
Abstract
Introduction
Esophageal cancer (EC) makes up 3.2% of all cancers but ranks sixth among cancer-related deaths worldwide. This real-world analysis determined the use of PD-1/PD-L1 (PD[L]1) inhibitors in EC patients after receiving first-line therapy.
Methods
Newly diagnosed EC patients initiating first-line treatment were identified in the IBM MarketScan administrative claims databases during the study period (1 May 2015 to 31 October 2020) using ICD-9/ICD-10 codes. Patients were assigned to either the chemotherapy only, radiation only, chemotherapy plus radiation (chemoradiation), or esophageal transhiatal/transthoracic surgery cohorts.
Results
7276 EC patients started first-line therapy (chemotherapy only = 2502, radiation only = 3355, chemoradiation = 1180, surgery = 239). The average age at diagnosis was 62 years and 23% were female. The median time from start of first-line therapy to utilization of a PD(L)1 inhibitor was 259 days. Pembrolizumab (72%) was the most frequently used PD(L)1 inhibitor across the three cohorts, followed by nivolumab (25%). Furthermore, the number of patients receiving a PD(L)1 inhibitor increased each year with the majority (73%) of use occurring between 2018 and 2020.
Discussion
Findings from this real-world study suggest that PD(L)1 inhibitors are increasingly used after first-line therapies in EC, especially among patients initially receiving chemotherapy only. New immunological therapies such as PD(L)1 inhibitors hold great promise for patients with solid tumors. A clearer understanding of their real-world utilization is critical.
1. Introduction
Esophageal cancer (EC), which includes esophageal squamous cell carcinoma and esophageal adenocarcinoma, makes up only 3.2% of all cancers but ranks as the seventh most common cancer and sixth among cancer-related deaths worldwideCitation1. EC includes both adenocarcinoma, which is the most common histologic type in the United States (US), and esophageal squamous cell carcinoma, which represents 90% of all cases worldwideCitation2. The overall burden of disease associated with EC varies widely within different geographies, with the burden resting disproportionately on developing countriesCitation3. However, the incidence of EC in the US has risen over the last 20 years, with an estimated 18,440 new cases and 16,170 deaths in 2020Citation4.
Overall, the age-standardized incidence of EC is higher among men than women (9.3 versus 3.5 per 100,000 worldwide; 5.6 versus 1.2 per 100,000 in North America)Citation1. Furthermore, specific factors that cause irritation in the cells of the esophagus have been found to increase the risk of EC, with higher rates attributed to tobacco and alcohol use, specific nutritional habits (e.g. consumption of processed meat; low consumption of fruits and vegetables), and gastroesophageal reflux diseaseCitation5,Citation6. In the US, the direct economic burden of EC was estimated at $1.7 billion for 2018, and patient-specific costs vary widely by histology, stage, and treatmentCitation7,Citation8.
If diagnosed early, the standard curative option for most patients with locally advanced EC is esophagectomy, often preceded by neoadjuvant therapyCitation9. However, surgical resection is challenging because of the close proximity to vital structures and is associated with a high rate of recurrence and postoperative complications, as well as decreased health-related quality of life (HRQoL) following surgeryCitation10,Citation11. More recently, minimally invasive techniques using thoracoscopic and/or laparoscopic approaches have been introduced to minimize complications and enhance postoperative recoveryCitation12. A meta-analysis reported that minimally invasive surgery is generally followed by better postoperative outcomes, including physical function, pain, and HRQoL, for up to 3 months as compared to open esophagectomy, although these differences failed to persist over the longer termCitation13.
Due to the lack of specific symptoms in early EC, most tumors are diagnosed late and rapidly progress to an advanced stage. At the late stage, treatment options are limited, and the survival rate is lowCitation14,Citation15. Standard first-line nonsurgical treatments include chemotherapy, radiation therapy, or a combination of chemotherapy plus radiation (chemoradiation). Second-line treatments for advanced disease include targeted therapies for human epidermal growth factor receptor 2 (HER2) positive disease and monoclonal antibodies that bind to the vascular endothelial growth factor (VEGF) receptor.
More recently, immunotherapy has emerged as a promising therapeutic approach for EC that targets checkpoint proteins and helps restore immune response against cancer cellsCitation16. Targets of current immune checkpoint inhibitors include programmed cell death protein 1 (PD-1) receptors found on the surface of T cells and B cells and PD-1 ligands 1 and 2 (PD-L1 and PD-L2), which are expressed in many solid tumorsCitation16. The primary role of the PD-1 and PD-L1 system, henceforth referred to collectively as PD(L)1 inhibitors, is to limit the response of T cells and thus limit immune-mediated tissue damage. Several PD(L)1 inhibitors are used to treat patients with EC, typically for refractory disease. In the US, pembrolizumabCitation17 and nivolumabCitation18 are currently approved for the treatment of patients with recurrent, advanced, or metastatic esophageal squamous cell carcinoma after prior therapy. Clinical trials have reported that PD(L)1 inhibitors are associated with improved outcomes in patients with advanced ECCitation19–21.
An increased emphasis on screening programs for EC has the potential to shift stage distribution and thus treatment patterns, since patients diagnosed earlier have more treatment options availableCitation8. Therefore, timely examinations of current treatment patterns for EC, especially focused on new immunotherapies, are critical.
The overarching objective of this real-world claims analysis was to determine the use of PD(L)1 inhibitors following first-line therapy in EC patients. The analysis also sought to determine the proportion of EC patients that switch to PD(L)1 inhibitors after receiving first-line therapy and examine which specific PD(L)1 inhibitors are utilized in these patients.
2. Methods
2.1. Data source
This retrospective observational study utilized administrative claims data (1 February 2014 to 31 October 2019) from the IBM MarketScanFootnotei Research databases, which provide detailed cost, resource use, and outcomes data for the healthcare services performed in both inpatient and outpatient settings. The MarketScan Commercial Claims and Encounters database contains the inpatient, outpatient, and outpatient prescription drug experience of approximately 195 million employees and their dependents. The MarketScan Medicare Supplemental and Coordination of Benefits (COB) database contains the healthcare experience (both medical and pharmacy) of over 14 million retirees with Medicare supplemental insurance. Data are de-identified and comply with the patient confidentiality requirements of the Health Insurance Portability and Accountability Act (HIPAA). Institutional Review Board (IRB) approval was not required since individual patient data were not identifiable.
2.2. Patient selection and cohort creation
Newly diagnosed EC (including both adenocarcinoma and squamous cell carcinoma) patients were identified in the IBM MarketScan Commercial and Medicare Supplemental databases during the study period of 1 May 2015 (approval of first PD(L)1 inhibitor in the US) through 31 October 2020. Eligible patients met the following criteria: (a) at least one claim for EC (ICD-9-CM: 150.x; ICD-10-CM: c15.3, c15.4, c15.5, c15.8, c15.9) during the study period, (b) no previous EC claim prior to study period, (c) continuous enrollment at least 60 days prior to and 60 days after first EC claim, (d) began EC treatment with a first-line therapy, and ≥18 years of age.
Newly diagnosed patients were assigned to one of four patient cohorts based on the first-line therapy they received: chemotherapy only, radiation only, chemoradiation, or esophageal transhiatal/transthoracic surgery. The drug and procedure codes (J-codes and HCPCS) used to identify each of the cohorts are included in Table 1 of the Supplementary Appendix. After first-line therapy, the database was searched for the first claim for a PD(L)1 inhibitor (i.e. pembrolizumab, nivolumab, atezolizumab, avelumab, durvalumab, cemiplimab-rwlc). The exact PD(L)1 inhibitor that was used was then recorded. A complete list of drug names and procedure codes for the PD(L)1 inhibitors are included in Table 2 of the Supplementary Appendix.
2.3. Key variables and analytic approach
Descriptive analyses examined demographic characteristics such as age and sex. Time in days from initial diagnosis to first-line therapy (Time to First-Line) as well as time from first-line therapy to initiation of a PD(L)1 inhibitor (Time to PD(L)1 inhibitor) were both examined. The Charlson Comorbidity Index (CCI) was calculated over the 30 days prior to EC diagnosisCitation22. Differences between cohorts were tested using chi-square for categorical variables and t-tests for continuous variables. Additional descriptive analyses were conducted to examine PD(L)1 inhibitor utilization within each patient cohort.
3. Results
A total of 7276 newly diagnosed EC patients starting first-line therapy were identified. Overall, the average age of patients at date of diagnosis was 61.9 years (standard deviation [SD] = 11.3) and 23.0% of patients were female.
3.1. First-line therapy
Of the 7276 EC patients in total, 2502 received first-line chemotherapy only, 3355 received first-line radiation only, 1180 received first-line chemoradiation, and 239 underwent surgery first. provides the patient characteristics of the four cohorts. There was a significant difference in age across cohorts. Follow-up pairwise comparisons indicated that the radiation only cohort was significantly older than the other three cohorts and the chemoradiation cohort was also significantly older than the chemotherapy only cohort. The proportion of females was statistically similar across the four cohorts. A significant difference for the CCI score was observed where average comorbidities were the highest in the chemotherapy only cohort followed by the chemoradiation cohort. A significant main effect for time to first-line therapy was found. Post-hoc analyses indicated that the median number of days between first diagnosis and initiation of first-line therapy was significantly different between all the cohorts, with the exception of chemotherapy only and radiation only. The surgery cohort experienced the longest duration to initiation of first-line therapy
Table 1. Characteristics of EC patients by first-line therapy cohort (n = 7276).
3.2. Initiation of PD(L)1 inhibitor therapy
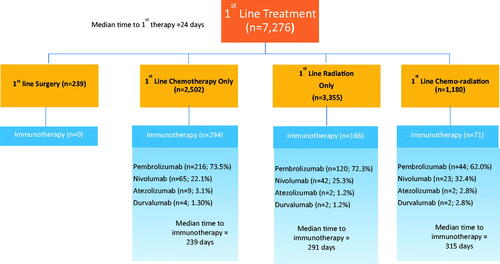
Of the total 7276 EC patients that began first-line therapy, 531 subsequently began therapy with a PD(L)1 inhibitor. The average age of these patients was 59.8 years (SD = 10.9) and 24% identified as female. Among them, 55.4% (294/531) of patients were from the first-line chemotherapy only cohort, 31.3% (166/531) of patients were from the first-line radiation only cohort, and 13.4% (71/531) of patients initially received chemoradiation as their first-line therapy. No patients from the first-line surgery cohort subsequently received a PD(L)1 inhibitor.
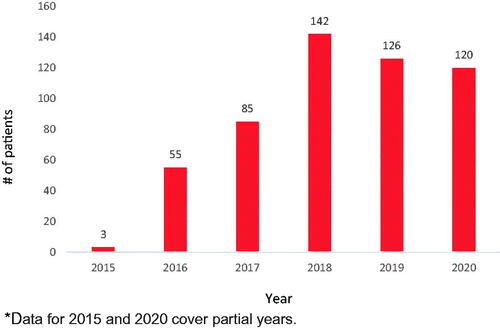
The median time from the start of first-line therapy to initiation of a PD(L)1 inhibitor was 259 days. The use of PD(L)1 inhibitors increased over the 5 years of the study period with 3 (1%) patients receiving PD(L)1 inhibitors in 2015, 55 (10.4%) in 2016, 85 (16.0%) in 2017, 142 (26.7%) in 2018, 126 (23.7%) in 2019, and 120 during the first 10 months of 2020 (22.6%) ().
Figure 1. Number of patients prescribed a PD(L)1 inhibitor over the study period. Data for 2015 and 2020 cover partial years.
provides a description of the PD(L)1 inhibitor subsample by first-line therapy cohort. There was a significant difference in mean age with patients in the radiation only cohort which was significantly older than the chemotherapy only cohort. The proportion of females was statistically similar across the four cohorts. Time from the start of first-line therapy to initiation of a PD(L)1 inhibitor was significantly shorter in the chemotherapy cohort relative to radiation only and chemoradiation cohorts.
Table 2. Characteristics of EC patients receiving a PD(L)1 by first-line therapy cohort (n = 531).
The specific PD(L)1 inhibitors that were utilized in each of the cohorts are presented in . Pembrolizumab (71.6%) was used most frequently across the three cohorts followed by nivolumab (24.5%), atezolizumab (2.4%), and durvalumab (1.5%). There was no evidence of avelumab or cemiplimab-rwlc use during the current study period.
Figure 2. Frequencies of EC patients receiving a PD(L)1 inhibitor by first-line therapy cohort (n = 531).
4. Discussion
To the best of our knowledge, the current study represents one of the first attempts to examine real-world patterns of PD(L)1 inhibitor utilization using US administrative claims data. Given the increasing incidence of EC and the associated high rate of mortality, this disease places a substantial burden on the healthcare system as well as the patient. Furthermore, increased emphasis on screening programs for EC has the potential to shift treatment patterns associated with earlier stage disease and improved survival. New immunological therapies such as PD(L)1 inhibitors hold great promise for patients with solid tumors and yet their real-world utilization has not been clearly defined.
The results of these analyses suggest that PD(L)1 inhibitors are increasingly used in EC after first-line therapies, especially among patients that initially received chemotherapy only (55%). Of the patients who received PD(L)1 inhibitors, a lower proportion received radiation only or combination chemoradiation as first-line therapy (31% and 13%, respectively). The current study did not examine survival of patients after first-line therapy, the number of patients that went on to receive other subsequent therapies, or what other treatment options may have been chosen. As such, additional research is needed to determine why some patients are not receiving a PD(L)1 inhibitor at later stages of therapy including the identification of patients that are not eligible to receive a PD(L)1 inhibitor.
One possible explanation why a higher proportion of first-line chemotherapy only patients received a PD(L)1 inhibitor is because pembrolizumab’s indication is for “disease progression after one or more prior lines of systemic therapy”, which may have limited commercial use of pembrolizumab in the radiation only cohort. It is not surprising that pembrolizumab was the most frequently used PD(L)1 inhibitor given that during the study timeframe of 2015–2020, it was the only PD(L)1 inhibitor approved in the US for the treatment of patients with recurrent locally advanced or metastatic squamous cell carcinoma of the esophagus. Nivolumab’s approval (June 2020) came after the timeframe of this study and therefore its current use in clinical settings could be higher.
The findings of this study also suggest a growth in the use of PD(L)1 inhibitors over the past 5 years. In fact, over 73% of the PD(L)1 inhibitor utilization occurred in the last 2 years. This growth in PD(L)1 inhibitor use reflects an increasing investment in health care resources for EC treatment in the US, which is a positive development given the high level of unmet medical needs in these patients.
Whereas the real-world results of this study provide important insight into PD(L)1 inhibitor use, they should be considered alongside several caveats. First, this exploratory analysis was based on retrospective administrative claims data, which lack clinical detail such as reasons for selection of therapy (including biomarkers) and the specific clinical response to therapy. Second, due to lack of granularity in ICD coding, distinctions could not be made between patients with adenocarcinoma and squamous cell carcinoma or between disease severity/stage. Third, given that data up to October 2020 is available, it is possible that more patients have received or will go on to receive a PD(L)1 inhibitor. Finally, this study was limited to only those individuals with commercial health coverage or private Medicare supplemental coverage. Consequently, results of this analysis may not be generalizable to EC patients with other insurance or without health insurance coverage, or patients outside the US.
5. Conclusions
The current study highlights that PD(L)1 inhibitor utilization in patients with EC has steadily grown in the US in recent years. Moreover, this growth is primarily in those EC patients that have undergone first-line chemotherapy and perhaps underutilized in patients that were treated at first-line with chemoradiation or radiation alone. Future real-world research should continue such timely examinations of current treatment patterns for EC, especially focusing on new immunotherapies, including exploring why the use of PD(L)1 inhibitors differ across patients and whether healthcare costs and utilization in patients that receive PD(L)1 inhibitor therapy differ compared to patients who do not. The current and continued growth of PD(L)1 inhibitor use reflects an increasing investment in health care resources for EC treatment in the US, which is a positive development given the high level of unmet medical needs in these patients.
Transparency
Declaration of funding
BeiGene, Ltd. funded the study and was responsible for the design, analysis, and reporting.
Declaration of financial/other relationships
JA has received consulting fees from BeiGene, Ltd.; MB, SA, HH, KY, GB, are employees of and own stock in BeiGene, Ltd. A reviewer on this manuscript has disclosed that they are a current employee and stockholder at Moderna Therapeutics, and have been, within the last 12 months, an employee and stockholder at GlaxoSmithKline. Peer reviewers on this manuscript have no other relevant financial relationships or otherwise to disclose.
Supplemental Material: Appendix
Download MS Word (19.2 KB)Acknowledgements
None.
Notes
i IBM MarketScan is a registered trademark of IBM Watson, Cambridge, MA, USA.
References
- Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today [Internet]. Lyon (France): International Agency for Research on Cancer. 2019 [cited 2019 Feb 27]. Available from: https://gco.iarc.fr/today.
- Wang Q-L, Xie S-H, Wahlin K, et al. Global time trends in the incidence of esophageal squamous cell carcinoma. Clin Epidemiol. 2018;10:717–728.
- Di Pardo BJ, Bronson NW, Diggs BS, et al. The global burden of esophageal cancer: a disability-adjusted life-year approach. World J Surg. 2016;40(2):395–401.
- Hur C, Miller M, Kong CY, et al. Trends in esophageal adenocarcinoma incidence and mortality. Cancer. 2013;119(6):1149–1158.
- Islami F, Goding Sauer A, Miller KD, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA: A Cancer Journal for Clinicians. 2018;68(1):31–54.
- World Cancer Research Fund International. American Institute for Cancer Research, Diet, Nutrition, Physical Activity and Cancer: a global perspective. The third expert report [Internet]. London (UK): WCRF. 2020 [cited 2020 Dec 11]. Available from: https://www.wcrf.org/dietandcancer
- National Cancer Institute. Cancer trends progress report: financial burden of cancer care [Internet]. Bethesda (MD): NCI. 2020 [cited 2020 Dec 11]. Available from: https://progressreport.cancer.gov/after/economic_burden
- Tramontano AC, Chen Y, Watson TR, et al. Esophageal cancer treatment costs by phase of care and treatment modality, 2000-2013. Cancer Med. 2019;8(11):5158–5172.
- Kauppila JH, Lagergren J. The surgical management of esophago-gastric junctional cancer. Surg Oncol. 2016;25(4):394–400.
- Jacobs M, Macefield RC, Elbers RG, et al. Meta-analysis shows clinically relevant and long-lasting deterioration in health-related quality of life after esophageal cancer surgery. Qual Life Res. 2014;23(4):1097–1115.
- Jiang R, Liu Y, Ward KC, et al. Excess cost and predictive factors of esophagectomy complications in the SEER-Medicare Database. Ann Thor Surg. 2018;106(5):1484–1491.
- Biere SS, van Berge Henegouwen MI, Maas KW, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet. 2012;379(9829):1887–1892.
- Kauppila JH, Xie S, Johar A, et al. Meta-analysis of health-related quality of life after minimally invasive versus open oesophagectomy for oesophageal cancer. Brit J Surg. 2017;104(9):1131–1140.
- Stat Facts (Esophageal Cancer). Surveillance research program [Internet]. Bethesda (MD): NCI. 2020 [cited 2020 Dec 11]. Available from: https://seer.cancer.gov/statfacts/html/
- Zhang Y. Epidemiology of esophageal cancer. World J Gastroenterol. 2013;19(34):5598–5606.
- Tanaka T, Nakamura J, Noshiro H. Promising immunotherapies for esophageal cancer. Expert Opin Biol Ther. 2017;17(6):723–733.
- KEYTRUDA® (pembrolizumab) injection, for intravenous use prescribing information [Internet]. Princeton (NJ): Bristol-Myers Squibb Company; 2020 [cited 2020 Dec 11]. Available from: https://www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf
- OPDIVO (nivolumab) injection, for intravenous use prescribing information [Internet]. Whitehouse Station (NJ): Merck & Co., Inc. 2020 [cited 2020 Dec 11]. Available from: https://packageinserts.bms.com/pi/pi_opdivo.pdf
- Chen K, Wang X, Yang L, et al. The anti-PD-1/PD-L1 immunotherapy for gastric esophageal cancer: a systematic review and meta-analysis and literature review. Cancer Control. 2021;28:107327482199743.
- Rogers JE, Xiao L, Trail A, et al. Nivolumab in combination with irinotecan and 5-fluorouracil (FOLFIRI) for refractory advanced gastroesophageal cancer. Oncology. 2020;98(5):289–294.
- Zayac A, Almhanna K. Esophageal, gastric cancer and immunotherapy: small steps in the right direction? Transl Gastroenterol Hepatol. 2020;5:9.
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson comorbidity index: ICD-9 update and ICD-10 translation. Am Health & Drug Benefits. 2019;12(4):188–197.