
Abstract
Modern society is faced with increasing incidence of mental and behavioural disorders. The objective of this study was to evaluate whether visits to boreal forests can be utilised for rehabilitation from exhaustion disorder (ED). This randomised controlled trial comprised of a forest rehabilitation group (n = 35) and a waiting list group (control group) (n = 43) with subsequent cognitive behavioural rehabilitation (CBR) for all participants in both groups. The recovery from ED was compared between the forest rehabilitation and the control group at baseline, after the forest rehabilitation (3 months), and at the end of the CBR (1 year). Both groups had enhanced recovery from ED after the 3-month intervention period and at the end of the CBR (1 year), and there were no significant differences between the groups in terms of psychological health measures. Mental state, attention capacity and preferences for different forest environments were studied during the forest visits. Mental state was improved, but it showed some seasonal differences. A significant effect on attention capacity was found for single forest visits, but there was no effect found for the rehabilitation period as a whole. The most popular forest environments contained easily accessible, open and bright settings with visible water and/or shelter. Forest rehabilitation did not enhance the recovery from ED compared to the control group, but the participants’ well-being was improved after single forest visits.
Introduction
Mental and behavioural disorders are an increasing problem in many industrial countries (Murray et al. Citation2012), and this presents a challenge to the health care system to find new preventive and rehabilitative measures in the fight against these disorders. “Burnout” is one such mental disorder and is related to chronic stress. In Sweden, the term “burnout” was replaced by “exhaustion disorder” (ED) (ICD-10, F43.8A) in 2003 by the Swedish National Board of Health (Socialstyrelsen Citation2003; Glise et al. Citation2010). The diagnosis describes mental and physical exhaustion caused by identifiable stressors at work and/or in private life. “Reaction to severe stress, and adjustment disorders” (ICD-10, F43) was the most prevalent diagnosis for new sick-leave cases related to psychological diseases in 2012, according to statistics from the Swedish Social Insurance Agency (Försäkringskassan Citation2013). The same authority also concluded that the morbidity of psychological diseases in Sweden is most frequent among women.
People suffering from ED experience problems with cognitive, somatic and psychosocial functioning. These deficiencies can be manifested as impaired memory and attention, mental and physical fatigue, unstable emotional states and disturbed sleep patterns. Our knowledge of effective rehabilitative methods for people affected by burnout or ED is inadequate even though cognitive behavioural therapy has shown some documented positive effects on emotional exhaustion (SOU Citation2011; Korczak et al. Citation2012). The Swedish National Council for Rehabilitation recommends a multimodal rehabilitation for people suffering from ED including conversational therapy, vocational rehabilitation, stress reduction and behavioural change related to balancing between activity and recovery (SOU Citation2011). Even though there is a lack of evidence regarding the efficacy of multimodal rehabilitation, the council points out that there is a broad clinical consensus about the use of multimodal rehabilitation. Stenlund et al. (Citation2012) showed some positive long-term effects on the recovery of patients from ED and reduction in depression medication in a randomised controlled trial of cognitive behavioural rehabilitation (CBR) in combination with Qigong (Qigong has its roots in Chinese medicine and philosophy and is a method for relaxation and recuperation), but residual symptoms were frequently experienced. A longitudinal mixed method study by Pálsdóttir et al. (Citation2014) and a retrospective cohort study by Währborg et al. (Citation2014) showed some beneficial effects from a multimodal nature-based rehabilitation programme in terms of returning to work and reducing health care consumption for patients suffering from severe stress and/or depression. Due to the lack of randomised controlled studies concerning rehabilitation from ED and the relief of residual symptoms, there is a great need to produce further evidence for effective strategies to help those affected by ED.
Nature produces positive emotional and physiological responses in humans. Some researchers claim that our preferences for natural environments are innate and connected to our basic needs for survival (Appleton Citation1975; Orians Citation1980; Wilson Citation1984). The plausible benefits of nature when suffering from psychiatric disorders have been discussed by Harold Searles (Citation1960), while Roger Ulrich (Citation1984) and Rachel and Steven Kaplan (Citation1989) studied the beneficial effects of nature on human emotions, attention and physiology. Nature has been shown to promote well-being through wilderness outings, images of nature shown in the laboratory, views from windows and virtual reality experiments (Kaplan & Talbot Citation1983; Ulrich Citation1984; Chang et al. Citation2008; Annerstedt et al. Citation2013). According to Korpela (Citation2003), adults suffering from negative mood states prefer the serenity of natural places for emotional regulation, and Grahn (Citation2005) argued that mentally fragile people feel the need to be in environments that, according to Attention Restoration Theory (ART; Kaplan & Kaplan Citation1989), provide a mental refuge such as those provided by nature.
Our earlier research (Sonntag-Öström et al. Citation2011, Citation2014) has shown that visits to forest environments lead to beneficial physiological reactions and subjective emotional wellness for people suffering from ED. These findings and other results about the positive effects of natural environments on human well-being (Bowler et al. Citation2010; Annerstedt & Währborg Citation2011) encouraged us to test whether rehabilitation that included visits to boreal forest environments could facilitate and support recovery from ED. Because forests in Sweden are free to access for the public, and often situated geographically close to residential areas, their potential to provide viable environments for rehabilitation and prevention of stress-related disorders is substantial.
The primary study objective was to evaluate whether a boreal forest can be used for rehabilitation from ED based on the hypothesis that the boreal forest itself has a restorative effect. We hypothesise that participation in the forest intervention will enhance recovery from ED. Moreover, since persons with ED often display unstable emotions and forest visits elicit positive emotions, we assume that the forest intervention will contribute to enhanced mental states in ED patients. Also, since attention capacity is assumed to be increased by the positive effects of the forest, it too is assumed to be enhanced during visits to the forest. Taken together, these improvements in both emotion and attention are thought to lead to easier assimilation to the subsequent CBR. The secondary objective is to study which type of boreal forest areas are preferred by the participants with possible future applications for forest management.
Materials and methods
Study population and study design
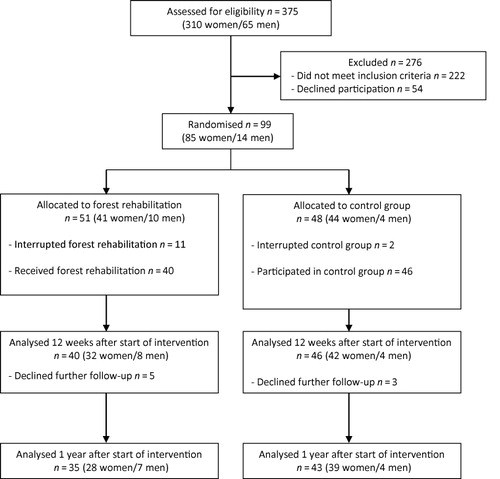
A randomised controlled study, forest for rest (ForRest), was carried out as a collaboration between the Swedish University of Agricultural Sciences in Umeå, Umeå University, and the Stress Rehabilitation Clinic (SRC) at the University Hospital of Umeå, Sweden. A total of 375 people (310 women and 65 men) were screened for participation between January 2007 and December 2010 (). The first 356 individuals (291 women and 65 men) were found through screening all patients referred to the SRC up to January 2009. Thereafter, new rules for sick-leave benefits and a shortened waiting list at the SRC made it very difficult for patients referred to the SRC to allocate time for participation. Therefore, the remaining 19 participants (19 women and 0 men) were found through the Swedish Social Insurance Agency in Umeå. Participants in this latter group received compensation of SEK 100 per visit to the forest.
All participants were assessed by a physician and a psychologist at the SRC to confirm a diagnosis of ED (Socialstyrelsen Citation2003; Glise et al. Citation2010), which was the first inclusion criterion. Other inclusion criteria were being in the age range of 24–60 years and obtaining a score of ≥4.0 on the Shirom–Melamed Burnout Questionnaire (SMBQ; Melamed et al. Citation1999). The exclusion criteria were other diseases or disorders that could result in future sick leave due to fatigue and/or stress-related symptoms (for example, chronic infections, chronic fatigue syndrome and endocrine disorders), other diseases or conditions that could interfere with active participation, the need for individual therapy or an urgent need for multimodal rehabilitation (CBR), known alcohol or drug abuse, and participation in other intervention studies. All participants received verbal and written information regarding the study and were included if they met the inclusion criteria and provided written informed consent.
One hundred and fifty-three people (134 women, 19 men) met the criteria for participation and were invited to participate (). Fifty-four of them declined (49 women, 5 men) due to working conditions or personal reasons. Persons who declined did not differ significantly in age, sex or SMBQ scores compared to those who participated (data not shown). The final study population consisted of 99 participants (85 women, 14 men) with a mean age of 44.6 (SD 8.6) years.
Randomisation was carried out when enough participants (maximum of 16 participants) were recruited to enable randomisation into two groups (one for the forest intervention and one for the control group). Randomisation occurred on eight different occasions and was always carried out after baseline assessments and approximately 2 weeks before the start of a new intervention period. The research nurse prepared a list of all the volunteers and put an equal number of lots for the forest intervention group and the control group into an opaque envelope. The allocation was carried out by an independent person who drew lots from the envelope and used that information (A = forest, B = control) to allocate consecutive participants on the list into groups.
After the study intervention, which lasted for 12 weeks, all of the participants received a multimodal CBR programme at the SRC. This consisted of an extensive CBR course over 24 weeks combined with advice on physical activity and vocational rehabilitation. The entire study period, including the intervention and CBR, lasted for 1 year. This study was approved by The Research Ethics Committee of Umeå University (Dnr 07-016M).
Forest intervention
A maximum of eight participants in each group visited the forest environments during either spring or autumn. During the first rehabilitation week, the participants were introduced to the forest environments. The forest visits then took place twice a week for 11 weeks (22 visits in total). The choices of the length of time and the number of visits were based on the following: (1) the need for daylight during the forest visits, (2) empirical knowledge from the SRC that recovery from ED usually takes several months, and earlier research showing the need for weeks/months of either cognitive or physical training to obtain positive effects on the body and the mind (Dahlin et al. Citation2008; Hillman et al. Citation2008), (3) snow limiting accessibility to the forest during the winter and (4) the difficulty that people had in participating during the summertime because of their summer vacations. Winter overalls, insulated rubber boots, and a raincoat were available to all participants to enable participation even in bad weather. Each visit to the forest lasted for four hours in total, two of which were spent alone in a preferred forest setting.
The participants were transported back and forth to the forest by two leaders. The transportation by car lasted for approximately 15 minutes, one way. The two leaders (one with a medical background and one with a forestry background) were requested not to initiate any therapeutic discussions or encourage social interaction. The group entered the forest at 10:00 am.
Each session started with the sharing of a simple breakfast and the lighting of a fire beside a shelter in the forest. Thereafter, the participants performed some short and simple relaxation exercises (Baer Citation2003; Brown et al. Citation2007) to provide them with a tool to control possible anxiety attacks during their visit to the forest. These exercises lasted for approximately 5–10 minutes and consisted of focusing on carrying out two activities in sequence (e.g. breathing and focusing on an object). On every visit to the forest, each participant chose a forest setting according to their own preference. The choice of preferred forest setting was recorded for all forest visits.
The two hours of solitude in the forest setting started at 11:00 am. The participants were instructed to spend the time in solitude in peace and quietness, and only be physically active if feeling cold. All participants had access to a lightweight sleeping mat in order to be able to sit or lie down in the forest. After returning from the forest, a simple lunch was served by the fire and the group left at 2:00 pm. The same schedule was followed on every visit to the forest.
Control condition
Participants in the control group were on a waiting list during the 12-week intervention period, which implied visiting the physician at the SRC when needed for renewals and changes to prescriptions and sick-leave certificates until starting the multimodal CBR at the SRC.
Outcome measures
Long-term psychological health measures
The long-term psychological health measures were studied using the SMBQ, the Perceived Stress Questionnaire (PSQ), the Checklist Individual Strength questionnaire (CIS), the Self-Concept Questionnaire (SCQ) and The Hospital Anxiety and Depression Scale (HAD-S). These were filled out by the participants before randomisation, at 12 weeks after the start of the intervention, and at 1 year after the start of the intervention. The questionnaires issued at 12 weeks and at the 1-year follow-up also contained questions about any complementary treatments received outside the SRC.
The SMBQ assesses the level of burnout. The questionnaire is composed of 22 items, including subscales relating to emotional and physical exhaustion, listlessness, tension and cognitive weariness. Each item is rated on a 7-point scale from 1 (almost never) to 7 (almost always). The mean of all items represents the overall index, and higher scores indicate a worse condition (Melamed et al. Citation1999).
The PSQ assesses the level of perceived generalised stress. The questionnaire is composed of 30 items related to conditions experienced during the previous week that are rated on a 4-point scale from 1 (almost never) to 4 (almost always). An index is calculated as (total score-30)/90. Higher scores indicate a worse condition (Levenstein et al. Citation1993).
The CIS questionnaire assesses the level of fatigue. It is composed of 20 items measuring (1) the subjective experience of fatigue, (2) concentration, (3) motivation and (4) level of physical activity. Each item is related to conditions during a previous 2-week period and is rated on a 7-point scale from 1 (Yes, that is true) to 7 (No, that is not true). The composite total score of the CIS represents the overall index and higher scores indicate a worse condition (Beurskens et al. Citation2000).
The SCQ assesses the level of self-esteem. The questionnaire is composed of 30 items measuring components of: significance, worthiness, competence, resilience, determination, appearance, social acceptability, control over personal destiny and the value of existence. Each item is rated on an 8-point scale from 0 (completely disagree) to 7 (completely agree). The composite total score on the SCQ is calculated, and higher scores indicate higher self-esteem (Robson Citation1989).
The HAD-S is divided into two subscales, anxiety and depression, which consist of seven items each. Both subscales are scored on a 4-point scale (0–3) with a composite total score of 0–21 points (Zigmond & Snait Citation1983). Higher scores indicate a worse condition.
Sick-leave data
Sick-leave data for the participants were collected from the patients’ records at the SRC at baseline and at 1 year. All patients saw a physician at the SRC, who was responsible for issuing sick-leave certificates. In Sweden sickness benefits are graded by quarters based on the ability to work, i.e. 25%, 50%, 75% or 100% sick leave.
Mental state and attention capacity in the forest intervention group
Mental state was evaluated on all forest visits using a questionnaire before and after each visit to the forest settings. The questionnaire asked about the participants’ perceived tenseness (tense/relaxed), fatigue (exhausted/alert), mood (sad/happy), irritability (irritated/harmonious), restlessness (restless/peaceful) and clear-headedness (mentally distracted/clear-headed) on a 10-point scale. Higher scores indicated a better mental state. The questionnaire was based on validated instruments such as the Profile of Mood States and the Zuckerman Inventory of Personal Reactions (McNair et al. Citation1971; Zuckerman Citation1977), but in a simplified form to minimise the participants’ mental strain (Sonntag-Öström et al. Citation2011).
The participants’ attention capacity was tested using the Necker Cube Pattern Control task (NCPC) and was carried out three times during the rehabilitation period – at baseline, at 6 weeks and at 12 weeks – before and after a forest visit in solitude. The NCPC task used a three-dimensional picture of a cube that can be seen from two different perspectives. The participant was instructed to look at the cube during two separate 30-second periods with a 1-minute rest in between. During the first 30-second period, the participant was instructed to look at the picture and tap on their thigh whenever the perspective of the cube changed. During the second 30-second period, the participant was instructed to focus on one perspective and try to hold that perspective. If and when the perspective changed, the participant was asked to indicate the change by tapping on their thigh. The number of reversals should be reduced when the patient has been instructed to focus and to try to stop them from happening (Liebert & Burk Citation1985). Each test was carried out individually.
Locality
The study was set up in the forest at Bäcksjön (coordinate system WGS 84: 63°58′ N, 20°21′ E) about 17 km outside the city of Umeå, which is situated in northern Sweden in the boreal zone (Ahti et al. Citation1968). The study was carried out during autumn (September–December) and spring (March–June).
The predominant colour in the forest was green at the beginning of autumn, but reductions in the temperature and day length over the study period resulted in the deciduous trees displaying their autumn colours. Towards the end of the autumn, snow periodically covered the landscape and the deciduous trees lost their leaves.
At the beginning of spring, the forest was covered with snow and the predominant colour was white. As the day lengthened and the temperature rose, the snow melted, the vegetation sprouted and the predominant colour became green. describes the temperature and humidity at the site along with the number of daylight hours and the amount of brightness.
Table 1. Climate data during the 3-month forest rehabilitation in spring (March–June) and autumn (September–December).
Eight different forest settings were available for visits, and these varied in size from 5000 m2 to 50,000 m2.
Forest by the lake – an open forest close to a lakeside dominated by Scots pine (Pinus sylvestris L.) with sparsely distributed Norway spruce (Picea abies (L.) H. Karst.), downy birch (Betula pubescens Ehrh.) and aspen (Populus tremula L.). The ground vegetation consisted mainly of shrubs e.g. bilberry (Vaccinium myrtillus L.), cowberry (Vaccinium vitis-idaea L.) and crowberry (Empetrum hermaphroditum Hagerup). The view from the forest setting was dominated by the broken shoreline with small forested headlands and the lake (approximately 3 × 1 km) with two forested islands. Managed pine and spruce forests without houses or settlements could be seen in the distance (). The walking distance from the shelter to this forest setting was approximately 1 km.

Rock outcrop – a sloping non-productive open area with bare bedrock and old, but small, Scots pine trees. The ground vegetation was dominated by various lichens e.g. reindeer lichens (Cladina spp.) and scattered mosses. Cowberry and crowberry were sparsely distributed in crevices and lower parts of the bedrock. The Rock outcrop was surrounded by a young pine forest in the upper part and an open mire (further described below) in the lower part (). The walking distance from the shelter to this forest setting was approximately 200 metres.

Pine forest – an open and rather light and stony 65-year-old, even-aged Scots pine stand with ground vegetation dominated by cowberry, crowberry, bilberry, some heather (Calluna vulgaris (L.) Hull), lichens and mosses such as Pleurozium schreberi (Brid.) Mitt. and Hylocomium splendens (Hedw.) B.S.G. (). The walking distance from the shelter to this forest setting was approximately 50 metres.

Spruce forest – a rather shady and dark closed forest dominated by 85-year-old Norway spruce and scattered mature Scots pine. The ground vegetation consisted mainly of bilberry and mosses (). The walking distance from the shelter to this forest setting was approximately 200 metres.

Mixed forest – an uneven aged forest with patchy dense groves and small glades. The tree layer consisted of 65-year-old Scots pine and 125-year-old Norway spruce and birch. The ground vegetation primarily consisted of shrubs as bilberry, cowberry, heather and various mosses (). The walking distance from the shelter to this forest setting was approximately 50 metres.

Forest with a small stream – a gentle slope with dark, mixed forest along the course of a small stream approximately 0.5 m wide. The forest was dominated by 65- to 75-year-old Scots pine with scattered Norway spruce and birch with mosses, peat mosses (Sphagnum spp.), bilberry, and crowberry in the field and bottom layers (). The walking distance from the shelter to this forest setting was approximately 1 km.

Mire surrounded by spruce forest – a fairly open mire dominated by peat mosses (Sphagnum spp.) and sedge (Carex spp.) in the ground and field layer and with scattered patches dominated by heather (Calluna vulgaris) and small, slow-growing Scots pine (). The walking distance from the shelter to this forest setting was approximately 350 metres.

Mire surrounded by spruce forest and rock outcrop – an open mire dominated by heather and sedges (Cyperaceae) such as cotton grass (Eriophorum spp.) and sedge (no photograph included). The walking distance from the shelter to this forest setting was approximately 250 metres.
Statistical methods
The Statistical Package for the Social Sciences (SPSS) version 20.0 and 21.0 (SPSS Inc., Chicago, IL, USA) and SAS version 9.3 (SAS Institute Inc., Cary, NC, USA) were used for the statistical analyses.
A power analysis, based on prior knowledge of the variation of the SMBQ, was carried out before the study. It was estimated that approximately 50 patients were needed in each group to give an 80% power to detect a statistically significant difference (p < 0.05) between the two groups, assuming a mean SMBQ difference of 0.4 and a standard deviation of 0.7. With an expected dropout rate of 25%, 130 randomised patients would be needed in total. However, we could not reach this goal of 130 participants because of difficulties the patients had in allocating time for participation due to new rules concerning sick-leave benefits and waiting list criteria.
The SPSS statistical analyses were conducted as per protocol analyses and included participants who completed the 1-year rehabilitation. This resulted in 35 participants in the forest intervention group and 43 participants in the control group. To evaluate changes over time in the long-term psychological variables, repeated-measures analysis of variance was used with time as a within-subject variable and group as a between-subject variable. When the sphericity assumption was not met, the Greenhouse–Geisser correction was used.
Independent t-tests and chi-square analyses were carried out on the differences between the two groups at baseline and also for sick-leave data at 1 year. When expected frequencies were five or less, Fisher's exact test was used.
To evaluate changes over time in mental state and the NCPC task, a non-parametric design for repeated measures was used. Single exposure (before and after the visit to the forest) and progress during the rehabilitation period were analysed with time as a within-subject factor, and season as a between-subject factor. The analyses were carried out using the F1_LD_F2 SAS macro (Brunner et al. Citation2002) in SAS version 9.3 (SAS Institute Inc., Cary, NC). The level of significance was set at p < 0.05 for all tests.
Single missing responses in the SMBQ, CIS, SCQ, PSQ and HAD-S measures were replaced with the corresponding median value for the whole group. This procedure was applied to 0.25–0.64% of items. Participants who had more than three missing responses on the SMBQ, CIS, SCQ and PSQ scales, or more than one missing response on the HAD-S, were excluded from the analysis.
Results
A total of 99 participants volunteered to participate in the study and were randomised. Fifty-one participants were randomised to the forest intervention (41 women/10 men) and 48 to the control group (44 women/4 men). There were no significant differences in baseline characteristics between the participants randomised to the forest intervention and those randomised to the control group regarding sex, age, working status, education, family situation or time since the onset of significant ED ().
Table 2. Baseline characteristics of patients in the forest rehabilitation group and the control group.
The forest intervention was completed by 40 participants and the control condition was completed by 46 participants. After the initial 12-week study period, all participants were offered the multimodal rehabilitation including the CBR course. Eighty-two participants (83%) completed the entire 1-year rehabilitation programme, including 38 participants (75%) in the forest intervention group and 44 (92%) in the control group. However, four participants did not return their questionnaires as required and were excluded from the analysis. A flow chart describing participation in the study is shown in .
Dropouts
The final total dropout rate at the 1-year follow-up was 21%. Three participants in the forest intervention group and one participant in the control group dropped out almost immediately after randomisation and before the actual start of the intervention. Seventeen participants (16 women/1 man) with a mean age of 41.7 years discontinued participation during the intervention, including 13 in the intervention group and 4 in the control group. There were no significant differences in age, time since the onset of significant ED or SMBQ score at baseline for all the dropouts compared to participants who completed the study per protocol (data not shown).
Compliance to randomised condition and complementary treatments
On average, the intervention group took part in 17 (range 9–22) forest visits. In the forest intervention group, 5% of the participants reported the use of complementary physical treatment during the intervention. In the control group, 40% reported complementary physical or mental treatment and/or individual or group conversational therapy during the 12 weeks on the waiting list.
Per protocol analysis
Long-term psychological health measures
There were significant improvements in the long-term psychological health measures estimated by SMBQ, PSQ, CIS, SCQ and the HAD-S in both the forest intervention group and the control group after the 3-month intervention period and at the end of the CBR (1 year) (). However, no significant differences were observed between the two groups, and a separate analysis with adjustments made for complementary treatment yielded the same results. Interaction effects were tested but yielded non-significant results.
Table 3. Long-term psychological health variables for patients in the per protocol analyses.
Subgroup analyses were carried out to study the effects of time since the onset of significant ED and the actual number of completed forest visits. There were no significant differences between participants with a short time since the onset of significant ED (≤365 days; n = 14), compared to a long time (>365 days; n = 20). Neither were there any significant effects of the forest intervention for participants with high compliance (≥16 visits; n = 26) compared to those with low compliance (<16 visits; n = 9) in forest visits (data not shown).
Sick-leave data
There was no difference in the level of sick-leave between the two groups after 1 year ().
Table 4. Per protocol analysis of level of sick leave at baseline and at 1 year.
Preferred forest settings
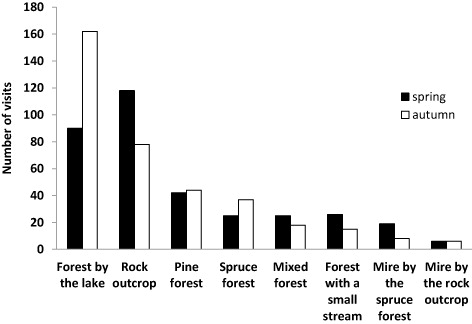
The participants’ choices of forest settings in each season during the entire forest intervention period are illustrated in . Overall, the most and least preferred forest settings were Forest by the lake (238 visits) and Mire by the rock outcrop (12 visits), respectively. Forest by the lake was most preferred during the autumn (162 visits), while Rock outcrop (103 visits) was most preferred during the spring. Mire by the rock outcrop had the least visits both during the autumn and the spring (6/6 visits each). shows the seasonal distribution of forest visits to the four most popular forest settings. The visits were evenly distributed during the autumn, but irregularly distributed during the spring with most visits to Forest by the lake towards the middle and the end of the season.

Mental state and attention capacity in the forest intervention group
Mean ratings of mental state before and after each forest visit, progress during the forest rehabilitation period and seasonal variations are presented in . The results from the non-parametric repeated-measures analysis are presented in . All mental state variables showed significant improvement for single exposure (E) after the two hours of solitude in the forest. The progress during the rehabilitation period (P) showed significant improvement towards the end of the rehabilitation period compared to the beginning in all mental state variables except for the irritated/harmonious scale. Two-way interaction effects were found between season (S) and single exposure (E) with decreasing values towards the end of the autumn period compared to the end of the spring period for the mental state scales tense/relaxed, irritated/harmonious and restless/peaceful. Variations for single exposure (E) can be seen in between spring and autumn. There were no main effects for season (S). Neither was there a three-way interaction effect for season, progress during the rehabilitation period and single exposure (S*P*E) (data not shown in ).
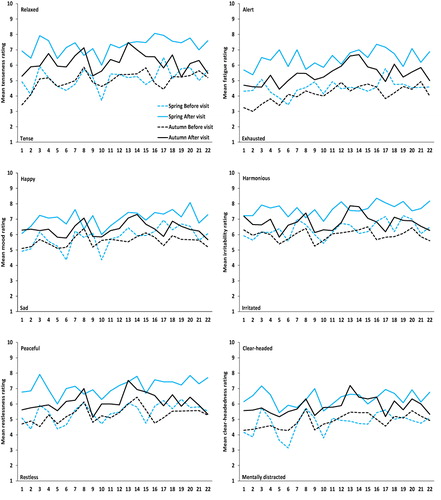
Table 5. Results of non-parametric testing of treatment effects on the mental state of patients in the forest intervention group taking into account effects of season (S), progress during the rehabilitation period (P) and a single exposure (E).
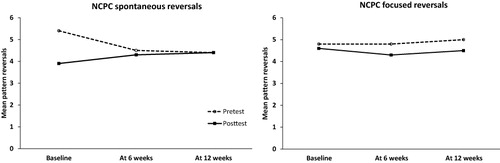
The results from the non-parametric repeated-measures analysis for the attention capacity test at baseline, at 6 weeks and at 12 weeks are shown in . The observation of a significant main effect for single exposure (E) in both spontaneous and focused reversals indicated improved attention capacity with fewer spontaneous and focused reversals after two hours of solitude in the forest. For spontaneous reversals, a two-way interaction effect was found between the rehabilitation period (P) and the single exposure (E) due to improved attention capacity with fewer spontaneous reversals after two hours of solitude in the forest at baseline but not at later occasions (see and ).
Table 6. Results of non-parametric repeated-measure analyses on attention capacity in the forest intervention group using the Necker Cube Pattern Control (NCPC) task. The results take into account the effects of season (S), progress during the rehabilitation period (P), and a single exposure (E).
Discussion
We carried out this study to determine if the boreal forest itself can help patients suffering from ED improve their mental state and attention capacity – and thus speed their recovery from ED – as well as to identify the types of environments that were preferred by the participants. There were also significant improvements in the long-term psychological health measures – which are considered to be intertwined with the recovery from ED – for the forest intervention group after 12 weeks and after 1 year of rehabilitation. However, the same improvement in psychological health was found in the control group, and there were no significant differences between the two groups. The results for the forest rehabilitation group show that forest visits appeared to produce a more favourable mental state, and there were also some positive effects on attention capacity. Open and bright forest environments containing shelter and visible water were the most popular in the forest intervention group.
That there were no significant differences in long-term psychological health measures between the groups might have been due to the fact that the participants in the control group utilised complementary treatment to a greater extent than those in the intervention group. We tried to control for the uneven distribution of complementary treatments in our study, but the results were unchanged and no significant differences in psychological health variables were seen between the two groups. Participants in the control group might also have been visiting forest or other nature environments on their own. We were not able to control for that. This is a common problem in many RCT studies with behavioural interventions. However, the participants in this study had a long history of ED, and we do not consider it probable that they managed to start visiting forest environments on a regular basis on their own.
The follow-up visits by the physician at the SRC for both groups might also have helped the recovery process, especially for the participants in the control group who lacked the opportunity to be seen, confirmed and taken care of in the same way as the participants in the forest intervention. The anticipation of the upcoming CBR might also have triggered the process of recovery in both groups. Previous research on patients with complex conditions leading to prolonged sick leave has shown that multimodal rehabilitation programmes are usually required in order to recover and regain the ability to work (SOU Citation2011). All patients in the ForRest study received multimodal CBR course after the initial 12-week study period, which was probably the most important intervention to help the patients to recover and regain the ability to work after 1 year. The hypothesis that a forest intervention would make the participants more prepared for the oncoming multimodal CBR, and would exert positive effects on the final recovery, could not be confirmed in this study.
Participants in the forest intervention group did show positive effects on mental state following single forest visits, which is in agreement with our earlier studies (Sonntag-Öström et al. Citation2011, Citation2014). We also observed a gradually improving mental state during the ongoing forest rehabilitation for all items except the irritated/harmonious scale. An interesting observation was the difference in the progress of mental state for individuals in the forest intervention between the spring and the autumn seasons. The overall evaluations of mental state during the spring showed a greater before and after effect on well-being compared with the evaluations during the autumn. The estimations of being relaxed, harmonious and peaceful after a visit to the forest were stronger towards the end of the spring compared to the autumn. There could be several reasons for this phenomenon, but the most probable are the reduced length of daylight, increasing coldness and other seasonal changes in the boreal forest as winter approaches. Daylight and weather are known to influence mental well-being (Molin et al. Citation1996; Keller et al. Citation2005; Denissen et al. Citation2008; Kämpfer & Mutz Citation2013), and the differences in light conditions between autumn and spring are noticeable at 65°00′ N. Even though the participants spent time in the forest during the brightest hours of the day, the differences in intensity of daylight during the seasons might have affected the participants. The start of decreasing estimations of good mental state occurred on approximately the 14th visit to the forest during the autumn. The end of Daylight Saving time for the year occurs around the end of October or the beginning of November, and this means it is dusk one hour earlier in the afternoon. This might have contributed to the reduced scores evaluated for well-being. There is also a great difference in the aesthetic experience and the stimulation of senses in the forest towards the end of autumn compared to spring. The forest is most often silent, clammy and colourless at the end of the autumn, while late spring offers a forest full of life and activity. The increasing greenness in shrubs during spring might also have contributed to a landscape with greater access of places for refuge.
The Forest by the lake had the highest overall rate of visits and was the most popular site during the autumn while the Rock outcrop was most popular during the spring. Both areas offered a good view over the surroundings and could be perceived as open and bright areas. This finding was not unexpected because environmental affordances such as prospect and refuge (Appleton Citation1975), as well as openness and light are important basic features for experiencing safety and recovery (Herzog et al. Citation2003; Stamps Citation2010). The high number of visits to the Forest by the lake is also in accordance with humans’ innate preference for environments with closeness to water (Appleton Citation1975; Orians Citation1980; Wilson Citation1984). One could have expected that the Forest by the lake would have been the most popular even during the spring. However, the spring forest rehabilitation visits started in March, which, at this latitude, usually means that the landscape is covered in a relatively thick layer of snow. Due to the low temperatures, the participants also started their visits in the spring wearing their winter overalls, which resulted in somewhat restrained mobility. Given that the walking distance to the Forest by the lake was farther than to other open and bright forest settings, it seems reasonable to assume that the more difficult access to the Forest by the lake made it easier to prefer forest settings closer to the meeting point by the shelter. As the weather became warmer and the snow melted, the easier access to the Forest by the lake made it more popular.
The mires had the best light conditions and a good view due to their openness, but they were not popular. This might be due to a lack of feeling safe and comfortable because the physical properties of the mires meant that there were no hiding spaces with a view (Appleton Citation1975; Stamps Citation2010). Even the accessibility was moderately reduced due to the wetness of the mires. The Spruce forest, the Mixed forest and the Forest with a small stream were the darkest forest settings, and this might have contributed to lower numbers of visits. In his study, Stamps (Citation2010) showed that people perceive darker conditions as more enclosed and, therefore, less favourable due to aspects of perceived safety.
We tested the effects of the forest visits on attention capacity with the NCPC task because people suffering from ED often show attentional disabilities (Sandström et al. Citation2005). The spontaneous reversals showed an interaction effect during the rehabilitation period with the greatest difference between the before and after values at baseline testing. We suspect that the high number of spontaneous reversals before resting in the forest at baseline might be due to feelings of insecurity in the participant during the very first test session involving the NCPC task. However, the focus of this test lies in the reduction of focused reversals compared to the spontaneous reversals as well as the reduction of focused reversals during the entire forest rehabilitation period. This study confirms the participants’ different reactions, which were identified in our earlier study (Sonntag-Öström et al. Citation2014), with an increased number of reversals when the participant actively tried to stop the perspective from reversing. The voluntary control, which is expected to reduce the perspective reversals, does not seem to be applicable for the participants in our two studies. However, the significant effect with a reduced number of focused reversals showed that the forest rehabilitation improved attention capacity during single forest visits. However, there was no accumulated effect of the visits on attention capacity, which suggests that the effect is transitory. It is possible, however, that more frequent or longer forest visits are needed to observe prolonged effects.
The positive effect on mental state during the forest intervention seemed to be short-lived and probably did not have any significant effect on the long-term psychological health measures that are affected when suffering from ED. As mentioned above, there might be several contributory factors to this result, and the way this study was carried out might have influenced the outcome. In addition, both the frequency of forest visits and the time spent in the forest environment might have been insufficient.
The social interaction during the gatherings by the shelter might also have contributed to the positive effects on the participants’ mental state. This is something we could not control for. However, the mental state was measured just before and after the two hours of solitude, which probably has minimised the effect of social interaction.
Earlier research (Herzog et al. Citation1997) showed that the ability to reflect on one's current life-situation is enhanced by visits to natural surroundings. Patients suffering from ED are in great need of working through their attitudes and changing their behavioural patterns, and they need guidance when doing so. Our study focused on the actual restorative effects of the boreal forest itself and, therefore, any therapeutic discussions during the forest visits were avoided by the leaders. Based on this, a reasonable interpretation of our results is that access to reflective thinking does not help people suffering from ED in their recovery if tools for new coping strategies are not being provided. A forest rehabilitation closely integrated with CBR would possibly have resulted in more beneficial effects on ED. The integration of time for self-reflection during forest visits with the sharing of other participants’ experiences in the CBR and vocational measures including developing new skills and coping strategies, might together be effective in restoring health. Garden therapy, when integrated into a multimodal rehabilitation, has already shown positive results when used for stress relief (Adevi & Lieberg Citation2012; Pálsdóttir et al. Citation2014; Währborg et al. Citation2014).
Most of the participants in this study had suffered from severe ED for several years, which also might have influenced the outcome. The recovery from severe ED is known to occur gradually over a long time, and people suffering from ED also usually require a multitude of different measures to improve their health (SOU Citation2011). In their study, Stenlund et al. (Citation2009) showed that the SMBQ scores reached a level of 4.0 two years after the start of the CBR. In our study, the mean level of the SMBQ score was still elevated in both groups and remained above 4.0 at the end of the study period.
The desired statistical power was not achieved due to difficulties in recruiting participants, but we still consider the results to be reliable. There was no indication of differences in the psychological health outcome measures between the two groups, and we would presumably have obtained the same results even if we had recruited our preferred number of participants. The significant changes over time in the mental state estimations experienced by the participants in the forest intervention group showed the same pattern as in our earlier study with fewer participants (Sonntag-Öström et al. Citation2011).
In conclusion, our study does not support the hypothesis that the forest visits in themselves enhance the recovery from ED. However, the results from the forest rehabilitation group suggest that visits to forest environments improve mental state and short-term attention capacity. Also, accessibility, openness and good light conditions seem to be important features according to the patients’ preferences of the forest settings. Forest visits should probably be closely integrated with other important rehabilitative measures such as CBR and vocational rehabilitation, and this should be evaluated in future research.
Acknowledgements
This study is part of the research programme “Forest and Health” at the University of Agricultural Sciences (SLU) that is financially supported by the forest company Sveaskog, the Swedish Forest Agency, Ekhagastiftelsen, the municipality of Umeå, the Faculty of Forest Sciences at SLU, the Centre of Environmental Research in Umeå and the Västerbotten County Council. We would also like to thank all of the participants in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Related Research Data
References
- Adevi AA, Lieberg M. 2012. Stress rehabilitation through garden therapy. A caregiver perspective on factors considered most essential to the recovery process. Urban For Urban Gree. 11:51–58.
- Ahti T, Hämet-Ahti L, Jalas J. 1968. Vegetation zones and their sections in north-western Europe. Ann Bot Fenn. 5:169–211.
- Annerstedt M, Jönsson P, Wallergård M, Johansson G, Karlson B, Grahn P, Hansen ÅM, Währborg P. 2013. Inducing physiological stress recovery with sounds of nature in a virtual reality forest – results from a pilot study. Physiol Behav. 118:240–250.
- Annerstedt M, Währborg P. 2011. Nature-assisted therapy: systematic review of controlled and observational studies. Scand J Public Health. 39:371–388.
- Appleton J. 1975. The experience of the landscape. New York: John Wiley.
- Baer RA. 2003. Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin Psychol Sci Pract. 10:125–143.
- Beurskens A, Bultmann U, Kant I, Vercoulen J, Bleijenberg G, Swaen G. 2000. Fatigue among working people: validity of a questionnaire measure. Occup Environ Med. 57:353–357.
- Bowler DE, Buyung-Ali LM, Knight TM, Pullin AS. 2010. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Publ Health. 10:456–465.
- Brown K, Ryan R, Creswell J. 2007. Mindfulness: theoretical foundations and evidence for its salutary effects. Psychol Inq. 18:211–237.
- Brunner E, Domhof S, Langer F. 2002. Nonparametric analysis of longitudinal data in factorial experiments. New York: John Wiley.
- Chang CY, Hammitt WE, Chen PK, Machnik L, Su WC. 2008. Psychophysiological responses and restorative values of natural environments in Taiwan. Landsc Urban Plan. 85:79–84.
- Dahlin E, Nyberg L, Backman L, Neely AS. 2008. Plasticity of executive functioning in young and older adults: immediate training gains, transfer, and long-term maintenance. Psychol Aging. 23:720–730.
- Denissen JJA, Butalid L, Penke L, van Aken MAG. 2008. The effects of weather on daily mood: a multilevel approach. Emotion. 8:662–667.
- Försäkringskassan. 2013. Sjukfrånvaro i psykiska diagnoser: Svar på regeringsuppdrag. Delrapport [Swedish social security agency 2013. Sick-leave due to psychiatric diagnosis. Response to a governmental mission. Progress report]. [cited 2013 Oct 21]. Available from: http://www.forsakringskassan.se/wps/wcm/connect/40ab7654-ad14-450b-95c8-d6295f98b420/regeringsuppdrag_sjukfranvaro_i_psykiska_diagnoser_delrapport.pdf?
- Glise K, Hadzibajramovic E, Jonsdottir IH, Ahlborg Jr G. 2010. Self-reported exhaustion: a possible indicator of reduced work ability and increased risk of sickness absence among human service workers. Int Arch Occup Environ Health. 83:511–520.
- Grahn P. 2005. Om trädgårdsterapi och terapeutiska trädgårdar [Horticultural therapy and therapeutic gardens]. In: Johansson M, Küller M, editors. Svensk Miljöpsykologi. Lund: Studentlitteratur ; p. 245–262. Swedish.
- Herzog TR, Black AM, Fountaine KA, Knotts DJ. 1997. Reflection and attentional recovery as distinctive benefits of restorative environments. J Environ Psychol. 17:165–170.
- Herzog TR, Maguire CP, Nebel MB. 2003. Assessing the restorative components of environments. J Environ Psychol. 23:159–170.
- Hillman HC, Erickson KI, Kramer AF. 2008. Be smart, exercise your heart: exercise effects on your brain and cognition. Nat Rev Neurosci. 9:58–65.
- Kaplan R, Kaplan S. 1989. The experience of nature: a psychological perspective. New York: Cambridge University Press.
- Kämpfer S, Mutz M. 2013. On the sunny side of life: sunshine effects on life satisfaction. Soc Indic Res. 110:579–595.
- Kaplan S, Talbot JF. 1983. Psychological benefits of a wilderness experience. In: Altman I, Wohlwill J, editors. Behavior and the natural environment. New York: Plenum press; p. 63–203.
- Keller MC, Fredrickson BL, Ybarra O, Côté S, Johnson K, Mikels J, Conway A, Wager T. 2005. A warm heart and a clear head: the contingent effects of weather on mood and cognition. Psychol Sci. 16:724–731.
- Korczak D, Wastian M, Schneider M. 2012. Therapy of the burnout syndrome. GMS Health Technol Assess. 8:Doc05. http://dx.doi.org/10.3205/hta000103.
- Korpela KM. 2003. Negative mood and adult place preference. Environ Behav. 35:331–346.
- Levenstein S, Prantera C, Varvo V, Scribano ML, Berto E, Luzi C, Andreoli A. 1993. Development of the perceived stress questionnaire: a new tool for psychosomatic research. J Psychosom Res. 37:19–32.
- Liebert RM, Burk B. 1985. Voluntary control of reversible figures. Percept Mot Skills. 61:1307–1310.
- McNair DM, Lorr M, Droppleman LF. 1971. Manual for the profile of mood states (POMS). San Diego, CA: Educational and Industrial Testing Service.
- Melamed S, Ugarten U, Shirom A, Kahana L, Lerman Y, Froom P. 1999. Chronic burnout, somatic arousal and elevated salivary cortisol levels. J Psychosom Res. 46:591–598.
- Molin J, Mellerup E, Bolwig T, Scheike T, Dam H. 1996. The influence of climate on development of winter depression. J Affect Disord. 37:151–155.
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuja K, Salomon JA, Abdalla S, et.al. 2012. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 380:2197–2223.
- Orians GH. 1980. Habitat selection: general theory and applications to human behavior. In: Lockard JS, editor. The evolution of human social behavior. Chicago: Elsevier; p. 49–66.
- Pálsdóttir AM, Grahn P, Persson D. 2014. Changes in experiences value of everyday occupations after nature-based vocational rehabilitation. Scand J Occup Ther. 21:58–68.
- Robson P. 1989. Development of a new self-report questionnaire to measure self-esteem. Psychol Med. 19:513–518.
- Sandström A, Nyström Rhodin I, Lundberg M, Olsson T, Nyberg L. 2005. Impaired cognitive performance in patients with chronic burnout syndrome. Biol Psychol. 69:271–279.
- Searles H. 1960.The nonhuman environment in normal development and in schizophrenia. New York: International University Press.
- Socialstyrelsen (National Board of Health and Welfare). 2003. Utmattningssyndrom. Stressrelaterad psykisk ohälsa [Exhaustion disorder. Stress-related mental ill health]. [cited 2014 May 19]. Available from: http://www.socialstyrelsen.se/lists/artikelkatalog/attachments/10723/2003-123-18_200312319.pdf.
- Sonntag-Öström E, Nordin M, Slunga Järvholm L, Lundell Y, Brännström R, Dolling A. 2011. Can the boreal forest be used for rehabilitation and recovery from stress-related exhaustion? A pilot study. Scand J For Res. 26:245–256.
- Sonntag-Öström E, Nordin M, Lundell Y, Dolling A, Wiklund U, Karlsson M, Carlberg B, Slunga Järvholm L. 2014. Restorative effects of visits to urban and forest environments in patients with exhaustion disorder. Urban For Urban Gree. 13:344–354.
- SOU 2011: 15. Socialdepartementet. Statens offentliga utredningar. Rehabiliteringsrådets slutbetänkande [Ministry of health and social affairs. Official reports of the Swedish government. The final report from the Swedish National Council for Rehabilitation]. [cited 2014 Jan 20]. Available from: http://www.regeringen.se/content/1/c6/16/19/74/b3ca17b2.pdf. Swedish.
- Stamps AE. 2010. Effects of permeability on perceived enclosure and spaciousness. Environ Behav. 42:864–886.
- Stenlund T, Ahlgren C, Lindahl B, Burell G, Steinholtz K, Edlund C, Nilsson L, Knutsson A, Slunga Birgander L. 2009. Cognitively oriented behavioral rehabilitation in combination with Qigong for patients on long-term sick leave because of burnout: REST – a randomized controlled trial. Int J Behav Med. 16:294–303.
- Stenlund T, Nordin M, Slunga Järvholm L. 2012. Effects of rehabilitation programmes for patients on long-term sick leave for burnout: a 3-year follow-up of the REST study. J Rehabil Med. 44:684–690.
- Ulrich RS. 1984. View through a window may influence recovery from surgery. Science. 224:420–421.
- Währborg P, Petersson IF, Grahn P. 2014. Nature-assisted rehabilitation for reactions to severe stress and/or depression in a rehabilitation garden: long-term follow-up including comparisons with a matched population-based reference cohort. J Rehabil Med. 46:271–276.
- Wilson EO. 1984. Biophilia. Cambridge, MA: Harvard University Press.
- Zigmond A, Snaith R. 1983. The hospital anxiety and depression scale. Acta Psychiatr Scand. 67:361–370.
- Zuckerman M. 1977. Development of a situation-specific trait-state test for the prediction and measurement of affective responses. J Consult Clin Psychol. 45:513–523.