

Abstract
Objectives
To evaluate incidence of stroke, myocardial infarction (MI), and peripheral artery disease (PAD) in patients with type 2 diabetes mellitus (T2DM) and assess associated health care resource utilization (HCRU) and costs in the United States.
Methods
Patients ≥18 years of age with a T2DM diagnosis, with or without incident stroke/MI/PAD, were indexed between 1 January 2012 and 31 December 2020, from the deidentified Optum Clinformatics Data Mart claims database. Incidence of stroke, MI, and PAD was evaluated in the year following T2DM. HCRU and costs were measured in the 12 months following study entry in patients with T2DM + stroke, T2DM + MI, and T2DM + PAD (experimental cohorts) and compared to HCRU and costs in patients with T2DM alone (control cohorts).
Results
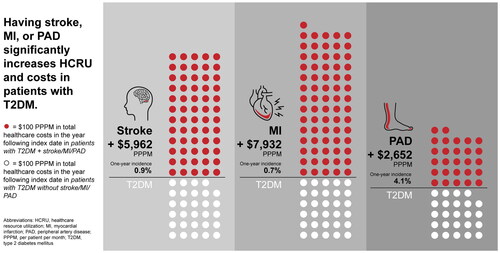
Incidence of stroke, MI, and PAD in patients with T2DM was 0.9% (n = 16,034), 0.7% (n = 13,681), and 4.1% (n = 68,479), respectively. Compared to matched patients with T2DM alone, patients with T2DM + stroke/MI/PAD had significantly higher total healthcare costs in the year post-index date (T2DM + stroke: +$5962 per patient per month [PPPM]; T2DM + MI: +$7932 PPPM; T2DM + PAD: +$2652 PPPM; p < .05). Patients with T2DM + stroke/MI/PAD had significantly higher mean HCRU than patients without stroke/MI/PAD in all categories measured.
Conclusion
Having stroke, MI, or PAD was associated with increases in HCRU and costs in patients with T2DM. Although PAD was associated with smaller per patient increases in total healthcare costs than patients with T2DM + stroke/MI, the higher frequency of incident PAD may make it more costly than MI or stroke in a large population of patients with T2DM.
Graphical Abstract
PLAIN LANGUAGE SUMMARY
Compared to patients without type 2 diabetes (T2D), patients with T2D have a greater chance of having a stroke, heart attack, and narrowing of blood vessels in the arms and legs (peripheral artery disease [PAD]). A stroke, heart attack, or PAD may lead to hospitalization or death. We sought to understand healthcare usage (hospital visits, emergency room visits, office visits, etc.) and costs associated with stroke, heart attack, and PAD in patients with T2D in the United States. Healthcare resource usage and costs were estimated by using data from health insurance claims to compare healthcare usage and costs among patients with T2D, some of whom had a stroke, heart attack, or PAD, and some who did not. Compared to patients with T2D without stroke/heart attack/PAD, patients with T2D and stroke/heart attack/PAD had more overnight hospital visits, doctors’ office visits, and emergency room visits. Patients with T2D and stroke/heart attack/PAD also had longer hospital stays. Patients with T2D and stroke/heart attack/PAD all had higher total healthcare costs in the year following their diagnoses, compared to patients with T2D without stroke/heart attack/PAD. By highlighting the greater costs and use of healthcare associated with stroke, heart attack, and PAD in patients with T2D, we hope to encourage more preventative management of stroke, heart attack, and PAD in patients with T2D.
Transparency
Declaration of funding
This study was funded by Novo Nordisk, Inc. which had a role in the design, conduct, and reporting of the study.
Declaration of financial/other relationships
Aaron King: reports receiving consulting fees from Novo Nordisk and payment/honoraria for presentations from Novo Nordisk, Mannkind, Abbot, Medtronic, Eli Lilly, and Dexcom. Jigar Rajpura: employee and shareholder of Novo Nordisk, Inc. Yuanjie Liang: employee and shareholder of Novo Nordisk, Inc. Yurek Paprocki: employee and shareholder of Novo Nordisk, Inc. Chioma Uzoigwe: employee and shareholder of Novo Nordisk, Inc. Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
All authors were involved in the conception and design of the study. YL conducted the statistical analyses, and all authors were involved in the interpretation of the data. All authors were involved in the drafting of the paper and revised it critically for intellectual content. All authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Acknowledgements
The authors thank John Newman, Ph.D. and Rebecca Hahn, MPH of KJT Group, Inc. (Rochester, NY, USA) for medical writing support funded by Novo Nordisk, Inc. (Plainsboro, NJ, USA). Data in this manuscript has been previously presented by the same author group as posters at the American Diabetes Association’s (ADA) 82nd Scientific Sessions taking place 3–7 June 2022 and the corresponding abstracts will be published in Diabetes following the conference.
Data availability statement
No data are available. None of the participant (de-identified) data collected in the study can be shared.
Notes
i Optum Clinformatics, Eden Prairie, MN, USA.
ii IBM, Armonk, NY, USA.