
Abstract
Objective
To investigate the efficacy of direct computed tomography venography (CTV) in early and accurate detection of lower extremity venous (LEV) abnormalities.
Methods
Cross-sectional research was conducted in Hebei General Hospital of China. A total of 211 CTV reports of both lower extremities from January 2017 to September 2019, 75 color Doppler ultrasound (DUS) examinations, and eight intravascular angiography records of these patients over the same period were collected from the hospital. Comparisons were made for the reported number and percentage of LEV abnormalities (thrombosis, stenosis including severe stenosis, and varicosities). Chi-square test and t-test were applied to compare the rates and means, respectively. Significance level α was 0.05. Individual interviews were performed to understand the perceptions of medical staff and patients on the application of CTV, and the interview results were analyzed.
Results
Of the 75 cases with both CTV and DUS reports, 159 abnormalities occurring in the lower extremity deep veins (LEDV) were reported, among which 125 (79%) and 18 (11%) were reported by CTV and DUS on a single basis, respectively, whereas 16 (10%) were reported by CTV and DUS simultaneously. A statistically significant greater number of abnormalities in LEDV were identified by CTV than DUS in both males and females (χ2males = 78.449, χ2females = 27.574, χ2total = 104.164, p < .05). In the 211 CTV reports, among the 383 abnormalities reported in total, the common iliac vein (CIV) had the highest number of reported abnormalities (132, 34.5%), followed by the femoral vein (93, 24.3%). The ratios between LEDV abnormality and patient numbers were 1.055 and 0.688 for left and right sides in males, and 0.892 and 0.461 for left and right sides in females, respectively, with that for the left side statistically significantly higher than the right one (tmale = 2.896, tfemale = 4.347, p < .05). The incidence of thrombosis was 10.9% (95% CI = 6.7 ∼ 15.1%). Reported abnormities in CIV by CTV were in agreement with those by intravascular angiography. The medical staff believed that CTV could guide the performance of surgeries for LEV and the patients perceived CTV acceptable.
Conclusions
Application of CTV for early and accurate detection of LEDV abnormalities including thrombosis has been proven to be efficient. Corresponding benefit in early intervention and reduction of severe complications of such abnormalities is of important value. CTV earned good recognition from medical staff and patients. Hence, it could be considered as part of global health assistance cooperation with developing countries to facilitate enhanced medical services.
Background
Application of direct computed tomography venography (CTV) as a new examination technique for investigation of the venous system of both lower extremities has been reported in previous literature to be of positive significanceCitation1–4 in clinical practice, although such information is scarce. This technique is in its exploration stage and research trend in China, and has been proven to play a substantial role in clinical practice in ChinaCitation5–7. The technique has been found to function in different capacities: evaluation of lesions of the lower extremity’s venous system, diagnosis of venous obstructive diseases of the lower extremities, such as thrombosis, tumor compression, erosion, or local venous obstruction caused by trauma, varicose veins, and to visually evaluate the sites and overall extent of the lesions as well as the involvement of the their surrounding tissuesCitation8. In addition, this advanced technique has the capacity to capture and detect deep vein thrombosis in the pelvis and calf, which is not easily detected by color Doppler ultrasound (DUS). This would not only provide a detailed anatomical reference structure for clinical surgery, but also enable the detection of early thrombosis which can inform the clinical decision for either a surgery or a thrombolytic therapy.
Since October 2016, Hebei General Hospital of China has applied CTV in its clinical practice. As an innovative detection technique introduced by the hospital, a study was launched to provide an insight into the benefits accrued to its use in diagnosis of abnormalities in lower extremity venous (LEV) system. Specifically, the researchers collected all medical reports on bilateral-lower-extremity investigated with CTV, all available vascular color DUS examination and intravascular angiography records of the same patients in the same hospital during the same period which lasted for a period of 33 months since 2017. Also, an interview was granted to medical staff and patients on an individual basis to investigate respondents’ perception of CTV introduction, the efficiency of CTV in early and accurate detection of abnormalities in LEV: thrombosis, stenosis, and varicosities. The detailed analysis and comparison of imaging reports and respondents’ perception tend to provide ample evidence on the critical necessity and proactive role of CTV in health care services as an advanced technique. Moreover, the researchers were interested in whether the introduction of CTV imaging technique could be considered in health assistance cooperation with developing countries. Hence the need for this study, which employed a survey design, to investigate the added value of CTV in the identification of abnormalities in the veins of lower extremities.
Methods
Study design
A cross-sectional quantitative study was conducted in Hebei General Hospital of China from January 2017 to September 2019. The study entails collection, analysis, and comparison of data generated from all the direct CTV reports (211 cases) of both lower extremities, and color DUS reports (75 cases) of both lower extremities of these patients in the same period. The time of the DUS examination of the same patient was 1–5 days before the CTV examination, the same day or within 15 days after CTV examination but without any operation in lower extremity veins between CTV and DUS examinations. The individual and combined reports of CTV and DUS on the same patient over numbers of deep vein thromboses, stenoses, varicosities, and other abnormalities in each lower extremity were described and compared. The number and proportion of thromboses, stenoses, and May-Thurner Syndrome in LEDV reported in 211 CTV reports were analyzed. The possible records of intravascular angiography in these patients were also collected (eight records) in order to corroborate the accuracy of CTV examination.
In the meantime, a qualitative survey based on individual interview was conducted. The researchers randomly selected two senior doctors and one nurse from each of the Departments of Imaging and Vascular Surgery at Hebei General Hospital. The selection of this group of respondents would help to understand their perceptions on the use of CTV in diagnosis and treatment of LEV abnormalities, comparative efficacy of both CTV and DUS examinations, and the pros and cons of using CTV as an imaging technique in clinical practice. Also, four male and four female patients undergoing CTV examination were randomly interviewed individually, to obtain their perceptions on the benefits, convenience, as well as other personal perceptions of the CTV examination.
The quantitative and qualitative surveys described above would provide more insight to the critical need of CTV application in early detection and treatment of LEV abnormalities, especially deep venous thromboembolism and severe stenosis. This implies that impairment and deaths associated with such abnormalities would be reduced.
General settings
Social, economic, and technical status of the study site
As part of the North China region, Hebei Province has its provincial capital situated in the City of Shijiazhuang. At the end of 2019, Hebei province was home to a population of 75.92 million, with a per capita Gross Domestic Product at 46,348 RMB (around 7,242 USD per the exchange rate of 100 RMB = 6.4 USD), and an average of 6.46 health workers per 1,000 population. Located in the urban area of Shijiazhuang City, Hebei General Hospital is a tertiary general hospital equipped with the following resources: 2,500 beds, 1,858 open beds, 71 clinical medical and technical departments, 541 medical and technical staff with a senior professional title, and 27 experts enjoying special allowances from the State Council. The hospital has two national key disciplines and 26 provincial key disciplines, and has employed medical equipment with a total value of 790 million RMB (123 million USD), including the first high-end FORCE open source CT. In 2020, the hospital received 1,103,445 outpatients, and 64,066 inpatients.
CTV measurement
The protocol of the technique establishes a delivery channel through the dorsal foot vein, then injects a diluted contrast agent bilaterally, with the ratio between contrast agent and normal saline at 1:8 or 1:9. Then, two groups of high and low energy data are obtained through one dual-source CT dual-energy scanCitation8,Citation9. Next, with the support of the unique dual-energy bone subtraction software, the high densities in the scan can be well distinguished, thus precisely separating the bones and blood vessels, displaying the vascular tree alone and obtaining high resolution images.
In this study, a low flow rate and low concentration contrast agent were used and was continuously injected with a high pressure syringe to reduce the risk of extravasation. Then 40 ml of contrast agent with a concentration at a ratio of 1:8 was diluted with 320 ml of normal saline. Then, intravenous indwelling needles were placed in both feet and the diluted contrast agent was injected simultaneously from the veins of both lower extremities at a flow rate of 1.2 ml per second. Volume rendering (VR), multiplanar reconstruction (MPR), maximum intensity projection (MIP), and curved projection reformation (CPR) were used to obtain post-processing images and generate two-dimensional and three-dimensional reconstruction of lower extremity deep veins (LEDV) and display the vascular tree separately. Covering from the toe to third lumbar vertebra, CTV scans for both lower extremities were performed with different lengths of time and with different radiation doses varying with the height and weight of patients (Absorption dose = Dose–length product (DLP)*0.015, ≈ 6 mSV). The total DLP (mGy·cm) was lower than the 25th percentile radiation dose of urography (870 mGy·cm) in China’s related standard (WS/T 637-2018). Before the examination, each of the patients signed an informed consent form.
Statistical analysis
Quantitative survey
The quantitative research data collected was double-entered with validation using Epidata Entry version 3.1 and exported into Statistical Package for Social Science (SPSS) 22 for analysis. The number and proportion of thromboses, stenoses (including severe stenosis), and varicosities in deep vein, superficial vein, and intermuscular vein in the CTV reports and DUS reports were described as percentages. Among the cases having both CTV and DUS examination reports, the number of LEV abnormalities reported by CTV and DUS and both CTV and DUS were described. The incidence of LEV thromboembolism (including old thrombosis) reported by CTV and the gender-disaggregated incidence of the abnormality were described.
In this study, we compared the incidences of LEV thromboembolism and stenosis detected by CTV based on gender (male and female) and lower extremities side (left and right) difference. Chi-square (χCitation2) and Student t-tests were applied to compare the rates and means, respectively. A significance level of α = 0.05 was used.
The LEVs analyzed include: deep veins, superficial veins, and intermuscular veins of lower extremities. The LEDVs included the common iliac vein (CIV), internal iliac vein (IIV), external iliac vein (EIV), femoral vein (CFV), popliteal vein (POV), anterior tibial vein (ATV), posterior tibial vein (PTV), and peroneal vein (PEV). The lower extremity superficial veins (LESV) analyzed include the great saphenous vein (GSV) and small saphenous vein (SSV). The LEV abnormalities analyzed in this study include thrombosis, stenosis, and varicosity or dilatation.
Qualitative survey
Based on the written records and recordings of the interviews, the collected information was checked, corrected, and finalized. Then, the topics, cases, and perspectives on the cases were coded and classified, followed by the sorting and analysis of the case information, and the description of the interview results.
Quality control
All the results of the CTV examinations in the study period and those of the DUS examinations of the same patients closest to the CTV examination time were collected as far as possible. Data double entry, check, and error correction were conducted. All individual interviews were conducted in the same manner by one major researcher.
Confidentiality
The quantitative data was analyzed from a population perspective but not correlated with the individual information such as the name, appearance characters, address, etc. of the patients directly. Individual information of the patients was not revealed in the demonstration of qualitative data.
Results
Case report results
A total of 211 CTV reports for lower extremities of 211 patients were collected, including 109 males and 102 females, aged 15 ∼ 85 (54.9 ± 13.7) and 22 ∼ 83 (56.5 ± 12.5) years, respectively (t = .884, p >.05). Among them, DUS reports for lower extremities in the same period were collected from 75 cases (CTV + DUS group), 42 males and 33 females, aged 15 ∼ 85 (57.4 ± 9.5) and 32 ∼ 74 (56.1 ± 5.9) years, respectively (t = .700, p >.05) ().
Figure 1. Number, age range, mean age, and median age (years) of the patients. 
 Median age
Median age  Average age
Average age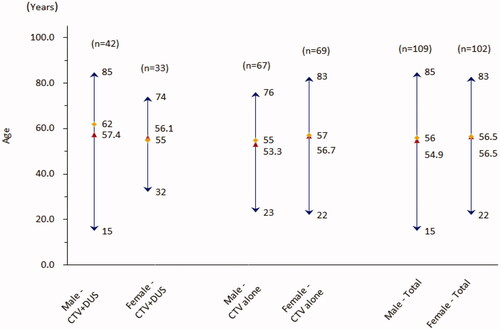
In the 75 cases with both CTV and DUS reports, 51 cases (68.0%) had LEV abnormalities (abn), including five patients (6.67%) with May-Thurner syndrome. There were also cases of lower extremity edema (LEE) or lower extremity soft tissue disease (LESTD), cardiovascular disease and cerebrovascular disease (CCVD), tumor, post-cesarean section delivery (CD), and other postoperative (PO) and physical examination (PE) cases ().
Table 1. Diseases and health status of CTV + DUS group.
The numbers of thromboses, stenoses, and varicosities reported by CTV were higher than those reported by DUS for all LEDVs (χ2stenoses = 139.176, χ2abnormalities = 104.164, p <.05), and for both males (χ2stenoses = 102.857, χ2abnormalities = 78.449, p <.05) and females (χ2stenoses = 39.224, χ2abnormalities = 27.574, p <.05) statistically significantly. The thromboses identified by CTV occurred in CFV, POV, and PEV. The number of thromboses reported simultaneously by CTV and DUS were more than that reported by CTV alone for both males and females. No thrombosis was reported in the iliac vein. The ratio between the number of thromboses in LEDV reported by CTV (19) and the number of all patients (75) was .253. The per capita number of LEDV stenoses reported by CTV was 1.5 and 1.2 in male and female patients, respectively, with severe stenosis accounting for 40% and 47.5%, respectively. The LEDV stenosis reported by CTV occurred mostly in the CIV (male 30.8%, female 45%), EIV (male 24.6%, female 17.5%), with statistical significance (χ2female = 5.000, χ2total = 26.076, p <.05), and a high proportion of them in the two locations were severe stenosis, which accounted for 57.7% (male) and 78.9% (female) of all severe stenosis reported in LEDV. DUS did not report the grades of stenosis. None of the LEDV stenosis reported by CTV in male patients was reported by the DUS examinations, while four of such cases were reported by the DUS in females. In terms of the reported number of thromboses, vascular stenoses, vascular varices in CFV, POV, ATV, PTV, and PEV, CTV was 3.3- and 2.2-times that of DUS in males and females, respectively, including 14.3% (male) and 22.7% (female) reported by both CTV and DUS ().
Table 2. The reported number of deep vein abnormalities in lower extremities (by CTV alone, both CTV and DUS, and DUS alone).
In the 75 patients with both CTV and DUS report, a total of 159 LEDV abnormalities were reported, among which 125 (79%) were reported by CTV alone, while 16 (10%) and 18 (11%) were reported simultaneously by CTV and DUS, and by DUS alone, respectively. Among the abnormalities reported by CTV alone, the CIV was the most frequently reported site (38, 24%), followed by the CFV (28, 18%), the EIV (24, 15%), and the POV (21, 13%). The abnormalities in other LEDVs were less frequently reported ().
Figure 2. Mix of lower extremity deep vein abnormalities reported by CTV and DUS. 
 CTV&DUS
CTV&DUS  DUS
DUS  CTV
CTV  IIV
IIV  EIV
EIV  CFV
CFV  POV
POV  ATV/PTV
ATV/PTV  PEV
PEV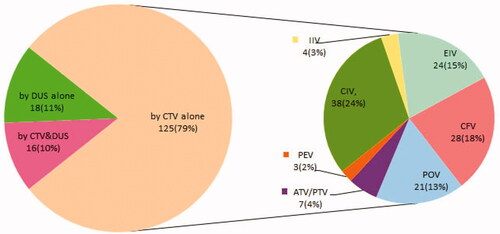
CTV reported a smaller number of thromboses, stenoses, and varicosities in the intermuscular calf vein than DUS, while for the lower extremity superficial vein (LESV) the number was close to that of DUS, but the abnormalities reported by both CTV and DUS simultaneously were very few ().
Table 3. The reported number of intermuscular and superficial abnormalities in lower extremities (by CTV alone, both CTV and DUS, and DUS alone).
In 136 patients with only CTV reports, 22 (14 for males and eight for females) LEDV thromboses were reported, with a ratio of 0.16 to the number of cases. The numbers of LEDV stenoses reported by CTV in male and female patients were 1.5 and 1.0 per capita, respectively, of which severe stenosis accounted for 50% and 29.9%, respectively. The main reported sites were CIV, CFV, and male EIV. All the reported superficial venous abnormalities were varicose ().
Table 4. The number of abnormalities in the lower extremity veins reported in the CTV group.
Among all of the LEDV abnormalities (thrombosis, stenosis, varicosity) reported by CTV (n = 211), the ratios between the numbers of reported abnormalities and patients were 1.055 and .688 for left and right extremities of male patients, and .892 and .461 for left and right of female patients, respectively. Therefore, the ratios for the left were higher than the right statistically significantly (tmale = 2.896, tfemale = 4.347, p <.05); and the ratios for males were higher than those for females with a statistical significance in the right (tright = 2.223, p <.05).
In terms of thrombosis, the ratios between the reported number and the number of patients were .193 and .018 for left and right extremities of males, and .137 and .078 for left and right extremities of females, respectively. Thus, the ratios were higher in the left than in the right, with a statistically significant difference for males (tmale = 2.475, p <.05); and the ratios were also higher in males than females, but no statistically significant difference was shown (p >.05).
When regarding vascular stenosis, the ratios between the reported number and the number of patients were higher in the left than in the right extremities, with a statistically significant difference for females (tfemale = 4.304, p <.05); and the ratio for males was higher than that of females, with a statistically significant difference for the right side (tright = 3.024, p <.05). The ratios of severe vascular stenoses had a similar situation but without a statistically significant difference (p >.05) ().
Figure 3. Gender and left–right comparison of the ratio between the number of lower extremity deep vein abnormalities reported by CTV and the number of cases. 
 Male-right
Male-right  Female-left
Female-left  Female-right. Notes: *p < 0.05, left vs right for the same gender. #p <.05, male vs female for the same side. The ratios between the number of lower extremity deep vein abnormalities reported by CTV and the number of patients.
Female-right. Notes: *p < 0.05, left vs right for the same gender. #p <.05, male vs female for the same side. The ratios between the number of lower extremity deep vein abnormalities reported by CTV and the number of patients.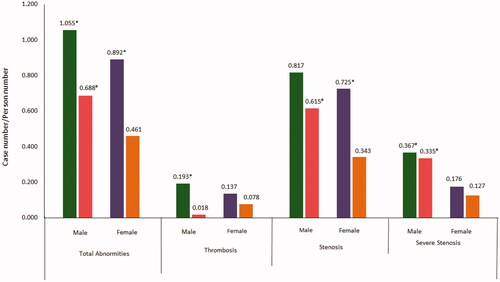
Twenty-three patients, accounting for 10.9% (95% CI = 6.7 ∼ 15.1%) of the 211 patients in total, were reported by CTV to have 41 deep vein thromboses (DVT). Among them, 10 patients (4.7%) consisting of seven males and three females were reported to have old thrombosis ().
Figure 4. Percentages of the patients with lower extremity deep vein thrombosis (including old thrombosis) reported by CTV. 
 Fresh thrombosis
Fresh thrombosis  None thrombosis
None thrombosis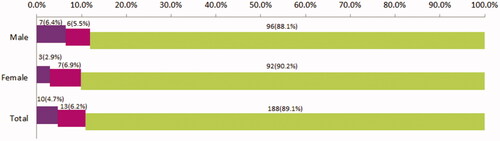
Eight of the 211 patients have records of intravascular angiography for lower extremities which is the golden standard of vascular examination. When comparing the CTV reports in the same patients, almost all of the reported abnormities in common iliac veins were in agreement ().
Table 5. The agreements and disagreement between the reports of CTV and intravascular angiography.
Perceptions of medical staff and patients on CTV
In the individual interviews, doctors from both departments believed that the CTV images can offer a highly visualized and comprehensive understanding of the venous conditions of lower extremities, especially in iliac veins, and can provide effective guidance to the surgery performance, which is also a prominent advantage over DUS. “CTV for lower extremities is more highly visualized than DUS, which can help us see which part of the blood vessel has stenosis and thus can adequately inform the design of the surgical plan. Therefore, the doctors can be guided to choose the appropriate surgical approaches. In comparison, DUS is only a real-time image and cannot effectively guide surgeries” (from a vascular surgeon). “CTV can detect the small thromboses in anterior tibial vein and peroneal vein clinically” (from an imaging doctor). “After the introduction of CTV for lower extremities, the post-processing images can be more highly visualized, and multi-faceted reconstruction can be made to see which way the blood vessels in the lower extremities flow, whether there exist thrombosis and compression of iliac vein from multiple angles. The diagnosis is more highly visualized and three-dimensional, which can provide the adequate information needed for clinical surgery and help you to select the best surgical approaches” (from an imaging doctor). “With CTV for both lower extremities, you can have better diagnosis of iliac vein stenosis, iliac vein compression and iliac vein thrombosis compared with DUS” (a vascular surgeon). Doctors also believed that CTV has the advantage of showing perivascular tissue lesions. “We can also see the peripheral tissue lesions, and the images can clearly show calcified plaques, while DUS only shows plaques without knowing if they are calcified” (from an imaging doctor).
Nurses commented that “CTV can guide the surgical operations, but it is difficult to locate the veins. So, you would have some challenge with venipuncture, but the examination is relatively smoother”.
During the individual interviews in patients, five patients gave positive feedback that the examination was useful, and that it was easy to operate. “I think it’s very nice and convenient and other examinations cannot find out the problem”. “It was part of the examination, and I don’t think it’s troublesome or inconvenient”. Two male patients thought it was inconvenient, but they could accept it as it was needed for the diagnosis. “It’s inconvenient, but there’s no other way when you get sick. Other parts of the examination were OK”. A 53-year-old female patient commented that it was inconvenient as indwelling needles were placed in both lower extremities. Jabs on the hands can be more convenient and cause less pain than on the feet.
Discussion
In this study, both quantitative and qualitative surveys were conducted to investigate the benefits of using CTV as an imaging technique in hospitals for identification of lower extremity vein abnormalities, especially deep vein thrombosis, stenosis, and varicosities. The results of the study revealed that: A greater number of deep vein abnormalities in the lower extremities were identified by CTV than DUS in both males and females (). At the same time, more abnormalities were detected in males than females, and in the left than right sides by CTV (p <.05) (); the incidence of thrombosis was 10.9%, which was higher in males than in females (); while the incidence of May-Thurner Syndrome was 6.67%. All of the above incidences are in conformity with the general rule of abnormalities observed in lower extremity veins reported in previous literatureCitation10,Citation11. Therefore, a comparatively representative sample was obtained in this study, although it simply included all of the cases for a given period without a special sampling operation.
Although some researchers reported that the serial ultrasound method had the high sensitivity and specificity in testing the DVT of the lower extremitiesCitation12, some other earlier studies demonstrated that DVT detection of CTV and DUS was comparableCitation13,Citation14. However, in the present study, the capacity of CTV was superior to DUS in the detection of deep vein abnormalities in the lower extremities, especially in the common iliac vein, internal iliac vein, and external iliac vein that were proximal LEDVs. Among the same patients, CTV reported 3.15-times more abnormalities of lower extremities than DUS in 75 patients although most of which were stenosis in this study. In agreement of our findings, the study of Jain et al.Citation15 had reported 2.60-times more iliac vein thromboses detected by CTV than DUS in 80 patients. This further elucidates the superiority of CTV detection capacity over DUS observed in this study. At the same time, 13 cases of dissatisfaction with the exploration of iliac vein were reported by DUS (). However, CTV had no advantage over DUS in the detection of intermuscular or superficial vein abnormalities in lower extremities, especially vascular varicosities (). The comparison between CTV and golden standard method of intravascular angiography showed a better level of agreement in the identification of abnormalities in common iliac veins, although the sample size was very small. Hence, CTV possesses prominent beneficial potency that ensures a satisfactory diagnosis of deep vein thrombosis, stenosis, and varicosities of lower extremities.
Also, the results obtained in this study showed that the most frequent site of LEDV abnormalities was the common iliac vein followed by the femoral vein. This is evidenced in the report of 75 patient cases examined with both CTV and DUS. CTV reported 25.8% (41) of the total abnormalities (159) in the common iliac vein, and 21.4% (34) in the femoral vein, which were the highest percentages (); in the 136 patients with only CTV reports, the figures were 40.6% (91) and 26.3% (59) of the total abnormalities (224), respectively, and also the highest (). They were 34.5% (132) and 24.3% (93) of the total (383) ( and ). The above results indicated that the common iliac and femoral veins are the most susceptible sites for LEDV abnormalities, while the CTV has high level sensitivity in detection of abnormalities in these sites.
According to CTV examination results, the total number of LEDV abnormalities was statistically significant (p <.05) for gender and side. There was a higher number of LEDV abnormalities in the left than right extremity of the same gender, while the right of the male was recorded as higher number than the right of the female. Also, there were variations among the number of thromboses. The number in the left was higher than that in the right for males. For stenosis, the number in the left was higher (p < .05) than that of the right in females, while that in the left of the males was higher (p < .05) than that in the right of the females. These results demonstrated that the left lower extremity of males were faced with the highest risk of LEDV thrombosis and stenosis, while female right lower extremities had relatively lower risk. We, therefore, speculated that the gender-disaggregated and left-right differences identified by CTV would become more obvious with a larger sample size and the greater number of thrombosis cases.
A small number of reports (11.32%) over LEDV abnormalities were made by DUS but not CTV, which may be explained by three reasons. Firstly, it may be caused by the different detection capacities between DUS and CTV examinations; secondly, the difference may arise from the different detection capacities of two teams of doctors and technicians performing DUS and CTV examinations; thirdly, it may be due to the vascular changes during the different timings when the patients received the CTV and DUS examinations. However, since the above-mentioned cases were very small, they did not affect the overall analysis results.
Additionally, this study adopted sociological method in the form of interviews to understand the subjective perceptions of medical staff and patients on the introduction of CTV technique into the clinical practices of the hospital which could be a supportive supplementary part to quantitative investigation to obtain a whole picture of the significance of CTV introduction. Because just quantitative data cannot demonstrate people’s concrete feeling on the CTV, and people’s acceptance to the technique is important because the technique is used by people and applied for people, the quality and value of medical services cannot be separated from human’s evaluation. According to the individual interview data collected from medical staff, CTV has inestimable benefits in diagnosis because it can guide the performance of venous surgeries for lower extremities, aid doctors to observe: the formation of collateral circulation, the function of vascular valve, and the specific status of perivascular tissues, including calcification plaques. The considerable potentials of the CTV as a method for the detection of LEDV abnormalities would lend a strong structure to hospitals for precise diagnosis and targeted treatment of the same, thus offering better health benefits to the patients with such health challenges. On the other hand, according to the interviews of patients, most patients believed that the use of CTV for examination was a convenient platform. Although a few patients felt slightly uncomfortable with needle retention and injection pain, they believed that the benefits from the CTV diagnosis outweighed the discomfort of the procedure, and that the examination was essential for them. The patient respondents suggested the medical staff to ensure that the CTV operation procedures were made to be friendlier for patients, in particular for those who are advanced in age, so as to promote general acceptance of the procedure among patients.
Venous thromboembolism of lower extremities can lead to lower extremities edema, pulmonary vein thrombosis, post-thrombotic syndrome, and impairment of venous valve function etc.Citation16–18. Thirty percent of pulmonary vein embolism is caused by venous thromboembolism. In recent years, the world, including developing and underdeveloped countries, has been increasingly confronted with a greater incidence of obesity, hyperlipidemia, hypertension, diabetes, rheumatoid arthritis, and tumors, the growing trend of aging population, and a higher C-section rate among the pregnant women and so on which are risk factors for thromboembolism in veinsCitation19–27. As the CTV technique can provide an earlier, highly visualized, and clearer imaging of the deep vein thrombosis, stenosis, and varicosities in the lower extremities including May-Thurner Syndrome, and help the doctors to observe the formation of post-thrombotic collateral circulation, it can help to take early and effective medical interventions to control the occurrence and progression of the conditions, alleviate impairments, optimize treatment outcomes, and reduce the burden of disease. Imperatively, this would register positive impacts on the reduction of severe outcomes and even death, although there exist insufficient studies on whether greater risk factors have led to an increased incidence of lower extremities venous thromboembolism.
The present research work which is considered to be of clinical significance is not without limitations and strengths, while proposed recommendations are drawn from the strengths and future adjustments made for the limitations. The present research was a retrospective cross-sectional study, the analysis was performed based on the most available data. Thus, the records of intravascular angiography for lower extremities which is the golden standard of vascular examination were so few to make a full evaluation on CTV, although some study use CTV as a golden standardCitation14. While the comparison of the eight cases could illustrate the accuracy of CTV method in a way () because six in eight report pairs had no disagreement, although the quantity of the case pairs was not enough to make statistical comparisons as what we did between CTV and DUS reports. Actually, in clinical practice, the patients with both CTV and angiography results are rare. Meanwhile, in the only three disagreements between CTV and intravascular angiography reports of the two other cases, CTV even reported one more thrombosis in left CIV than intravascular angiography. On the other hand, the two pieces of missed reporting by CTV were one POV obstruction and a severe stenosis at the left CIV fork. Whether they could be the common weakness in identifying the abnormities in LEDV by CTV is needed to be noted and observed further to accumulate related experiences. Another, the investigated number of patients was not large enough to show more DVT patients which would allow for an in-depth analysis of observations on the occurrence site, gender-disaggregated, and left-right differences, etc. Despite the aforementioned limitations of this study, it has drawn strengths from the comparatively larger size of CTV and DUS report pairs for the same patients that was scarce in previous available literature. Also, the results in all collected reports were analyzed in comparison to 10 lower extremity veins to show the identification capacity of CTV. A further research in line with the present study may entail the investigation of cost-benefit analyses to corroborate this view from the perspective of reducing the disease burden.
Shijiazhuang city, where the present study was conducted, is a second-tier city rather than a first-tier city in China. The patients visiting Hebei Provincial General Hospital do not only come from Shijiazhuang, but also from the surrounding cities and rural areas. After the introduction of CTV, satisfactory results have been observed in many aspects, such as diagnosis and treatment, and satisfaction of both the medical staff and patients. Based on these positive findings with supportive quantitative and qualitative evidences, the CTV technique can be introduced into developing countries for early identification of abnormities in LEDV where it is feasible with suitable conditions.
Conclusions
Application of CTV for early and accurate detection of LEDV abnormalities including thrombosis has been proven to be efficient. Corresponding benefit in early intervention and reduction of severe complications of such abnormalities is of important value and significance. CTV earned good recognition and acceptance from medical staff and patients. Hence, it could be considered as part of global health assistance cooperation with developing countries to facilitate enhanced medical services.
Transparency
Declaration of funding
The source of funding for the research reported comes from Hebei Provincial Health Commission Scientific Research Funding Program 20190405 and China’s Public Health Assistance Capacity Building Program by China CDC 131031001000160006. The funding bodies have financially supported the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Declaration of financial/other relationships
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
YQL has engaged in the design of the study and collection, analysis, and interpretation of data and drafting the manuscript. ZFX has engaged in the technical support to collection of data and drafting the manuscript. JJT has engaged in the technical support to the collection and interpretation of data. YMC has engaged in the technical support to the design of the study and interpretation of data. YFW has engaged in the analysis of data and drafting of the manuscript. NF has engaged in the design of the study and collection, analysis, and interpretation of data and drafting the manuscript. All authors have read and approved the manuscript and ensured that this is the case.
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki. After reviewing, this paper conforms to the principals of medical ethics. It is accepted to publish by Hebei General Hospital Ethics Committee (No. 202117, April 21, 2021).
Acknowledgements
The authors wish to thank all doctors, nurses and patients who participated in the individual interviews of the study and all patients whose CTV, DUS, and intravascular angiography examination reports were analyzed in the study.
Data availability statement
All data generated or analyzed during this study are included in this published article.
References
- Coelho A, O'Sullivan G. Usefulness of direct computed tomography venography in predicting inflow for venous reconstruction in chronic post-thrombotic syndrome. Cardiovasc Intervent Radiol. 2019;42(5):677–684.
- Coelho A, O’Sullivan G. Evaluation of incidence and clinical significance of obturator hook sign as a marker of chronic iliofemoral venous outflow obstruction in computed tomography venography. J Vasc Surg. 2020;8(2):237–243.
- Mavili E, Ozturk M, Akcali Y, et al. Direct CT venography for evaluation of the lower extremity venous anomalies of Klippel-Trenaunay Syndrome. AJR Am J Roentgenol. 2009;192(6):W311–W316.
- Choi JW, Jae HJ, Kim H-C, et al. CT venography for deep venous thrombosis: can it predict catheter-directed thrombolysis prognosis in patients with iliac vein compression syndrome?. Int J Cardiovasc Imaging. 2015;31(2):417–426.
- Junwei WANG, Xinling C, Jianbo GAO, et al. The diagnostic value of different reconstruction methods of 320-slice CT in deep venous thrombosis of lower extremities. Chin J Integr Trad Chin Western Med. 2018;16(2):128–130.
- Yuefeng ZHU, Ming YUE. Early diagnosis of lower extremity deep vein thrombosis caused by trauma fracture through direct multi-layered spiral CT angiography of both lower extremities. Chin J Med Imag. 2016;24(7):524–526.
- Shi W-Y, Wang L-W, Wang S-J, et al. Combined direct and indirect CT venography (combined CTV) in detecting lower extremity deep vein thrombosis. Medicine. 2016;95(11):e3010.
- Image Technology Branch of Chinese Medical Association Radiology, Branch of the Chinese Medical Association. Expert consensus on CT examination technique. Chin J Radiol. 2016;50(12):916–928.
- Iyama Y, Nakaura T, Kidoh M, et al. Relationships between patient characteristics and contrast agent dose for successful computed tomography venography with a body-weight-tailored contrast protocol. Medicine. 2018;97(14):e0231.
- Sedhai YR, Golamari R, Salei A, et al. May-Thurner syndrome. Am J Med Sci. 2018;355(5):510–514.
- Harbin MM, Lutsey PL. May-Thurner syndrome: history of understanding and need for defining population prevalence. J Thromb Haemost. 2020;18(3):534–542.
- Bhatt M, Braun C, Patel P, et al. Diagnosis of deep vein thrombosis of the lower extremity: a systematic review and meta-analysis of test accuracy. Blood Adv. 2020;4(7):1250–1264.
- Taffoni MJ, Ravenel JG, Ackerman SJ. Prospective comparison of indirect CT venography versus venous sonography in ICU patients. AJR Am J Roentgenol. 2005;185(2):457–462.
- Shiver SA, Lyon M, Blaivas M, et al. Prospective comparison of emergency physician-performed venous ultrasound and CT venography for deep venous thrombosis. Am J Emerg Med. 2010;28(3):354–358.
- Jain AK, Soult MC, Resnick SA, et al. Detecting iliac vein thrombosis with current protocols of lower extremity venous duplex ultrasound. J Vasc Surg Venous Lymphat Disord. 2018;6(6):724–729.
- Chopard R, Albertsen IE, Piazza G. Diagnosis and treatment of lower extremity venous thromboembolism. JAMA. 2020;324(17):1765–1776.
- Di Nisio M, van Es N, Büller HR. Deep vein thrombosis and pulmonary embolism. Lancet. 2016;388(10063):3060–3073.
- Sato T, Yoshimura N, Horii Y, et al. Low tube voltage computed tomography venography for patients with deep vein thrombosis of the lower extremities – a comparison with venous ultrasonography. Circ J. 2021;85(4):369–376.
- Chan W, Wang B, Li Q, et al. Study on the risk factors of preoperative deep vein thrombosis (DVT) in patients with lower extremity fracture. Clin Appl Thromb/Hemost. 2021;27(3):1–6.
- Chen J, Guo L, Li S, et al. Efficacy and safety of postural intervention on prevention of deep venous thrombosis of lower extremity in postpartum women with pregnancy induced hypertension. Medicine. 2021;100(12):e24959–16.
- Ay C, Pabinger I, Cohen AT. Cancer-associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost. 2017;117(2):219–230.
- Gregson M, Sweeting AR, Folsom J, et al. Cardiovascular risk factors associated with venous thromboembolism. JAMA Cardiol. 2019;4(2):163–173.
- Riva N, Donadini MP, Ageno W. Epidemiology and pathophysiology of venous thromboembolism: similarities with atherothrombosis and the role of inflammation. Thromb Haemost. 2015;113(6):1176–1183.
- Tian Q, Li M. Risk factors of deep vein thrombosis of lower extremity in patients undergone gynecological laparoscopic surgery: what should we care. BMC Womens Health. 2021;21(1):130–135.
- Ogdie A, Kay McGill N, Shin DB, et al. Risk of venous thromboembolism in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: a general population-based cohort study. Eur Heart. 2018;39(39):3608–3617.
- Peng Y-H, Lin Y-S, Chen C-H, et al. Type 1 diabetes is associated with an increased risk of venous thromboembolism: a retrospective population-based cohort study. PLoS One. 2020;15(1):e022699.
- Mulder F, Horvàth-Puhó E, van Es N, et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021;137(14):1959–1969.