

Abstract
Objective
To assess the current status of shared decision making (SDM) in rheumatoid arthritis (RA) clinical practice in Japan from the perspectives of physicians and patients.
Methods
A web-based survey was conducted to recruit patients with RA who were prescribed, for the first time, a conventional synthetic disease-modifying antirheumatic drug (csDMARD) or a biological drug/Janus kinase (JAK) inhibitor, and physicians who prescribed these treatments to patients with RA. The SDM Questionnaire-Physician version (SDM-Q-Doc) and the 9-item SDM Questionnaire (SDM-Q-9) were used to assess the SDM levels of physicians and patients, respectively. The scale ranged from 0 to 100, and higher scores indicated better SDM status.
Results
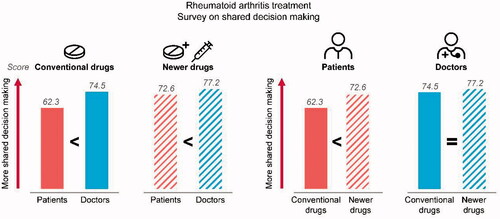
The responses from 107 physicians who treat patients with RA, 107 patients prescribed a csDMARD, and 110 patients prescribed a biological drug/JAK inhibitor were collected. The mean SDM score for SDM-Q-Doc was 74.5 when physicians decided to prescribe a csDMARD and 77.2 when they decided to prescribe a biological drug/JAK inhibitor. However, the mean SDM score for SDM-Q-9 was 62.3 when patients were prescribed csDMARDs and 72.6 when they were prescribed biological drugs/JAK inhibitors.
Conclusions
The results showed differences in SDM level between patients and physicians and, from the patient perspective, between treatment types.
PLAIN LANGUAGE SUMMARY
Rheumatoid arthritis (RA) is a long-term disease that causes swelling and pain, mainly in the joints of the hands and feet. Because RA cannot be cured, treatment usually continues for a long time. Shared decision making (SDM) involves people and their doctors deciding on the best treatment together. This study was done to understand how SDM is used for RA treatment in Japan. We sent one survey to 107 doctors who treat RA and a different survey to 217 people with RA. Each survey asked the doctors or the people with RA to score, on a scale of 0 to 100, how involved the person with RA was in making the decision on what treatment to use. A higher score meant more involvement in SDM. Doctors gave higher SDM scores than people with RA did, which meant doctors thought there was more SDM than what people with RA thought. This was true whether the person started treatment with a conventional RA drug or a newer RA drug (biological/JAK inhibitor). However, for both doctors and people with RA, the SDM scores were higher when a newer drug was used than when a conventional drug was used. This may be because the newer drugs are often prescribed for people with more severe RA or because there are more treatment types available. This was the first study to look at SDM in RA treatment in Japan. Increasing SDM will help improve treatment satisfaction in people with RA and increase patient-centered medical care.
Transparency
Declaration of funding
This study was funded by Eli Lilly Japan K.K.
Declaration of financial/other relationships
Hiroto Tsuboi has received speaking fees and/or honoraria from Eli Lilly Japan K.K. Yuko Kaneko has received grants or speaking fees from AbbVie GK, Astellas Pharma Inc., AYUMI Pharmaceutical Corporation, Bristol Myers Squibb K.K., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., Janssen Pharmaceutical K.K., Kissei Pharmaceutical Co., Ltd., Kyowa Kirin Co., Ltd., Novartis Pharma K.K., Pfizer Japan Inc., Sanofi K.K., Takeda Pharmaceutical Company Limited, Mitsubishi Tanabe Pharma Corporation, and UCB Japan Co. Ltd. Kei Ikeda has received speaking fee from Eli Lilly Japan K.K., AbbVie GK, Novartis Pharma K.K., Mitsubishi Tanabe Pharma Corporation, and Asahi Kasei Pharma Corporation and has received research grants from Mitsubishi Tanabe Pharma Corporation. Toshihiko Aranishi, Zhihong Cai, and Tomoko Ishizuka are full-time employees of Eli Lilly Japan K.K. and minor stockholders of Eli Lilly and Company. Toshihiko Aranishi is a stockholder of Chugai Pharmaceutical Co., Ltd.
A reviewer on this manuscript has disclosed that they have served as a consultant to Lilly but had no prior knowledge or involvement in the work being reviewed. Peer reviewers on this manuscript have no other relevant financial relationships or otherwise to disclose.
Author contributions
TA and ZC contributed to the study design, conception, analysis, interpretation of data, critical revision of draft and final approval. HT, YK, KI, and TI contributed to the data interpretation, critical revision of the draft, and final approval.
Acknowledgements
The authors would like to thank all patients and physicians for participating in this study, which helps us understand the current status of SDM in RA clinical practice in Japan. We are also grateful to the members of Social Survey Research Information Co., Ltd.; Tomoyuki Kusaka for the study design; Kohei Mizui for conducting the survey and the statistical analysis; Chie Kikutake for conducting the statistical analysis, supporting the interpretation of study results and drafting; and Sachiko Funabashi for the study design, supporting the interpretation of study results and drafting. Additional writing and editorial assistance were provided by Rebecca Lew, PhD, CMPP, and Jeanne Claypoole of ProScribe – Envision Pharma Group, funded by Eli Lilly Japan K.K.
Data availability statement
The raw data supporting the findings of this study are not available because consent was obtained from participants on the condition that it would not be disclosed to third parties.