Abstract
Purpose. Recently, Varian Medical Systems have announced the introduction of a new treatment technique, RapidArc, in which dose is delivered over a single gantry rotation with dynamically variable MLC positions, dose rate and gantry speed. At Rigshospitalet, the RapidArc technique was brought into clinical practice in May 2008 for treatment of prostate cancer patients. We report here our experiences with performing treatment planning using the Eclipse RapidArc optimization software for this patient group. Material and methods. A stand-alone installation of Eclipse 8.5 with RapidArc optimization capability was performed at Rigshospitalet. Patient data for 8 prostate cancer patients were imported, most of whom were previously treated at Rigshospitalet using IMRT. Three of the patients were treated at Rigshospitalet using the RapidArc technique. Treatment plans were optimized using objectives as given by standard guidelines for clinical treatment planning. RapidArc plans were compared to the IMRT plans by which the patients were actually treated or in the three cases treated with the RapidArc technique to IMRT plans achieved using standard guidelines. Comparison was done with respect to target coverage, doses to rectum and bladder, over-all maximum dose and number of monitor units. Results. Overall, the RapidArc treatment plans gave better or equal sparing of the organs at risk than the IMRT treatment plans. The number of monitor units was lower in most cases, by up to approximately 75%. However, the target dose homogeneity was not as high as for IMRT. The low-dose bath was larger than for IMRT. Conclusion. RapidArc optimization is very promising, especially regarding the potential of reducing the number of monitor units, while providing good sparing of organs at risk. Some improvement is still warranted with respect to achieving high target dose homogeneity.
Over the last decade or more there has been an increasing interest in the use of arc delivery of radiation for treatment of cancer. This has been a part of the computer aided development towards achieving highly conformal radiation doses to the tumors while sparing the surrounding healthy tissues. The principle of simple conformal arc therapy is to spread the entrance dose shaped to the projected tumor outline over many angles with the rotational center in the tumor so that the high dose is focused there with a steep fall-off outside the tumor. Following another path, the development has included the introduction of intensity-modulated radiotherapy (IMRT) which has the ability to tailor the dose distribution around targets with complex shapes, facilitated by inverse optimization to the desired dose distribution often using many (5–9) beam angles. In the most advanced approaches, the intensity modulated and arc delivery approaches are combined to techniques such as intensity-modulated radiosurgery Citation[1], intensity-modulated arc therapy Citation[3], and helical tomotherapy Citation[4].
Most recently, a single arc modulated technique has been introduced by Varian Medical Systems, Inc., and termed RapidArc™. With this technique, the MLC positions, the dose rate and the gantry speed can be dynamically varied during the delivery of radiation over one arc, typically taking 70–90 seconds (for delivery of a 2 Gy fraction). The pattern of the delivery is obtained by inverse optimization in the Eclipse environment to achieve specified dose objectives Citation[5]. RapidArc™ was released for clinical use in late April 2008, and was installed at Rigshospitalet, Copenhagen University Hospital, in the beginning of May 2008.
Since mid 2007, Rigshospitalet has been involved in collaboration with Varian Medical Systems for testing of the RapidArc optimization environment, and of the RapidArc delivery equipment. We here report our experiences with using the arc optimization, specifically for prostate cancer irradiation, and results obtained using the clinically released version of the optimizer (Eclipse version 8.5).
Material and methods
CT-scans for eight patients with prostate cancer were imported into the Eclipse treatment planning system (version 8.5). Five of the patients have been treated at Rigshospitalet using a five-field sliding window IMRT technique. Two of the patients started their treatment with five-field IMRT, and were then transferred to RapidArc during their treatment course, and one patient started treatment using the RapidArc technique. This last patient was also planned for IMRT, although not treated according to the IMRT plan. Two patients were prostastectomized and the prescribed dose was 66 Gy to the prostate bed. For five patients, prescription dose was 78 Gy, and for one patient prescription dose was 74 Gy. All plans were normalized to PTV mean dose. Patient characteristica are given in .
Table I. Demographics of patient group.
All IMRT optimizations were performed in Eclipse version 8.0, and all RapidArc optimizations were performed in Eclipse 8.5. In Eclipse 8.5, the couch including rails (Exact couch) is modeled during both optimization and dose calculation, while this is not the case in Eclipse 8.0. All IMRT plans were exported to Eclipse 8.5 and recalculated (without the couch model as this was not used during IMRT optimization). For both the IMRT and the RapidArc plans, beam angles irradiating through the couch rails were avoided. For RapidArc plans, the rails were placed centrally in the couch, and the gantry rotation did not include the angles from directly below the couch (see below). For the IMRT plans, the rails were placed at the outer edges of the couch, and these beam angles were likewise avoided (see below). Dose calculation was performed using the AAA algorithm.
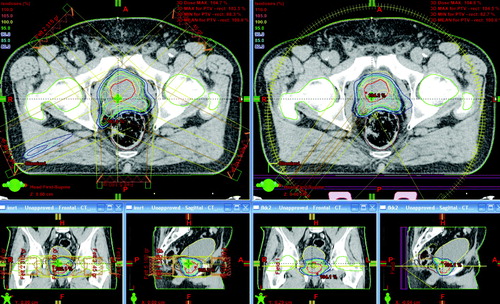
The IMRT plans used five fixed beam angles – 245, 315, 45, 115 and 180 degrees (IEC scale)-with the collimator set to 2 degrees to minimize tongue and groove effect. For the RapidArc plans, arcs covering 300 degree arcs from 210 to 150 degrees clockwise rotation were used. The posterior angles were not used in order to avoid beaming through the central couch rails. For the RapidArc plans, the collimator was set to approximately 45 degrees, however the angle was variable from patient to patient, and was chosen automatically by the system during optimization.
In , the IMRT and RapidArc beam setups are shown for one patient.
Figure 1. The beam set-up for the RapidArc plan (right) and the IMRT plan (left) for patient 5.
For all optimizations (IMRT and RapidArc), the plan objectives were:
Minimum 95% of the prescription dose to at least 95% of the PTV minus rectum (PTV including rectum for the two prostastectomized patients).
Maximum over-all accepted hotspot dose was 107% of the prescription dose.
The bladder and rectum should receive as little as possible above 50 Gy and above respectively 60 Gy for prescription dose 66 Gy, and above 70 Gy for prescription doses 74 and 78 Gy.
The femoral heads should receive no more than 50 Gy in all cases.
The optimization criteria (dose objectives and priorities) were interactively tuned during optimization to achieve the best possible treatment plan. Specifically, the risk organ objectives were continuously lowered for as long as this did not compromise target coverage.
For each patient, the IMRT plans and RapidArc plans are compared with respect to target coverage and doses to healthy tissues. We report the following magnitudes:
Whether or not the femoral heads receive more than 50 Gy
The bladder volume receiving more than 50 Gy and 60/70 Gy
The rectum volume receiving more than 50 Gy and 60/70 Gy
The PTV volume receiving more than 95% of the dose
The PTV minus rectum volume receiving more than 95% of the dose
The hotspot dose (highest point dose)
The number of monitor units given in the plan
Planning for RapidArc treatment is still at the start of clinical implementation which means that we are still on the learning curve. There is also an ongoing further development of the possibilities and features, such as interactive tuning, of the RapidArc optimization process.
The optimization sequence is a stochastic process which means that two optimizations with identical initial conditions can give different results. At this time we perform several optimizations for each patient in order to achieve the best plan. The stochastic nature of the optimization process is necessary due to the big amount of possibilities for a single treatment.
At the time of this study an optimization takes 25–30 minutes and a volume calculation takes about 15 minutes.
Results
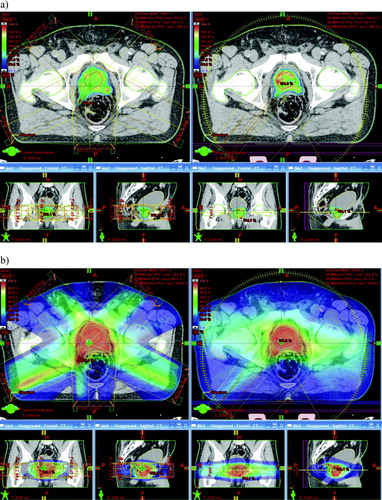
In , an example is shown for one case of the dose distributions resulting from the IMRT and RapidArc optimizations, illustrating cut-off levels at the 95% and 5% dose levels.
Figure 2. Dose wash images for the RapidArc plan (right) and the IMRT plan (left) for patient 5. In (a) the lower cut-off level is 95% dose, and in (b) the cut-off level is 5% dose. In both cases, the upper cut-off level is 104.5% dose.
In , the optimization results are summarized for all eight patients for both the IMRT and RapidArc plans. Generally, the RapidArc plans are better than the IMRT plans with respect to bladder and rectum doses-by up to ∼23% less volume receiving the high dose levels. In only one case is the bladder volume receiving more than 50 Gy slightly higher for the RapidArc plan. The plans are comparable with respect to dose to femoral heads. With respect to PTV coverage, the IMRT plans are generally better (six of eight cases). In two RapidArc plans is the volume receiving 95% dose smaller than the accepted 95%, whereas this is only true for one IMRT plan. However looking at the PTV minus rectum, several (five out of seven) of the RapidArc plans are better than the IMRT plans. The hotspots are higher for the RapidArc plans in all cases, by up to 3.4%, and in one case slightly (0.4%) above the accepted 107%. The number of monitor units is lower for the RapidArc plans for six of eight cases.
Table II. Treatment plan parameters for IMRT and RapidArc plans for all patients.
The integral dose to the whole body is comparable for IMRT and RapidArc plans, although generally slightly higher (up to 0.7%) in the IMRT plans.
There is a larger low-dose bath for all RapidArc plans than for the IMRT plans. Looking for instance at the 5% dose level, this is received by 17.9–37.8% of the entire scanned range for the RapidArc plans, and by 15.0–32.2% for the IMRT plans with a mean difference of 3.9%. This effect is also seen in the dose wash illustration in , and is inherent to the arc delivery technique.
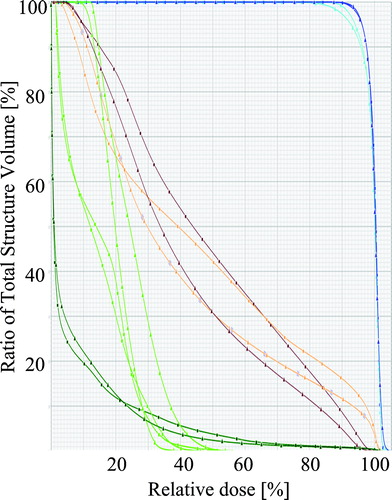
At we have showed a dose volume histogram for a single comparing IMRT and RapidArc for the PTV and OAR.
Figure 3. The dose-volume histograms for the RapidArc and IMRT plans for patient 6. The triangles denote the RapidArc plan and the squares the IMRT plan. The color coding denotes: blue ∼ PTV, cyan ∼ PTV-rectum, dark green ∼ body, light green ∼ femoral heads, orange ∼ bladder, brown ∼ rectum.
Discussion
The results of this study indicate that the RapidArc™ technique can give better treatment for prostate cancer than IMRT in most cases. Given the treatment plans obtained in the present study, in all cases would the RapidArc plans have been chosen for treatment by the oncologists in the department based only on the doses to organs at risk and target coverage. In most cases, the amount of monitor units is also smaller in RapidArc plans than in IMRT plans.
Furthermore, the treatments are delivered in a single arc over approximately 70–90 seconds. These are considerably shorter times than it takes to deliver the IMRT plans, which take approximately 4–5 minutes to deliver. This obviously is good for patient through-put, but also the shorter time span of the treatment reduces the risk of positional displacements during the beam-on time. Specifically for prostate cancer, it has been shown that for some patients the prostate moves considerably (SD 0.9 mm, and range up to 2.5 mm) during the time frame of a short IMRT treatment (∼6 minutes), and that generally it is true that the longer the time span of the treatment the larger the movement Citation[2]. This movement is most probably due to bladder filling and bowel movements. With the short beam-on time of the RapidArc treatment, this risk is reduced. At our clinic, image guided set-up is performed on a daily basis using the ExacTrac X-ray system (BrainLab AG) with matching to gold markers implanted in the prostate. Combining this technique with the short beam delivery time, the treatment field margins from CTV to PTV can be safely maintained very tight at 5 mm in all directions.
Dosimetric verification of the delivery of RapidArc beams has been performed extensively at Rigshospitalet – first as part of a preclinical test installation, and also in connection with the introduction of the technique into clinical practice. Using several different dosimetric equipments, we have shown that there is high consistency between planned and delivered dose, and that the delivery is highly reproducible. Both the performance of the linac and daily QA for the single treatment show mechanical and dosimetric stability. The treatment delivery is performed with no interlocks, which means we have been able to use standard time slots from the first day of clinical introduction.
So far, we are only treating the group of prostate cancer patients using the RapidArc technique at Rigshospitalet. The plans are to expand with further cancer sites, starting with cervix cancer, then anal canal cancer, head and neck cancer and brain metastases. Treatment planning for all of these cancer sites have been investigated in other groups in the Varian initiated European RapidArc council (see below in acknowledgements).
Conclusion
We have demonstrated that the RapidArc treatment technique can be used advantageously in the radiation treatment of prostate cancer patients. The RapidArc treatment plans gave better sparing of organs at risk, in most cases smaller amount of monitor units, and good target homogeneity. The only parameter which was consistently better for the IMRT plans was the lower hotspot dose. Delivery of the RapidArc treatment plans can be performed 4–5 times faster than for a five-field IMRT technique using the same linac.
Acknowledgements
The authors wish to thank Varian Medical Systems for the fruitful collaboration in the RapidArc testing process, as well as the other clinics (the European “RapidArc council”) involved in the testing period – VU Medical center Amsterdam, CRLC Val d'Aurelle Montpellier, University Hospital Zürich, and Oncology Institute of Southern Switzerland Bellinzona.
Also, chief consultants at Rigshospitalet Peter Meidahl and head of department Svend Aage Engelholm are thanked for their contributions in assessing the treatment plans.
References
- Benedict SH, Cardinale RM, Wu Q, Zwicker RD, Broaddus WC, Mohan R. Intensity-modulated stereotactic radiosurgery using dynamic micro-multileaf collimation. Int J Radiat Oncol Biol Phys 2001; 50: 751–8
- Enmark M, Korreman S, Nystrom H. IGRT of prostate cancer; is the margin reduction gained from daily IG time-dependent?. Acta Oncol 2006; 45: 907–14
- Ma L, Yu CX, Earl M, et al. Optimized intensity-modulated arc therapy for prostate cancer treatment. Int J Cancer 2001; 96: 379–84
- Mackie TR, Balog J, Ruchala K, et al. Tomotherapy. Semin Radiat Oncol 1999; 9: 108–17
- Otto K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med Phys 2008; 35: 310–7