
Abstract
Introduction and Aims
This study aimed to explore the perspectives and experiences of mothers of school-age children with asthma in care.
Methods
A phenomenological study was conducted using qualitative research methods from August 2021 to November 2021. Mothers (from Sichuan, China) of school-aged children with asthma who sought outpatient care at the pediatric asthma clinic were purposively sampled based on their occupation, education level, and duration of their child’s illness. Semi-structured face-to-face interviews were conducted in consultation room A07 of the pediatric asthma clinic. The interviews were audio-recorded, transcribed verbatim, and analyzed thematically.
Results
23 mothers expressed interest, but data saturation was reached after recruiting 15 mothers.Four main themes encompassing ten sub-themes emerged from the analysis: (1) Negative psychological burden, with sub-themes including anxiety shock, fear of death, guilt, and stigma. (2) Family dysfunction, with sub-themes including impaired quality of life, family emotional crisis, and heavy economic burden. (3) Difficulty in seeking medical treatment. (4) Active response, with sub-themes including emotional adjustment, family empowerment, and social support.
Conclusions
In this sample, the caregiving experience of mothers of school-age children with asthma is diverse and complex, reflected not only in personal psychological aspects but also in family functioning and social support. Taking into account various factors, such as addressing psychological well-being, emphasizing family and social support, and promoting the sharing of positive experiences, may result in more effective alleviation of caregiving stress for mothers of school-age children with asthma.
Introduction
Asthma is a chronic respiratory disease that affects over 300 million people worldwide.Its prevalence is approximately 5–10% in adults and 20% in children (Citation1). In China,the prevalence of asthma is high among school-aged children (6–14 years old).(Citation2). Asthma, as a stressor, not only has multiple impacts on children’s learning, socializing, and mental health (Citation3,Citation4) but also profoundly affects the daily life, physical and mental health of the primary caregivers and families (Citation5,Citation6). Studies have shown that parents of children with asthma experience varying degrees of anxiety and depression (Citation7,Citation8). 81.52% of caregivers reported high levels of parenting stress and psychological distress (Citation9), 67.57% of caregivers experienced varying degrees of depression, and 29% of caregivers were diagnosed with post-traumatic stress disorder (Citation9,Citation10), It is crucial to explore effective ways to cope with and alleviate the stress. But in most families, mothers are the primary caregivers for the children (Citation11,Citation12). During the long-term care process of the illness, they often choose negative coping strategies such as taking on multiple part-time jobs, sacrificing rest and social activities (Citation12,Citation13). However, these negative coping strategies can prolong and worsen the child’s symptoms, creating a vicious cycle for their treatment and recovery (Citation14,Citation15).
Richard S. Lazarus proposed the stress and coping model in the 1960s, which suggests that the experience of stress primarily depends on cognitive appraisal and coping, two important psychological processes.The transactional theory of stress and coping was translated into a specific intervention framework by Folkman to improve stress management abilities (Citation16). The occurrence of asthma in school-aged children is a significant stressor for the family, and the cognitive appraisal and coping processes of the caregivers are the response to this stressful event. Understanding the experiences of mothers in the caregiving process of children with asthma is of great significance for implementing targeted intervention measures.However, many previous studies (Citation17,Citation18) examining caregivers’ responses to children with asthma mainly relied on cross-sectional surveys involving the distribution of scales and questionnaires, but with limited qualitative research on the experiences of school-age children with asthma and their mothers.Descriptive phenomenology can present an individual’s subjective experience, describe the true situation of phenomena, and explore the experiences and feelings of individuals in a broader and deeper way (Citation19). Therefore, based on the Lazarus stress-coping model, we conducted a descriptive phenomenological study on mothers of school-aged children with asthma to explore their caregiving experiences. This study aims to delve into the cognitive appraisal and coping strategies of mothers of school-aged children with asthma, providing reference for developing targeted intervention measures to enhance the coping skills of mothers and alleviate caregiver stress.
Methods
Participants
In order to ensure sample heterogeneity, we employed purposive sampling based on the mother’s occupation, education level, and duration of the child’s illness when selecting research subjects.Mothers who visited the Pediatric Outpatient Department were asked to indicate their interest to participate in the study. The researchers provided a brief introduction to the participants (personal background, research purpose and significance, etc.) and created a WeChat group for interviews with mothers of school-aged children with asthma (each person’s phone number was added as a note after the group name for contact purposes). The specific interview time and location were determined in advance according to the participants’ needs to ensure the smooth progress of the interview work.Eligible participants were the mothers of children aged 6–14 years (Citation20) with a diagnosis of “Asthma” (Citation21) based on the Guidelines for the diagnosis and prevention of asthma in children, Chinese speaking, and having the ability to provide consent. Participants were selected to ensure diversity in demographics and potential patient caring experience. The sample size of the study is based on the collected data reaching a saturation state (Citation22). From August 2021 to November 2021,Data saturation was achieved at the 14th participant when no new findings emerged and one additional interviews were conducted to confirm the findings,A total of 15 mothers of school-aged children with asthma were included as study participants and were assigned the identifiers P1-P15. The ethical approval by the Deyang People’s Hospital,number for this study is: 2021-04-21-K01.
Development of interview guideline
The interview guideline was developed through literature review (Citation23–25), consultation with three clinical nursing experts in the relevant field, two project team discussions, and pre-interviews: (1) How do you feel during the process of taking care of your child after he (or she) was diagnosed with asthma? (2) What difficulties did you encounter in taking care of your child with asthma (such as negative impacts on work, family, and children’s studies), and how did you respond to these challenges? (3) What impact has the problems encountered in caring for your children had on your daily work and life? (4) Who do you hope to receive or what type of help do you hope to get? (5) What other feelings and thoughts do you have?
Data collection
All interviews were conducted in the pediatric asthma outpatient department, room A07, to ensure the independence and quietness of the interview process. The interviews were conducted by one experienced qualitative researcher (female, Master of Medicine, head nurse). The corresponding author (male, Master of Medicine, director) supervised and oversaw the entire progress of the study.Each interview lasted 30–50 min.Interviews were audio-recorded and transcribed verbatim. (1) Prior to the interview: The researcher introduced themselves to the participants, explained the purpose, content, guidelines, and privacy protection of the interview, and obtained written informed consent from the participants. (2) Formal interview: One-on-one interviews were conducted, with only the researcher and participant present. The entire interview was recorded using the iFlytek Voice Notes app. During the interview, the researcher asked questions based on the interview guideline and provided sufficient time for the participant to express their views and thoughts. Detailed records were kept during the interview, capturing the participant’s language descriptions, tone, and non-verbal expressions. (3) Conclusion of the interview: The researcher informed the participant that their opinions may need to be confirmed during data analysis and summarized the main points discussed during the interview.
Data analysis
All participants completed a brief questionnaire including demographics and background information about their child’s asthma. Within 24 h after the interview, the audio recordings were transcribed into text and combined with the notes taken during the interview for further organization. NVIVO 12.0 qualitative analysis software and the 7-step Colaizzi phenomenological research data analysis method proposed by Liu Ming (Citation26) in 2019 were used for data organization and analysis, which included the following 7 steps: (1) Familiarization with the data: Carefully and repeatedly reading all interview materials. (2) Identification of meaningful statements: Identifying and marking statements in the interview findings that are relevant to the research questions. (3) Construction of meaning units: researcher(scribes and principal investigator) and corresponding author(The facilitator) cross-checked the recurring viewpoints in the interview data and coded them to avoid subjective coding. (4) Clustering of themes: Clustering the important viewpoints from step 3 to form themes/subthemes. (5) Detailed description: Providing a detailed description and explanation of the themes/subthemes formed in step4. (6) Generating basic structure: Summarizing the similar viewpoints. (7) Validating the basic structure: Seeking confirmation from the participants on the analysis results to ensure the accuracy and reliability of the research findings.This study’s findings were reported using the Consolidated Criteria for Reporting Qualitative Research checklist (COREQ) (Citation27).
Results
The total duration of the interviews in this study was 520 min, with an average interview time of approximately 35 min per participant. Among the participants, the mothers had a mean age of 35 years (range: 29–41), and the children with asthma had a mean age of 8 years (range: 6–12). The duration of asthma diagnosis ranged from 12 to 90 months. While 23 individuals expressed interest in participating, only 8 were not able to participate. There were no dropouts among the participants. For detailed information, please refer to . Four main themes encompassing ten sub-themes emerged from the analysis: (1) Negative psychological burden, with sub-themes including anxiety shock, fear of death, guilt, and stigma. (2) Family dysfunction, with sub-themes including impaired quality of life, family emotional crisis, and heavy economic burden. (3) Difficulty in seeking medical treatment. (4) Active response, with sub-themes including emotional adjustment, family empowerment, and social support,please refer to .
Figure 1. Perspectives and experiences of mothers of school-age children with asthma.
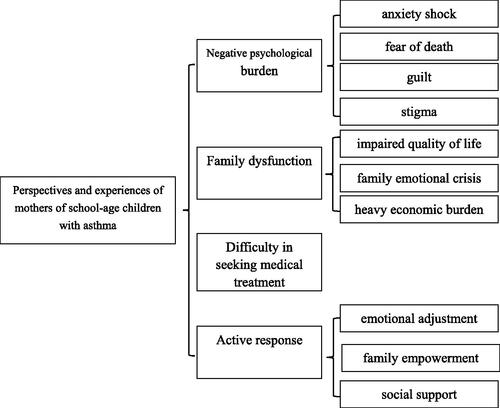
Table 1. mothers and child characteristics.
Theme 1: Negative psychological burden
Anxiety shock
Most of the interviewees believed that asthma had an immeasurable impact on the learning, physical activities, sleep, growth and development, and psychological well-being of school-age children.P1: "(Asthma) has a significant impact on his studies. When he has an attack, he has to take leave from school."; P6: "Every time he exercises intensely, he starts coughing. So, I communicate with the physical education teacher privately and let him participate only in easy physical education classes. For classes with heavy exercise, he doesn’t join. (Frowning)"; P10: "When he runs or jumps too much at home, he starts coughing. I often tell him to stop running and jumping, but sometimes he doesn’t listen. It really frustrates me. (Pounding leg)"; P5: "After getting sick, she couldn’t sleep well. She wakes up every night (between 12-2 am). This has led to her being short in height."; P12: "When the teacher handed out the family survey questionnaire, I filled in that my daughter has asthma. Afterwards, she still wanted to participate in sports events, but the teacher canceled her registration, as well as her qualification to compete for the position of labor committee member. During that time, her mood was very low, and she didn’t even want to go to school."
Fear of death
Due to the weaker self-control and lower asthma control rate of school-age children, coupled with the fact that they have to leave parents with long-term care experience when going to school, mothers bear varying degrees of fear. P13: "Once I couldn’t help but mention it to her, she started getting excited, and then had an attack. She felt like she couldn’t breathe and kept grasping her neck. I was really scared at the time (lowers head, sighs). I shouted at her to calm down, fanned her with an electric fan, and washed her face with cold water. It only eased after a while. Since then, I have been worried about what to do if she has conflict with classmates in school and this happens again? (Wipes tears)";P15: "It worsens every time he catches a cold, back and forth. It’s okay now that we take care of him, but what if he has an attack when he goes to college or work and there’s no one to help him? He’s our only child."
Guilt
During interviews, it was found that more than half of the respondents believed that their child’s asthma was caused by their own inadequate care, lack of attention to initial symptoms, or delayed treatment. P4 stated, "At the beginning, when there was no diagnosis yet, my child coughed frequently, and I didn’t know the reason. I took her to see doctors and even tried traditional Chinese medicine, but none of them worked (sigh). My friends around me kept saying it might be asthma, so I searched for information online, and later found out the condition was getting worse. That’s when I came to the hospital."; P14 said, "My child caught a cold when I was in confinement, and I felt the cold never completely went away after that (looks out the window). Now he catches colds often, and it’s probably because I didn’t know how to take care of him properly at that time and left a hidden disease."; P15 recalled, "He would often ask me, ‘Mom, when will I get better?Hearing that really made me feel guilty, and I thought I was an incompetent mother (chokes up)."
Stigma
Due to varying levels of awareness and understanding of asthma among the general public, some respondents were hesitant to acknowledge the fact that their children had asthma out of fear of being judged or misunderstood. P2: "When people ask me if my kid has asthma, I don’t dare to answer truthfully because I’m afraid they won’t understand the illness." P7: "I feel embarrassed about it (she laughs awkwardly), I can’t accept it internally, and I’m also afraid that my child will be made fun of by classmates (she cries and laughs). Even though we always seek medical treatment promptly whenever we get sick, I can’t accept that my child has this disease (she shakes her head)."
Theme 2: Family dysfunction
Impaired quality of life
Mothers are the primary caregivers for children with asthma, and to ensure that this long-term and arduous task is effectively carried out, they have to sacrifice a significant amount of their time and energy, which leads to a decline in their quality of life. P1: "Nowadays, my child has to take asthma medicine every day and I have to give him nasal drops too. It’s really exhausting (sighs and touches her hair). Whenever I want to go out or meet up with friends, it’s a hassle because I have to bring so many things for him. Taking care of him is even more tiring than going to work."; P3: "Sometimes he coughs for more than an hour at night, so he doesn’t sleep alone now. I’m afraid that something might happen to him."; P4: "I feel like I’m always running to the hospital (touches her hair and smiles wryly). I really want her to get better soon. I already have poor sleep and I’m sensitive. Since she got asthma, I often wake up at night to check if she’s wheezing or has a fever. If we go out and she gets too tired, I have to keep an eye on her at night, afraid that she might feel uncomfortable."; P13: "She was so excited after taking ShunErNing(Chinese trade name for Montelukast.) that she didn’t want to sleep until midnight. (shaking her head)."
Family emotional crisis
The family is the strongest pillar of support for children with asthma during long-term treatment; however, during the interviews, it was discovered that the fathers were less involved, and the intervention of the elderly had a certain degree of impact on family relationships. P5: "Almost everything concerning the child is handled by me. Regarding the father’s role, I feel very frustrated and don’t want to talk about it." (helpless expression); P6: "The father is very busy with work and plays with his phone after work. He doesn’t have time to take care of the child, and everything is my responsibility." (frowning); P14: "The grandmother is the commander-in-chief. If she says not to use the asthma inhaler, then there’s nothing we can do. Everyone in the family has to obey her. His grandpa and father are used to it. She had a previous illness and has a disability in her foot, so we have to indulge her." (sighing)
Heavy economic burden
Asthma requires long-term and standardized treatment, and a quarter of the respondents had to take frequent leave to better care for their children, resulting in a decrease in total family income. In addition to the ongoing expenses related to asthma treatment, additional tutoring fees further add to the heavy economic burden on families. P1: "It costs over 10,000 yuan a year, which is still expensive and burdensome." (sadly bowed head); P8: "Since he got sick, I have used up all the medical insurance on him. I haven’t even had a chance to use it myself (awkward smile). Plus, I have to take leave from work from time to time for follow-up appointments, and it ends up costing me money. It’s really annoying.";P10: "Sometimes, to make up for his studies, I have to sign him up for tutoring classes, which are expensive and cost more than his medication expenses. But we don’t have a choice; we have to attend." (shakes head)
Theme 3: Difficulty in seeking medical treatment
Asthma is characterized by its complex and difficult-to-cure nature, and once diagnosed, most children require long-term hospital follow-up. Some of the interviewees reported experiencing varying degrees of difficulty in seeking medical treatment during the long-term treatment process. For example, P8 said, "I initially went to Chongqing Children’s Hospital for treatment in 2016, and then had to go back for follow-up appointments every three months or so. I saw a lot of different specialists, and it was really frustrating. The journey to Chongqing was long and we had to stay in a hotel at night. It’s been so painful for so many years." P1 said, "I hope more doctors can treat this disease. It’s time for my child’s follow-up examination, but we can’t get an appointment with Dr. Deng or Professor Jiang." P2 added, "At the beginning of treatment, we often had to go to the emergency room at night. During winter nights, children get sick a lot, and we would wait in line for hours. It’s really chaotic." Finally, P8 said, "We waited for three hours and saw the doctor for only three minutes. Sometimes, we wanted to ask the doctor more questions, but there was no time because there were too many people outside."
Theme 4: Active responses
As a mother of a school-age child with asthma, despite the various burdens of caring for asthma, some mothers reported many positive changes in their emotional well-being, family, and social support.
Emotional adjustment
Almost all mothers of children with asthma experience varying degrees of negative emotions and express the need to face and adjust to them in a timely manner. P3: "As a nurse, I think asthma is not that scary as long as it’s well controlled. There are many treatments available now."; P4: "Since my daughter was born, she has become very sensible and actively helps me with some things. Both her dad and I feel that if children can be optimistic like this, we should be more positive."; P7: "Since the diagnosis has been confirmed, we should listen to the doctor and get treated properly. It’s better than always dragging and not knowing what’s wrong."
Family empowerment
The positive impact of family support on individuals and family members is self-evident. P7: "My husband always says that money is not something you should worry about. Even if the sky falls, he’s still here for me, and he really does it. This makes me very relieved."; P15: "Our family is very harmonious, and along the way, my grandparents have helped us a lot. My husband is also a relatively optimistic person. He often comforts me and encourages me. They are my spiritual pillar (smiling)."
Social support
Seeking social support can help alleviate burdens to some extent. P2: "After my child was diagnosed with asthma in 2018, I was particularly worried and scared. I tried to learn on my own and asked friends at the hospital for help. They were very enthusiastic and even helped me make appointments."; P9: "Now there is a WeChat group for parents of asthmatic children at the city hospital. Whenever I have questions, I can ask in the group. Sometimes, Someone(a nurse) can even help me make appointments for checkups. It’s really helpful."
Discussion
Guided by Lazarus’s stress-coping model, this study used a descriptive phenomenological approach in qualitative research to conduct in-depth interviews with 15 mothers from Sichuan, China caring for school-age children with asthma to understand their caregiving experiences. Through our research, we have identified four main themes: “negative psychological burden”,“dysfunctional family dynamics”, “difficulties in seeking medical care” and “positive coping strategies” .Additionally, corresponding sub-themes have been identified for each theme, providing reference for targeted intervention measures to enhance the coping skills of mothers of children with asthma and alleviate caregiver stress.
The majority of mothers mentioned experiencing varying degrees of negative psychological burden, such as anxiety, fear, and guilt, during the long-term caregiving process. This may be related to the fact that once asthma is diagnosed, it accompanies the child throughout their life, and asthma treatment is difficult and lengthy (Citation28). The results of studies by Jianli Chen (Citation9), PARS H (Citation29), ALZAYER R (Citation30), FORONDA C L (Citation6), and others also show that caregivers of children with asthma experience complex emotional reactions and distress during the caregiving process. This suggests that healthcare professionals should not only focus on disease control in children with asthma but also pay attention to the psychological well-being of mothers. Psychological interventions such as cognitive-behavioral therapy, family therapy, motivational interviewing, and problem-solving therapy (Citation11,Citation31) may be necessary to reduce the generation of negative emotions.
Family and social support are crucial. Many mothers expressed experiencing varying degrees of insufficient family and social support, which negatively impacted their quality of life, strained family relationships, and increased financial pressure. This aligns with the findings of Licari’s (Citation32)study, suggesting that the specific nature of asthma and weak social support systems may contribute to these issues (Citation33,Citation34). Research has shown that a strong support system can enhance caregivers’ ability to cope with challenges (Citation5,Citation28). It is recommended for family members, especially spouses, to understand and support each other, take turns in caring for and accompanying the child. Additionally, at the governmental and societal levels, providing more job opportunities or flexible working hours for caregivers (Citation28) and further improving the social medical insurance system, as well as implementing special medical insurance programs for children with asthma and promoting affordable medication (Citation35), can help alleviate the physical and mental stress of mothers as the primary caregivers.
Difficulties in seeking medical care are also a prominent issue. Due to the chronic and recurrent nature of childhood asthma, long-term follow-up is often required once diagnosed (Citation36). However, there is a significant gap between the healthcare needs and supply for children in China (Citation37), leading to difficulties in seeking medical care for some participants. Firstly, at the national level, policies should be implemented to reduce the disparity in the distribution of medical resources between different regions and urban and rural areas. For example, establishing medical consortiums between different levels of medical institutions and encouraging pediatricians from tertiary hospitals to provide outpatient services at primary care facilities can help effectively redirect patients. Secondly, encouraging the establishment of standardized pediatric asthma clinics (Citation38,Citation39) and increasing the availability of weekend pediatric asthma specialty clinics (Citation40) can alleviate difficulties in seeking medical care to some extent.Finally, utilizing internet platforms can accelerate the construction and expansion of internet hospitals providing “convenient medical treatment at your fingertips”for asthma patients and caregivers and easing the current difficulty in accessing medical treatment offline (Citation41).
Some mothers expressed that although they bear a series of burdens in the long-term caregiving process of asthma, some positive changes are also occurring. This is consistent with the findings of Hedi Jiang et al., which suggest that caregivers not only bear the burden of the disease in the long-term caregiving process but also experience a series of positive experiences (Citation42). Previous studies have shown that positive psychological change can help individuals develop stronger beliefs and values, which can help buffer the negative effects of stressors (Citation43). Therefore, healthcare professionals and society can fully acknowledge the personal growth of caregivers to stimulate the generation of positive experiences. At the same time, establishing communication platforms between caregivers, such as creating WeChat or QQ groups, organizing parent-child activities, and peer support meetings (Citation25,Citation28,Citation44), can facilitate the sharing of resources for positive experiences.
Strengths and limitations
Currently, there is a lack of research on the caregiving experiences of mothers of school-age children with asthma, both domestically and internationally,The findings of this study will contribute to a deeper understanding of their caregiving experiences and provide support strategies for them.Of course,This study also has certain limitations. Firstly, during the general data collection, we did not gather information on the severity of asthma, which may restrict our ability to discuss the results in detail.Secondly,The participants in this study all belonged to the same ethnic/cultural group and were from Sichuan, China. Therefore, they may not represent all mothers of school-aged children with asthma, limiting the generalizability of the study findings.
Conclusion
In this sample, the caregiving experiences of mothers of school-age children with asthma are diverse and complex, encompassing not only individual psychological aspects but also family functioning and social support. By considering various factors such as addressing psychological well-being, emphasizing family and social support, and fostering the sharing of positive experiences, developing coping strategies may be more effective in alleviating the caregiving stress experienced by mothers of school-age children with asthma.
Authors’ contributions
Fang Yang: The principal investigator, responsible for the development, analysis, and paper writing of the research; Cheng Chen and Xuexue Deng: Participated in data collection; Tingting Hu and Dan Bi:Participated in data analysis, Huawei Li: Guidance throughout the research process and proofreading for English language refinement. All authors read and approved the final manuscript. All authors read and approved the final manuscript.
Supplemental Material
Download MS Word (11.2 KB)Acknowledgments
We thank all the participants in this study.
Declaration of interest
The authors declare there is no Complete of Interest at this study.
Disclosure statement
The authors report no conflicts of interest.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Participants of this study did not agree for their individual responses to be shared publicly due to privacy or ethical restrictions, so this information is not available.If you want to inquire about registration information, can be made at https://www.chictr.org.cn/bin/project/edit?pid=131367 (Chinese Clinical Trial Registry Registration number:ChiCTR2200056746)
Additional information
Funding
References
- Bagnasco D, Paggiaro P, Latorre M, Folli C, Testino E, Bassi A, Milanese M, Heffler E, Manfredi A, Riccio AM, et al. Severe asthma: one disease and multiple definitions. World Allergy Organ J. 2021;14(11):100606. doi:10.1016/j.waojou.2021.100606.
- Mou JH, Shao MJ, Liu CH, et al. Comparison of food allergy among children with bronchial asthma and children without bronchial asthma in Chinese cities. Chinese Clin J Pract Pediatr. 2018;33(9):684–687.
- Wu YH, Liu F, Tang XJ, et al. Study and effect analysis of action plan for bronchial asthma management in children. Chinese J Pract Med. 2020;15(36):41–44.
- Wang G, Wang F, Gibson PG, Guo M, Zhang W-J, Gao P, Zhang H-P, Harvey ES, Li H, Zhang J, et al. Severe and uncontrolled asthma in China: across-sectional survey from the Alustralasian Severe Asthma Network. J Thorac Dis. 2017;9(5):1333–1344. doi:10.21037/jtd.2017.04.74.
- Gibson-Young LM, Aroian KJ, Weglicki LS, Lang JE, Norris CL. Interviens with aregivers during acute asthma hepitalisatins. J Asthma. 2020;57(7):778–786. doi:10.1080/02770903.2019.1602875.
- Foronda CL, Kelley CN, Nadeau C, Prather SL, Lewis-Pierre L, Sarik DA, Muheriwa SR. P’sychobgieal and socioecmnomie burdens faed by family cargivers of children with asthm; an integative review. J Pediatr Health Care. 2020;34(4):366–376. doi:10.1016/j.pedhc.2020.02.003.
- Hu J. Effect of relaxation training on anxiety and depression in parents of children with asthma. Nanchang University, 2021.
- Kheirabadi G, Malekian A, Fakharzadeh M. Comparative Study on the Prevalence of Depression in Mothers with Asthmatic, type I Diabetic and Healthy Children. J Res Behav Sci. 2007;5(1):21–25.
- Chen JL, Chu XL, Li Y, et al. Effect of social support on family intimacy adaptability and depression level of parents with bronchial asthma. Maternal Child Health Care China. 2021;36(8):1865–1868.
- Guo M, Gao G, Guo J, Wen L, Zeng L. Burden among caregivers for children with asthma:a mixed-method study in Guangzhou, China. Int J Nurs Sci. 2015;2(4):394–401. doi:10.1016/j.ijnss.2015.10.004.
- Wang HH, Fan H, Zhu WP. Qualitative study on maternal stressors in school-age children with asthma. Modern Nurse. 2022;29(3):113–116.
- Borhani F, Asadi N, Mohsenpour M. The experiences of mothers with asthmatic children: a content analysis. J Caring Sci. 2012;1(3):115–121. doi:10.5681/jcs.2012.017.
- Rullander A-C, Lundström M, Lindkvist M, Hägglöf B, Lindh V. Stress symptoms among adolescents before and after scoliosis surgery:correlations with postoperative pain. J Clin Nurs. 2016;25(7–8):1086–1094. doi:10.1111/jocn.13137.
- Chong Y-Y, Mak Y-W, Leung S-P, Lam S-Y, Loke AY. Acceptance and Commitment Therapy for Parental Management of Childhood Asthma: an RCT. Pediatrics. 2019;143(2):e20181723. doi:10.1542/peds.2018-1723.
- Cano-Garcinuño A, Mora-Gandarillas I, Bercedo-Sanz A, Callén-Blecua MT, Castillo-Laita JA, Casares-Alonso I, Forns-Serrallonga D, Tauler-Toro E, Alonso-Bernardo LM, García-Merino Á, et al. Looking beyond patients: canparents’quality of life predict asthma control in children. Pediatr Pulmonol. 2016;51(7):670–677. doi:10.1002/ppul.23336.
- Folkman S, Chesney M, Mckusick L, Ironson G, Johnson DS, Coates TJ, Lazarus RS, Folkman S. 1991. Translating coping theory into an intervention. In J. ECKENRODE (Ed.), The social context of coping. (pp. 239–260). New York: Plenum Press. 1984. Stress, appraisal, and coping. New York: springer.
- Wang JN, Li AQ, Li TT, et al. A study on the correlation between caregiver burden and quality of life of asthmatic children. Chinese Journal of Modern Nursing. 2018;24(20):2414–2418.
- Foronda C, Gonzalez JM, Snowden K, Prather S, Majilton C, Weisman A, Parmeter S, Herrera A, Gattamorta KA, Gonzalez JE, et al. Improving knowledge and decreasing depressive symptoms in caregivers of children with asthma through the asthma academy: a randomized controlled trial. International Journal of Nursing Studies Advances. 2021;3:100047. doi:10.1016/j.ijnsa.2021.100047.
- Brown J, Sorrell JH, McClaren J, Creswell JW. Waiting for a liver transplant. Qual Health Res. 2006;16(1):119–136. doi:10.1177/1049732305284011.
- Cui Y, Yang SF. Pediatric Nursing. Beijing: People’s Medical Publishing House, 2017. 302–303.
- Bao YX, Chen AH, Fu Z. Guidelines for the diagnosis and prevention of asthma in children(2016edition). Chinese J Pediatr. 2016;54(03):167–181.
- Wang Y. Method is more important than conclusion–introduction of qualitative research methods and social science research. Journal of Haidian University, 2001;(01):85.
- Ou MX, Zheng Z, Liu Y, et al. A qualitative study on the disease care needs of asthma patients and their family caregivers. Shanghai Nurs. 2020;20(06):19–23.
- Zhou CX, Li ZM. Phenomenological study on parental care experience of children with asthma. Modern Nurse. 2018;25(09):122–124.
- Zhang HM, Pan XZ, Zhang YL, et al. Qualitative study on nursing experience of asthmatic children caregivers. Chinese Rural Med. 2021;28(15):67–68. doi:10.19542/j.cnki.1006-5180.005467.
- Liu M. Colaizzi The application of seven steps in the analysis of phenomenological research data. J Nurs Sci. 2019;34(11):90–92.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042.
- Hu JJ, Wang JN. Cuiying Gong et al. Meta-integration of care experience for family caregivers of children with asthma. Nurs Manage China. 2023;23(01):79–86.
- Pars H, Soyer Ö, Şekerel BE. The experiences, perceptions and challenges of mothers managing asthma in their children:a qualitative study. Turk J Pediatr. 2020;62(5):734–745. doi:10.24953/turkjped.2020.05.004.
- Alzayer R, Chaar B, Basheti I, Saini B. Asthma managem ent experiences of Australians who are native Arabic speakers. J Asthma. 2018;55(7):801–810. doi:10.1080/02770903.2017.1362702.
- Law E, Fisher E, Eccleston C. Psychological int erventions for parents of children and adolescents with chronic illness. Cochrane Database Syst Rev. 2019;3(3):9660.
- Licari A, Ciprandi R, Marseglia G, Ciprandi G. Anxiety and depression in adolescents with asthma and in their parents:a study in clinical practice. Monaldi Arch Chest Dis. 2019;89(3):507–510. doi:10.4081/monaldi.2019.1063.
- Yin Y, Lu YM, Qiao J, et al. Clinical diagnosis and treatment strategies for bronchial asthma in primary children: expert recommendations from Pudong New Area/Fengxian District of Shanghai (with peer review). Chinese General Med. 2020;23(6):633–643.
- Ableti J, Turson C, Upul D. Research progress on the correlation between bronchial asthma and psychological disorders. J Tubercul Pulmon Dis. 2020;1(4):285–288.
- Ughasoro MD, Eze JN, Oguonu TO, et al. Burden of childhood and adolescence asthma in Nigeria: disability adjusted life years. Paediatr Respir Rev. 2022;41:61–67. doi:10.1016/j.prrv.2021.07.004.
- Yang JY, Gao WJ. Effects of group acceptance and commitment therapy combined with Roy adaptation model on perceived disease burden and sleep quality in elderly patients with chronic asthma. Clin Res Pract. 2021;6(28):159–161.
- Pan ZH, Yao M, Qi JN. The present situation of children’s seeking medical care in our country and the problems and countermeasures of carrying out graded diagnosis and treatment. Chin General Pract. 2018;21(10):1177–1182.
- Qian QF. Effect of peer demonstration education on the success rate of pulmonary function monitoring and rehabilitation effect in preschool children with asthma. Nurs Pract Res. 2019;16(16):111–113.
- Lu CJ, Du CF, Huang F. Effect of standardized outpatient nursing management on disease control and family function in children with asthma. Nurs Pract Res. 2021;18(20):3120–3123.
- Chen ZH, Liu Y, Wang RL, et al. Maternal environment and drinking risk factors during pregnancy in asthma with neuropsychiatric comorbidity. Chin J Appl Clin Pediatr. 2019;34(9):675–679.
- Wu DM, Cui WB, Yu GJ. Analysis on the operation strategy of Internet Hospital in our country. Chinese Hosp. 2021;25(10):79–80.
- Jiang HD, Jiang WL, Xiao YL, et al. Effect of continuing gratitude emotion intervention after discharge on long-term positive experience and care burden of spouses of patients with brain tumor after operation. Chinese J Modern Nurs. 2017;23(19):2541–2544.
- Park JH, Lee JS. Predictors of post-traumatic growth in young adult burn survivors. Burns. 2021;48(4):744–752. doi:10.1016/j.burns.2021.08.018.
- Xu SD, Xie J, Wang Q, et al. Qualitative Study on the stress of primary caregivers of asthmatic children in two-child families. Modern Nurses. 2023;30(05):122–125. doi:10.19793/j.cnki.1006-6411.2023.15.030.