
Abstract
Objective
To explore the Nordic municipal health and care services’ ability to promote principal goals within care for older people during the COVID-19 pandemic.
Design and setting
Two surveys were conducted among managers of municipal health care services for older people in Denmark, Finland, Norway and Sweden; the first around 6 months into the pandemic (survey 1), and the second around 12 months later (survey 2). Data were analysed through descriptive statistics, and multiple regression (OLS).
Subjects
1470 (survey 1, 2020) and 745 (survey 2, 2021) managers. 32% in home care, 51% in nursing homes, 17% combined.
Results
In all countries the pandemic seems to have had more negative impact on eldercare services’ ability to promote an active and social life, than on the ability to promote or enhance older people’s mental and physical health. The regression analysis indicates that different factors influence the ability to promote these goals. Managers within nursing homes reported reduced ability to promote mental and physical health and an active social life to a significantly lower degree than managers of home care. The effect of three prevention strategies (lock down, testing, and/or organisational change), were explored. Organisational change (reorganize staff and practice, restrict use of substitutes) tended to impact the units’ ability to promote a social life in a positive direction, while lock down (areas, buffets etc) tended to impact both the ability to promote mental/physical health and a social life in a negative direction.
Conclusion
Measures that can improve opportunities for an active and social life during a pandemic should have high priority, particularily within home care.
KEY POINTS
It is important to learn from how the COVID-19 outbreak in 2020 affected the municipal health and care services’ ability to achieve principal goals within care for older people.
The pandemic had a more negative impact on the services’ ability to promote an active and social life, than on their ability to promote or enhance mental and physical health.
Measures that can improve opportunities for an active and social life during a pandemic situation should have high priority, particularily within home-based care.
Introduction
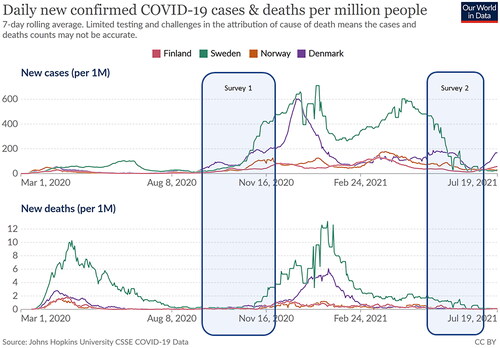
The Nordic countries share many similarities in their health care services for older people [Citation1]. Yet, they in many respects reacted differently to the outbreak of the COVID-19 pandemic. While the Swedish national health authorities, for instance, hesitated in their recommendation of tough preventive measures for the municipal health care service, or favoured optional or less restrictive approaches [Citation2], Denmark, Finland and Norway implemented a strict set of measures at an early stage [Citation3,Citation4]. The pandemic also had different consequences for older people in these countries. Sweden experienced a much higher disease burden than other Nordic countries, where the proportion of COVID-19 cases among people 80+ was about twice that of the other Nordic countries. Much public debate has been devoted to the differences between these neighbouring countries in both COVID-19 strategies and outcomes for various groups of the population, including older people in need of care [Citation2].
In this paper we examine how managers of health care services at the municipal level in Denmark, Finland, Norway, and Sweden evaluate their service or unit’s ability to sustain or promote principal goals within care for older people during the pandemic, and which factors that may explain variations between the four countries. We draw on two sets of survey data, one set from the first half year after the outbreak of the pandemic, and the second almost one year later. In these sets of data, we look specifically into how the outbreak affected the possibility of maintaining key principles within active and healthy ageing.
Health care services and age-friendly strategies in the Nordic countries
Over the last decades, principles involved in the strategy ‘active and healthy ageing’ has been vital to meet challenges due to an ageing population in western countries [Citation5]. In the Nordic countries, the ageing population is also a key issue in these countries’ welfare policies, yet with somewhat different strategies chosen [Citation6–8].
The Nordic countries expect a doubling of the proportion of people aged 80+ by the year 2060, from four to eight per cent, which is expected to provide substantial challenges within several areas, health care service delivery included [Citation6]. The strategies for active and healthy ageing in all the Nordic countries consists of four areas: Age friendly places/communities, intergenerational housing and meeting places, prevention of loneliness and social isolation, and active and healthy ageing through welfare technology [Citation6].
Norway differs somewhat from the other Nordic countries because the country has an explicit strategy for an age-friendly society, whereas the other Nordic countries integrate ageing related aspects in different parts of their welfare policy areas such as care, housing and labour market. In Sweden, strategies involved in care for older people are driven from national regulations and specific values that to a large extent allow municipalities to decide how services and support should be provided, while in Denmark and Norway the national health authorities (Sundhedsstyrelsen and Helsedirektoratet) have played a more active role in the strategy for an age-friendly society [Citation6]. In Finland, care for older people have been part of a more general public health strategy instead of a free-standing strategy, where policies for older people are primarily integrated into various political sectors, such as environmental sector, educational sector, and law [Citation6]. Nevertheless, despite the differences, all four Nordic countries by-and-large share the four-area strategy mentioned above.
The COVID-19 pandemic has increased the attention drawn to ageing, because of measures such as social distancing and lockdown of social arenas that in particular affected the oldest age groups negatively [Citation9]. Tough restrictions in some places and increased mortality rates among older people in other places, indicate that issues concerning ageing are closely related to place, and as such support discussions on age and place in publications within geographical gerontology [Citation10–14]. Some studies also indicate that communities that were forerunners in age-friendly planning [Citation15] seem to have been more prepared to respond to the needs of older people during COVID-19 [Citation9].
Care for older people in Nordic countries
Care for older people is in the Nordic countries characterized by a universal provision, i.e. provided to all citizens according to their needs and with a high level of public funding [Citation16,Citation17]. During the last decades de-institutionalization has been a general trend for long-term care in all these countries. Denmark and Sweden, however, have taken this trend a step further than Norway. In Denmark institutional care was suspended through the introduction of a new act (Eldreboliglov) in 1987, and from then on only a low volume of established nursing homes remained. Five years later (1st of January 1992) a similar change occurred in Sweden (Ädelreformen). It has, however, been debated whether this formal de-institutionalisation in Denmark and Sweden to some extent has been replaced by a re-institutinalisation [Citation18,Citation19]. Home care dominates also in Norway, but long-term care in nursing homes is still offered for people with extensive need of daily care [Citation18]. Finland, on the other hand, has recently chosen a model of assisted living with 24-h services that replaces institutional care. Nevertheless, across the countries the overall strategy seems to be that people can stay in their own home for as long as possible [Citation20].
Pandemic responses and eldercare service provision
In all Nordic countries older people have been regarded as a group in particular risk, from the beginning of the pandemic [Citation21]. The protective measures and other responses to the pandemic, have affected the ageing population particularly hard. All Nordic countries have had restrictions within eldercare, and all have recommended older people to limit their social contacts. Contacts with family members have also been reduced or in periods been “forbidden” or strongly restricted [Citation6]. Studies have, however, indicated that social distancing have been too general, and produced unnecessary loneliness among older people [Citation22–27]. The pandemic has also increased the severity of existing challenges within the services, such as mental health problems among users [Citation6].
Finding solutions to problems that social distancing and other restrictive measures have caused among older people has become urgent [Citation28]. National and local authorities have changed administrative routines and management techniques, and experimental forms of governance have emerged, implying both opportunities and risks [Citation29–31]. The use of welfare technology and digital conferences between service users and providers have been beneficial for both users and providers. Digital interaction has also been promoted as a means to maintain contact between users of health care services and their family members.
It is reasonable to believe that eldercare services may be affected by both the pandemic indirectly through implemented measures, and directly through staff and/or users of the services being infected by COVID-19.
Aim and research questions
The primary aim of the paper is to explore the municipal health care services’ promotion of an active and healthy ageing during the first 1,5 years of the COVID-19 pandemic in four Nordic countries: (1) To what extent has the pandemic affected the services’ capability to achieve the principal goal of healthy ageing among older people? (2) To what extent has the pandemic affected the capability to promote an active and social life among older people? We aim to explain and understand potential differences between the four countries’ health care services and investigate how potential differences may be related to various factors such as contagion level, type of service (nursing home versus home care), sector (private versus public), types of prevention measures, and size of unit.
Material and methods
Data
The present paper draws on two web-based surveys carried out in Denmark, Finland, Norway, and Sweden in a collaboration between four research teams, one from each country. The surveys explore in general how managers responded to and experienced the COVID-19 crisis through different phases of the pandemic (). The surveys’ design and content were partly informed by data from 25 qualitative interviews with Danish managers of different health care services for older people, and from members of the collaborating research teams which ensured comparability between the countries. Some of the items in the questionnaire used in this article were based on these interviews (prevention measures, see measurement section) while others (service type, sex, age, education, size of unit) were based on scales and categories commonly used in microdata surveys. The two items measuring the dependent variable (performance) in the article were constructed uniquely for this survey, and were based on formulations in policy documents on health care for older people in the Nordic countries, as well as discussions among the research members. The survey was pretested among a small sample of Danish eldercare managers, and the questionnaire was adjusted where necessary based on their input and considerations by members of the research teams with expertise on eldercare. The questionnaire included 103 questions with separate items for three separate phases of the pandemic, and an additional number of questions related to each respondent’s individual and organizational background. The final Danish version of the questionnaire was translated into Norwegian, Swedish, and Finnish respectively. The Nordic research team had frequent digital meetings where wordings and translation issues in the questionnaire were discussed, in order to ensure comparability across countries. Data from the survey including details on the development of the questionnaire are also presented in [Citation21,Citation28,Citation32].
Figure 1. Daily new confirmed COVID-19 cases and deaths per million people from March 1st 2020 to July 19th 2021, Denmark, Finland, Norway, Sweden. (https://ourworldindata.org). Survey 1 = Survey 1 data collection period (2020). Survey 2 = Survey 2 data collection period (2021).
Sample
The two surveys represents repeated cross-sectional data, where both surveys targeted all managers of public and private nursing homes and home care services in all municipalities in Denmark, Finland, Norway and Sweden, at two time points with a 12 months interval. The surveys were conducted anonomously , and we can only study changes at country level, not at individual (manager) or municipal level. The managers were reached by email either indirectly through a municipal registry (Finland, Norway, Sweden) or directly through personal (work) email addresses (Denmark). Three reminders followed the initial invitation of each survey. We do not have exact knowledge about the size of the eligible population of managers in each country. What we do know, is that in Denmark, 93% of the municipalities were represented in the first survey and 88% in the second. Similarly, 39% and 28% were represented in Finland, 41% and 40% in Norway, and 52% and 34% in Sweden. Entries from each municipality varied from one up to 38 in the first survey and up to 23 in the second. Data for the present paper was derived from both the first (2020) and second survey (2021) with a total of 1300 complete responses (1955 including incomplete responses) for the first survey, and 694 complete responses (1183 including incomplete responses) for the second survey.
A comparison of sex, age, education level and tenure among the respondents in the first and the second survey does not indicate any substantial differences in sample characteristics between the two surveys (see ). A test for non-respondent bias [Citation33] in the Danish data set in the first survey showed only few and unsystematic statistically significant (p < .05) differences in the data between early and late responses.
Ethics
Data collection has followed the General Data Protection Regulation (GDPR). From each respondent informed consent was obtained at the opening page of the online questionnaire. In the invitation respondents were provided information on the purpose of the study, made aware of aspects such as confidentiality, that participation in the study was voluntary and that data would be collected, processed and reported in such a way that individual respondents could not be identified.
Measurement
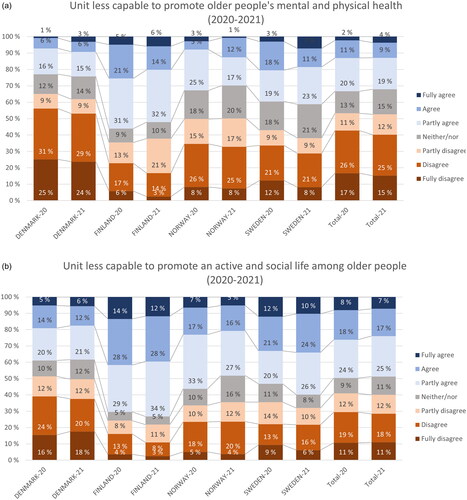
Ability to promote activity and health, is the main (dependent) variable, and is measured by two items: The managers were asked whether their unit during the corona pandemic had become less capable to promote (1) the mental and physical health of older people, and (2) an active and social life among older people. The response scale was a Likert scale with seven values, from 1 (fully disagree) to 7 (fully agree). Both statements were formulated negatively (“unit less able to”). Thus, positive scores/coefficients indicate decline or change in a negative direction, while negative scores/coefficients indicate improvement or a change in a positive direction (). We refer to these two indicators as “health promotion” and “social promotion”, respectively. We note that the indicators are measuring performance in a relative sense, as perceived changes due to the pandemic, and cannot be taken as an indicator for exact changes.
Figure 2. Perceived promotion of health and promotion of social life by country (2020 = survey 1, and 2021 = survey 2).
Country dummies:
35% of our respondents are from Denmark (38% survey 1/32% survey 2), 24% from Sweden (23% survey 1/24% survey 2), 22% from Norway (20% survey 1/23% survey 2) and 19% from Finland (19% survey 1/20% survey 2). When we compare this distribution with the population distribution across the four countries (Denmark representing 22%, Sweden 38%, Norway 20%, and Finland 21%, source: https://en.wikipedia.org/wiki/Nordic_countries), it becomes evident that Denmark has a significantly higher response rate compared to the other three countries. It is likely that the higher response rate in Denmark can be explained by the more direct sampling strategy in this country, compared to the three other countries. The variable is recoded into dummies. Sweden is used as the reference category in the regression models. We have also estimated marginal means for each country to enable a detailed country comparison (). Different sample sizes between the countries makes it necessary to control for country in the regression model . As a support we have also estimated models at country level ().
Table 1. Estimation of country-level marginal means.
Experienced COVID-19 contagion in the unit
The managers were asked about the number of C19 contagion cases among staff (and/or their family/social network) and patients/users (and/or their family/social network) for three specified measurement periods in each of the two surveys (). In total 603 of the 1470 (41%) managers providing valid responses for the question in the first survey, and 546 of 745 (83%) in the second (2021), indicated that they had experienced one or more contagion cases in their unit. The Swedish managers reported contagion cases more often than managers in any of the other three countries, with 73% in 2020 and 97% in 2021. In comparison, 40% and 83% reported one or more cases in Denmark, 26% and 58% in Norway, and 20% and 40% in Finland. The average number of cases was also substantially higher in Sweden when contagion had been present in the unit with 11.8 cases on average in 2020 and 24.1 in 2021. Corresponding figures for Denmark are 5.7 and 13.1, for Finland 5.4 and 5.5, and for Norway 5.0 and 8.5. Since the original variable was skewed and many zero values prevented the use of log-transformations, we applied a dummy version of the variable indicating whether contagion cases were present (coded as 1) or not (codes as 0).
Table 2. Sum of contagion cases among staff or citizens reported by managers (2020 = survey 1, and 2021 = survey 2).
Size of unit
We have used the number of full-time employed persons in the unit as indicator for organisational size. Size of unit is correlated with contagion cases, but a Pearson’s r = 0.37, indicates that multicollinearity is not a substantial problem. The variable was log-transformed when included in the model to adjust for non-normality [Citation34].
Service type (dummies)
51% of the Nordic respondents manage units within nursing homes while 32% manage home care units, and 17% manage both categories of units. The variable is recoded into dummies, where “home care” is used as the reference category in the regression model.
Prevention measures
The survey contained a set of questions with the response options yes or no for mapping the use of a total of 17 measures that the initial interviews had identified as commonly used for preventing COVID-19 contagion in the manager’s own care unit. Through an explorative factor analysis (EFA) with principal axis factoring (PAF) as extracting method and varimax as rotation method we were able to identify three common factors with a meaningful theoretical interpretation. The analysis was guided by consideration of scree plots, the items’ factor loadings, and the factors’ eigenvalues. Each of the three factors relied on three items accounting for a total of 36% of the total variation in the 17 items. In the final solution with tree factors and nine items, 57.9% of the variance was explained. All nine primary loadings were 0.35 or higher (eight above 0.47 and six above 0.63), which are all above the recommended minimum of 0.32 [Citation35].
The first factor relates broadly to organizational changes (labelled ‘prevention 1’) and consists of the survey items indicating the use of ‘splitting staff in smaller teams’, ‘restricting use of substitutes for permanent staff’, ‘reorganizing care in order to reduce users’ social contact.’ The second factor relates to the lockdown of areas and facilities (‘prevention 2’) and consists of items for ‘sectioning/closing of inhouse areas’, ‘avoiding/closing buffets for meals, restricting entrance/visits’. The third factor relates to test and isolation of residents (‘prevention 3’) and consists of items for ‘testing of all new users/residents’, ‘control test of all users discharged to unit from hospital’, and ‘isolation/quarantining of users/residents returning from hospital visits.’ The variables in our analysis for the three types of preventive measures are based on calculation of summative indexes.
Results
Perceived performance during the first 1.5 year with pandemic
The analysis reveals that the COVID-19 pandemic was perceived to have considerably more negative impact on the ability to promote a social and active life than mental and physical health (see ). We find that one third (33% in survey 1 and 32% in survey 2) of the managers agreed fully or partly that their unit had become less able to promote older people’s physical and mental health, while 50% and 49% agreed fully or partly with the statement concerning active and social life. Yet around one half of the managers reported that the ability to promote physical and mental health was not reduced, and around 40% disagreed that ability to enhance a social life was reduced. The managers’ reportings are consistent between the first and the second data collections. These results are also consistent across the time points for our surveys (2020 and 2021) at the country level. In all countries the scores on perceived performance are markedly lower concerning ability to promote active and social life than for ability to promote mental or physical health. We also find substantial differences between countries. For both performance indicators, managers in Finland reported lower performance than managers in the other countries (57% in the first and 51% in the second survey reported reduced health performance and 76% and 79% reported reduction in promotion of social life). At the other end, managers in Denmark reported changes in a negative direction to a lesser extent in both surveys (35% and 38% reported reduced health promotion, and 49% and 51% reported reduced social promotion
Multivariate analysis
A multiple regression analysis was performed with the purpose to examine the variations in performance evaluations further across the countries (). We also aimed to examine the relative impact of COVID-19 contagion experience in the unit compared to other factors. The analysis draws on a pooled dataset with data from both surveys. A control variable is included to test for possible differences between the time periods covered by the surveys.
Table 3. OLS regressions.
The analysis examines the perceived loss of ability to promote older people’s mental and physical health and an active and social life under the COVID-19 pandemic. We note that coefficients with a positive sign indicate higher average loss of ability, and a negative sign indicates lower average loss of ability.
The statistical software package IBM SPSS 27.0 was used for estimations. We report p-values at three levels (p ≤ .1, p ≤ .05, p ≤ .01). p-values ≤ .05 were considered statistically significant. We use a robust estimation to mitigate possible bias due to heteroscedasticity in the data across the countries.
We observe that experience of COVID-19 contagion in own unit impacts both promotion of social life and promotion of health significantly, and in a negative way (positive sign). At country level the effect of contagion is most pronounced in Denmark and Finland (). Managers in Denmark and Finland perceive that local outbreaks of COVID-19 are negatively related to the ability to promote social and active life and physical and mental health while no relationship is found for Norway and Sweden. It is also of interest to highlight that only managers in Sweden with responsibilities for relatively larger organizational units perceive that ability to promote social and active life and physical and mental health is less affected compared to those with responsibilities for relatively smaller organizational units. Finally, we note that there are sector differences in the ability to promote social and active life and physical and mental health in Denmark and Finland between home care units and nursing home units but no statistically significant differences in Norway and Sweden.
A predominant result, for both promotion of social life and health, is that managers of nursing home units tend to be more positive in their evaluation than managers of home care. This is a tendency that seems to hold at country level for all four countries. The same tendency can be observed among respondents that manage both nursing homes and home care.
Looking at prevention strategies, we observe two main patterns: Prevention strategies involving organisational changes (splitting staff in smaller teams, restricting use of substitutes in staff, reorganise care to reduce users’ social contact) tend to impact perceived promotion of social life in a positive manner. Furthermore, this is a tendency that seems to hold also to some degree at country level, in Sweden and Denmark (). Locking down (restricting entrance/visits, sectioning/closing of area, avoiding/closing buffets), on the other hand, seems to have a tangible effect on both promotion of health and a social life. A negative sign indicates that locking down in fact tends to decrease ability to promote both health and active and social life. Here too, the tendency is statistically significant only for Denmark and Sweden. The third prevention strategy, contagion control through testing of residents and isolation/quarantining of users returning from hospital visits, shows little effect and is inconclusive.
The estimation of marginal means with 95% confidence intervals (see ) indicates that Denmark scores significantly more positive (lowest mean values) than the other countries on both social promotion and health promotion, and that Finland scores significantly more negative (highest mean values) than the other three countries. The scores for Norway and Sweden are quite similar. The marginal means also indicate that the score on promoting social life in all four countries is significantly lower than promoting health.
Discussion and conclusion
The aim of this paper has been to explore the Nordic countries’ care for older people during the first 18 months of the COVID-19 pandemic, based on assessments by managers within municipal health care services for older people. Data is derived from two surveys carried out in Denmark, Finland, Norway, and Sweden in 2020 and 2021.
The study reveals a substantial variation in the managers’ assessment of the impact of the Corona pandemic on their unit’s ability to promote or enhance mental and physical health and an active and social life among older people, which both are principal goals within the “active and healthy ageing” strategy. Around one third of the managers agreed fully or partly that their ability to promote older people’s mental and physical health was reduced, while half of the managers agreed that their ability to promote an active and social life was reduced. On the other hand, a substantial number also disagreed with the statement presented. Around half of the managers disagreed that the ability to promote health was reduced, and around 40% disagreed that the promotion of social life was reduced. In all four countries promotion of social life was given a more negative score than promotion of health, indicating that the pandemic - despite the fatal consequences it had on mortality, and on physical and mental health - from the managers’ point of view has had adverse effects on the municipal health care services’ ability to promote an active and social life among older people. This is a consistent finding across both surveys and across all four countries. Nonetheless, we should not neglect that there is a likely association between these two main outcomes, where e.g. reduced opportunities for activity and social life could be expected also to have subsequent negative effects for mental and physical health (but also effects in the other direction are imaginable - since weak health condition also reduces possibilities for activity and social life to some extent). We do not have data to follow this up further in the two surveys, but the relationship between these two principal outcomes in health care for older people would deserve attention in future research.
When we look at individual countries, managers in Finland indicated the lowest evaluation on both social promotion and health promotion, while managers in Denmark were at the other end with the most positive evaluation out of the four countries. This ranking of the countries is not on par with the contagion levels and death rates registered in the four countries, where Sweden was by far the country with the highest level, followed by Denmark, while Finland together with Norway showed a relatively low level at the time of the data collection. It is not easy to see a straightforward way to interpret this pattern observed for Finland in particular. One should, however, be careful not to automatically interpret the low score in Finland in negative terms. We cannot rule out that there might be some methodological or cultural (or even combined) aspects involved in this type of data collection that could possibly explain some of the observations. It could for example be argued that the Finnish managers were more accurate (or “frank”) with their responses and that they therefore reflect a greater concern with and consciousness of the quality of care than managers in the other countries. Hopefully, such issues could be addressed in future studies comparing health care performance between Nordic countries.
The statistical analysis revealed that there are quite substantial country differences in performance that could not be explained by the available variables at unit level (managers) or municipal level. There may be several ways to interpret this. The unexplained inter country variance must be due to explanatory factors outside the set of items/variables that were used in the questionnaire. The questionnaire was built as a multi-purpose instrument where performance was only one of several dependent variables to be explored. In addition, performance turned up as a topic relatively late in the process of developing the questionnaire. This logic also affected the range of independent variables that would be included. Nonetheless, it is important to recognize the possibilities the included variables give and that the survey provides valuable pieces of new knowledge about intra- and inter-country differences (and some of their explanations) concerning the managers’ perception of their units’ performance concerning health care services for older people during the first 1–2 years of the COVID-19 pandemic.
One main result is that managers of nursing home units reported systematically more positively on ability to promote both health and social life than managers of home care. This was a tendency in all four countries, yet strongest in Denmark and Finland.
The effect of three prevention strategies (closing/locking down, testing residents and/or organisational change), was modest. The analysis concludes a positive impact of organisational change (reorganize staff and care, restrict use of substitutes) on promotion of social life. Interestingly, the analysis also indicates that locking down (areas, buffets etc) in fact tended to (weakly) decrease both promotion of social life and promotion of health.
A main implication of this study is that, in the pursuit for health care services to be better prepared and adapted for future pandemics, policies and measures that can stimulate health care services’ ability to promote social activity and prevent unwanted social isolation among older people with health care needs, would address a pronounced deficiency. The results indicate that the gains would be higher within home care than in nursing home units. The results also indicate that closing areas for users and restricting visits, is a less effective strategy than organisational changes.
One limitation of the study is that the questionnaire was translated from a Danish version to the three other Nordic languages and that, despite thorough back-translation, small differences in the meanings of concepts may exist. Different distribution methods between the countries (via municipal digital postal addresses in Finland, Norway, and Sweden, and directly to managers’ email addresses in Denmark) may to some degrees have affected nonresponse (rate and bias). In the regression models we observed a modest explained variance (adj. R2). However, since the main purpose of the regression analysis has been to explore the impact of specific factors and not to explain the total variance in performance evaluation, we do not evaluate this limitation as critical for the value of the analysis.
Acknowledgements
The authors wish to thank the health care managers in the four countries who participated in the study, and two anonoymous referees for constructive comments to an earlier version of the paper.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Myndigheten för vård och omsorg. Den nordiska äldreomsorgen. En jämförande kartläggning av struktur, organisation och innehåll. Vård och omsorgsanalys. Stockholm 2021.
- NOU 2021:6. The authorities’ handling of the COVID-19 pandemic. Report from the corona commission. Oslo: Norwegian Ministry of Local Government and Modernisation; 2021.
- Yarmol-Matusiak EA, Cipriano LE, Stranges S. A comparison of COVID-19 epidemiological indicators in Sweden, Norway, Denmark, and Finland. Scand J Public Health. 2021;49(1):69–78. doi: 10.1177/1403494820980264.
- Diderichsen F. How did Sweden fail the pandemic? Int J Health Serv. 2021;51(4):417–422. doi: 10.1177/0020731421994848.
- WHO. Active ageing: a policy framework. Geneva: WHO; 2002.
- Bodin E, Kumlin L, Tengqvist A. Att åldras i Norden: en kartläggning av strategier och initiativ för aktivt och hälsosamt åldrande i de nordiska länderna. 2020.
- Wolmesjö M, Solli R. Räkna med framtida arbetskraftsbehov i välfärden. Äldre i Centrum. 2019;2019(4):74–77.
- Wolmesjö M, Solli R. Framtidens välfärd – hållbar styrning, organisering och ledning. Lund: Studentlitteratur AB; 2021.
- Angel JL, Mudrazija S. Local government efforts to mitigate the novel coronavirus pandemic among older adults. J Aging Soc Policy. 2020;32(4-5):439–449. 2020/07/03 doi: 10.1080/08959420.2020.1771240.
- Buffel T, Phillipson C. Urban ageing: new agendas for geographical gerontology. In: Skinner MW, Andrews GJ, Cutchin MP, editors. Geographical gerontology: perspectives, concepts, approaches. London: Taylor and Francis; 2018.
- Skinner MW. Ageing, place and voluntarism: towards a geographical perspective on third sector organisations and volunteers in ageing communities. Volunt Sect Rev. 2014;5(2):161–179. doi: 10.1332/204080514X14020630062723.
- Skinner MW, Andrews GJ, Cutchin MP, editors. Geographical gerontology: perspectives, concepts, approaches. London: Taylor and Francis; 2018.
- Skinner MW, Cloutier D, Andrews GJ. Geographies of ageing: progress and possibilities after two decades of change. Prog Hum Geogr. 2015;39(6):776–799. doi: 10.1177/0309132514558444.
- Skinner MW, Hanlon N. Ageing resource communities: new frontiers of rural population change, community development and voluntarism. In: Routledge studies in human geography. Oxon: Taylor and Francis; 2016.
- Lui C-W, Everingham J-A, Warburton J, et al. What makes a community age-friendly: a review of international literature. Australas J Ageing. 2009;28(3):116–121. doi: 10.1111/j.1741-6612.2009.00355.x.
- Szebehely M, Meagher G. Four Nordic countries – four responses to the international trend of marketisation. Stockholm Studies in Social Work. 2013. p. 241.
- Vabø M, Zechner M, Stranz A, et al. Is nordic elder care facing a (new) collaborative turn? Soc Policy Adm. 2022;56(4):549–562. doi: 10.1111/spol.12805.
- Daatland SO, Høyland K, Otnes B. Scandinavian contrasts and Norwegian variations in special housing for older people. J Hous Elderly. 2015;29(1–2):180–196. doi: 10.1080/02763893.2015.989778.
- SOU 2020:80. Äldreomsorgen under pandemin. Stockholm: Socialdepartementet; 2020.
- Authority DH. Home nursing in the Nordic countries. Danish Health Authority; 2021. p. 67.
- Rauhala, A., Fagerström, L. M., Lindholst, A. C., Sinervo, T. S., Bertelsen, T. M., Bliksvær, T., Lunde, B. V., Solli, R., Wolmesjö, M. G., & Hansen, M. B. (2022). Which factors are associated with COVID-19 infection incidence in care services for older people in Nordic countries? A cross-sectional survey. Scandinavian Journal of Public Health, 50(6), 787–794 .
- Dahlberg L. Loneliness during the COVID-19 pandemic. Aging Ment Health. 2021;25(7):1161–1164. doi: 10.1080/13607863.2021.1875195.
- Landry MD, Van den Bergh G, Hjelle KM, et al. Betrayal of trust? The impact of the COVID-19 global pandemic on older persons. J Appl Gerontol. 2020;39(7):687–689. Jul doi: 10.1177/0733464820924131.
- Vahia IV. COVID-19, aging, and mental health: lessons from the first six months. Am J Geriatr Psychiatry. 2020;28(7):691–694. doi: 10.1016/j.jagp.2020.05.029.
- Vislapuu M, Angeles RC, Berge LI, et al. The consequences of COVID-19 lockdown for formal and informal resource utilization among home-dwelling people with dementia: results from the prospective PAN.DEM study. BMC Health Serv Res. 2021;21(1):1003. doi: 10.1186/s12913-021-07041-8.
- Fyhn K, Lønning MN. Sånne små ting som å holde hender, det gjør så mye med hele deg: eldre menneskers hverdag under koronapandemien. Oslo: Norges røde kors; 2021.
- Bonsaksen T, Schoultz M, Thygesen H, et al. Loneliness and its associated factors nine months after the COVID-19 outbreak: a cross-national study. Int J Environ Res Public Health. 2021;18(6):2841. doi: 10.3390/ijerph18062841.
- Hansen, M. B., Bertelsen, T. M., Lindholst, C., Bliksvær, T., Lunde, B. V., Solli, R., & Wolmesjö, M. Minimizing COVID-19 in Nordic Eldercare. Challenges and Solutions. Institut for Politik og Samfund, AalborgUniversitet; 2020..
- Willi Y, Nischik G, Braunschweiger D, et al. Responding to the COVID-19 crisis: transformative governance in Switzerland. Tijd Voor Econ Soc Geog. 2020;111(3):302–317. doi: 10.1111/tesg.12439.
- Bertelsen TM, Lindholst C, Hansen MB. Manager characteristics and early innovation adoption during crises: the case of COVID-19 preventive measures in Danish Eldercare, Public Management Review, 2022; 25:9, 1755-1775 .
- Poulsen VR, Juul Nilsson C, Hansen MB, et al. How risk management during COVID-19 influences eldercare personnel’s perceptions of their work environment. J Occup Environ Med. 2022;64(11):957–963. doi: 10.1097/JOM.0000000000002609.
- Bertelsen TM, Lindholst C, Jørgensen MS, et al. Forebyggelse og håndtering af COVID-19 i nordisk kommunal ældrepleje- Afrapportering fra en surveyundersøgelse til ledere i dansk ældrepleje. Aalborg Universitet, Department of Politics and Society/Institut for Politik og Samfund; 2021.
- Armstrong JS, Overton TS. Estimating nonresponse bias in mail surveys. J Market Res. 1977;14(3):396–402. doi: 10.1177/002224377701400320.
- Raykov T, Marcoulides GA. An introduction to applied multivariate analysis. Hoboken: Taylor and Francis; 2012.
- Tabachnick BG, Fidell LS. Using multivariate statistics. Boston: Allyn and Bacon; 2001.
Appendix
Table A1. Country-level OLS regression.
Table A2. Descriptive statistics.
Table A3. Characteristics of respondents in sample, by year and country.