
Background
Several countries have reported a decline in cancer diagnoses during the COVID-19 pandemic [Citation1–7]. The European Cancer Organisation estimated that clinicians diagnosed 1.5 million fewer cancer patients in Europe than expected in the first year of the pandemic [Citation8]. In Denmark, we have previously reported a decline in cancer diagnoses during the first months of the pandemic in the spring of 2020 [Citation9]. COVID-19 infections, hospitalisations, and deaths as well as societal restrictions varied during the months of 2020 in Denmark (Supplementary Appendix 1). In Mid-March, a national lockdown of the whole society was implemented and resources in the health sector were reprioritized to release resources for COVID-19 patients [Citation10]. Cancer screening programs were kept open, but with lower attendance rates [Citation11]. Despite the re-allocation of healthcare resources, the capacity to care for individuals with acute and life-threatening conditions appears to have been largely upheld in Denmark during the pandemic. Still, some hospitals might not temporarily have been able to fully provide timely care for acute non-COVID-19 medical conditions, such as cancer [Citation12].
During summer 2020, the COVID-19 infection rate was low and restrictions were lifted gradually. However, in the late summer and early autumn, the COVID-19 rates increased again and even though several restrictions were resumed, a second wave of COVID-19 emerged in December 2020 and peaked in January 2021 [Citation13].
In this report, we examined the impact of the COVID-19 pandemic on cancer detection in Denmark during 2020, with the aim of estimating potential missing diagnoses and elucidating catch-up effects between the first and the second waves. We examined differences in incident diagnoses in 2020 according to cancer type, age, and gender, compared with 2019. In addition, we evaluated differences in cancer stage distribution.
Material and methods
The National Patient Register covering the entire Danish population was used to identify the number of new cancer diagnoses during the COVID-19 pandemic from March to December 2020 and in the corresponding period in 2019. All cancer diagnoses at in- and outpatient hospital settings are recorded in the Patient Register and the register has been the primary source of the Danish Cancer Registry since 2004 [Citation14]. The Cancer Registry is also linked to the Danish Pathology Register for validation [Citation15] and the Danish Register of Causes of Death [Citation16] to include cancer deaths that are not hospitalised (<1%). Thus, The Cancer Registry has a delay due to the validation process of 1–1.5 year. Therefore, we used the Patient Register for identification of cancer diagnoses in 2020 (and 2019) in the current study. Patients with cancer diagnoses before 2019 were excluded by linkage to the Cancer Registry, which has recorded almost complete nationwide information on cancer incidence since 1943 [Citation14].
We defined ‘all cancer’ as ‘malignant neoplasms’ (except ‘non-melanoma skin cancer’), ‘polycythaemia vera’, and ‘myelodysplastic syndromes’ (ICD10 codes: C00–C96 and D45–47, except C44). The cancers were divided according to the ICD10 code into seven categories: female breast cancer, prostate cancer, colon cancer, lung cancer, brain cancer, melanoma skin cancer, and other cancers (see Supplementary Appendix 2). The patients were categorised into three age groups (<50 years; 50–69 years, and 70+ years) according to assumed age-related risk of severe COVID-19 infection, and by sex.
Numbers of incident cancer diagnoses were identified for each month, quarterly, and for the entire period March to December 2020 and compared to the corresponding numbers in 2019. Percentage change (PC) was calculated as the difference in first diagnosed cancer between 2020 and 2019 divided by the corresponding numbers in 2019. Ninety-five percent confidence intervals (CI) for the PC were estimated from a Poisson regression model for each month including a year as covariates, where the resulting rate ratio (RR) is a direct transformation of the percentage change (PC = [RR − 1]*100) assuming same population size at risk for 2020 and 2019 [Citation17].
For assessment of cancer stage, we used Tumour Node Metastasis (TNM) records in the Patient Register [Citation18]. Cancers were divided into three categories: ‘localised’, ‘non-localised’, or ‘unknown’ stage (Supplementary Appendix 3). The highest registered stage within four months from the first hospital contact was selected. The stage distribution was calculated in percent for all cancers, as well as for cancers of the breast, colon, prostate, and lung.
Legal approval to use data was obtained from The Danish Health Data Authority. Ethical review is not required for registry-based studies in Denmark. Statistical software SAS version 9.4 was used for data handling and analyses.
Results
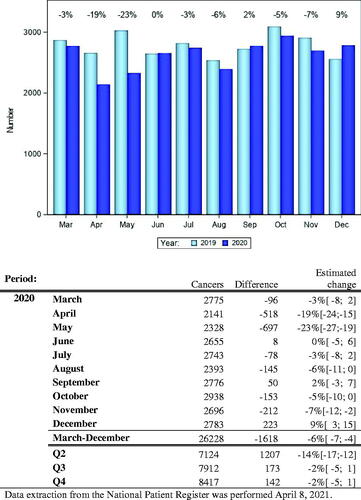
shows the number of new cancer diagnoses per month for 2019 and 2020 and the difference between the two years in percent for the study periods (March-December). We found a substantial reduction in new cancer diagnoses of 19% [95% CI 15–24] in April and 23% [95% CI 19–27] in May and a slight increase of 9%[95% CI 3–15] in December. Stratification into quarters yielded a reduction in new cancer diagnoses of 14% [95% CI 12–17] in Q2, whereas only a slight reduction of 2% was seen in both Q3 and Q4 [95% CI −1–5] compared with 2019. For the total period (March-December 2020) we observed a decline in new cancer diagnoses of 6% [95% CI 4–7] compared with the same period in 2019 ().
Figure 1. Incident cancer diagnosis during the COVID-19 pandemic in Denmark 2020.
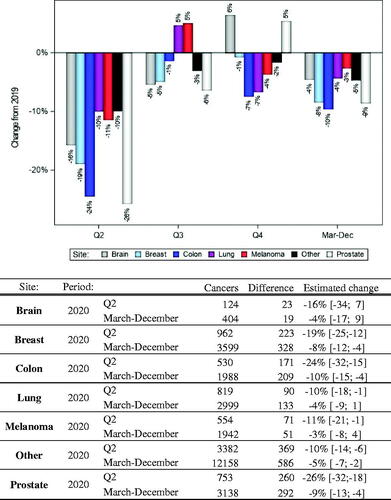
The reduction in cancer diagnoses in Q2 2020 was most pronounced for prostate cancer [26%; 95% CI 18–32], colon cancer [24%; 95% CI 15–32], and breast cancer [19%; 95% CI 12–25]. For lung cancer, melanoma, and other cancers we found reductions around 10%, and for brain cancer 16%. For the total period, March to December 2020, we found slight reductions for all seven cancer categories compared to 2019 with the most pronounced effects for prostate cancer, colon cancer, and breast cancer ().
Figure 2. Change in cancer diagnoses in Q2 to Q4 2020 according to the type of cancer.
The reduction in cancer diagnoses in Q2 2020 was evident in all three age groups and with almost similar magnitude. For the entire period, March to December 2020, we also observed reductions in all three age groups, the largest in the age group 50–69 years (8%) (see Supplementary Appendix 4).
No material differences in cancer diagnoses were seen according to gender (Supplementary Appendix 5).
We observed no substantial differences in the distribution of localised and non-localised cancer diagnoses between 2020 and 2019 (Supplementary Appendix 6). For colon, lung, and prostate cancer, we found small increases in non-localised stage in August 2020 of about 8–9% and for colon also in September 2020. For the other months, the stage distribution in 2020 exhibited the same pattern as 2019 for the four selected cancer types (Supplementary Appendix 7).
Discussion
Based on registrations in the Patient Register, we observed an overall reduction in the number of new cancer diagnoses of 6% in March-December 2020 compared to the same period in 2019. This corresponds to about 1600 fewer cancer diagnoses in the period affected by the COVID-19 pandemic.
As the population in Denmark ages [Citation19], cancer incidence increases with annually about 2% additional cases diagnosed [Citation20]. A small increase in cancer incidence from 2019 to 2020 would thus be expected, and consequently, our estimates of a reduction in cancer diagnoses in 2020 can be assumed to represent an, albeit modest, underestimate.
The overall reduction in new cancer diagnoses in March–December 2020 derived primarily from a substantial reduction in the number of cancer diagnoses in April and May 2020. We did not observe a corresponding increase in the number of new cancer diagnoses during summer 2020, which may indicate that several undetected cancer diagnoses in spring 2020 were not subsequently identified. The even level in new cancer diagnoses during summer 2020 compared to 2019 might also result from a mixture of undetected cancer diagnoses from the spring and continued reduced cancer detection due to reluctance to contact the doctor under a pandemic. In contrast, we did not observe any reductions in cancer diagnoses in December 2020, but a slight increase through the second wave of the COVID-19 pandemic was starting at that time. This observation might be related to the increased experience with handling COVID-19 in the health care sector and a shift in the communication to the public that handling of other acute diseases, such as cancer, cannot be postponed and people should seek medical attention when experiencing symptoms of, e.g., cancer.
In our previous analysis [Citation9], we reported a reduction of one-third in new cancer diagnoses during the first three months of the COVID-19 pandemic in Denmark (March–May 2020) based on data extracted ultimo July 2020. The present analysis, based on data extraction from primo April 2021, confirms a reduction in new cancer diagnoses in the spring of 2020, albeit less pronounced. This indicates that the various COVID-19 mitigation efforts also affected the cancer reporting to the Patient Register, with a longer delay in the final registration than usual for this register.
In January 2019, the Danish Health and Medicines Authority (DHMA) launched a new registration system for the Patient Register (LPR3). In the initial phase of the LPR3 registration, there were challenges with the data quality and coverage. However, a report by the DHMA in July 2020 stated that the data quality and degree of completeness of LPR3 has reached the same level as in the preceding patient register, LPR2 [Citation21]. Still, in January and February 2019, substantially fewer cancer diagnoses were registered in the LPR3 than expected, presumably due to conversion issues. In consequence, as Denmark was not affected by the COVID-19 pandemic in January–February 2020, we omitted these two months in our analyses. Since 2020 cancer data were not available in the Danish Cancer Registry for this report, we used The Patient Register for our analyses. Alternatively, we could have used the Pathology Register, however, this would exclude cancer diagnoses that were not histologically verified, and potentially underestimate the impact of the COVID-19 pandemic on diagnoses of, e.g., haematologic malignancies, prostate cancer, and brain tumours.
Even though there was a substantial reduction in the diagnosis of incident cancers in the spring of 2020 we did not observe any substantial stage migration towards advanced cancer diagnoses in the latter half of 2020. This could be due to several reasons. First, our categorisation into localised and non-localised diseases might have been too crude to detect a smaller increase in the cancer stage. Second, the patients with delayed cancer diagnoses in April and May 2020 would most likely have been diagnosed with cancer over several months in the latter half of 2020, which would diminish differences per month. Third, at the end of 2020 not all undetected cancers from the spring were identified and will therefore not be evident in our data period.
A recent study of cancer detection in Belgium based on pathology reports showed a similar pattern as our study for Denmark, with a 44% reduction in April 2020 compared with 2019 during the first COVID-19 wave. The cumulated reduction in cancer diagnoses in 2020 was estimated to be 6% or about 4000 diagnoses outstanding for 2020 [Citation22].
During the COVID-19 pandemic, Denmark experienced a substantial reduction in the number of new cancer diagnoses in the spring of 2020. In the entire period affected by the pandemic (March–December 2020), we observed 6% fewer cancer diagnoses compared to the same period in 2019, corresponding to about 1600 undetected cancer cases. Following the reduction in cancer diagnoses in spring 2020, no ensuing increase in the number of cancer diagnoses was observed in the remaining period of 2020, indicating that there may still be individuals having undetected cancer for longer periods, notably for prostate, colon, and breast cancer. We found no firm evidence of drift in cancer diagnoses towards more advanced stages during the pandemic, however, this needs further evaluation in future studies.
Supplemental Material
Download MS Word (361 KB)Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
References
- Dinmohamed AG, Visser O, Verhoeven RHA, et al. Fewer cancer diagnoses during the COVID-19 epidemic in The Netherlands. Lancet Oncol. 2020;21(6):750–751.
- Maringe C, Spicer J, Morris M, et al. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study. Lancet Oncol. 2020;21(8):1023–1034.
- Kaufman HW, Chen Z, Niles J, et al. Changes in the number of US patients with newly identified cancer before and during the coronavirus disease 2019 (COVID-19) pandemic. JAMA Netw Open. 2020;3(8):e2017267.
- Uppskjuten cancervård, Jämförelse av antalet nyregistrerade cancerfall under covid-19-pandemin 2020 och motsvarande period 2019; 2020. Fastställd av Regionala cancercentrumi samverkan.
- Northern Ireland pathology reports. Available from: https://www.qub.ac.uk/research-centres/nicr/FileStore/PDF/Covid19/Filetoupload,986705,en.pdf
- Lai AG, Pasea L, Banerjee A, et al. Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: near real-time data on cancer care, cancer deaths and a population-based cohort study. BMJ Open. 2020;10(11):e043828.
- Kempf E, Lamé G, Layese R, et al. New cancer cases at the time of SARS-Cov2 pandemic and related public health policies: a persistent and concerning decrease long after the end of the national lockdown. Eur J Cancer. 2021;150:260–267.
- Lawler M. Impact of COVID-19 on cancer. Chair in Translational Cancer Genomics at Queen's University Belfast.
- Skovlund CW, Friis S, Dehlendorff C, et al. Hidden morbidities: drop in cancer diagnoses during the COVID-19 pandemic in Denmark. Acta Oncol. 2021;60(1):20–23.
- Danish Health Authorities. Notat om reduktion af hospitalsaktivitet ifm COVID-19; 2020. Available from: https://www.sst.dk/da/Udgivelser/2020/Notat-om-reduktion-af-hospitalsaktivitet-i-forbindelse-med-COVID-19
- Danish Health Authorities. COVID-19: Monitorering af aktivitet i sundhedsvaesenet Beskrivelse af udviklingen i aktivitet i sundhedsvaesenet under COVID-19 epidemien – 10. Rapport; 2021. Available from: https://www.sst.dk/-/media/Udgivelser/2020/Corona/Monitorering/10_-monitoreringsrapport.ashx?la=da&hash=BB8C063DE9C55189F3A1191C12A0570E2620C6C4
- Bodilsen J, Nielsen PB, Søgaard M, et al. Hospital admission and mortality rates for non-covid diseases in Denmark during covid-19 pandemic: nationwide population based cohort study. BMJ. 2021;373:n1135.
- Statens Serums Institut. Available from: https://covid19.ssi.dk/overvagningsdata/download-fil-med-overvaagningdata. Data-Epidemiologiske-Rapport-31122020-4ho2
- Gjerstorff ML. The Danish Cancer Registry. Scand J Public Health. 2011;39(7 Suppl):42–45.
- Bjerregaard B, Larsen OB. The Danish Pathology Register. Scand J Public Health. 2011;39(7 Suppl):72–74.
- Helweg-Larsen K. The Danish Register of causes of death. Scand J Public Health. 2011;39(7 Suppl):26–29.
- Clayton D, Hills M. Statistical models in epidemiology. New York (NY): Oxford University Press; 1993.
- Schmidt M, Schmidt SAJ, Sandegaard JL, et al. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490.
- Danmarks Statistik, Statistikbanken befolkningspyramide; 2021. Available from: http://extranet.dst.dk/pyramide/pyramide.htm#!y=2019&v=2&o=2020
- Sundhedsdatastyrelsen, Nye kraefttilfaelde i Danmark 2019; 2021. Available from: https://sundhedsdatastyrelsen.dk/da/tal-og-analyser/analyser-og-rapporter/sygdomme/kraeft-_-nyetilfaelde (Table 8).
- Sundhedsdatastyrelsen, LPR3 datakvalitetsrapport; 2020. Available from: https://sundhedsdatastyrelsen.dk/da/registre-og-services/om-de-nationale-sundhedsregistre/sygedomme-laegemidler-og-behandlinger/landspatientregisteret/landspatientregisteret-moderniseres
- Peacock HM, Tambuyzer T, Verdoodt F, et al. Decline and incomplete recovery in cancer diagnoses during the COVID-19 pandemic in Belgium: a year-long, population-level analysis. ESMO Open. 2021;6(4):100197.