
Abstract
Background: Previous studies indicate that visual size estimation (in situ) of polyp size tends to differ from postfixation measurements, which effects allocation to surveillance intervals. Little is known about interobserver variation of in-situ measurements of large polyps. The primary objective was to assess interobserver variation of in situ measurements of large colorectal polyps. Secondary objectives were the agreement of in situ measurements with postfixation measurements, and the agreement on detection of ≥20 mm polyps between these measurements.
Material and methods: Interobserver variability of in situ polyp size measurements was assessed between a diagnostic colonoscopy and the secondary therapeutic colonoscopy by dedicated endoscopists, in patients that were referred for an advanced polypectomy. After excision pre- and postfixation polyp sizes were measured with a ruler in three dimensions.
Results: A total of 40 patients, with 45 polyps, were included in the study. The average difference between the two in situ measurements was 2.4 mm (95% confidence interval (CI): −0.4–5.2). The differences between the first in situ, second in situ and pre-fixation measurement in comparison to postfixation measurements were 1.8 mm (95% CI: −1.2–4.9), 0.1 mm (95% CI: −1.5–1.8) and 1.0 mm (95% CI: −0.2–2.2). Cohen’s Kappa on detection of ≥20 mm polyps in agreement with postfixation measurements was 0.65 in the primary and 0.88 in the secondary in situ measurements.
Conclusion: This study shows a variation between in situ size measurements of large polyps. Improvements in daily clinical routines can be made by using an instrument to compare polyp size with and refraining from rounding sizes up or down. A randomized controlled trial assessing which instruments should be used for in-situ measurements of large polyps is warranted, in order to optimize size measurements of large colorectal polyps.
Introduction
The majority of colorectal cancers are thought to arise in benign adenomatous polyps [Citation1,Citation2]. In screening and routine clinical practice the number, size and histology of colorectal polyps determines treatment and surveillance interval [Citation3]. Previous studies assessing the quality of in-situ measurements found that these measurements are generally larger than postfixation measurements [Citation4–7]. In a large retrospective study 46% of the polyps with an in situ size of over 1 cm had a size of less than 1 cm in postfixation measurements [Citation8]. Eichenseer et al. [Citation9] investigated the consequences of these inconsistent measurements with respect to the timing of surveillance colonoscopy in polyps with in-situ sizes between 10 and 25 mm. In 63% of these polyps, a size-difference of at least 33% was detected between in situ and postfixation measurements, leading to inappropriate surveillance recommendations in over a third of the cases, regardless of histology and the number of detected polyps. Multiple studies show that in situ measurements differ significantly from postfixation measurements, but there are few studies assessing interobserver variation of in-situ measurements [Citation10–13]. Most of these interobserver studies have been performed in colon models [Citation11,Citation12] or on video fragments [Citation10,Citation13] and do not specifically address large polyps. Since the proportion of advanced histology increases rapidly with increasing polyp sizes [Citation14], an evaluation of in-situ measurements of large polyps is warranted. The objective of this study is to assess the interobserver variation by comparing in situ measurements of large polyps in two consecutive colonoscopies. The secondary objectives were agreement of in situ measurements with post-fixation measurements, and agreement on detection of ≥20 mm polyps between all measurements.
Material and methods
Study design
This prospective interobserver study assesses the reproducibility of in-situ polyp size measurements as well as the accuracy in comparison to post-fixation measurements of polyp size. Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) is the recommended treatment for polyps with a basis larger than 1.5 cm in our center. All patients referred for an advanced polypectomy (EMR or ESD) are therefore expected to have large colorectal polyps.
Study population
All patients referred to Odense University Hospital for advanced polypectomies were invited to participate in this study. Their primary colonoscopies were performed in our colonoscopy unit in either Nyborg or Svendborg, Denmark. In case of multiple polyps, the two largest were included for each patient. Exclusion criteria were piecemeal resection with over three pieces and multiple polyps at the same location.
Size measurements
In situ measurements during the first colonoscopy were performed by trainees and surgeons, who estimated the largest diameter. These physicians were not informed of this study, in order to obtain a real-life assessment of in-situ measurements. In the second colonoscopy dedicated endoscopists (NB, TK, GB) each with over 10 years colonoscopy experience, used an instrument to compare polyp size with. Prefixation measurements were carried out by pinning the polyps on Styrofoam and subsequently measuring size in three dimensions with a ruler. Postfixation measurements were carried out by a pathologist who measured all polyps in three dimensions.
Data collection
Data on patient demographics and the first colonoscopy was retrospectively collected from the electronic patient journal including age, sex, indication for colonoscopy, number of detected polyps, localization and morphology of the polyps as well as in-situ size measurements. Polyp localization, size measurements, morphology and subsequent histologic assessments of the second colonoscopy were collected prospectively.
Statistics
This study was planned as a pilot-study and aimed to include 30 patients. Due to the number of patients with incomplete data and/or piecemeal resection 40 patients were included. Basic characteristics are presented as means with standard deviations for continuous variables and percentages for binary and ordinal variables. Interobserver agreement between the different size measurements was determined by Bland-Altman graphs, determining the 95% limits of agreement of each comparison. Significance of agreement between the size measurements was calculated with a two-sided paired t-test. Mean differences were assessed by endoscopy experience with a one-way ANOVA. Agreement on detection of ≥20 mm polyps between the size measurements was determined by Cohen’s Kappa. Statistical analyses were performed using Stata IC 15.0 (StataCorp, College Station, TX, USA).
Ethics
The ethics committee was informed of this study but not required to give their permission due to the noninvasive nature of this study. The data protection agency gave their consent (case nr: 16/14701). The study was registered with the Odense Patient data Explorative Network, as project number 274 ‘The value of polyp size in colorectal cancer screening’. All patients received written information on the study and were given the opportunity to talk to the primary investigator. All patients signed an informed consent form before entering the study and could withdraw from the study at any time without consequences.
Results
Fifty patients gave consent, of which 10 were excluded due to multipiecemeal resections or multiple polyps in the same location. Forty patients with a total of 45 polyps were enrolled between July 1st 2016 and December 31st 2016. The primary colonoscopy was performed by trainees (20%), surgeons (62.5%) and colorectal surgeons (17.5%). Data of the primary colonoscopy were missing on size (n = 9) and morphology (n = 4). Nine piecemeal resections were performed and the pathologist received a total of 11 polyps in multiple pieces. All available size measurements were used in the analysis ().
Table 1. Demographics.
The average polyp sizes were 23.9 ± 9.3 mm and 21.1 ± 8.5 mm, in the primary (OC1) and secondary (OC2) colonoscopy. The pre- and post-fixation polyp sizes were 21.7 ± 8.5 mm and 19.3 ± 8.5 mm, respectively. The agreement between the different measurements expressed by limits of agreements is presented in and .
Figure 1. OC1 vs OC2 with 95% LA. On the left-hand side a scatter plot comparing in-situ measurements of both colonoscopies. On the right-hand side a Bland–Altman plot showing the differences between the measurements in comparison to the average of both measurements as well as 95% limits of agreement (horizontal lines on equal distance from the mean). OC1: primary optical colonoscopy. OC2: secondary optical colonoscopy. LA: limits of agreement.
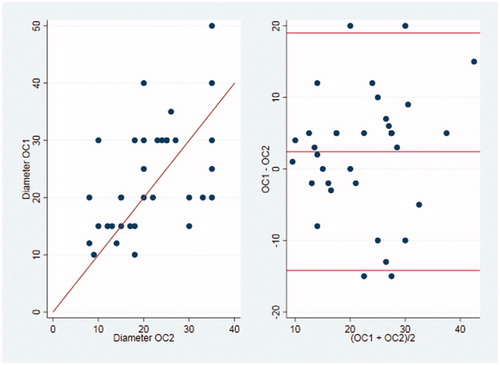
Table 2. Average difference between size measurements.
The variation between OC1 and OC2 was not-significantly affected by experience, as the mean difference was 4.2 mm in trainees, 2.2 mm in surgeons and 1.6 in colorectal surgeons (p = .2). Excluding the trainees from analysis did not affect analyses (data not shown).
A sub-analysis was performed to assess the agreement on large polyps (≥20 mm), using Cohen’s kappa (). The agreement on detection of ≥20 mm polyps between the dedicated endoscopists and postfixation measurement was good (Cohen’s Kappa: 0.88), and significantly higher than the agreement between the primary colonoscopy and postfixation measurement.
Table 3. Agreement on ≥20 mm polyp sizes.
Discussion
This pilot study indicates that dedicated endoscopists are superior to other physicians in determining in-situ polyp size of large polyps, because of smaller limits of agreements and a higher agreement to post-fixation sizes. The reduced variation of in situ measurements in the second colonoscopy is probably due to the combination of more experience as well as the use of instruments with known size when measuring in situ polyp size. The significant higher agreement on detection of ≥20 mm by dedicated endoscopists in comparison to postfixation size is relevant, since the Danish national guidelines regard polyps ≥2 cm as high-risk polyps that warrant a surveillance colonoscopy after 1 year instead of 3 years for ≥1 cm polyps [Citation15].
Although the variation in our study is large, the mean polyp sizes among the different measurements are not significantly different. This is unlike previous studies that tend to show either an overestimation [Citation8] or underestimation of polyp size [Citation11]. As Sakata [Citation17] presented this is likely be caused to rounding up and down to 5 mm in larger polyps. Since this study only included large polyps, rounding up or down might have attributed to evening out the mean differences as well as the general large variation in the differences in the primary colonoscopy.
The differences between pre- and postfixation sizes are larger than in the study of Turner et al. [Citation16], in which a difference of 0.3 mm (95% LA: −3.4–2.8) was shown in 107 polyps. This smaller difference could be explained by the inclusion of smaller polyps as well as a larger sample size in Turner’s study.
A strength of this study is that the polyp sizes are measured in repeat colonoscopies, which was possible due to referral for advanced polypectomies in our center. This unique set-up is likely to give a more realistic assessment of the variations in in-situ size measurement than assessment of a video or colon model, where multiple variables like dexterity of individual endoscopists and amount of inflation of the colon have been eliminated.
Both a limitation and strength of this study is that we retrieved the in-situ size measurement from the first colonoscopy from the patient file, without informing the primary endoscopists of this study. We have therefore no information on how polyp size was determined in the first colonoscopy. Not all primary endoscopists specified polyp size on referral for advanced polypectomy, which caused nine sizes to be missing.
Another limitation of this study is the small sample size, but even in this population a large variation in size estimations can be found that cannot be explained by a lack of experience since the majority of endoscopists were certified surgeons (80%).
Kim et al. investigated interobserver variability in 40 endoscopists (16 experts, 24 beginners) and found that the use of an open biopsy forceps increased the diagnostic accuracy in both experts and beginners [Citation10]. In polyps ≥10 mm the difference between true polyp size and visual estimation was 2.7 ± 0.8 mm and reduced to 2.4 ± 0.7 mm when using the biopsy forceps. An improvement of 0.3 mm might indicate that a biopsy forceps (that is usually less than 1 cm in width) is not an appropriate measuring tool for large polyps. Previous studies used polyps with an average size of less than 1 cm, and showed that comparison to an instrument of known size (for example biopsy forceps or snare) is likely to improve the quality of in situ estimations [Citation6,Citation7,Citation10,Citation18]. However, no specific instrument has been investigated in large colorectal polyps.
The consequences of estimating in situ size incorrectly are currently minor, due to the habit of removing all polyps. However, the in situ size does affect those patients who are referred for an advanced polypectomy due to size and location of the polyp. More accurate size estimation could decrease the amount of secondary colonoscopies with corresponding discomfort, risks of perforation and bleeding in these patients [Citation19]. Another group of patients that are affected by incorrect polyp sizes are those in which surveillance intervals are based on in situ polyp size [Citation9], especially because of piecemeal resections. Larger polyps are more likely to be treated with a piecemeal resection, which increases the importance of accurate in-situ size measurements of large colorectal polyps for surveillance recommendations.
This study shows a variation between in-situ colorectal polyp size measurements of large polyps, which might have consequences for referral for advanced polypectomies and surveillance. Improvements in daily clinical routines can be made by estimating the size of all referred polyps in the primary colonoscopy, the use of an instrument to compare polyp size with and refraining from rounding in-situ size up. In the near future artificial intelligence might also be used for assessing both histology and polyp size during endoscopy. This pilot study will be followed-up by new guidelines for measuring and reporting polyp size for polyps that are referred for advanced polypectomies. A randomized trial assessing which instruments should be used for in-situ measurements of large colorectal polyps is warranted, in order to optimize size measurements of large polyps.
References
- Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981.
- Winawer SJ. Natural history of colorectal cancer. Am J Med. 1999;106:3S–6S.
- Danske Regioners tvaerregionale implementeringsgruppe vedr. tarmkraeftscreening. Screenings- or adenomankontrol program for tyk- og endetarmskraeft - Guidelines for koloskopi og patologi. Copenhagen 2014. Danish.
- Schoen RE, Gerber LD, Margulies C. The pathologic measurement of polyp size is preferable to the endoscopic estimate. Gastrointest Endosc. 1997;46:492–496.
- Moug SJ, Vernall N, Saldanha J, et al. Endoscopists' estimation of size should not determine surveillance of colonic polyps. Colorectal Dis. 2009;12:646–650.
- Morales TG, Sampliner RE, Garewal HS, et al. The difference in colon polyp size before and after removal. Gastrointest Endosc. 1996;43:25–28.
- Gopalswamy N, Shenoy VN, Choudhry U, et al. Is in vivo measurement of size of polyps during colonoscopy accurate?. Gastrointest Endosc. 1997;46:497–502.
- Anderson BW, Smyrk TC, Anderson KS, et al. Endoscopic overestimation of colorectal polyp size. Gastrointest Endosc. 2016;83:201–208.
- Eichenseer PJ, Dhanekula R, Jakate S, et al. Endoscopic mis-sizing of polyps changes colorectal cancer surveillance recommendations. Dis Colon Rectum. 2013;56:315–321.
- Kim JH, Park SJ, Lee JH, et al. Is forceps more useful than visualization for measurement of colon polyp size? Wjg. 2016;22:3220–3226.
- Rubio CA, Hoog CM, Brostrom O, et al. Assessing the size of polyp phantoms in tandem colonoscopies. Anticancer Res. 2009;29:1539–1545.
- Kaz AM, Anwar A, O’Neill DR, et al. Use of a novel polyp “ruler snare” improves estimation of colon polyp size. Gastrointest Endosc. 2016;83:812–816.
- Aziz Aadam A, Wani S, Kahi C, et al. Physician assessment and management of complex colon polyps: a multicenter video-based survey study. Am J Gastroenterol. 2014;109:1312–1324.
- Lieberman D, Moravec M, Holub J, et al. Polyp size and advanced histology in patients undergoing colonoscopy screening: implications for CT colonography. Gastroenterology. 2008;135:1100–1105.
- Rasmussen M, Ingeholm P, Linnemann D, et al. Screenings- og adenomkontrol program for tyk- og endetarmskraeft [Screening and adenoma control program for colorectal cancer]. Copenhagen: Danish Regions; 2014. Danish.
- Turner JK, Wright M, Morgan M, et al. A prospective study of the accuracy and concordance between in-situ and postfixation measurements of colorectal polyp size and their potential impact upon surveillance. Eur J Gastroenterol Hepatol. 2013;25:562–567.
- Sakata S, Klein K, Stevenson ARL, et al. Measurement bias of polyp size at colonoscopy. Dis Colon Rectum. 2017;60:987–991.
- Jin HY, Leng Q. Use of disposable graduated biopsy forceps improves accuracy of polyp size measurements during endoscopy. Wjg. 2015;21:623–628.
- Wilson AI, Saunders BP. New paradigms in polypectomy: resect and discard, diagnose and disregard. Gastrointest Endosc Clin N Am. 2015;25:287–302.