoms, this was coded as “ADHD-combined subtype”. Eighteen samples included a participant group of “ADHD-combined subtype”. Two studies included samples of “ADHD-predominantly hyperactive/impulsive”, and three studies included samples of “ADHD-predominantly inattentive”. We also coded the presence of comorbid Conduct Disorder and medication status within the ADHD participants. Three studies included ADHD participants with CD or ODD (Cadesky et al., Citation2000; Chronaki, Benikos, et al., Citation2015; Noordermeer et al., Citation2020). In 11 studies, participants with ADHD were on medication but withdrew from their medication between 4- and 48-hours prior to the study. In one study, all ADHD participants were non-medicated (Plećević et al., Citation2021), and in another, all ADHD participants were on medication (Norvilitis et al., Citation2000). In three studies, the medication status of ADHD participants was mixed, in that some participants were medicated, and some were not. In three studies, medication status was not reported.
Publication status and year of study were coded. Six studies were unpublished, and 15 were published between the years of 1999 and 2021. Design variables coded included the name of the VER task, the type of response participants made, the linguistic properties of the stimuli, and the characteristics (i.e. age and gender) of the actor who voiced the stimuli. See a and b for full details of participant, and design characteristics associated with all included studies.
Table 1a. Participant characteristics of included studies.
Table 1b. Design characteristics of included studies.
Analysis strategy
Since we defined ADHD as a categorical variable, effect sizes were computed as standardised mean differences (SMD; hedges g) for VER accuracy scores between individuals with ADHD and controls (ADHD group minus TD group; Hedges & Olkin, Citation1985). All effects from correlational studies were converted from Pearson’s r to hedges g. In total there were 93 effect sizes from 21 included studies. The variance for each effect size was also computed. As we can assume that the effect sizes gathered differ due to heterogeneity in samples recruited and study methods, the data were analysed using random-effects models (Borenstein et al., Citation2010). In typical random-effects models, there is the assumption that all effect sizes are independent from one another (Borenstein et al., Citation2010). However, in the present meta-analysis, this assumption was violated because we gathered more than one relevant effect size per included study. For example, some studies reported multiple effect sizes for each emotion type (e.g. anger, happiness, neutral), and ADHD participant group. This resulted in clusters of correlated effects for each study. To handle multiple dependent effect sizes within our meta-analyses, the method of robust variance estimation (RVE) was used (Tanner-Smith et al., Citation2016). There was also evidence of some hierarchical effects within our included studies (e.g. multiple studies from the same lab group). Note though, that most of the dependent effects were correlated, and therefore variance weights for correlated effects were employed (Tanner-Smith et al., Citation2016).
Two meta-analyses using RVE with variance weights for correlated effects in random-effects models were conducted separately. The first meta-analysis computed the average synthesised effect size for the presence of VER deficits. Twenty studies were included in this analysis as these studies provided the relevant statistics for overall VER accuracy scores. The second analysis explored the moderating effect of the theoretical moderator variables – emotion type and valence – on VER deficits in ADHD. Eleven studies were included in the moderator analyses as these studies provided relevant statistics for each specific emotion type included in the study. All analyses were conducted in the R environment (version 4.1.0). The Metafor package (Viechtbauer, Citation2010) was used to calculate and convert effect sizes into hedges g. The Robumeta package was used to estimate mean effect sizes using the RVE method (Tanner-Smith et al., Citation2016). The Grid package was used to create forest plots.
All exploratory moderator variables included in this meta-analysis contained distributions from fewer than 10 studies reporting relevant effect sizes for each variable condition. Therefore, following Kjærvik and Bushman (Citation2021) and Sterne et al. (Citation2011), we judged there was insufficient data to undertake formal statistical exploratory moderator analyses in line with best practice for conducting comprehensive meta-analyses. For transparency of data, we report the numerical trends (SMD and Standard Error) of all exploratory categorical variables in . However, these should be interpreted with caution due to paucity of data.
Table 2. Numerical trends (SMD and Standard Error) of vocal emotion recognition deficits for all categorical exploratory moderator variables.
Results
When quantifying VER accuracy scores from 20 studies, there was a medium statistically significant effect size (SMD = −0.56, [−0.78, −0.34]). See for a forest plot showing the weight of each effect size within the analyses, taking into consideration sample size and clusters of correlated effects. Similarly, across all emotion-specific VER accuracy scores from 11 studies, there was a small effect size (SMD = −0.39,
[−0.59, −0.18]). The slightly smaller effect size in the emotion-specific compared to the overall analyses is likely due to fewer effect sizes and studies included in the emotion-specific analysis. The I squared statistic indicated that 72% of the heterogeneity in the effects was due to between-study differences. These results suggest there is strong evidence for VER deficits in ADHD, in accordance with our primary prediction. Moderator analyses showed that neither emotion type or valence significantly influenced the magnitude of the effect size for emotion-specific accuracy scores (). This indicates the presence of a generic VER deficit in ADHD, supporting cognitive behavioural theories (Barkley, Citation1997; Nigg et al., Citation2005). Alternatively, it is possible there is insufficient power within the literature to provide evidence that emotion moderates VER deficits in ADHD.
Figure 2. Forest plot showing SMD (hedges g) for 20 studies which included a generic VER accuracy score, and the corresponding weight of each effect size.
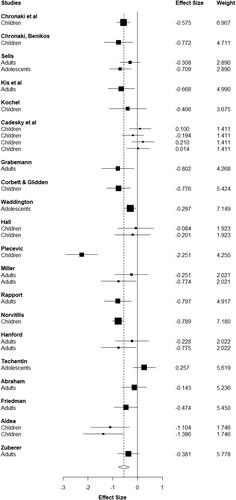
Table 4. Table showing the effect size (Standardise Mean Difference; SMD) and associated statistics for the sensitivity analyses, with and without outliers (w/o).
Sensitivity analyses were conducted to explore the robustness and validity of the effect for the presence of VER deficits in ADHD. A naïve SMD (Copas & Shi, Citation2000), along with prediction intervals (Riley et al., Citation2011), and tests for publication bias (Duval & Tweedie, Citation2000; Egger et al., Citation1997) were calculated (see ). Potential outliers were identified from funnel plots (see and ). Thus, we re-ran all analysesFootnote1 with two extreme outliers (Plećević et al., Citation2021; Techentin, Citation2009) excluded. Additionally, to rule out the possible influence of medication of VER deficits in ADHD, we re-ran the analyses excluding all 7 studies in which the medication status of ADHD participants was not reported, mixed or “on medication”. Excluding all 7 studies did not change the results. Overall, sensitivity analyses showed publication bias was not present within the current meta-analyses, nor did outliers or medication status influence the overall effect size for VER scores. However, when outliers were removed, the prediction intervals suggested the range of true effects that could be reported within an individual study were negative 95% of the time (between −0.90 and −0.04). This provided strong support that our reported effect of a VER deficit in ADHD was consistent and robust (Riley et al., Citation2011).
Figure 3. Funnel plot for generic VER analysis.
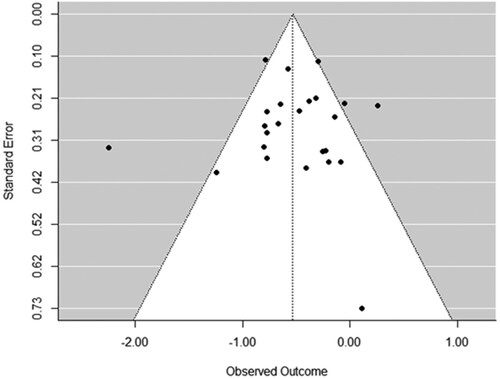
Figure 4. Funnel plot for generic VER analysis without outliers.
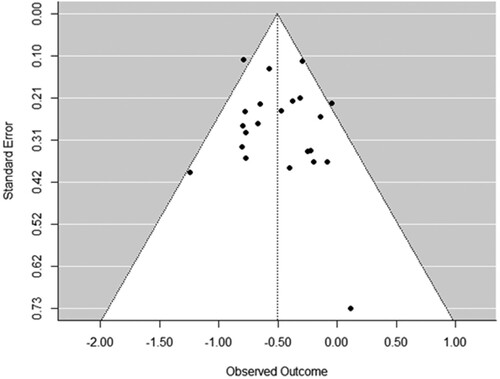
Table 3. Table showing coefficient estimate, and associated t values, significance (p values), and CI of emotion type and valence moderator analyses.Footnote2
Discussion
This meta-analysis provided evidence for the presence of VER deficits in ADHD and explored whether they were reflective of a generic attention deviancy and/or atypical emotion processing. Twenty-one published and unpublished studies were included as part of two meta-analyses quantifying VER accuracy scores, and the moderating effect of emotion type and valence on VER deficits in ADHD. First, our results showed a medium effect size for the presence of VER deficits in ADHD (d = 0.56). Despite heterogeity in study methods and characteristics of ADHD participants within the included studies, our results indicated VER deficits in ADHD are found in 95% of studies employing VER tasks, suggesting this effect is reliable and robust. This result is consistent with previous reviews reporting the presence of FER deficits in ADHD (Borhani & Nejati, Citation2018; Collin et al., Citation2013; Cooper et al., Citation2020). This is supportive of the preliminary finding from Bora and Pantelis (Citation2016) who reported an effect of d = 0.4 for VER deficits from only six papers prior to 2015. Importantly, the present meta-analyses confirms the effect of VER deficits in ADHD is reliable and consistent due to synthesising effects from a high number of studies (more than 10), in line with best practice. Therefore, our results add weight to the literature stating difficulties to recognise vocal emotional expressions, are present in ADHD.
Second, our meta-analysis showed a lack of moderation to VER deficits present in ADHD by emotion type or valence. There are two possible explanations for this finding. One explanation is that this is a true effect, indicating that the pattern of errors made by individuals with ADHD during VER tasks is random. This suggests VER deficits in ADHD are generic in nature, in support of attentional mechanisms being implicated in emotion recognition difficulties in ADHD. This is consistent with previous research suggesting emotion regulation difficulties in ADHD are associated with deficits in executive function (Groves et al., Citation2020; Sjowall et al., Citation2013). These findings are in line with cognitive behavioural theories (Barkley, Citation1997; Nigg et al., Citation2005), which imply individuals with ADHD may have difficulty regulating emotions due to a core deviancy in allocating attention towards emotions. It is also important to consider that attentional and socio-cognitive mechanisms are not mutually exclusive, as perceptual processes, including attention, may be influenced by processes related to motivation and impact subsequent interpretations of emotional information from vocal cues (Crick & Dodge, Citation1994; Lemerise & Arsenio, Citation2000).
An alternative explanation for this finding is that this result has arisen because of a lack of power in regard to the moderator analyses, despite including all VER studies to date, and gathering missing emotion-specific data from authors. For instance, most studies in the present meta-analysis only consistently included angry and happy vocal emotion types within the VER tasks. The other emotion types which were included within the VER literature (i.e. fear, sadness, neutral expressions) were not consistent throughout task designs. This inconsistency in emotion types made it difficult to reliably perform moderator analysis with a varied and nuanced selection of emotion types within the present meta-analysis. If this explanation regarding a lack of power is true, it indicates the cumulative evidence within the behavioural VER literature is not statistically robust to provide evidence for emotion-specific VER deficits in ADHD. Therefore, there is insufficient data reported within the behavioural VER literature to provide support for atypicalities in emotional processes implicated by socio-cognitive (Crick & Dodge, Citation1994) and motivational (Sonuga-Barke, Citation2005) theories of ED in ADHD. More thorough research is necessary to determine whether emotion-specific deficits are present in individuals with ADHD, and whether they may be causally implicated in poor clinical and functional outcomes.
Future research might aim to explore whether emotion processing atypicalities contribute to vocal emotion processing deficits in ADHD through use of different experimental designs, employing neuro-imaging techniques, and by considering other important moderator variables, such as ADHD subgroup and comorbidities. This is important as there appear to be some trends within the literature indicating the presence of processing abnormalities at the perceptual processing stage of emotion recognition. For example, neuro-imaging data, such as those from fMRI and EEG studies, have provided support for a specific atypicality to process vocal anger in ADHD (Chronaki, Benikos, et al., Citation2015; Kochel et al., Citation2015). Moreover, there is some evidence which indicates exploring biases in emotion perception may be a better marker of “cognitive distortion”, reflecting misinterpretation at a perceptual level of emotion recognition, compared to deficits, which are suggestive to be a better marker of attention deviancies (Cadesky et al., Citation2000; Uekermann et al., Citation2010). Within the present meta-analysis, the decision to quantify VER deficits was justified due to limited research exploring recognition biases in the literature. Additionally, trends within the VER literature suggest it is possible that other variables, such as varying ADHD subtypes, and comorbid CD, may affect the nature of VER deficits in ADHD. For example, Miller et al. (Citation2011) found ADHD-inattentive type was associated with generic VER deficits in adults, whereas hyperactive/impulsive symptoms were associated with a specific deficit for recognising negative emotions. Moreover, children with comorbid ADHD and CD were more likely to make VER errors due to a bias to label ambiguous voices as anger, which was not found in children with ADHD-only (Cadesky et al., Citation2000). Overall, these trends should be interpreted with caution due to limited evidence. Further research is required to substantiate them within the VER literature.
The finding of robust VER deficits in ADHD complements results from the extensive reports of FER deficits in ADHD (Bora & Pantelis, Citation2016; Borhani & Nejati, Citation2018; Collin et al., Citation2013; Cooper et al., Citation2020). Together, these findings suggest emotion recognition deficits in ADHD are present across modalities, in both the face and voice. However, there is no evidence from the behavioural literature to support the presence of emotion-specific deficits in the voice, as previously found in the face (Bora & Pantelis, Citation2016; Borhani & Nejati, Citation2018). One explanation for this could be due to the dynamic nature of vocal stimuli, compared to static stimuli generally employed in FER studies. For example, perceiving emotions in voices, involves a participant attending to various acoustic parameters which change over time. This activates different areas of the brain compared to interpreting a single static image in FER studies (Schirmer & Adolphs, Citation2017). It is therefore possible that, due to the nature of the stimuli, FER tasks are more sensitive, compared to VER tasks, in demonstrating the moderating effects of emotion in individuals with ADHD. In support of this, FER tasks which employed dynamic facial stimuli reported deficits for both positive and negative stimuli in children with ADHD compared to controls but did not report any specific deficits for negative emotions (Jusyte et al., Citation2017; Ludlow et al., Citation2014). Future research might aim to employ dynamic multimodal presentations of emotional stimuli (e.g. presentation of the voice and face together), which has been shown to increase the accuracy of emotion perception in typical individuals (Klasen et al., Citation2012). This will enable us to understand whether emotion-specific effects are present when vocal emotional signals are integrated into more holistic emotional expressions, thought to be a more reliable measure of emotion perception (Schirmer & Adolphs, Citation2017).
In summary, this meta-analysis provides evidence for a robust and reliable effect for the presence of VER deficits in ADHD, in accordance with previous reviews and facial emotion recognition research (Bora & Pantelis, Citation2016). Secondly, there is a lack of robust evidence in support of the modulation of emotion on VER deficits in ADHD. This suggests VER deficits are generic in nature, supporting the view that ED in ADHD is a secondary problem underpinned, at least in part, by primary attention deficits (Barkley, Citation1997; Nigg et al., Citation2005). There is currently not sufficiently robust evidence within the behavioural VER literature to support the definite presence of atypicalities in the perceptual emotion processing mechanisms in ADHD. There is a clear need for further behavioural and neuro-imaging emotion processing studies exploring both biases and deficits in vocal, and multimodal, emotion processing, which take into consideration ADHD subtype and comorbidities.
Acknowledgements
The authors would like to thank Brad J. Bushman and Sophie L. Kjaervik for their advice on the design and analyses, which we incorporated into this review. The authors also thank the researchers of the studies which were included in this meta-analysis, and those who responded to requests of additional data and information. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Declaration of interest: none
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are openly available in Open Science Framework at DO I 10.17605/OSF.IO/GJM4D.
Additional information
Funding
Notes
1 We also calculated the RVE analyses again for both the generic analyses and emotion-specific analyses, but with the outliers (Plećević et al., Citation2021; Techentin, Citation2009) removed. When we re-ran the moderator analyses with the outliers removed, we found no change to the significance of the moderating effect of emotion type and valence. See row 5 in for associated statistics.
2 Within the “emotion type” moderator analysis, anger was the intercept for contrasts with the four other emotion types (happiness, fear, neutral and sadness). Within the “valence” moderator analysis, negative was the intercept for contrasts with two other valence types (positive and neutral). It is important to note, not all 11 studies included in the emotion-specific analyses provided effect sizes for all emotion types (i.e. fearful, sadness, and neutral expressions). There were 36% missing for sadness, 45% missing for fear, 45% missing for neutral expression. As a sensitivity analysis, we re-ran the moderator analysis with only the emotions which were included in all 11 studies (anger and happiness). The mean SMD was −0.369, with 95% CI between −0.574 and −0.164. Moderator analyses (anger vs happiness) remained non-significant. Please see for numerical trends of all other exploratory variables which cannot reliably be analysed via moderator analysis.
References
References marked with an Asterix were included in the formal meta-analyses.
- *Abraham, J. (2004). Emotional intensity and affect recognition among adults with ADHD. Southeastern Louisiana University.
- *Aldea, R. F. (2013). Emotion recognition and social functioning in children with and without attention deficit hyperactivity disorder. University of Kentucky.
- APA. (2013). Diagnostic and statistical manual of mental disorders (DSM-5) (5th ed.). American Psychiatric Publishing.
- Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121(1), 65–94. https://doi.org/10.1037/0033-2909.121.1.65
- Barkley, R. A., & Fischer, M. (2010). The unique contribution of emotional impulsiveness to impairment in major life activities in hyperactive children as adults. Journal of the American Academy of Child & Adolescent Psychiatry, 49(5), 503–513. https://doi.org/10.1097/00004583-201005000-00011
- Barkley, R. A., & Murphy, K. R. (1998). Attention-deficit hyperactivity disorder, a clinical workbook (2nd ed.). New York: Guildford Press.
- Bisch, J., Kreifelts, B., Bretscher, J., Wildgruber, D., Fallgatter, A., & Ethofer, T. (2016). Emotion perception in adult attention-deficit hyperactivity disorder. Journal of Neural Transmission, 123(8), 961–970. https://doi.org/10.1007/s00702-016-1513-x
- Blakemore, S. J. (2008). The social brain in adolescence. Nature Reviews Neuroscience, 9(4), 267–277. https://doi.org/10.1038/nrn2353
- Bora, E., & Pantelis, C. (2016). Meta-analysis of social cognition in attention-deficit/hyperactivity disorder (ADHD): Comparison with healthy controls and autistic spectrum disorder. Psychological Medicine, 46(4), 699–716. https://doi.org/10.1017/S0033291715002573
- Borenstein, M., Hedges, L. V., Higgins, J. P., & Rothstein, H. R. (2010). A basic introduction to fixed-effect and random-effects models for meta-analysis. Research Synthesis Methods, 1(2), 97–111. https://doi.org/10.1002/jrsm.12
- Borhani, K., & Nejati, V. (2018). Emotional face recognition in individuals with attention-deficit/hyperactivity disorder: A review article. Developmental Neuropsychology, 43(3), 256–277. https://doi.org/10.1080/87565641.2018.1440295
- Breitenstein, C., Daum, I., Ackermann, H., Lütgehetmann, R., & Müller, E. (1996). Erfassung der Emotionswahrnehmung bei zentralnervösen Läsionen und Erkrankungen: Psychometrische Gütekriterien der “Tübinger Affekt Batterie”. Neurol Rehabil, 2(9).
- Bunford, N., Evans, S. W., & Wymbs, F. (2015). ADHD and emotion dysregulation among children and adolescents. Clinical Child and Family Psychology Review, 18(3), 185–217. https://doi.org/10.1007/s10567-015-0187-5
- *Cadesky, E. B., Mota, V. L., Mota, V. L., & Schachar, R. J. (2000). Beyond words: How do children with ADHD and/or conduct problems process nonverbal information about affect?. Journal of the American Academy of Child & Adolescent Psychiatry, 39(9), 1160–1167. https://doi.org/10.1097/00004583-200009000-00016
- *Chronaki, G., Benikos, N., Fairchild, G., & Sonuga-Barke, E. J. (2015). Atypical neural responses to vocal anger in attention-deficit/hyperactivity disorder. Journal of Child Psychology and Psychiatry, 56(4), 477–487. https://doi.org/10.1111/jcpp.12312
- *Chronaki, G., Garner, M., Hadwin, J. A., Thompson, M. J., Chin, C. Y., & Sonuga-Barke, E. J. (2015). Emotion-recognition abilities and behavior problem dimensions in preschoolers: Evidence for a specific role for childhood hyperactivity. Child Neuropsychology, 21(1), 25–40. https://doi.org/10.1080/09297049.2013.863273
- Chronaki, G., Hadwin, J. A., Garner, M., Maurage, P., & Sonuga-Barke, E. J. (2015). The development of emotion recognition from facial expressions and non-linguistic vocalizations during childhood. British Journal of Developmental Psychology, 33(2), 218–236. https://doi.org/10.1111/bjdp.12075
- Collin, L., Bindra, J., Raju, M., Gillberg, C., & Minnis, H. (2013). Facial emotion recognition in child psychiatry: A systematic review. Research in Developmental Disabilities, 34(5), 1505–1520. https://doi.org/10.1016/j.ridd.2013.01.008
- Cooper, S., Hobson, C. W., & van Goozen, S. H. (2020). Facial emotion recognition in children with externalising behaviours: A systematic review. Clinical Child Psychology and Psychiatry, 25(4), 1068–1085. https://doi.org/10.1177/1359104520945390
- Conners, C. K. (1990). Manual for Conner's rating scales. Multi-Health Systems, Incorporated.
- Copas, J., & Shi, J. Q. (2000). Meta-analysis, funnel plots and sensitivity analysis. Biostatistics (Oxford, England), 1(3), 247–262. https://doi.org/10.1093/biostatistics/1.3.247
- *Corbett, B., & Glidden, H. (2000). Processing affective stimuli in children with attention-deficit hyperactivity disorder. Child Neuropsychology, 6(2), 144–155. https://doi.org/10.1076/chin.6.2.144.7056
- Crick, R., & Dodge, K. R. (1994). A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychological Bulletin, 115(1), 74.
- D’Agostino, A., Covanti, S., Rossi Monti, M., & Starcevic, V. (2017). Reconsidering emotion dysregulation. Psychiatric Quarterly, 88(4), 807–825. https://doi.org/10.1007/s11126-017-9499-6
- De Sonneville, L. M. (1999). Amsterdam neuropsychological tasks: A computer-aided assessment. Cognitive Ergonomics, Clinical Assessment and Computer-Assisted Learning, 6, 187.
- Döpfner, M., Schmeck, K., & Berner, W. (1994). Handbuch: Elternfragebogen über das Verhalten von Kindern und Jugendlichen–Deutsche Bearbeitung der Child Behaviour Checklist (CBCL/4-18). Arbeitsgruppe Kinder-, Jugend-und Familiendiagnostik, Köln.
- Döpfner, M., Lehmkuhl, G., Görtz-Dorten, A., Breuer, D., Lehmkuhl, G., & Görtz-Dorten, A. (2008). DISYPS-II: Diagnostik-System für psychische Störungen nach ICD-10 und DSM-IV für Kinder und Jugendliche-II. Huber: Hogrefe Testverl.
- Drechsler, R., Brem, S., Brandeis, D., Gruenblatt, E., Berger, G., & Walitza, S. (2020). ADHD: Current concepts and treatments in children and adolescents. Neuropediatrics, 51(05), 315–335. https://doi.org/10.1055/s-0040-1701658
- Duval, S., & Tweedie, R. (2000). Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56(2), 455–463. https://doi.org/10.1111/j.0006-341x.2000.00455.x
- Egan, G. J., Brown, R. T., Goonan, L., Goonan, B. T., & Celano, M. (1998). The development of decoding of emotions in children with externalizing behavioral disturbances and their normally developing peers. Archives of Clinical Neuropsychology, 13(4), 383–396. https://www.ncbi.nlm.nih.gov/pubmed/14590616
- Egger, M., Davey Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ, 315(7109), 629–634. https://doi.org/10.1136/bmj.315.7109.629
- Fantozzi, P., Sesso, G., Muratori, P., Milone, A., & Masi, G. (2021). Biological bases of empathy and social cognition in patients with attention-deficit/hyperactivity disorder: A focus on treatment with psychostimulants. Brain Sciences, 11(11), 11. https://doi.org/10.3390/brainsci11111399
- Fayyad, J., Sampson, N. A., Hwang, I., Adamowski, T., Aguilar-Gaxiola, S., Al-Hamzawi, A., Andrade, L. H., Borges, G., de Girolamo, G., Florescu, S., Gureje, O., Haro, J. M., Hu, C., Karam, E. G., Lee, S., Navarro-Mateu, F., O’Neill, S., Pennell, B. E., Piazza, M., … Collaborators, W. H. O. W. M. H. S. (2017). The descriptive epidemiology of DSM-IV adult ADHD in the world health organization world mental health surveys. ADHD Attention Deficit and Hyperactivity Disorders, 9(1), 47–65. https://doi.org/10.1007/s12402-016-0208-3
- *Friedman, S. R. (2000). Emotion recognition, social skills and adult attention-deficit/hyperactivity disorder. Wayne State University.
- Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
- Goyette, C. H., Conners, C. K., & Ulrich, R. F. (1978). Normative data on revised Conners parent and teacher rating scales. Journal of Abnormal Child Psychology, 6, 221–236.
- *Grabemann, M., Mette, C., Zimmermann, M., Heinrich, V., Uekermann, J., Wiltfang, J., & Kis, B. (2013). No clear effects of acute tryptophan depletion on processing affective prosody in male adults with ADHD. Acta Psychiatrica Scandinavica, 128(2), 142–148. https://doi.org/10.1111/acps.12130
- Graziano, P. A., & Garcia, A. (2016). Attention-deficit hyperactivity disorder and children’s emotion dysregulation: A meta-analysis. Clinical Psychology Review, 46, 106–123. https://doi.org/10.1016/j.cpr.2016.04.011
- Greenbaum, R. L., Stevens, S. A., Nash, K., Koren, G., & Rovet, J. (2009). Social cognitive and emotion processing abilities of children with fetal alcohol spectrum disorders: A comparison with attention deficit hyperactivity disorder. Alcoholism: Clinical and Experimental Research, 33(10), 1656–1670. https://doi.org/10.1111/j.1530-0277.2009.01003.x
- Grosbras, M. H., Ross, P. D., & Belin, P. (2018). Categorical emotion recognition from voice improves during childhood and adolescence. Scientific Reports, 8(1), 14791. https://doi.org/10.1038/s41598-018-32868-3
- Groves, N. B., Kofler, M. J., Wells, E. L., Day, T. N., & Chan, E. S. M. (2020). An examination of relations among working memory, ADHD symptoms, and emotion regulation. Journal of Abnormal Child Psychology, 48(4), 525–537. https://doi.org/10.1007/s10802-019-00612-8
- *Hall, C. W., Peterson, A. D., Webster, R. E., Bolen, L. M., & Brown, M. B. (1999). Perception of nonverbal social cues by regular education, ADHD, and ADHD/LD students. Psychology in the Schools, 36(6), 505–514. https://doi.org/10.1002/(SICI)1520-6807(199911)36:6<505::AID-PITS6>3.0.CO;2-9
- *Hanford, R. B. (2000). Working memory and nonverbal affect recognition: Differentiation among ADHD subtypes in adults. Emory University.
- Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. Academic Press.
- Jovičić, S., Kašić, Z., Đorđević, M., Vojnović, M., Rajković, M., & Savković, J. (2004). Corpus creating of speech expression of emotions and attitudes in serbian language. Sovilj Meditor Speech and Language., 36–62.
- Jusyte, A., Gulewitsch, M. D., & Schonenberg, M. (2017). Recognition of peer emotions in children with ADHD: Evidence from an animated facial expressions task. Psychiatry Research, 258, 351–357. https://doi.org/10.1016/j.psychres.2017.08.066
- *Kis, B., Guberina, N., Kraemer, M., Niklewski, F., Dziobek, I., Wiltfang, J., & Abdel-Hamid, M. (2017). Perception of emotional prosody in adults with attention deficit hyperactivity disorder. Acta Psychiatrica Scandinavica, 135(6), 506–514. https://doi.org/10.1111/acps.12719
- Kjærvik, S. L., & Bushman, B. J. (2021). The link between narcissism and aggression: A meta-analytic review. Psychological Bulletin, 147(5), 477. https://doi.org/10.1037/bul0000323
- Klasen, M., Chen, Y. H., & Mathiak, K. (2012). Multisensory emotions: Perception, combination and underlying neural processes. Reviews in the Neurosciences, 23(4), 381–392. https://doi.org/10.1515/revneuro-2012-0040
- *Kochel, A., Schongassner, F., Feierl-Gsodam, S., & Schienle, A. (2015). Processing of affective prosody in boys suffering from attention deficit hyperactivity disorder: A near-infrared spectroscopy study. Social Neuroscience, 10(6), 583–591. https://doi.org/10.1080/17470919.2015.1017111
- Lemerise, E. A., & Arsenio, W. F. (2000). An integrated model of emotion processes and cognition in social information processing. Child Development, 71(1), 107–118. https://doi.org/10.1111/1467-8624.00124
- Loytomaki, J., Ohtonen, P., Laakso, M. L., & Huttunen, K. (2020). The role of linguistic and cognitive factors in emotion recognition difficulties in children with ASD, ADHD or DLD. International Journal of Language & Communication Disorders, 55(2), 231–242. https://doi.org/10.1111/1460-6984.12514
- Ludlow, A. K., Garrood, A., Lawrence, K., & Gutierrez, R. (2014). Emotion recognition from dynamic emotional displays in children with adhd. Journal of Social and Clinical Psychology, 33(5), 413–427. https://doi.org/10.1521/jscp.2014.33.5.413
- Manassis, K., Tannock, R., & Barbosa, J. (2000). Dichotic listening and response inhibition in children with comorbid anxiety disorders and ADHD. Journal of the American Academy of Child & Adolescent Psychiatry, 39(9), 1152–1159. https://doi.org/10.1097/00004583-200009000-00015
- Manassis, K., Tannock, R., Young, A., & Francis-John, S. (2007). Cognition in anxious children with attention deficit hyperactivity disorder: A comparison with clinical and normal children. Behavioral and Brain Functions, 3(1), 4. https://doi.org/10.1186/1744-9081-3-4
- Maurage, P., Joassin, F., Philippot, P., & Campanella, S. (2007). A validated battery of vocal emotional expressions. Neuropsychological Trends, 2(1), 63–74.
- *Miller, M., Hanford, R. B., Fassbender, C., Duke, M., & Schweitzer, J. B. (2011). Affect recognition in adults with ADHD. Journal of Attention Disorders, 15(6), 452–460. https://doi.org/10.1177/1087054710368636
- Murphy, K., & Barkley, R. A. (1995). Preliminary normative data on DSM-IV criteria for adults. ADHD Report, 3(3), 6–7.
- Nigg, J. T., Stavro, G., Ettenhofer, M., Hambrick, D. Z., Miller, T., & Henderson, J. M. (2005). Executive functions and ADHD in adults: Evidence for selective effects on ADHD symptom domains. Journal of Abnormal Psychology, 114(4), 706–717. https://doi.org/10.1037/0021-843x.114.3.706
- *Noordermeer, S. D. S., Luman, M., Buitelaar, J. K., Hartman, C. A., Hoekstra, P. J., Franke, B., Faraone, S. V., Heslenfeld, D. J., & Oosterlaan, J. (2020). Neurocognitive deficits in attention-deficit/hyperactivity disorder with and without comorbid oppositional defiant disorder. Journal of Attention Disorders, 24(9), 1317–1329. https://doi.org/10.1177/1087054715606216
- *Norvilitis, J. M., Casey, R. J., Brooklier, K. M., & Bonello, P. J. (2000). Emotion appraisal in children with attention-deficit/hyperactivity disorder and their parents. Journal of Attention Disorders, 4(1), 15–26. https://doi.org/10.1177/108705470000400102
- Nowicki, S., & Duke, M. P. (1994). Individual differences in the nonverbal communication of affect: The diagnostic analysis of nonverbal accuracy scale. Journal of Nonverbal Behavior, 18, 9–35.
- Orwin, R. G., & Vevea, J. L. (2009). Evaluating coding decisions. The Handbook of Research Synthesis and Meta-Analysis, 2, 177–203.
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hrobjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Revista Española de Cardiología (English Edition), 74(9), 790–799. https://doi.org/10.1016/j.rec.2021.07.010
- *Plećević, V., Djoković, S., & Kovačević, T. (2021). Recognition of emotions and affective attitudes in children with attention-deficit hyperactivity disorder. Vojnosanitetski pregled, 78(10). https://doi.org/10.2298/VSP191004025P
- Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434–442. https://doi.org/10.1093/ije/dyt261
- *Rapport, L. J., Friedman, S. R., Tzelepis, A., & Van Voorhis, A. (2002). Experienced emotion and affect recognition in adult attention-deficit hyperactivity disorder. Neuropsychology, 16(1), 102–110. https://doi.org/10.1037//0894-4105.16.1.102
- Retz-Junginger, P., Retz, W., Blocher, D., Weijers, H. G., Trott, G. E., Wender, P. H., & Rössler, M. (2002). Wender Utah rating scale. The short-version for the assessment of the attention-deficit hyperactivity disorder in adults. Der Nervenarzt, 73(9), 830–838.
- Riley, R. D., Higgins, J. P., & Deeks, J. J. (2011). Interpretation of random effects meta-analyses. BMJ, 342(feb10 2), d549. https://doi.org/10.1136/bmj.d549
- Rutter, M., Bailey, A., & Lord, C. (2003). SCQ. The Social Communication Questionnaire. Torrance, CA: Western Psychological Services.
- Rothenberg, B. (1970). Children’s social sensitivity and the relationship to interpersonal competence, intrapersonal comfort, and intellectual level. Developmental Psychology, 2(3), 335. https://doi.org/10.1037/h0029175
- Rösler, M., Retz, W., Retz-Junginger, P., Thome, J., Supprian, T., Nissen, T., … & Trott, G. E. (2004). Tools for the diagnosis of attention-deficit/hyperactivity disorder in adults: Self-rating behaviour questionnaire and diagnostic checklist. Der Nervenarzt, 75, 888–895.
- Schacher, R., Ickowicz, A., Wachsmuth, R. (1995). Parent interview for child symptoms-revised for DSM-IV. Toronto: Hospital for Sick Children, Department of Psychiatry.
- Schirmer, A., & Adolphs, R. (2017). Emotion perception from face, voice, and touch: Comparisons and convergence. Trends in Cognitive Sciences, 21(3), 216–228. https://doi.org/10.1016/j.tics.2017.01.001
- *Sells, L., & Chronaki, G. (Unpublished). Associations between externalising behaviours and the recognition of vocal anger in adolescents and adults.
- Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M. K., & Schwab-Stone, M. E. (2000). NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry, 39(1), 28–38. https://doi.org/10.1097/00004583-200001000-00014
- Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E. (2014). Emotion dysregulation in attention deficit hyperactivity disorder. American Journal of Psychiatry, 171(3), 276–293. https://doi.org/10.1176/appi.ajp.2013.13070966
- Sjowall, D., Roth, L., Lindqvist, S., & Thorell, L. B. (2013). Multiple deficits in ADHD: Executive dysfunction, delay aversion, reaction time variability, and emotional deficits. Journal of Child Psychology and Psychiatry, 54(6), 619–627. https://doi.org/10.1111/jcpp.12006
- Sonuga-Barke, E. J. (2005). Causal models of attention-deficit/hyperactivity disorder: From common simple deficits to multiple developmental pathways. Biological Psychiatry, 57(11), 1231–1238. https://doi.org/10.1016/j.biopsych.2004.09.008
- Steinberg, E. A., & Drabick, D. A. (2015). A developmental psychopathology perspective on ADHD and comorbid conditions: The role of emotion regulation. Child Psychiatry & Human Development, 46(6), 951–966. https://doi.org/10.1007/s10578-015-0534-2
- Sterne, J. A., Sutton, A. J., Ioannidis, J. P., Terrin, N., Jones, D. R., Lau, J., Carpenter, J., Rucker, G., Harbord, R. M., Schmid, C. H., Tetzlaff, J., Deeks, J. J., Peters, J., Macaskill, P., Schwarzer, G., Duval, S., Altman, D. G., Moher, D., & Higgins, J. P. (2011). Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ, 343(jul22 1), d4002. https://doi.org/10.1136/bmj.d4002
- Tanner-Smith, E. E., Tipton, E., & Polanin, J. R. (2016). Handling complex meta-analytic data structures using robust variance estimates: A tutorial in R. Journal of Developmental and Life-Course Criminology, 2(1), 85–112. https://doi.org/10.1007/s40865-016-0026-5
- *Techentin, C. (2009). Integrating semantic and emotional information in boys with and without ADHD during an auditory stroop-like task. University of New Brunswick.
- Thomas, R., Sanders, S., Doust, J., Beller, E., & Glasziou, P. (2015). Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics, 135(4), e994–1001. https://doi.org/10.1542/peds.2014-3482
- Tucker, D. M., Watson, R. T., & Heilman, K. M. (1977). Discrimination and evocation of affectively intoned speech in patients with right parietal disease. Neurology, 27(10), 947–950. https://doi.org/10.1212/wnl.27.10.947
- Uekermann, J., Kraemer, M., Abdel-Hamid, M., Schimmelmann, B. G., Hebebrand, J., Daum, I., Wiltfang, J., & Kis, B. (2010). Social cognition in attention-deficit hyperactivity disorder (ADHD). Neuroscience & Biobehavioral Reviews, 34(5), 734–743. https://doi.org/10.1016/j.neubiorev.2009.10.009
- Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1–48. https://doi.org/10.18637/jss.v036.i03
- *Waddington, F., Hartman, C., de Bruijn, Y., Lappenschaar, M., Oerlemans, A., Buitelaar, J., & Rommelse, N. (2018). Visual and auditory emotion recognition problems as familial cross-disorder phenomenon in ASD and ADHD. European Neuropsychopharmacology, 28(9), 994–1005. https://doi.org/10.1016/j.euroneuro.2018.06.009
- Wehmeier, P. M., Schacht, A., & Barkley, R. A. (2010). Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. Journal of Adolescent Health, 46(3), 209–217. https://doi.org/10.1016/j.jadohealth.2009.09.009
- *Zuberer, A., Schwarz, L., Kreifelts, B., Wildgruber, D., Erb, M., Fallgatter, A., Scheffler, K., & Ethofer, T. (2020). Neural basis of impaired emotion recognition in adult attention-deficit/hyperactivity disorder. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, https://doi.org/10.1016/j.bpsc.2020.11.013