
Abstract
Background: Malignant pleural mesothelioma (MPM) is a rare occupational cancer with a poor prognosis. Even with a multimodality treatment approach, the treatment outcomes remain unsatisfactory. The use of asbestos has been banned in most developed countries, but MPM continues to be a significant occupational disease also in these countries. Aim of this study is to identify modern epidemiology and assess equality in care.
Methods: Our study cohort consists of 1010 patients diagnosed with MPM in Finland during 2000–2012. The data were collected from the Finnish Cancer Registry, the National Workers’ Compensation Center Registry and the National Registry of Causes of Death, Statistics Finland.
Results: Women were diagnosed a mean of 4.5 years later than males (p = .001), but survival did not differ (overall median survival 9.7 months). A workers’ compensation claim was more common in males (OR 11.0 [95% CI 7.5–16.2]) and in regions with a major asbestos industry (OR 1.7 [95% CI 1.3–2.2]). One-year and three-year survivals did not differ regionally. Patients without chemotherapy treatment had an inferior survival (RR 1.8 [95% CI 1.5–2.0]). The initial survival benefit gained with pemetrexed was diluted at 51 months.
Conclusions: MPM is a disease with a poor prognosis, although chemotherapy appears to improve survival time. Significant gender and regional variation exists among patients, with notable differences in diagnostic and treatment practices. Long-term outcomes with pemetrexed remain indeterminate.
Impact: Emphasize centralized consult services for the diagnosis, treatment and support that patients receive for MPM, facilitating equal outcomes and compensation.
Introduction
Malignant pleural mesothelioma (MPM) is a rare cancer, with a median survival of 12 months or less [Citation1–7]. The most important risk factor for MPM is exposure to asbestos, most commonly arising from occupational exposure, and thus, showing a higher incidence in males [Citation2,Citation8,Citation9]. The latency period from asbestos exposure to cancer can vary between 20 and 70 years [Citation2,Citation3,Citation5]. Globally, the incidence of mesothelioma still seems to be increasing [Citation3,Citation10]. The three main histologic subtypes are epithelioid, sarcomatoid and mixed subtype (biphasic), epithelioid being the predominant type [Citation3]. The epithelioid subtype has the best prognosis [Citation3,Citation5,Citation11].
In Finland, employers are legally obligated to insure their employees against occupational diseases and accidents [Citation12]. The National Workers’ Compensation Center is a nationwide institute that supervises this insurance system [Citation12].
The goal of this study was to describe the occurrence and demographics, the current therapy practices and the insurance claim and compensation policies of mesothelioma on a national level as well as a regional level in Finland. Use of asbestos in Finland was increasingly restricted starting in the 1970s and, finally, all use of asbestos was banned in Finland from 1994 onwards [Citation13,Citation14]. A secondary goal here was to evaluate the mortality of patients in relation to chemotherapy and pemetrexed treatment. In addition, we aimed to determine whether local differences exist in the treatment and claims practices.
Methods
Patients
The study cohort consists of 1010 patients diagnosed with MPM in Finland during 2000–2012. Data were derived from the Finnish Cancer Registry, the National Workers’ Compensation Center Registry and the National Registry of Causes of Death, Statistics Finland. The Finnish Cancer Registry collects nationwide information about malignancies diagnosed in the population. The data completeness in the Finnish Cancer Registry was recently reported to be 96% for all solid tumors and 99.2% for mesothelioma [Citation15]. The data are based on diagnostic information gathered from pathology laboratories and reports completed by clinicians as well as death notices. The information includes date of birth, gender, side of cancer (left, right, bilateral), histologic type (epithelioid, sarcomatoid, mixed, not otherwise specified), given therapies (surgery, chemotherapy, radiation therapy), date of diagnosis, date of death, causes of death and district of residence. The date of death served as the date of diagnosis in patients where MPM was diagnosed at autopsy to avoid negative survival times. The data had been collected from the Finnish Cancer Registry on 13 January 2014, to include all patients with reported International Statistical Classification of Diseases and Related Health Problems (ICD) diagnosis for mesothelioma and World Health Organization (WHO) pathologic tumor classification. All non-pleural mesothelioma patients’ registry data were verified that there were no pleural origin of the tumor. Occupational data had been collected from the National Workers’ Compensation Center Registry by means of cross-referencing the data from the Finnish Cancer Registry. The follow-up time for the patients still alive ended when the last update to the details of the death was conducted at Statistics Finland on 17 February 2017. The number of patients still alive was 23.
Statistical analysis
The data were analyzed by using IBM SPSS Statistics 22.0 and SAS Analytics 9.4. Survival time was calculated from the date of diagnosis to the date of death or 17 February 2017 for those alive. Survivals (mesothelioma mortality) are represented in the form of Kaplan–Meier curves (Wilcoxon test was used to test survival difference because we were interested in early survival times). A Cox proportional hazards regression model was used to examine the effect of confounding factors. The number of the population in the five healthcare districts and the number of men and women living in Finland during 2000–2012 were obtained from Statistics Finland, and these were used to calculate the incidences for these subgroups [Citation16]. The Finnish Population Information System is a high-quality register containing personal details about Finnish citizens as well as some foreign citizens [Citation17].
Ethical considerations
Approval to use the data was received from the Finnish National Institute for Health and Welfare, the National Workers’ Compensation Center and Statistics Finland. A statement of approval for the study protocol was given by the Ethics Committee of the Hospital District of Helsinki and Uusimaa (418/13/03/02/2015).
Results
Characteristics
Our cohort of 1010 patients comprised 801 men (79.3%) and 209 women (20.7%). Mean age at time of diagnosis was 68.1 years in men and 72.6 years in women (p = .001, T-test). Age at time of diagnosis ranged from 25.4 years to 96.2 years. The side on which mesothelioma occurred was reported for 872 patients (86.3%). It was right-sided in 497 cases, left-sided in 345 cases and bilateral in 30 cases at diagnosis. Diagnosis of MPM was not obtained until autopsy for 79 patients (7.8%). Patient characteristics are shown in .
Table 1. Patient characteristics.
Treatment
In the Finnish Cancer Registry, clinical supplemental information was submitted for 766 patients (75.8%). The number of patients treated with chemotherapy and/or radiotherapy was 440 and 167, respectively. Pemetrexed was officially approved for use in Finland in September 2004 by the Finnish Medicines Agency (Fimea) [Citation18], but the usage started somewhat earlier through clinical trials. In the group of 440 patients treated with chemotherapy, 269 received pemetrexed in some form, either as a single agent or in combination with some other agent.
Treatment methods seem to differ regionally (, ). Differences between healthcare districts were significant in all modalities (p < .05, Chi-square test). The treatment data are unknown for some patients, and therefore, these values might be slightly underestimated.
Table 2. Treatment practices among healthcare districts, N (%).
Incidence of MPM in Finland during the observation period
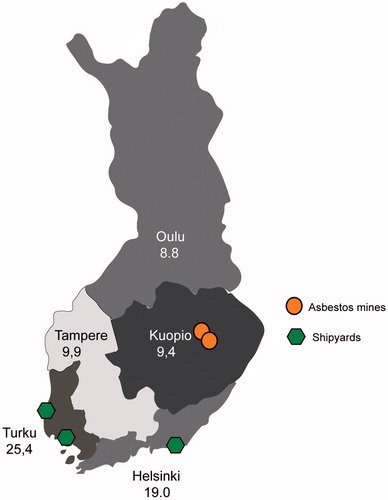
The incidence of MPM in the whole cohort was 14.7/million/year. demonstrates more closely the slight variation between each year. The incidence clearly differed between genders and regionally. The incidence of MPM in men was 23.8/million/year compared with only 6.0/million/year in women. The greatest incidence of MPM was 25.4/million/year in Turku University hospital district (TYKS), followed by 19.0/million/year in Helsinki University hospital district (HYKS). The incidences were markedly smaller in Tampere University hospital (TAYS), Kuopio University hospital (KYS) and Oulu University hospital (OYS) districts at 9.9/million/year, 9.4/million/year and 8.8/million/year, respectively. shows the geographical location of the Finnish healthcare districts and previous major industrial sources of asbestos. Differences between genders and healthcare districts were significant (p = .001, Chi-square test).
Figure 1. The incidence per year for the whole cohort is shown.
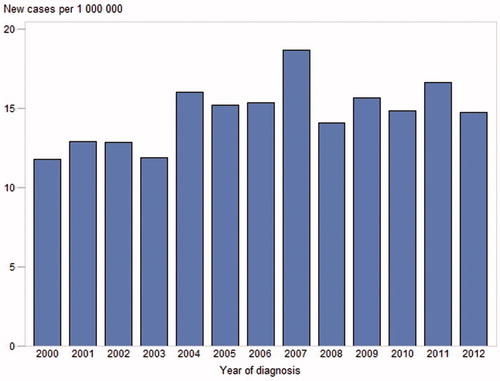
Figure 2. Five healthcare districts and major industrial plants. Shipyards are depicted by green pentagons and major asbestos mining locations by orange circles.
Occupational aspects
Collected occupational data included information about whether the patient has started a legal process regarding suspected occupational disease and made a claim for compensation (yes, no) and the registered outcome of this process (occupational disease, suspicion of occupational disease, or no occupational cause). Suspicion of occupational disease means that the patient has claimed for compensation with a negative outcome. Occupational disease may also be diagnosed after death.
The number of claims and occupational diseases for MPM differed between male and female patients. Altogether 519 men (64.8%) and 34 women (16.3%) submitted a claim for compensation for an occupational disease after the diagnosis of MPM, and mesothelioma was classified as an occupational disease for 528 men (65.9%) and for 22 women (10.5%). The odds ratio (OR) for men submitting a claim for workers’ compensation was 11.0 (95% CI 7.5–16.2).
MPM seemed to be better recognized as an occupational disease in the areas where a major asbestos industry was located (, ). The OR for patients making a workers’ compensation claim in the HYKS and TYKS healthcare districts combined was 1.7 (95% CI 1.3–2.2) compared with the other healthcare districts. Differences between healthcare districts and genders were significant in both number of claims and occupational diseases (p = .001, Chi-square test).
Table 3. Occupational aspects among healthcare districts, N (%).
Survival
The patients´ median survival (MS) differed depending on whether the patient died of MPM or with MPM. For two patients, this data was unavailable. MS in the group dying of MPM was 9.7 months. Altogether 944 patients (93.5%) died of MPM and only 41 patients (4.1%) died of other causes. The maximum survival time was 197.7 months (16.5 years) for a patient who is still alive. The 1-year survival was 43.0% and the 3-year survival 11.2%. The 1-year (p = 0.78, Chi-square test) and 3-year (p = 0.89, Chi-square test) survivals did not differ between healthcare districts. The survival time did not differ between genders (p = 0.65, Kaplan–Meier method, Wilcoxon test).
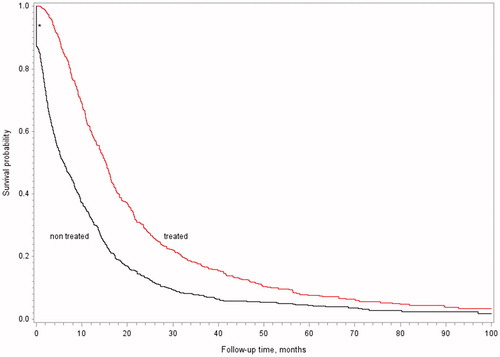
shows better survival for the group of patients treated with chemotherapy (p < .001, Kaplan–Meier method, Wilcoxon test) than in the group without chemotherapy treatment. We compared the treated and nontreated groups in terms of age, histology, gender and side of tumor to identify possible confounding factors and discovered that non-sarcomatoid subtypes and younger patients were more frequently treated with chemotherapy. Therefore, a Cox proportional hazards regression model was applied to test the role of histologic subtype and age on survival analysis, and the result remained significant (p = .001), albeit the effect was slightly diminished. The risk ratio (RR) for the non-chemotherapy group to die was 1.8 (95% CI 1.5–2.0).
Figure 3. Kaplan–Meier curve representing survival of a group treated with chemotherapy versus a group without chemotherapy treatment. *Survival is zero for patients whose disease was diagnosed at autopsy; hence, the vertical line at the beginning of the Kaplan–Meier curve.
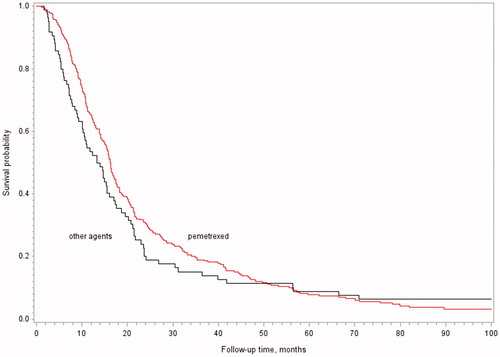
shows the survival for the group treated with pemetrexed compared with the group treated with other cytostatic agents. The pemetrexed group mostly consisted of patients treated with a combination of pemetrexed and either cisplatin (n = 77, 65.8%) or carboplatin (n = 58, 21.6%). Some patients received pemetrexed only (n = 31, 11.5%). The pemetrexed group initially appeared to have superior survival (p = .02, Kaplan–Meier method, Wilcoxon test), but the curves intersected at 51 months. A comparison with the same confounding factors aforementioned (age, histology, gender, side of tumor) was done for these two groups, and patients treated with pemetrexed were found to be older (mean age: 64.8 years for pemetrexed and 62.4 years for other cytostatic agents). A Cox proportional hazards regression model was computed (pemetrexed, age, histology), and no evidence of a survival benefit among patients treated with pemetrexed emerged (p = .16).
Figure 4. Kaplan–Meier curve representing survival of a group treated with pemetrexed versus a group treated with other cytostatic agents.
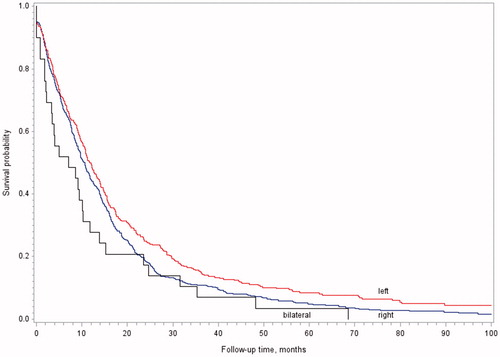
The side of MPM seemed to be a prognostic factor; the best survival is seen in patients with mesothelioma on the left side and the worst for bilateral disease (p = .03, Kaplan–Meier method, Wilcoxon test, ). The RR for patients with a right-sided MPM to die was 1.2 (95% CI 1.03–1.4) compared with patients with a left-sided MPM (patients with bilateral disease were excluded). No difference existed between these groups in gender, age, sarcomatous versus non-sarcomatous histology and chemotherapy and pemetrexed treatment.
Figure 5. Kaplan–Meier curve representing survival in terms of the side of mesothelioma.
Discussion
This study is based on systematically collected data from a national cohort of MPM patients in 2000–2012. A large variation in disease incidence exists regionally. There were major differences in how patients were treated and diagnosed as occupational disease in different geographical areas. Vast differences were also present in occupational claims depending on patients’ gender. Survival data confirm that mesothelioma remains a disease with a dismal prognosis, but the offered therapeutic means do have some influence on patient survival.
In our study, female patients were diagnosed at an older age than men. In contrast, another study [Citation19] showed no significant difference between genders in age at diagnosis in 1993–2008. Despite the later onset of mesothelioma in females in our cohort, the disease appears to progress equally in both genders. One explanation for the later onset of the disease might be that women have a lower occupational exposure to asbestos because of the traditional distribution of occupations between genders, which then results in a longer latency period.
The incidence of MPM during the study period in Finland was 14.7/million/year, which is much higher than the reported background incidence of 1–2 cases/million/year [Citation20]. Regional differences in MPM incidence were seen in our study, probably due to the distribution of the main asbestos-using industrial plants. Our study suggests that the incidence of MPM in Finland has not yet started to decline. In other European countries, the peak incidence period has been predicted to occur in the next few decades [Citation21].
Besides the variation in incidences, we also found regional differences in occupational disease practices. There was a clear indication that MPM was more frequently reported as an occupational disease in the areas where the incidence of MPM was high and the major asbestos-using industrial plants were located. In addition, the number of claims and occupational diseases also varied between males and females.
MPM is generally acknowledged to be a fatal malignancy, and the median survival of 9.7 months observed in our study in the group of patients dying of mesothelioma is consistent with previous publications [Citation4,Citation5]. The relatively low 1- and 3-year survival rates further emphasize the poor prognosis associated with MPM. In our study, the 1-year survival was similar to the results obtained in a Norwegian population for the period 2005–2009 [Citation22]. In contrast, a study performed in the Republic of Ireland between 1994 and 2009 showed lower 1-year and 3-year survival rates than we observed in the Finnish population [Citation23].
Chemotherapy treatment appeared to improve survival in MPM patients. However, we were unable to show any beneficial effect for pemetrexed treatment, despite the slight increase in survival initially seen in the pemetrexed group. In contrast to our results, the study by Vogelzang et al. [Citation24] in 2003 showed that treatment with the combination of pemetrexed plus cisplatin resulted in a significantly better survival than with cisplatin alone and the addition of pemetrexed was concluded to mainly cause this positive effect. Since their study showed survival time only to 30 months and in our study the intersection of the curves was located at 51 months, the results for pemetrexed are not fully comparable. A similar but earlier intersection of curves was also demonstrated in the study conducted by Shukuya et al. [Citation25], in which survivals were compared between the group treated with cisplatin plus pemetrexed and the group treated with cisplatin plus gemcitabine. It is noteworthy that our study was observational and differences between the patients with different treatment regimens may exist despite statistical controlling.
In our study, the side of the mesothelioma also seemed to be a prognostic factor, showing different survival times. Two previous studies have provided similar results [Citation26,Citation27]. Ak et al. [Citation27] suggested that this survival time difference by laterality could be due to structural differences between the lungs, leading to unequal distribution of asbestos fibers in the pleurae. Another hypothesis for the poorer survival seen with a right-sided disease could be the larger number of lung lobes resulting to a greater pleural surface area or the location of ductus thoracicus perhaps enhancing the tumor spread from this side, both of these theories resulting to a bigger tumor burden.
Limitations of the study
Our study has limitations shared by most registry studies, but coverage of the Finnish Cancer Registry is comprehensive [Citation15]. The quality and quantity of the data during treatment and staging collected in clinical reports are not as comprehensive as in the reports from tumor pathological laboratories. We, therefore, assumed that patients who did not have a clinical report available had not received therapy. Additionally, the Finnish Cancer Registry does not collect data regarding performance status but as a best available estimation, we have used age on survival analyses trying to minimize the effect of missing performance status. However, the size of our study cohort was relatively big in view of the rarity of the disease, and it also included MPM cases for the entire country during the study period, giving insight into treatment protocols at a national level and beyond the parameters of the study.
Conclusions
This study is one of the few nationwide descriptive epidemiologic studies on MPM in the 21st century. The main findings were that female patients were older at the time of diagnosis and had fewer workers’ compensation claims. Also, there were less claims in regions where mesothelioma incidence was lower, indicating that the evaluation process is not nationally uniform. This was also supported by the marked heterogeneity in treatment. Awareness of the disease and its occupational etiology probably still needs to be increased among those taking care of these patients, although the use of asbestos has been discontinued in most developed countries. We were unable to show beneficial effects of the use of pemetrexed in our study setting.
Disclosure of interest
No potential conflict of interest was reported by the authors.
Acknowledgments
Data collected and maintained by the Finnish Cancer Registry and the National Workers’ Compensation Center Registry made this study possible. We thank Yvonne Sundström for secretarial assistance.
Additional information
Funding
References
- van Meerbeeck JP, Damhuis R. Facts, rumours and speculations about the mesothelioma epidemic. Respirology. 2011;16:1018–1019.
- Roe OD, Stella GM. Malignant pleural mesothelioma: history, controversy and future of a manmade epidemic. Eur Respir Rev. 2015;24:115–131.
- Porpodis K, Zarogoulidis P, Boutsikou E, et al. Malignant pleural mesothelioma: current and future perspectives. J Thorac Dis. 2013;5:S397–S406.
- Robinson BW, Musk AW, Lake RA. Malignant mesothelioma. Lancet. 2005;366:397–408.
- Patel SC, Dowell JE. Modern management of malignant pleural mesothelioma. Lung Cancer (Auckl). 2016;7:63–72.
- Milano MT, Zhang H. Malignant pleural mesothelioma: a population-based study of survival. J Thorac Oncol. 2010;5:1841–1848.
- Robinson BWS, Lake RA. Medical progress: advances in malignant mesothelioma. N Engl J Med. 2005;353:1591–1603.
- McDonald JC, McDonald AD. The epidemiology of mesothelioma in historical context. Eur Respir J. 1996;9:1932–1942.
- Peto J, Decarli A, La Vecchia C, et al. The European mesothelioma epidemic. Br J Cancer. 1999;79:666–672.
- Zhang W, Wu X, Wu L, et al. Advances in the diagnosis, treatment and prognosis of malignant pleural mesothelioma. Ann Transl Med. 2015;3:182.
- Mott FE. Mesothelioma: a review. Ochsner J. 2012;12:70–79.
- Sauli N. President of the Rebuplic, Laura Räty, Minister of Social Affairs and Health. Työtapaturma- ja ammattitautilaki; [cited April 24, 2018]. Available from: http://www.finlex.fi/fi/laki/alkup/2015/20150459
- Ilkka K. Minister of Labour, Matti Kajantie SI. Valtioneuvoston päätös asbestin ja asbestipitoisen tuotteen valmistuksen, maahantuonnin, myymisen ja käyttöön ottamisen kieltämisestä; [cited April 24, 2018]. Available from: http://www.finlex.fi/fi/laki/alkup/1992/19920852
- Ilkka K. Minister of Labour, Matti Kajantie SI. Valtioneuvoston päätös asbestin ja asbestipitoisen tuotteen valmistuksen, maahantuonnin, myymisen ja käyttöön ottamisen kieltämisestä annetun valtioneuvoston päätöksen muuttamisesta; [cited April 24, 2018]. Available from: http://www.finlex.fi/fi/laki/alkup/1993/19931133
- Leinonen MK, Miettinen J, Heikkinen S, et al. Quality measures of the population-based finnish cancer registry indicate sound data quality for solid malignant tumours. Eur J Cancer. 2017;77:31–39.
- Statistics Finland. Statistics finland's PX-web databases: population according to age (1-year) and sex by area 1972–2016; [cited April 24, 2018]. Available from: http://pxnet2.stat.fi/PXWeb/pxweb/en/StatFin/StatFin__vrm__vaerak/058_vaerak_tau_104.px/?rxid=146981e6-8fc8-40bc-bac8-a6320e704ff2
- Population Register Centre. Population information system; [cited April 24, 2018]. Available from: http://vrk.fi/en/population-information-system
- Finnish Medicines Agency (Fimea). Databases and registers, FimeaWeb, pemetrexed; [cited 2017]. Available from: http://www.fimea.fi/web/en/databases_and_registeries/fimeaweb
- Corfiati M, Scarselli A, Binazzi A, et al. Epidemiological patterns of asbestos exposure and spatial clusters of incident cases of malignant mesothelioma from the Italian National Registry. BMC Cancer. 2015;15:1–14.
- Montanaro F, Bray F, Gennaro V, et al. Pleural mesothelioma incidence in Europe: evidence of some deceleration in the increasing trends. Cancer Causes Control. 2003;14:791–803.
- Neumann V, Loseke S, Nowak D, et al. Malignant pleural mesothelioma: incidence, etiology, diagnosis, treatment, and occupational health. Dtsch Arztebl Int. 2013;110:319–326.
- Helland A, Solberg S, Brustugun OT. Incidence and survival of malignant pleural mesothelioma in Norway: a population-based study of 1686 cases. J Thorac Oncol. 2012;7:1858–1861.
- Jennings CJ, Walsh PM, Deady S, et al. Malignant pleural mesothelioma incidence and survival in the republic of Ireland 1994-2009. Cancer Epidemiol. 2014;38:35–41.
- Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21:2636–2644.
- Shukuya T, Takahashi T, Imai H, et al. Comparison of cisplatin plus pemetrexed and cisplatin plus gemcitabine for the treatment of malignant pleural mesothelioma in Japanese patients. Respir Investig. 2014;52:101–106.
- Flores RM, Zakowski M, Venkatraman E, et al. Prognostic factors in the treatment of malignant pleural mesothelioma at a large tertiary referral center. J Thorac Oncol. 2007;2:957–965.
- Ak G, Metintas S, Metintas M, et al. Prognostic factors according to the treatment schedule in malignant pleural mesothelioma. J Thorac Oncol. 2009;4:1425–1430.