Abstract
Introduction. Papillary microcarcinomas (PMC) of the thyroid gland are defined according to The WHO Committee as papillary carcinomas measuring 10 mm or less in diameter. A large proportion of these tumours are found coincidentally in the treatment of symptomatic goitre and most cases follow an indolent course with an excellent prognosis. However, a more aggressive behaviour with regional and distant metastases does occur. The aim of this study was to evaluate if the immunohistochemical markers cyclin D1 or galectin-3 might indicate the presence of metastatic disease in patients with PMC at the time of diagnosis. Material and methods. From the 1st of January 1996 to 31st of December 2002 a total of 169 PMC patients were diagnosed and registered in the national Danish thyroid cancer database DATHYRCA and 131 of these were eligible for the study. Forty-three (33%) had histologically verified regional or distant metastases. Slides were cut from the primary tumour and immunostaining and quantification was subsequently performed. Results. The percentage of positive cells was examined for patients with and without metastases. For cyclin D1 the median values were 31% (range: 0–59) and 21% (range: 0–75), respectively, showing a statistically significant difference (p=0.02). For galectin-3 the medians were 87% (range: 6–96) and 85% (range: 0–99) and no significant difference was found. Conclusion. Cyclin D1 showed significantly higher median expression in patients with metastases compared to those without, indicating a correlation to tumour aggressiveness. However, both groups showed large variation in expression, which disqualify the marker as a discriminator for the detection of metastases. Galectin-3 was without any significant correlation to the presence of metastases from PMC.
Papillary microcarcinomas (PMC) of the thyroid gland are defined according to The WHO Committee as papillary carcinomas measuring 10 mm or less in diameter. A large proportion of these tumours are found coincidentally in the treatment of symptomatic goitre and most cases follow an indolent course with an excellent prognosis. However, a more aggressive behaviour with regional and distant metastases does occur and in these situations supplementary treatment with completing thyroid surgery, neck dissection and radioiodine ablation therapy might be indicated. To achieve an individualized and balanced treatment level with sufficient efficacy and without the risk of unnecessary complications an indicator of metastatic disease in PMC would be a valuable tool in the planning of treatment.
Cyclin D1 is a regulator of cell-cycle transition through G1 phase, the point where the cells commit themselves to another round of DNA replication. The nuclear protein forms a holoenzyme with a cyclin-dependant kinase (CDK), either CDK4 or CDK6, and phosphorylates and thereby inactivates the retinoblastoma gene product pRB, an important tumour suppressor protein. Cells overexpressing cyclin D1 have a shortened G1 phase and less dependence on growth factors and are able to transverse the G1/S transition under conditions that limit the growth of normal cells Citation[1], Citation[2]. Overexpression has been shown in a number of carcinomas, and furthermore seems to identify head and neck cancer patients and breast cancer patients with poor survival rates Citation[3].
Several studies have dealt with the subject of cyclin D1 expression in thyroid carcinomas Citation[4–7]. They have shown, that the protein is expressed in papillary thyroid carcinomas but not in normal thyroid tissue, and it is suggested that cyclin D1 expression may play a role in tumour progression. Khoo et al. Citation[8] and Muro-Cacho et al. Citation[1] examined whether expression of cyclin D1 could be used as a prognostic parameter in papillary thyroid carcinoma and both studies found that overexpression was correlated to lymph node metastases from this cancer.
In PMC, three studies suggest an association between overexpression and the presence of lymph node metastases Citation[9–11]. The results suggest that cyclin D1 might be an indicator of metastases from PMC and a study of a larger patient material seems justified.
Galectin-3 is a β-galactoside binding lectin which has been implicated in various biological functions, most of which are not precisely determined. Among these the protein has been shown to play a role in cell-cell interactions, adhesion, migration, invasion, tumour growth and metastatic and apoptotic resistance Citation[12]. It has been shown in several studies that galectin-3 is expressed in the cytoplasm of papillary thyroid carcinomas Citation[13–19] and it is therefore considered useful in the diagnosis of this cancer. Kawachi et al. Citation[19] compared the expression from primary tumours with metastases to those without. Their results revealed that cases with metastases scored significantly higher than those without. Only one study was found concerning the subject of galectin-3 expression in PMC. Cvejic et al. Citation[20] found expression in 80.9% (51/63) of tumours and concluded that galectin-3 is expressed at a slightly lower frequency in PMC compared to clinically evident papillary cancers. However, they also concluded that the presence of galectin-3 in clinically silent cases of PMC might indicate that the protein is not related to aggressiveness in this tumour.
Because earlier, but minor studies in this way indicate, that the expression of Cyclin D1 and galectin-3 might be correlated to the occurrence of metastatic disease it has been found of interest to examine these markers in a larger and national based patient material.
The purpose of this study is to evaluate if the immunohistochemical markers cyclin D1 or galectin-3 might be indicators of metastatic disease in PMC at the time of diagnosis.
Material and methods
The patients were retrieved from the national Danish thyroid cancer database – DATHYRCA. The database is prospectively registering data concerning Danish thyroid cancer patients. Registration has been done since the 1st of January 1996. Because of an ongoing cross-revision with The Danish National Cancer Registry the content of the database might change over time. To have a consistent set of data for immunohistochemical analyses the patients in the database at the 1st of January 2005 founded the basis of the actual study. Missing or supplementary data have been added when possible.
The inclusion criteria were as follows:
Histologically verified papillary thyroid carcinoma ≤ 10 mm in the largest diameter;
Diagnosis between the 1st of January 1996 and the 31st of December 2002;
Patient alive at the time of diagnosis;
No prior history of thyroid cancer.
Patients were diagnosed and treated according to local recommendations. Only histologically verified metastases were considered an event. No systematic lymph node surgery was performed in the group without suspicion of regional metatsases. Selected characteristics of the patient material are shown in .
From the paraffin embedded specimens 5 µm thick sections were cut and mounted on coated slides, dried at 60°C, dewaxed and rehydrated. The endogenous peroxidase reaction was blocked in 1.5% hydrogen peroxide in TBS buffer, pH 7.4 for 10 min. Antigen retrieval was performed using microwave treatment for 15 min in a solution of 10 mM Tris and 0.5 mM EGTA at pH 9 (TEG). Tissue-Tek containers (Miles Inc, Elkhart, IN USA), each with 24 slides in 250 mL buffer were placed on the edge of a turntable inside a microwave oven. Slides were heated for 11 min full power (900 W), then for 15 min at 440 W. After heating, slides remained in buffer for 15 min.
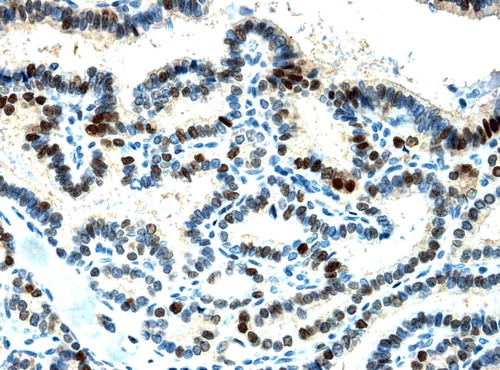
The immunostaining for cyclin D1 was performed on the Autostainer Universal Staining System (DakoCytomation, Glostrup, Denmark). The machine applies the reagent, a rabbit monoclonal antibody (Lab Vision, USA, Cyclin D1 Clone SP4, Code nr.RM-9104), to horizontally placed slides. The degree of dilution was 1 + 200 and the incubation period was 60 min at room temperature. The detection system was the Advance system (DakoCytomation, Glostrup, Denmark). Immunostaining was followed by a brief nuclear counter staining in Mayer's haematoxylin. Finally cover slips were mounted. shows a cyclin D1 staining of a histologic slide.
Figure 1. Cyclin D1 staining of papillary microcarcinoma (×200)
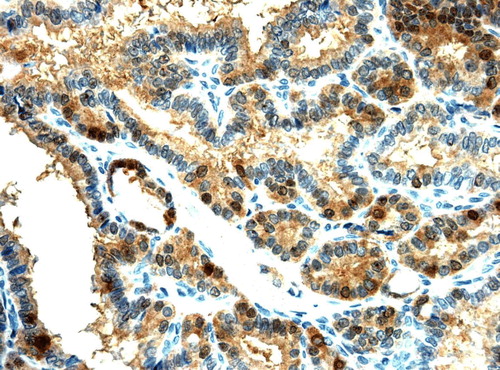
Immunostaining for galectin-3 was also performed on the Autostainer Universal Staining System (DakoCytomation, Glostrup, Denmark) in this process applying a mouse monoclonal antibody (Novocastra, UK, Galectin-3 Clone 9C4, code nr. NCL-GAL-3), to the slides. The degree of dilution was 1 + 400 and the incubation period was 60 min at room temperature. The detection system was the Envision + system K4001 (DakoCytomation, Glostrup, Denmark). Immunostaining was followed by a brief nuclear counter staining in Mayer's haematoxylin. Finally cover slips were mounted. shows a galectin-3 staining of a histological slide.
Figure 2. Galectin-3 staining of papillary microcarcinoma (×200)
Negative and positive controls were performed as a standard routine.
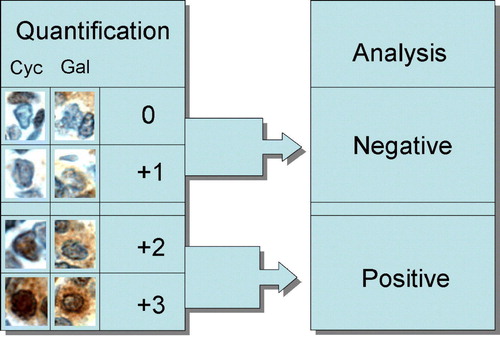
Quantification of the two immunohistochemical markers was done after the same principals; cyclin D1 is a nuclear staining and for galectin-3 the staining is cytoplasmatic. Two times 100 cells at 200× magnification were counted with the use of a grid; the first 100 cells were counted in a random area of the tumour and the second 100 at the opposite quadrant. During the quantification the examiner was blinded according to the metastatic status of the patients. The cells were graded by an arbitrary scale in which negative cells were registered as 0, weak positivity as +1, moderate positivity as +2 and strong positivity as +3.
For the statistical analysis of the immunohistochemical markers the cells with moderate or strong staining (+2 or +3) were considered positive and the cells with weak or no staining (+1 or 0) were considered negative. An illustration of this aspect is shown in .
Figure 3. Principles behind the quantification and analysis of immunohistochemical markers. “Cyc” means Cyclin D1 (nuclear staining), “Gal” means Galectin-3 (cytoplasmic staining)
Statistical analyses were performed by the clinical data management and analysis system Medlog. Wilcoxon rank sum test were used for comparison of continuous variables between two groups. Spearman's rank was used for correlation between variables and a t-test was used to test the hypothesis, that the two variables in question are independently distributed. For analyses of categorical data, the χ2 test with correction was used. A p-value < 0.05 was considered statistically significant. All tests were two-sided.
Results
The number of patients eligible for the study was 131. Among these 43 had histologically verified regional or distant metastases (33%) at the time of primary treatment.
The cyclin D1median percentage of cells according to expression category for patients with and without metastases can be seen from . The percentage of positive cells (+2 and +3) was examined for patients with and without metastases. The median values were 31 (range: 0–59) and 21 percentage (range: 0–75), respectively. This difference was statistically significant in a Wilcoxon rank sum test (p = 0.02). A graphic illustration showing the percentage of positive cells in each case for the groups with and without metastases is presented in . The overall median value of 23% is indicated by the solid line.
Figure 4. Percentage of Cyclin D1 positive cells (+2 and +3) in each case of 131 papillary microcarcinomas combined with the median for the whole group, the metastatic (43 patients) and the non metastatic ones (88 patients).
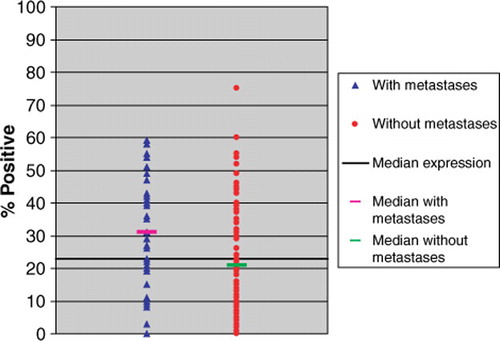
Table I. Selected characteristics according to the presence of metastases for 131 patients with papillary microcarcinoma. Neck dissection includes all types also isolated level VI procedures.
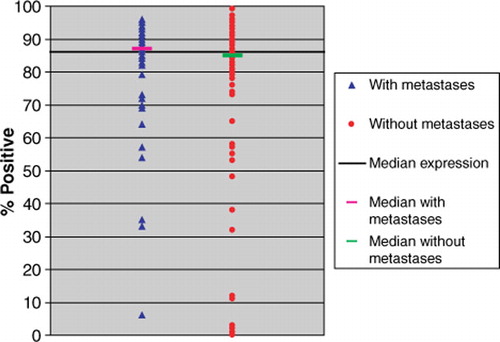
The galectin-3median percentage of cells according to category for patients with and without metastases is shown in . The overall galectin-3 median of positive cells was 86%. The percentage of positive cells (+2 and +3) was examined for patients with and without metastases and a median of 87 (range: 6–96) and 85 (range: 0–99) percent was found, respectively (). This difference was not significant in a Wilcoxon rank sum test (p = 0.27).
Figure 5. Percentage of galectin-3 positive cells (+2 and +3) in each case of 131 papillary microcarcinomas combined with the median for the whole group, the metastatic (43 patients) and the non metastatic ones (88 patients).
Of 43 patients with metastases 42 (97.7%) had regional lymph node metastases and only one patient (2.3%) had distant metastasis (lungs). When the analyses were repeated omitting the patient with distant metastasis, only including those with regional spread, the findings were almost unchanged (Cyclin D1; p = 0.01 and galectin-3; p = 0.21).
A correlation test of the overall series (n = 131) based on the percentage of positive cells was performed and no significant correlation between the two markers in question was found (Spearman's rho = 0.12 and p = 0.17).
A total of 22 patients with PMC were excluded from the study because it was not possible to retrieve the specimens (15 patients) or because no tumour tissue was left in the paraffin block (7 patients). To investigate if these patients were comparable to the study group some key-variables were analysed. The median tumour size was 3.5 mm (range: 1–10); median age at diagnosis was 46.3 years (range: 32.1–78.7), male/female ratio was 1/10 and the percentage of patients with metastases was 13.6%. By comparison to the patients included for the study no significant differences were found.
Discussion
The purpose of the actual study was to evaluate if the immunohistochemical markers cyclin D1 or galectin-3 might be indicators of metastatic disease at the time of diagnosis and perhaps be a tool of guidance in the planning of treatment. It has neither been the aim to correlate the expression to later recurrences nor survival. Therefore, no time factors are included in the analyses.
The treatment of thyroid cancer in Denmark is centralized in five university centres for Head and Neck Oncology and one department of general surgery. These six centres are responsible for registration in the national thyroid cancer database DATHYRCA, which is situated in The DAHANCA (Danish Head and Neck Cancer Group) structure. During the process of the actual study all pathological and some clinical records have been reviewed and corrections made in the database when indicated.
Only patients with histologically proven metastases have been considered an event. In patients without suspicion no systematic lymph node surgery has been performed to secure their status, which might be a weakness since very small metastases could have been missed. However, all patients have been subjected to a full diagnostic procedure in most cases including radiography of chest and ultrasound examination of the neck.
The basic characterization () of the patient material shows significant more males in the metastatic group. This might be because the cervical metastases have been the first sign in most of these patients explaining that the sex-distribution tends towards a more fifty-fifty distribution normally observed in thyroid cancer series. In the non-metastatic group the majority of patients might have been diagnosed by coincidentally found micro foci of papillary carcinoma in presumed benign goitres. Therefore the sex-distribution is in female favour as seen in most surgically treated benign series. The observed differences in surgical procedures are natural consequences of the tumour stage.
Table II. Median percentage of cells in the four Cyclin D1 and Galectin-3 expression categories according to the presence of metastases in 131 patients with papillary microcarcinoma. Because median values are used the total sum in each column may not be 100%.
Analyses of basic parameters for the 22 patients with PMC not eligible for the study did not show any significant differences compared to those included and the loss is considered without essential influence on the results.
Since the surgical specimens were prepared at different pathological departments some differences in the fixation process may exist. Ideally, all specimens should have been stained simultaneously. However, this was not possible as the specimens were retrieved from several departments of pathology and received on different dates. Consequently, to keep up with the project schedule, slides were stained in more steps. As standardized procedures and automated staining machines have been employed the impact of day-to-day variation is estimated to be insignificant.
Difficulty was sometimes experienced in grading the cells according to the criteria of quantification. The clearest distinction was observed from +1 to +2 where +2 cells are distinctly brown. In order to ensure maximal reproducibility, 0 and +1 was regarded as negative, and +2 and +3 as positive, for the analysis. The markers (Cyclin D1 and galectin-3) were simply chosen because newer literature indicates that they might contain significant information concerning the metastatic potential of papillary thyroid carcinomas and not because of a presumed biological connection. However, to identify a possible relation between the two markers a correlation test was performed. It showed no correlation.
Several quantification methods are possible in a study like this. Evaluation of “hot spots” might have been a possibility. Because of difficulties in defining and identifying these in very small and relatively homogenous tumours like PMC this method was not chosen. In the actual quantification process two times 100 tumour cells were counted in random areas and the cells categorized according to grade of positivity.
Two studies have previously dealt with the subject of cyclin D1 expression and metastases from PMC of the thyroid. Khoo et al. Citation[10] examined the expression in tumours presenting as gross regional metastases and compared this with the expression in controls with nonmetastasizing microcarcinoma. They found that 20 of 22 (90.9%) metastasizing tumours overexpressed cyclin D1 compared to only 3 of 34 (8.8%) nonmetastasizing tumours. Hence cyclin D1 was significantly overexpressed in the first group. Ito et al. Citation[11] did not find any relationship between metastases from papillary microcarcinoma and cyclin D1 expression, but found a pattern of high expression level of cyclin D1 and low expression level of p27 more frequently in 19 cases with clinically apparent metastases as opposed to 14 cases with occult metastasis and 22 patients without metastasis. The patient materials in the two studies were not completely comparable since Ito et al. classified their patients by preoperative ultrasonography while the cases of Khoo et al. were diagnosed by intraoperative findings. The classification in our study was also based on intraoperative findings but supplemented with the result of histopathological examination of the specimens. By this procedure some patients with small not palpable or ultrasonographically visible metastases might be identified. Therefore, our study might implement a group of patients not examined by Khoo et al. and classified as occult metastases in the study by Ito et al.
When we compared the expression of cyclin D1 in patients with and without metastases a significant difference was found. Thus, our results indicate a correlation between the expression of cyclin D1 and the presence of metastases. However, the level of expression of the marker varied over a broad range in both the patients with and without metastases and a significant overlap was observed. Therefore, the immediate usefulness as a clinical marker for metastases in PMC is doubtful and further investigation is needed in order to determine whether cyclin D1 might be a marker for a subgroup of metastases.
Several studies Citation[15–17], Citation[19], Citation[21], Citation[22] have shown that cytoplasmic expression of galectin-3 is high in papillary carcinomas and therefore it can be useful in the diagnosis of this cancer. In the actual study of PMC the galectin-3 expression was generally high with a median of 86% positive cells in the tumours, indicating that the usefulness also applies for this variant of the papillary carcinoma. Cvejic et al. Citation[23] examined galectin-3 in tumours from 63 patients incidentally diagnosed with papillary microcarcinoma after surgery for benign or autoimmune causes. The results showed that 51 cases were found to be positive, and it was proposed that galectin-3 is not related to tumour aggressiveness since it is expressed in clinically silent PMC. The findings in our study support this theory, since no difference in median expression between tumours with and without metastases was found.
Conclusion
Cyclin D1 showed significantly higher median expression in patients with metastases, than in those without indicating a correlation to tumour aggressiveness. However large variation in expression in both groups seems to disqualify the marker as a discriminator for the detection of metastases. Galectin-3 was without any significant correlation to the presence of metastases from PMC.
Acknowledgements
This is a study from The Danish Thyroid Cancer Group – DATHYRCA. The authors thank all who have contributed patient information to the DATHYRCA database or tissue specimens for the immunohistochemical part of the study. We also thank the financial supporters: “Statens forskningsstyrelse”, “Dagmar Marshalls fond” and “Fonden for lægevidenskabelig forskning ved Fyns Amts Sygehusvæsen”. According to the rules The Regional Scientific Ethical Committee has been informed about the study. The results have been presented at the 18th Annual Meeting of The Scandinavian Society of Head and Neck Oncology, Denmark April 27th 2006.
References
- Muro-Cacho CA, Holt T, Klotch D, Mora L, Livingston S, Futran N. Cyclin D1 expression as a prognostic parameter in papillary carcinoma of the thyroid. Otolaryngol Head Neck Surg 1999; 120: 200–7
- Neumeister P, Pixley FJ, Xiong Y, Xie H, Wu K, Ashton A, et al. Cyclin D1 governs adhesion and motility of macrophages. Mol Biol Cell 2003; 14: 2005–15
- Frierson HF, Jr., Gaffey MJ, Zukerberg LR, Arnold A, Williams ME. Immunohistochemical detection and gene amplification of cyclin D1 in mammary infiltrating ductal carcinoma. Mod Pathol 1996; 9: 725–30
- Wang S, Lloyd RV, Hutzler MJ, Safran MS, Patwardhan NA, Khan A. The role of cell cycle regulatory protein, cyclin D1, in the progression of thyroid cancer. Mod Pathol 2000; 13: 882–7
- Basolo F, Caligo MA, Pinchera A, Fedeli F, Baldanzi A, Miccoli P, et al. Cyclin D1 overexpression in thyroid carcinomas: Relation with clinico-pathological parameters, retinoblastoma gene product, and Ki67 labeling index. Thyroid 2000; 10: 741–6
- Saiz AD, Olvera M, Rezk S, Florentine BA, McCourty A, Brynes RK. Immunohistochemical expression of cyclin D1, E2F-1, and Ki-67 in benign and malignant thyroid lesions. J Pathol 2002; 198: 157–62
- Pickett CA, Agoff SN, Widman TJ, Bronner MP. Altered expression of cyclins and cell cycle inhibitors in papillary thyroid cancer: Prognostic implications. Thyroid 2005; 15: 461–73
- Khoo ML, Beasley NJ, Ezzat S, Freeman JL, Asa SL. Overexpression of cyclin D1 and underexpression of p27 predict lymph node metastases in papillary thyroid carcinoma. J Clin Endocrinol Metab 2002; 87: 1814–8
- Lantsov D, Meirmanov S, Nakashima M, Kondo H, Saenko V, Naruke Y, et al. Cyclin D1 overexpression in thyroid papillary microcarcinoma: Its association with tumour size and aberrant beta-catenin expression. Histopathology 2005; 47: 248–56
- Khoo ML, Ezzat S, Freeman JL, Asa SL. Cyclin D1 protein expression predicts metastatic behavior in thyroid papillary microcarcinomas but is not associated with gene amplification. J Clin Endocrinol Metab 2002; 87: 1810–3
- Ito Y, Uruno T, Takamura Y, Miya A, Kobayashi K, Matsuzuka F, et al. Papillary microcarcinomas of the thyroid with preoperatively detectable lymph node metastasis show significantly higher aggressive characteristics on immunohistochemical examination. Oncology 2005; 68: 87–96
- Califice S, Castronovo V, Van Den BF. Galectin-3 and cancer (Review). Int J Oncol 2004; 25: 983–92
- Bartolazzi A, Gasbarri A, Papotti M, Bussolati G, Lucante T, Khan A, et al. Application of an immunodiagnostic method for improving preoperative diagnosis of nodular thyroid lesions. Lancet 2001; 357: 1644–50
- Coli A, Bigotti G, Zucchetti F, Negro F, Massi G. Galectin-3, a marker of well-differentiated thyroid carcinoma, is expressed in thyroid nodules with cytological atypia. Histopathology 2002; 40: 80–7
- Feilchenfeldt J, Totsch M, Sheu SY, Robert J, Spiliopoulos A, Frilling A, et al. Expression of galectin-3 in normal and malignant thyroid tissue by quantitative PCR and immunohistochemistry. Mod Pathol 2003; 16: 1117–23
- Gasbarri A, Martegani MP, Del Prete F, Lucante T, Natali PG, Bartolazzi A. Galectin-3 and CD44v6 isoforms in the preoperative evaluation of thyroid nodules. J Clin Oncol 1999; 17: 3494–502
- Kovacs RB, Foldes J, Winkler G, Bodo M, Sapi Z. The investigation of galectin-3 in diseases of the thyroid gland. Eur J Endocrinol 2003; 149: 449–53
- Mehrotra P, Okpokam A, Bouhaidar R, Johnson SJ, Wilson JA, Davies BR, et al. Galectin-3 does not reliably distinguish benign from malignant thyroid neoplasms. Histopathology 2004; 45: 493–500
- Kawachi K, Matsushita Y, Yonezawa S, Nakano S, Shirao K, Natsugoe S, et al. Galectin-3 expression in various thyroid neoplasms and its possible role in metastasis formation. Hum Pathol 2000; 31: 428–33
- Cvejic D, Savin S, Petrovic I, Paunovic I, Tatic S, Krgovic K, et al. Galectin-3 expression in papillary microcarcinoma of the thyroid. Histopathology 2005; 47: 209–14
- Bartolazzi A, Gasbarri A, Papotti M, Bussolati G, Lucante T, Khan A, et al. Application of an immunodiagnostic method for improving preoperative diagnosis of nodular thyroid lesions. Lancet 2001; 357: 1644–50
- Mehrotra P, Okpokam A, Bouhaidar R, Johnson SJ, Wilson JA, Davies BR, et al. Galectin-3 does not reliably distinguish benign from malignant thyroid neoplasms. Histopathology 2004; 45: 493–500
- Cvejic D, Savin S, Petrovic I, Paunovic I, Tatic S, Krgovic K, et al. Galectin-3 expression in papillary microcarcinoma of the thyroid. Histopathology 2005; 47: 209–14