

Abstract
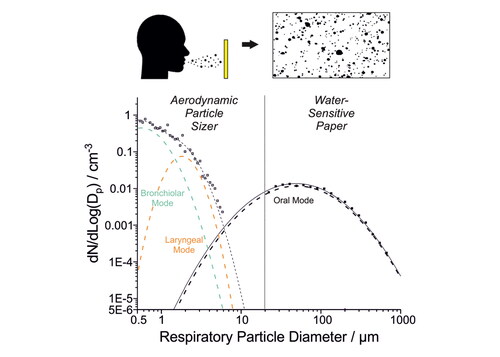
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has brought renewed attention to respiratory aerosol and droplet generation. While many studies have robustly quantified aerosol (<10 µm diameter) number and mass exhalation rates, fewer studies have explored larger droplet generation. This study quantifies respiratory droplets (>20 µm diameter) generated by a cohort of 76 adults and children using a water-sensitive paper droplet deposition approach. Unvoiced and voiced activities spanning different levels of loudness, different lengths of sustained phonation, and a specific manner of articulation in isolation were investigated. We find that oral articulation drives >20 µm droplet generation, with breathing generating virtually no droplets and speaking and singing generating on the order of 250 droplets min−1. Lip trilling, which requires extensive oral articulation, generated the most droplets, whereas shouting “Hey,” which requires minimal oral articulation, generated relatively few droplets. Droplet size distributions were all broadly consistent, and no significant differences between the children and adult cohorts were identified. By comparing the aerosol and droplet emissions for the same participants, the full size distribution of respiratory aerosol (0.5–1000 µm) is reported. Although <10 µm aerosol dominates the number concentration, >20 µm droplets dominate the mass concentration. Accurate quantification of aerosol concentrations in the 10–70 μm size range remains very challenging; more robust aerosol analysis approaches are needed to characterize this size range.
Graphical Abstract
EDITOR:
Data availability
Data underlying the figures are publicly available in the BioStudies database (https://www.ebi.ac.uk/biostudies/) under accession ID S-BSST925.
Acknowledgments
The authors acknowledge funding from the Engineering and Physical Sciences Research Council (EPSRC, EP/V050516/1). B.R.B. acknowledges the Natural Environment Research Council (NE/P018459/1). J.H. and L.P.M. acknowledge funding from the EPSRC Centre for Doctoral Training in Aerosol Science (EP/S023593/1). L.P.M. acknowledges funding from EPSRC IILF (EP/R513179/1). K.E.J.P. was supported by the Imperial College Clinician Investigator Scholarship. Fortius Surgical Centre, Marylebone, London, is acknowledged for the generous provision of space to conduct the measurements. Vyaire MedicalTM is acknowledged for the loan of CPET testing equipment. We acknowledge the participants for their contributions to this study.