
ABSTRACT
In this paper we paper evaluate the effectiveness of eight sessions of cognitive analytic therapy (CAT) for treating obsessive morbid jealousy (OMJ), using a mixed-methods A/B with followup single-case design. Ideographic jealousy measures were collected throughout baseline (2 sessions), treatment (6 sessions) and follow-up phases (one session), creating a 160-day time series. Nomothetic measures were completed at assessment, end of treatment and at followup. A structured qualitative interview was completed. Significant reductions to idiographic jealousy measures occurred during the treatment phase, with these gains maintained over followup. The intensity of the jealousy shifted from moderate to mild and this change was attributed to CAT. Methodological issues and future directions for the treatment of OMJ are discussed.
Introduction
Jealousy is a complex process of thoughts, feeling and reciprocal actions existing within a romantic relationship when one partner perceives that the relationship is under some real or imaginary threat of loss from a rival (White & Mullen, Citation1989). Pathological jealousy differs from pathological love by the latter being defined by inappropriate selfless dedication to a partner and the need to provide perfect care, affection and attention at the expense of appropriate independence and self-care (Stravogiannis et al., Citation2018). Jealousy is always triangulated (i.e. accuser, accusee and presumed rival), but also exists on a continuum (Marazziti et al., Citation2003). At lower levels for example, reactive jealousy is seen as non-problematic and is actually related to relationship quality (Barelds et al., Citation2017), with jealousy also being reduced in more long-standing relationships (Dijkstra et al., Citation2010). Marazziti et al. (Citation2010) noted the clinical similarities between attachment and jealousy: both are triggered by separation, have the aim of maintaining relationships and a sense of psychological safety, and involve the same basic emotions of fear, anger, sadness. Wenger et al. (Citation2018) found that secure and dismissive attachment styles were unrelated to jealousy, whereas fearful attachment was associated with aggression, and preoccupied attachment was associated with non-assertive communication. One study noted that even infants can experience jealousy (Hart, Citation2002).
In terms of risk factors for morbid jealously, there appear many potential (probably interacting) etiological factors. Enoch and Trethowan (Citation1979) conceptualised the interplay of a chronic sense of inadequacy, oversensitivity and personal insecurity to be predisposing factors for the development of morbid jealousy. The personality feature that best distinguishes proneness to jealousy is high trait anxiety (Costa et al., Citation2015), and people with damaged self-esteem tend to be more jealous than those with fragile self-esteem (Stieger et al., Citation2012). Past experiences of parents having (or being accused of) conducting extra-marital affairs or previous partners being unfaithful are commonly reported (Karunarathne et al., Citation2017). Kingham and Gordon’s (Citation2004) review of risk factors highlighted four factors: sexual dysfunction, poor relationship functioning, poor social functioning and ongoing alcohol and drug misuse. The more recent Singh et al. (Citation2017) review strongly emphasised the role of substance misuse in morbid jealousy, with alcohol appearing to act as a key risk factor (DiBello et al., Citation2014).
Morbid jealousy also creates a significant risk of domestic abuse, homicide and/or suicide (Batinic et al., Citation2013). Domestic abuse may be a feature in any relationship containing jealousy, but this risk escalates when the jealousy is morbid (Mullen, Citation1990). More than half of morbidly jealous people have assaulted their partner at some point (Mullen & Maack, Citation1985), with the use of weapons a feature particularly of delusional jealousy (Silva et al., Citation1998). Children that observe jealous domestic violence are at heightened risk of trauma (Kingham & Gordon, Citation2004). Violence can also be directed towards the third party believed to be the love rival (Tarrier et al., Citation1990). Risk of violent jealous attack can also unfortunately escalate in the face of repeat denials, or when false confessions are elicited (Karunarathne et al., Citation2017). Females, either as perpetrators or victims, carry a higher risk of suicide as compared to males (Singh et al., Citation2017).
Clinicians can encounter morbid jealousy either as the primary disorder or as a comorbidity with other mental health problems (Kingham & Gordon, Citation2004). Extreme or morbid jealousy presents in either delusional or obsessional subtypes, whereby the sufferer/perpetrator issues repeated accusations that a partner is sexually unfaithful based on insignificant, minimal, or no evidence, and often using commonplace events or interactions to substantiate accusations (Batinic et al., Citation2013). The lifetime prevalence of morbid jealousy in either obsessional or delusional forms is unknown, but clinicians do encounter it frequently (Kingham & Gordon, Citation2004), with the clinical features cross-culturally stable (De Silva & De Silva, Citation1999). Whilst the impact of morbid jealousy on partners has not been extensively studied, partners’ mental health is often negatively affected due to the levels of coercion, control, imposed restrictions/limitations and cross-examining that are often features of jealous relationships (De Silva, Citation1997).
Delusional morbid jealousy (DMJ) occurs in the context of substance misuse, organic brain disease, schizophrenia and affective disorder (Graff-Radford et al., Citation2012; Ortigue & Bianchi-Demicheli, Citation2011; Seaman, Citation1979) or can present as the single delusion in a delusional disorder (APA, Citation2013). Obsessive morbid jealousy (OMJ) occurs when fleeting infidelity thoughts transform into obsessive, intrusive and persistent cognitions, creating a persistent and marked fear of abandonment, that drives associated compulsive behaviours (Cobb & Marks, Citation1979). Compulsive behaviours are often confirmatory and can include being controlling, recording, stalking, pleading, accusing, interrogating, blaming, checking and reassurance-seeking. Insight is retained as there is awareness that the fear and paranoia are excessive, with OMJ negatively impacting relationships, and sufferers often feeling extensive shame and guilt regarding their ego-dystonic compulsions (Kingham & Gordon, Citation2004). OMJ impairs the ability of the sufferer to function in valued areas of their life (Marazziti et al., Citation2003). OMJ is associated with poor emotional wellbeing and risks of emotional abuse of children in families where jealousy is a feature of the parental relationship (Kingham & Gordon, Citation2004).
Morbid jealousy has been traditionally seen as a complex, risky and difficult disorder to treat (Cobb & Marks, Citation1979). In terms of psychotherapeutic treatments for OMJ, the literature reports examples of effective behavioural (Cobb & Marks, Citation1979; Crowe, Citation1995; De Silva, Citation1987; López, Citation2003; Margolin, Citation1981; Teisman, Citation1979), cognitive (Bishay et al., Citation1989; Dolan & Bishay, Citation1996) and cognitive behavioural therapy (Kellett & Totterdell, Citation2013; Marks & De Silva, Citation1991). For those studies that reported the duration of treatments delivered, behavioural interventions ranged from 5 to 20 sessions, cognitive therapy for 4 sessions and cognitive behavioural therapy 13–16 sessions. In recent years, there has also been a stream of evidence regarding the treatment of OMJ using a focused integrative psychotherapy termed cognitive analytic therapy (CAT). Cognitive analytic therapy is a relational, integrative and time-limited psychotherapy informed by cognitive and psychodynamic theory or methods (Ryle & Kerr, Citation2002) and is delivered in 8, 16 or 24 session formats. CAT differs from behavioural, cognitive and cognitive behavioural therapies by taking a relational approach, working with the past, using enactments within the therapeutic relationship and associated analysis of habitual relationship patterns (Ryle & Kellett, Citation2018).
The effectiveness of a 16-session cognitive analytic therapy (CAT) was initially explored by Kellett and Totterdell (Citation2013) in a single-case experimental design (SCED). CAT was seen to facilitate significantly reduced jealousy for the patient, but the partner did not report a reduction in controlling behaviours. Curling et al. (Citation2017) produced an adjudicated hermeneutic single-case efficacy design that illustrated the causal therapeutic effect of a 16-session CAT on a female case. Curling et al. (Citation2018) then produced a case series of three patients treated with CAT (two 16 sessions and one 24 session intervention) to show significant reductions in the daily experience of OMJ across the three cases. Therefore, the CAT evidence base for the treatment of OMJ has been previously demonstrated for the 16 and 24 session formats, but there has not been any previous credible evaluation of the briefest 8-session version of the model. The 8-session version of CAT only differs in treatment duration, as the reformulation, recognition and revision structure of the therapy is retained. Calvert and Kellett (Citation2014) noted that the CAT outcome evidence base particularly required more studies of the briefest 8-session format of the model.
The rationale for the present study was to provide a thorough evaluation of the impact of the 8-session version of the CAT model via a mixed-methods single-case methodology. The 8-session version of the CAT model was selected as there is recent evidence that this version of the model is safe and effective in the treatment of depression, suggesting that when there is a single issue, then a brief intervention can be usefully provided (Kellett et al., Citation2018). We hypothesised that change would occur during treatment (compared to baseline), be maintained during follow-up on ideographic outcome measures, and that this change would be mirrored in the nomothetic outcome measures. Interviewing of the participant regarding the change process was also employed to create greater confidence as to whether CAT created the changes observed in the idiographic and nomothetic outcomes.
Method
Design
The case is reported according to the single-case reporting guidelines (SCRIBE) statement (Tate et al., Citation2016). Ethical approval was achieved for the analysis of the outcomes (ref: 032867). We used a mixed-methods A/B design with an extended follow-up; this is deemed a quasi-experimental single case design due to the lack of treatment withdrawal. The methodology was a phase change without reversal design (Shadish & Sullivan, Citation2011), which is the most common and pragmatic single-case method used to evaluate outcomes in routine clinical practice (Hersen, Citation1990). The study had three phases. The first phase (A) was the baseline (3-week duration, 21 days, containing two sessions) and entailed the assessment of the patient. The second phase (B) entailed treatment (10-week duration, 70 days, containing six sessions) and the final phase was at the 10-week (69 d) followup, with one follow-up session at the termination of contact with the participant. The contact with the patient was therefore two assessment sessions, six treatment sessions and one follow-up session. The three-week baseline enabled an assessment of any natural course of symptom improvement that may have occurred (Hersen, Citation1990), and reflects the two-session assessment period before an intervention pattern commonly seen in routine clinical practice (Morley, Citation2010). The study, therefore, generated a time series of N = 160 continuous days of data collection reflecting three distinct phases (baseline, treatment and follow-up). The treatment ("B") phase was started by discussion (at session 3) of a narrative reformulation of the OMJ – this is consistent with the CAT for OMJ single-case research (Curling et al., Citation2017; Curling et al., Citation2018; Kellett & Totterdell, Citation2013). Nomothetic outcome measures were completed at assessment, termination and follow-up. The participant was interviewed about their experience of therapy by an independent researcher (DS) at the follow-up point. The clinical follow-up was conducted by the therapist (SK).
The study was conducted in a tertiary specialist psychotherapy service within a National Health Service (NHS) mental health Trust. The participant gave consent for the collection and analysis of the qualitative and quantitative outcome data. The collection of the daily diary data was explained to the patient as being (a) wholly voluntary, (b) that they could stop completing the diary at any point should they feel that was the best option and (c) receiving the therapy was not contingent on data collection. The therapy was conducted by a male Consultant Clinical Psychologist and accredited cognitive analytic psychotherapist (SK) under weekly clinical supervision and the data were analysed by an independent researcher (DS).
The case
The case was assessed using the Kellett et al. (Citation2012) diagnostic interview format for OMJ. This focusses on three aspects; psychological assessment (e.g. form of jealousy, attachment style, history, trigger analysis, autonomic, cognitive and behavioural symptoms), mental state examination and risk assessment. The case was a male patient (50 years of age). No previous psychological interventions had been attempted. The patient was referred by his General Practitioner due to OMJ and had been prescribed an anti-depressant for many years. The patient reported a long comorbid history of depression with suicidal ideation, low self-esteem and anxiety.
Long-standing difficulties with morbid jealousy across all romantic relationships (including previous marriages and current long-term relationship) were reported. The patient’s current relationship had lasted for ten years and the couple lived alone. The partner also had a history of obsessive compulsive disorder (OCD) and the relationship was described as being riddled with frequent arguments, tensions and conflict. The patient reported a profound fear of abandonment and chronic fears/suspicions regarding infidelity. The patient reported watching his partners every move for any signs of potential rejection and when he perceived any sign of rejection, he became filled with physiological symptoms of fear and disgust. The physiological symptoms were interpreted as signs that “hunches” and “theories” regarding partner infidelity must have been true. The patient listed many triggers focussed around rejection. For example, the partner showing interest in herself would be a clear sign that another man was interested in her and vice versa. When jealous, the patient reported high-frequency checking of his partner’s whereabouts, phone usage, underwear, bed-clothes and internet records. In relation to his partner, daily reassurance-seeking was a feature, as well as frequent intense interrogations regarding fidelity and honesty. The interrogations were prompted by obsessive and intrusive images of his partner being unfaithful and engaging in sexual acts. The patient stated that the visual images were as if he was watching a film and were highly detailed and long-lasting.
The patient stated that he would spend long tracts of time worrying about attending future social events with his partner in case she met someone new and also ruminating over past social events for signs that he had been duped. The patient would obsess about this partner’s past sexual history. The patient reported that his thoughts were organised around a schema of mistrust. Apart from verbal aggression when jealous, no major aspects of major behavioural disinhibition were reported and the patient denied ever physically assaulting his partner. The patient was aware that when he engaged in jealousy-driven behaviour (e.g. shouting) he was being intimidating, but felt powerless to behave in any other manner and felt guilty and ashamed when the jealousy receded. Whilst the patient was ashamed of the manner in which he treated his partner, he felt he could not change.
The patient reported growing up in a nuclear family in which there was a lot of conflict between the parents. The mother was reported to be kind, caring and protective and the father as distant, rejecting and also controlling (i.e. restricting what the participant could and could not do). The mother was jealous of the father and would frequently cross-examine the father about his actions and whereabouts. The patient stated that there was no warmth in the paternal relationship and that he was fearful of his father’s quick temper and infrequent rage. The patient stated that he became hypervigilant of his father in order to protect himself from his rage and that he was always trying to please him. The patient reported chronic bullying at school due to his severe dyslexia and that he was frequently truant. The patient reported three significant romantic relationships in his life, all of which has been affected by jealousy and his insecure attachment style. The patient reported flying into jealous fits of verbal aggression when not reassured by his partners across all the relationships. The second marriage produced two children and one of the children died as an adolescent due to cerebral palsy. His wife was killed in a car accident on the way back from the funeral of the child. The patient reported being saddled with excessive guilt and self-blame regarding these life events.
Ideographic measures and their analysis
Seven ideographic (5 intensity type and 2 frequency type) measures were collaboratively designed in the first session for daily completion. The collaboration entailed identifying what the key concerns of the patient were and then the therapist suggesting possible methods of measurement. In this manner, the daily diary was constructed. The function of the daily diary was introduced to the patient as a means of enabling self-reflection and as a means of evaluating whether the therapy had been effective. Because of the patient’s dyslexia, care was taken to ensure that the measures could be easily comprehended and completed. Measure 1, “Today, I have been feeling jealous”; measure 2, “Today, I have been feeling anxious”; measure 3 “Today, I have been feeling untrusting / suspicious” and measure 4 “I have been ‘over-thinking’ today” were all scored 0 ‘not at all’ – 10 ‘all the time.’ Measure 5 “Today, we have functioned as a couple” was scored 0 “really poorly” – 10 “really well”. The two frequency measures indexed the daily number of images of infidelity (measure 6) and the number of checking incidents (checking 7). Measure one was the primary ideographic measure considering the presenting problem of the participant.
Serial dependency in the time series data was controlled for by creating a lagged variable that demonstrated the strongest correlation to each variable (Chatfield, Citation2003). Partial autocorrelations were used to demonstrate which lag was appropriate for each ideographic variable and this was inputted as a covariate in each analysis of covariance analyses (ANCOVA) that assessed for treatment effects between the three study phases. The ANCOVA had a single factor for the study phase, which had three levels (assessment, treatment and follow-up phases). No idiographic variables were normally distributed showing a positive skew (apart from couple functioning which was negatively skewed). However, ANCOVA is robust against violations of normal distribution (Glass et al., Citation1972) and post-hoc pairwise comparisons identified during which phases significant differences occurred. A Bonferroni correction was applied to control the familywise error rate and reduce the likelihood of type 1 errors. Graphs were created for each ideographic measure with trend lines fitted and descriptive statistics (mean, median and standard deviation) were calculated of the phase data. Degree of change in ideographic measures was quantified through the proportion of non-overlapping data (PND) points method between paired phases (Parker & Vannest, Citation2009). The Scruggs and Mastropieri (Citation1998) guidelines for interpreting PND results (1998) were applied; PND > 90 represent very effective treatment, 70–90 represents effective treatment, scores from 50–70 represent questionable treatment effectiveness, and scores below 50 are deemed an ineffective intervention. Percentage of data exceeding the median (PEM) was also employed to account for vulnerability to outliers in the PND method (Morley, Citation2010). Estimates of treatment effects based on PEM used the Wendt (Citation2009) criteria; <70% indicates questionable or ineffective treatment, 70–90% indicates a moderately effective treatment and >90% indicates a highly effective treatment.
Nomothetic measures and their analysis
The Prestwich Jealousy Questionnaire (PJQ; Beckett et al., Citation1992). The PJQ measures cognitive, affective and behavioural aspects of OMJ, with a score of >50 indicating clinically significant jealousy (Intili & Tarrier, Citation1998). Full-scale PSQ scores are classed as follows: no jealousy (0-33), mild jealousy (34-49), moderate jealousy (50-99), severe jealousy, (100-132) and very severe jealousy (>133). Given the presenting problem, the PSQ was selected as the primary nomothetic outcome measure for the study. Beck Depression Inventory-II (BDI-II; Beck, Steer, Ball, et al., Citation1996). The BDI-II is a 21-item valid and reliable measure of the intensity of depressive symptoms (Beck, Steer, and Brown, Citation1996). BDI-II scores are coded as follows: 0–13 (minimal depression), 14–19 (mild depression), 20–28 (moderate depression) and 29–63 (severe depression). Brief Symptom Inventory (BSI; Derogatis, Citation1993). The BSI (53 items) is a valid and reliable measure psychological distress (Derogatis, Citation1993) and breaks down into three subscales, with the global severity index (GSI) the most commonly reported. A raw score greater than .78 on the BSI-GSI relates to the patient reaching “caseness”. Inventory of Interpersonal Problems-32 (IIP-32; Barkham et al., Citation1996). The IIP-32 is a reliable (Barkham et al., Citation1996) and valid (Hughes & Barkham, Citation2005) measure of interpersonal problems and is the short version of the Inventory of Interpersonal Problems-126. Nomothetic outcomes for the case were evaluated regarding the degree and clinical significance of the change. The degree of psychometric change was assessed with the reliable change index (RCI; Jacobson & Truax, Citation1991). The RCI tests for the degree of change required for change to be considered reliable, rather than that expected to occur by chance. Clinically significant change (CSC, Jacobson & Truax, Citation1991) occurs when outcomes shift in classification from a “case” to a “non-case”. Simultaneous reliable and clinically significant change is a credible index of recovery in routine practice (Barkham et al., Citation2012). It was not possible to complete RCI analysis of the PJQ, due to the lack of necessary psychometric foundations.
Qualitative interview
The Change Interview (CI). The CI is a 60–90 min (10-item) semi-structured interview conducted after therapy has been completed which assesses whether change (or not) has occurred during a therapy, and then specifies what these changes were (Network for Research on Experiential Psychotherapies, Citation2003). The CI explores whether changes are associated with the therapy conducted or are more the result of processes and influences outside of the therapy (Elliott et al., Citation2001). Participants identify changes (including any changes for the worse) and then rate according to expected/surprised (1 expected change to 5 surprising change), likely/unlikely without therapy (1 unlikely without therapy to 5 likely without therapy) and the personal significance (1 not at all important to 5 extremely important). Finally, the participant is asked to consider what was helpful about therapy, and name the events which were hindering, unhelpful, negative or disappointing.
Case conceptualisation
CAT is divided into three sections; a reformulation of the patient’s presenting difficulties, a recognition phase to increase self-awareness and a final revision stage based on change work. The reformulation of the patient takes two forms; (1) a narrative reformulation and (b) a diagrammatic reformulation (this is termed a sequential diagrammatic reformulation, SDR, in CAT). The narrative reformulation is an attempt to redefine the presenting problems of the client by linking their current distress to previous (often childhood) trauma, define the relational style of the patient, the manner in which the patient may experience the therapy and also how the patient might react to the ending of the therapy. The narrative reformulation also states how the presenting problems are maintained through the actions of snags (self-sabotaging), traps (vicious circles) and dilemmas (either-or and if–then assumptions) – and these are stated in the first person. In the current case then three problems were defined. The first problem was jealousy and the trap was stated as: I have a strong fear of rejection from being a child that means I watch my partner closely for any signs that she might be rejecting me. Anything that even hints slightly at rejection from X results in me feeling really anxious, challenging X and then getting into an argument. In the heat of the argument, I can often think that X will leave me and my fear of rejection intensifies and never gets resolved. The second problem was checking and the trap was defined as: I have had to endure the painful losses of my Dad, wife and daughter and have never really processed the deep feelings of loss I feel inside. When I argue with X, then the feelings of loss are easily triggered which makes me feel abandoned and alone in my relationship again. I then need to check up on what X is doing for fear that she might leave me. Though I feel reassured in the short-term in the long-term my feelings of loss remain. The third problem was enmeshment and the dilemma was defined as: I am either wrapped up in bliss in my relationships or feel lonely on the outside and looking in.
The SDR was completed collaboratively within sessions 3 and 4 by the therapist and patient “mapping together” (Potter, Citation2020) and this entailed summarising the narrative reformulation in the form of a diagrammatic map. Therefore, the SDR contained the key states, reciprocal roles and associated procedural sequences creating and maintaining the OMJ. To aid with mapping, an initial list of dominant reciprocal role procedures (described in the patient’s own words) was created to represent the skeleton of his interaction with self and others. The patient began to use the SDR out of sessions to self-monitor and increase awareness. Treatment was theoretically grounded in the sequential diagrammatic formulation which was underpinned by CAT’s multiple self-states model (MSSM; Pollock et al., Citation2001). The various states the patient occupied were elicited using the states description procedure (SDP) approach (Ryle, Citation2007) and a self-states SDR was co-produced with the patient (Ryle et al., Citation1995). The patient named self-states that were summaries of the reciprocal role procedures and these are described below:
Self-state 1 “jealous/paranoid monster”
A1 Bullying/criticising to A2 Passive criticised victim
Self-state 2 “lost and alone”
B1 Abandoning to B2 Abandoned
Self-state 3 “egg shells”
C1 Creeping to C2 Reassured
Self-state 4 “perfect love”
D1 Perfectly loving to D1 Endlessly loved
Within the SDR procedural patterns were added which accounted for state-shifts enabling the patient to start to make sense of previously confusing state-shifting. For example, a state-shift the patient was able to notice the sharp oscillation between perfect love state and his dual fear of abandonment. This was conceptualised as a state-shift from perfect love (SS1; B2/B2) to lost and alone (SS2; C1/C2). The construction of the SDR also enabled the patient to recognise role reversals (Pollock, Citation1996). For example, in the jealous/paranoid monster state he could enact an RRP towards himself of pulling himself to pieces and being extremely self-critical after a jealous rage had settled. A healthy island state (Pollock et al., Citation2001) was added to the SDR for balance and contained the aspects of self the patient felt proud of; these were listed as being kind, honest and hard worker.
Treatment
The 8-session intervention was provided via weekly (50 min) out-patient sessions and every session was attended. The patient identified a goal for the therapy of being better able to manage jealous feelings and so to reduce the negative impact of jealousy on the quality of the relationship with their partner. The fidelity of the intervention to the CAT model was assessed using the competence in cognitive analytic therapy measure (CCAT; Bennett & Parry, Citation2004) with one session rated and scored. CCAT scores need to be >20 to represent competent CAT and the session was scored 25, indicating that the treatment was CAT and it was being competently delivered. A further index of fidelity to the CAT model is that there was a narrative reformulation, sequential diagrammatic reformulation and goodbye letters were exchanged. The change methods used in the current case can be summarised as: (1) analysis of reciprocal role enactments in the therapeutic relationship (i.e. noticing when the dyad fell into a perfect me:perfect you enactment), (2) engaging in alliance rupture-repair sequences (i.e. when the participant felt criticised by the therapist and would withdraw within sessions or excessive submit), (3) exposure to obsessive intrusions and response prevention to confirmatory compulsions, (4) exposure to a hierarchy of independent activity outside the relationship, (5) assertiveness training, (6) grieving for losses, (6) thinking before acting and (6) detailed endings work. In relation the exposure, then the patient was encouraged to stay with the intrusive jealous images, thoughts and associated feelings, rather than to avoid these (e.g. via walking away from the situational/relational cues or via distraction for imagery or intrusions). This is consistent with an exposure-based approach to anger treatment (Brondolo et al., Citation1997). A limitation on this exposure-based work was that should the participant feel that they were entering a rage state, then the exposure would be terminated. The safety plan for the intervention, therefore, consisted of two elements; management of rage states and also reduced alcohol intake (DiBello et al., Citation2014; Knox et al., Citation2007). In the final session, both therapist and participant shared “goodbye letters”. The ending was worked towards and acknowledged throughout the therapy and was an important aspect of the case because of abandoned state. The function of goodbye letters is to reflect on the ending of the therapy and what this means to the patient, name the dominant relational patterns that occurred within the therapeutic relationship, name abandonment feelings, mark progress, identify relapse prevention strategies, achievement of goals and to highlight the ongoing challenges the patient faces (Ryle & Kellett, Citation2018). The goodbye letter was therefore an attempt to help the client internalise the changes made from the CAT, through a formal statement of what had been achieved, and also what might sabotage change over the follow-up period. The goodbye letter from the therapist therefore emphasised the utility of appropriate independence, autonomy and individuation.
Results
The results are presented in three sections (1) ideographic outcomes, (2) nomothetic outcomes and (3) change interview. Graphical representations of progress on each idiographic measure according to the phase of the study are presented in . Trend lines indicate a slight improvement during the baseline for ideographic daily jealousy, being interpersonally untrusting, jealousy imagery frequency and jealousy-driven checking frequency. However, the baseline data for such measures did not increase monotonically, with an equal number of scores worsening and improving for each measure during this phase. Furthermore, there is only one scale-point difference between the first and last data points at baseline for each of these idiographic measures. Trend line trajectories during the treatment phase indicate improvement across the majority of ideographic measures, with exceptions in the overthinking and checking measures (i.e. indicating deterioration), and daily imagery frequency (which had a flat trend line). There was a large degree between day variability on ideographic intensity measures, but not on the frequency measures (imagery and checking frequency). Trend lines show improvement across the follow-up period for overthinking and couple functioning; progress was maintained over the follow-up in terms of daily jealousy and frequency of daily checking. The occasional occurrence of checking during the follow-up phase would index low levels of jealousy-fuelled checking on the partner. Trend lines suggest some deterioration during follow-up period in terms of daily anxiety, trust and image frequency. There was no evidence in the ideographic measures of any harm.
Figure 1. Ideographic measure 1: “Today I have been feeling jealous”.
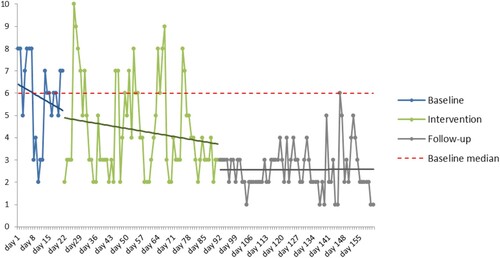
Figure 2. Ideographic measure 2: “Today I have been feeling anxious”.
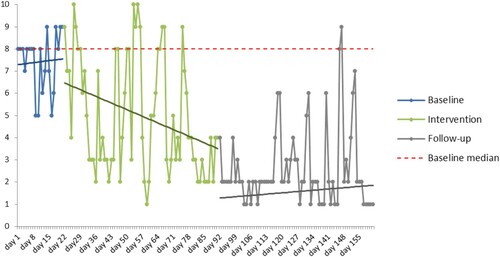
Figure 3. Ideographic measure 3: “Today I have been feeling untrusting / suspicious”.
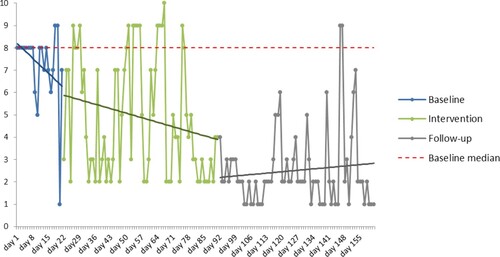
Figure 4. Ideographic measure 4: “I have been ‘over-thinking’ today”.
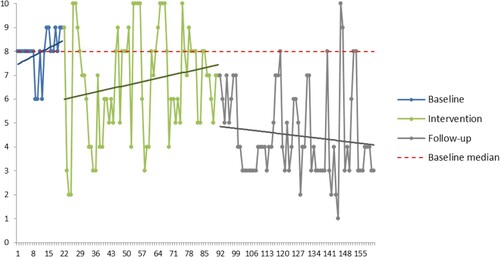
Figure 5. Ideographic measure 5: “Today, we have functioned as a couple … ”.
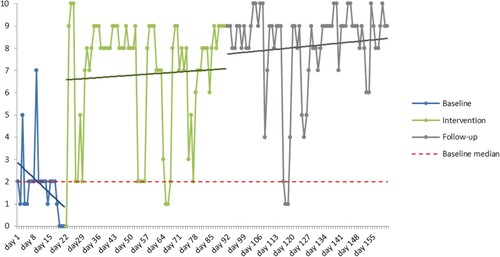
Figure 6. Ideographic measure 6: Number of images of infidelity.
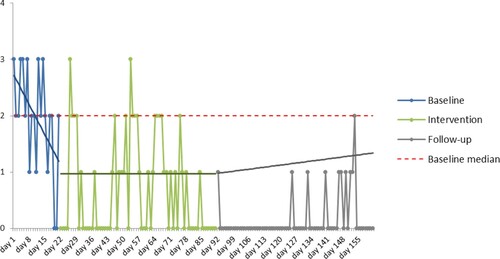
Figure 7. Ideographic measure 7: Number of times I’ve checked today.
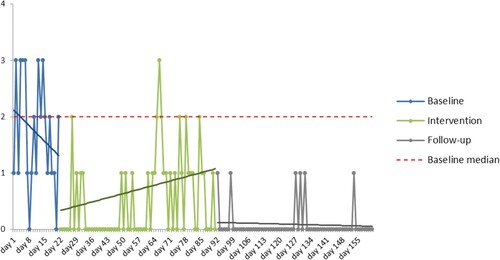
presents the mean scores on ideographic measures according to the phase of the study. There were large SDs for all measures during the intervention phase, which when considered in conjunction with visual analysis of the graphs, indicates a large degree of variability in daily subjective distress. SDs reduced across all measures during the follow-up phase indicating less variability during this phase. presents the ANCOVA, with p values added for the pairwise comparisons between treatment phases. There was a significant main effect of phase on each idiographic measure on the ANCOVA analyses indicating changes over time to jealousy, anxiety, being untrusting of the partner, overthinking, intrusive imagery, compulsive checking and the overall functioning of the couple. All the baseline to follow-up pairwise comparisons were significant.
Table 1. Grand phase summaries of the idiographic measures.
Table 2. Summary of study phase comparisons.
presents the PMD and PEM results. Interpretation of PND between baseline and treatment phases indicates that CAT had questionable treatment effectiveness on daily anxiety and the ability to function as a couple. All other ideographic measures would be interpreted as indexing an ineffective intervention. Interpretation of PND between baseline and follow-up scores indicates that anxiety, over thinking and couple functioning demonstrated a moderately effective intervention, with the remaining measures demonstrating an ineffective intervention. Interpretation of PEM between baseline and intervention scores indicates that all measures demonstrate that treatment has been moderately effective, with the exception of over thinking, which had questionable effectiveness. Interpretation of PEM between baseline and follow-up scores indicates that all measures demonstrated a highly effective intervention.
Table 3. PND and PEM non-overlapping data analysis results.
The outcomes on the nomothetic outcome measures are reported in . In terms of the presenting problem of jealousy, the patient was in the moderate category at assessment on the PSQ and in the mild category at follow-up. The patient had a reliable and clinically significant reduction in depression over time; depression fell from severe at assessment, to mild at treatment termination, to minimal at follow-up. In terms of psychological distress, the patient experienced a reliable and clinically significant reduction in global psychological distress (i.e. the global severity index score on the BSI) between assessment to the termination. There was a reliable improvement in interpersonal functioning between assessment and end of treatment, and assessment and follow-up. Overall, the psychometric outcomes would suggest an effective intervention, with little evidence of relapse occurring over the follow-up period.
Table 4. Nomothetic outcomes with clinical and reliable change analyses.
The Change Interview results are summarised in . The participant gave a positive account of therapy and reported that CAT had been helpful in eight different ways (i.e. understanding why, understanding consequences, reduced instigation of arguments, happier, individuation, grieving and reduced checking). Changes tended to be rated as unexpected (M = 4.5, SD = 0.53), important (M = 1, SD = 0.00) and unlikely to have occurred without therapy (M = 5, SD = 0.00). No changes for the worse as a result of the therapy were named by the participant. No adverse events as a result of therapy were noted. The Change Interview results generally reflected the ideographic and nomothetic outcomes and provide some verification that the changes observed were due to the therapy delivered, and not the action of extraneous events.
Table 5. Summary of changes noted in the change interview and associated ratings.
Discussion
The purpose of the study was to evaluate the impact of the briefest format of an already brief integrative psychotherapy (CAT) for a patient meeting criteria for OMJ via a mixed-methods single-case design. Whilst there have been previous examples of the use of single-case evaluations of different therapies with OMJ (see Dolan & Bishay, Citation1996, for an example of behaviour therapy), this is the first single-case evaluation of the effectiveness of the 8-session version of the CAT model. There was a significant effect of phase on the primary ideographic measure of jealousy. This indicates that the patient was less jealous during treatment compared to baseline and that these gains were maintained over the follow-up period. On the primary nomothetic outcome measure (PJQ), jealousy reduced from moderate at assessment to mild at follow-up with no evidence of deterioration over the follow-up period. The qualitative outcomes suggested that therapy had been experienced by the participant as helpful, and the changes achieved were attributed to the CAT and were unexpected and important to the patient. It is possible to be reasonably confident that CAT was apprpopriately delivered due to the fidelity and competency evidence presented.
In terms of comparisons with the other CAT-OMJ studies that have been conducted, the outcomes appear pretty similar. The primary nomothetic outcome measure (i.e. the Prestwich Jealousy Questionnaire) has been consistently used across all these studies. The current study indexed a shift from moderate to mild jealousy, whilst Kellett and Totterdell (Citation2013) showed a shift from severe to moderate, Curling et al. (Citation2017) from severe to moderate and Curling et al. (Citation2018) from severe to mild (case 1), severe to mild (case 2) and moderate to no jealousy (case 3). The studies combined indicate that gains in idiographic and nomothetic outcomes tend to be maintained or improved upon over the follow-up period. CAT is a therapy that pays close attention to the ending of therapy and has a specific tool of collaboratively produced “goodbye letters” that facilitate the emotional processing of the meaning of the ending to the patient to prevent relapse (Ryle & Kellett, Citation2018). This paper suggests that a positive outcome is possible when treating OMJ, even when the treatment contact is brief. Whilst some of the OMJ treatment evidence base cite shorter treatment durations (e.g. Bishay et al., Citation1989, p. 4 sessions), this is based on treatments being unrestricted in length, and is rather the count of the average number of sessions attended. Brief interventions for OMJ need to be able to deliver the clinical model and ensure a sufficient dose in order to be effective.
It is an interesting feature of the shape of change in this study that on some ideographic measures (over thinking and couple functioning), there was evidence of continued change occurring during the follow-up period. This could be seen as an example of the therapy being internalised (Salvini et al., Citation2012) and the endings work mitigating against the end of therapy being experienced by the participant as an abandonment (Ryle & Kellett, Citation2018). The possibility of this form of enactment was also highlighted in the narrative reformulation. The 8-session version of the CAT model does not have the structured follow-up of the 24-session version (i.e. follow-ups three one-month apart after the end of weekly therapy and one final session six-months after the end of weekly therapy) and so support is not offered over the follow-up period. The promise of CAT appears based on the fact that reciprocal roles are able to capture self-to-self dynamics (i.e. the relationship the OMJ patient has with themselves, to formulate low self-esteem), self-to-other dynamics (i.e. how the OMJ patient relates to their partner and the therapist, to formulate reassurance-seeking) and other-to-self dynamics (i.e. to formulate what the OMJ patient does to elicit rejection and abandonment from others and also how they experience others, including the therapist). The states approach taken here also enables the patient to recognise when they are in a jealous state, as OMJ patients often refer to their jealousy as a distinct state of mind (White & Mullen, Citation1989). The use of the multiple self-states model (MSSM; Pollock et al., Citation2001) and the states description procedure approach (Ryle, Citation2007) appear useful with OMJ, as they are able to show to the patient the defining symptomatic features of states and also how states can interlink (e.g. how a jealous rage state can, for example, create the conditions for guilt and self-harm).
Limitations
As the present study was an SCED, the generalisability of the results is questionable due to the sample size. An A/B design is seen as a quasi-experimental single-case design rather than a true single-case experimental design, due to the absence of a multiple baseline or use of a reversal design (Kazdin, Citation1978). All data was self-report which is a study weakness, as self-report outcomes are seen as less reliable and subject to social desirability (Nicklas et al., Citation2010). The follow-up period was short. There is an example of CAT OMJ outcome research in which outcomes were also collected from the partner (Kellett & Totterdell, Citation2013) and this current study would have benefitted from such methods (or addition of a clinician-rated outcome measures, such as the Yale–Brown Obsessive–Compulsive Scale; Y-BOCS; Goodman et al., Citation1989) to supplement the self-report outcomes. Indeed, the study would have been improved by contacting the partner of the patient to ensure her safety during the course of the intervention and to confirm that there were no current acts of physical violence being perpetrated towards her. It is acknowledged that the safety plan for the intervention could have been expanded to include more direct management of manipulation in the relationship, accurate labelling of aggression to include verbal and relational aggression, and increased help-seeking and support from friends.
Brody and Miller (Citation2003) have reflected on the potential ethical dilemmas when dual roles are occupied when the therapist is also the researcher, and it has been previously noted that this is often particularly unavoidable in terms of SCED research (Barlow et al., Citation2008). This dilemma was managed in the current case by the outcome data being analysed by a second independent researcher (DS). It is possible that the outcomes reported are merely an artifact and reflection of the patient’s desire to please the therapist (Braiker, Citation2001). In terms of other study weaknesses, graphing of the ideographic results would suggest that the start of the treatment phase lead to continued improvements in jealousy, being untrusting and checking, but that treatment was not effective in causing such improvement, due to baselines containing improvement trends. As such, the treatment phase caused a facilitation effect of a change process that had already started. It is worth noting that two of idiographic measures had deteriorating baselines (i.e. these problems were worsening) and then improved during the active treatment phase. An assumption of SCED is a stable baseline against which intervention (and withdrawal if used) can be compared (Barlow et al., Citation2008) and this was not the case here. Daily imagery frequency was the single idiographic measure that had a flat baseline trend. In clinical problems, such as OMJ, with marked impulsivity issues and mood variability then it is perhaps the research ideal to have stable baselines, but this is relatively clinically rare. One approach could be to assess the standard deviation per phase to assess a reduction in variability across phases and this is less reliant on baseline stability.
Originally, SCED methods were used in animal behavioural research in which it is possible to wait for a stable baseline in the laboratory, but this wait period is not ethical during psychotherapy research. In routine clinical situations, the patient requires treatment immediately when the assessment is completed (Kazdin, Citation1978). Baseline instability limits the confidence with which the improvements that occurred during treatment (and then were maintained over the follow-up period) in the primary ideographic jealousy measure can be assumed to be independent of another maturational change process. This implicates the therapeutic impact of engaging in the assessment process over the two sessions of the baseline, or possibly a mere measurement effect (Godin et al., Citation2008). The method of the study would have been improved in terms of internal validity through the use of an adjudicated hermeneutic single-case efficacy design, as this would have enabled far greater confidence in the conclusions regarding outcome able to be drawn from the study (Bohart et al., Citation2011).
Conclusion
The brief 8-session CAT intervention appeared to facilitate improvement in OMJ symptoms, as measured by psychometric and ideographic outcomes in a disorder that has traditionally been seen as difficult to treat (Cobb & Marks, Citation1979), with change being attributed to the therapy by the participant. The CAT model appeared therefore able to reformulate the OMJ rapidly and then quickly scaffold a positive relational change process. It could not be concluded with complete confidence that the CAT intervention was effective in itself, however, due to the presence of unstable baselines and the lack of a true single-case experimental design, such as a withdrawal or a cross-over design (Barlow et al., Citation2008). When conducting this type of research, the rights of the patient to decline data collection are important, the function of the data collection spelt out, consent sought and also checks be made as far as possible that the patient is accurately recording and not simply pleasing the therapist. The power dynamics of helping situations are complex (De Varis, Citation1994) and when detailed data collection is added to that context, the potential for collusion or coercion is amplified. The next research step in the evaluation of the CAT for OMJ evidence base would appear to be the use of a randomised multiple baseline design, generate lengthier follow-up, more intensive competency assessment, idiographic measurement of risk and also a collection of outcome data from partners to assess whether changes in OMJ are reciprocally experienced by others. Such evidence would serve as a valuable foundation of proof of concept to then progress onto a waitlist controlled clinical trial.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Stephen Kellett
Stephen Kellett is the Programme Director of the Clinical Associate Psychologist (CAP) clinical training programme at University of Sheffield (UK) and works clinically in Sheffield Health and Social Care NHS Foundation Trust (UK) as a Consultant Clinical Psychologist in their Specialist Psychotherapy Service.
Daniel Stockton
Daniel Stockton is a Clinical Psychologist working at the Mid Yorkshire Hospitals NHS Trust (UK) with people with long-term physical health conditions.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. American Psychiatric Publishing.
- Barelds, D. P. H., Dijkstra, P., Groothof, H. A. K., & Pastoor, C. D. (2017). The dark triad and three types of jealousy: And self and partner perceptions of relationship quality. Clinical Psychology and Psychotherapy, 14(3), 176–188. https://doi.org/10.1002/cpp.532
- Barkham, M., Hardy, G. E., & Startup, M. (1996). The IIP-32: A short version of the inventory of interpersonal problems. British Journal of Clinical Psychology, 35(1), 21–35. https://doi.org/10.1111/j.2044-8260.1996.tb01159.x
- Barkham, M., Stiles, W. B., Connell, J., & Mellor-Clark, J. (2012). Psychological treatment outcomes in routine NHS services: What do we mean by treatment effectiveness? Psychology and Psychotherapy: Theory, Research and Practice, 85(1), 1–16. https://doi.org/10.1111/j.2044-8341.2011.02019.x
- Barlow, D. H., Nock, M. K., & Hersen, M. (2008). Single case experimental designs: Strategies for studying behaviour change (3rd ed.). Allyn and Bacon.
- Batinic, B., Duisina, D., & Burisic, B. (2013). Obsessive versus delusional jealousy. Psychiatria Danubina, 25(3), 334–339.
- Beck, A. T., Steer, R. A., Ball, R., & Ranieri, W. (1996). Comparison of Beck Depression Inventories–IA and –II in psychiatric outpatients. Journal of Personality Assessment, 67(3), 588–597. https://doi.org/10.1207/s15327752jpa6703_13
- Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II. Psychological Corporation.
- Beckett, R., Tarrier, N., Intili, R., & Beech, A. (1992). The Prestwich Jealousy Questionnaire. Unpublished Manuscript, Manchester University.
- Bennett, D., & Parry, G. (2004). A measure of psychotherapeutic competence derived from cognitive analytic therapy. Psychotherapy Research, 14(2), 176–192. https://doi.org/10.1093/ptr/kph016
- Bishay, N. R., Petersen, N., & Tarrier, N. (1989). An uncontrolled study of cognitive therapy for morbid jealousy. British Journal of Psychiatry, 154(3), 386–389. https://doi.org/10.1192/bjp.154.3.386
- Bohart, A. C., Tallman, K. L., Byock, G., & Mackrill, T. (2011). The ‘research jury method’: The application of the jury trial model to evaluating the validity of descriptive and causal statements about psychotherapy process and outcome. Pragmatic Case Studies in Psychotherapy, 7, 101–144. https://doi.org/10.14713/pcsp.v7i1.1075
- Braiker, H. B. (2001). The disease to please: Curing the people-pleasing syndrome. McGraw-Hill.
- Brody, H., & Miller, F. G. (2003). The clinician-investigator: Unavoidable but manageable tension. Kennedy Institute of Ethics Journal, 13(4), 329–346. https://doi.org/10.1353/ken.2004.0003
- Brondolo, E., DiGiuseppe, R., & Tafrate, R. C. (1997). Exposure based treatment for anger problems; focus on the feeling. Cognitive and Behavioural Practice, 4(1), 75–98. https://doi.org/10.1016/S1077-7229(97)80013-2
- Calvert, R., & Kellett, S. (2014). Cognitive analytic therapy: A review of the outcome evidence base for treatment. Psychology and Psychotherapy; Theory, Research and Practice, 87(3), 253–277. https://doi.org/10.1111/papt.12020
- Chatfield, C. (2003). The analysis of time series: An introduction (6th ed.). Chapman & Hall.
- Cobb, J. P., & Marks, I. M. (1979). Morbid jealousy featuring as obsessive-compulsive neurosis: Treatment by behavioural psychotherapy. British Journal of Psychiatry, 134(3), 301–305. https://doi.org/10.1192/bjp.134.3.301
- Costa, A. L., Eglacy, C. S., Sanches, S., Tavares, H., & Zilberman, M. L. (2015). Pathological jealousy: Romantic relationship characteristics, emotional and personality aspects, and social adjustment. Journal of Affective Disorders, 174, 38–44. https://doi.org/10.1016/j.jad.2014.11.017
- Crowe, M. (1995). Management of jealousy in couples. Advances in Psychiatric Treatment: Journal of Continuing Professional Development, 1, 75–77. https://doi.org/10.1192/apt.1.3.71
- Curling, L., Kellett, S., & Totterdell, P. (2018). Cognitive analytic therapy for obsessive morbid jealousy: A case series. Journal of Psychotherapy Integration, 28(4), 537–555. https://doi.org/10.1037/int0000122
- Curling, L., Kellett, S., Totterdell, P., Parry, G., Hardy, G., & Berry, K. (2017). Treatment of obsessive morbid jealousy with cognitive analytic therapy: An adjudicated hermeneutic single-case efficacy design evaluation. Psychology and Psychotherapy; Theory, Research and Practice, 91(1), 95–116. https://doi.org/10.1111/papt.12151
- Derogatis, L. R. (1993). Brief symptom inventory: Administration scoring and procedures manual (3rd ed.). National Computer Systems.
- De Silva, P. (1987). An unusual case of morbid jealousy treated with role reversal. Sexual and Marital Therapy, 2(2), 179–192. https://doi.org/10.1080/02674658708407862
- De Silva, P. (1997). Jealousy in couple relationships: Nature, assessment and therapy. Behaviour Research and Therapy, 35(11), 973–985. https://doi.org/10.1016/s0005-7967(97)00051-x
- De Silva, D., & De Silva, P. (1999). Morbid jealousy in an Asian country: Clinical exploration from Sri Lanka. International Review of Psychiatry, 11(2-3), 116–121. https://doi.org/10.1080/09540269974276
- De Varis, J. (1994). The dynamics of power in psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 31(4), 588–593. https://doi.org/10.1037/0033-3204.31.4.588
- DiBello, A. M., Neighbors, C., Rodriguez, L. M., & Lindgren, K. (2014). Coping with jealousy: The association between maladaptive aspects of jealousy and drinking problems are mediated by drinking to cope. Addictive Behaviors, 39(1), 94–100. https://doi.org/10.1016/j.addbeh.2013.08.032
- Dijkstra, P., Barelds, D. P. H., & Groothof, H. A. K. (2010). An inventory and update of jealousy-evoking partner behaviours in modern society. Clinical Psychology and Psychotherapy, 17(4), 329–345. https://doi.org/10.1002/cpp.668
- Dolan, M., & Bishay, N. (1996). The effectiveness of cognitive therapy in the treatment of non-psychotic morbid jealousy. British Journal of Psychiatry, 168(5), 588–593. https://doi.org/10.1192/bjp.168.5.588
- Elliott, R., Slatick, E., & Urman, M. (2001). Qualitative change process research on psychotherapy; alternative strategies. In J. Frommer, & D. L. Rennie (Eds.), Qualitative psychotherapy research, methods and methodology (pp. 69–81). Pabst Science Publishers.
- Enoch, M. D., & Trethowan, W. H. (1979). Uncommon psychiatric syndromes (2nd ed., pp. 25–40). John Wright Publishing.
- Glass, G. V., Peckham, P. D., & Sanders, J. R. (1972). Consequences of failure to meet assumptions underlying the fixed effects analyses of variance and covariance. Review of Educational Research, 42(3), 237–288. https://doi.org/10.3102/00346543042003237
- Godin, G., Sheeran, P., Conner, M., & Germain, M. (2008). Asking questions changes behavior: Mere measurement effects on frequency of blood donation. Health Psychology, 27(2), 179–184. https://doi.org/10.1037/0278-6133.27.2.179
- Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R., Hill, C. L., Heninger, G. R., & Charney, D. S. (1989). The Yale-Brown Obsessive-Compulsive Scale I: development, use, and reliability. Archives of General Psychiatry, 46(11), 1006–1011. https://doi.org/10.1001/archpsyc.1989.01810110048007
- Graff-Radford, J., Whitwell, J. L., Geda, Y. E., & Josephs, K. A. (2012). Clinical and imaging features of Othello’s Syndrome. European Journal of Neurology, 19(1), 38–46. https://doi.org/10.1111/j.1468-1331.2011.03412.x
- Hart, S. (2002). Jealousy in 6-month-old infants. Infancy, 3(3), 395–402. https://doi.org/10.1207/s15327078in0303_6
- Hersen, M. (1990). Single-case experimental designs. In A. S. Bellack, M. Hersen, & A. E. Kazdin (Eds.), International handbook of behavior modification and therapy (pp. 175–210). Springer.
- Hughes, J., & Barkham, M. (2005). Scoping the inventory of interpersonal problems, its derivatives and short forms: 1988-2004. Clinical Psychology & Psychotherapy, 12(6), 475–496. https://doi.org/10.1002/cpp.466
- Intili, R., & Tarrier, N. (1998). Attentional bias in morbid jealousy. Behavioural and Cognitive Psychotherapy, 26, 323–338.
- Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59(1), 12–19. https://doi.org/10.1037/0022-006X.59.1.12
- Karunarathne, S., Liyanage, N., & Rodrigo, A. (2017). Role of negative experiences in the past relationships and adverse childhood experiences in morbid jealousy. SL J Psychiatry, 8, 20–23. https://doi.org/10.4038/sljpsyc.v8i2.8156
- Kazdin, A. E. (1978). Methodological and interpretive problems of single-case experimental designs. Journal of Consulting and Clinical Psychology, 46(4), 629–642. https://doi.org/10.1037/0022-006X.46.4.629
- Kellett, S., Boyden, P., & Green, H. (2012). Morbid jealousy; a brief clinical guide to assessment in adult mental health. Clinical Psychology, 235, 38–44.
- Kellett, S., Stockton, C., Marshall, H., Hall, J., Jennings, C., & Delgadillo, J. (2018). Efficacy of narrative reformulation during cognitive analytic therapy for depression: Randomized dismantling trial. Journal of Affective Disorders, 239, 37–47. https://doi.org/10.1016/j.jad.2018.05.070
- Kellett, S., & Totterdell, P. (2013). Taming the green-eyed monster: Temporal responsivity to cognitive behavioral and cognitive analytic therapy for morbid jealousy. Psychology and Psychotherapy: Theory, Research and Practice, 86(1), 52–69. https://doi.org/10.1111/j.2044-8341.2011.02045.x
- Kingham, M., & Gordon, H. (2004). Aspects of morbid jealousy. Advances in Psychiatric Treatment, 10(3), 207–215. https://doi.org/10.1192/apt.10.3.207
- Knox, D., Breed, R., & Zusman, M. (2007). College men and jealousy. College Student Journal, 41, 494–498.
- López, F. J. C. (2003). Jealousy: A case of application of functional analytic psychotherapy. Psychology in Spain, 7(1), 86–98.
- Marazziti, D., Consoli, G., Albanese, F., Laquidara, E., Baroni, S., & Catena Dell'osso, M. (2010). Romantic attachment and subtypes/dimensions of jealousy. Clinical Practice and Epidemiology in Mental Health, 8(1), 53–58. https://doi.org/10.2174/1745017901006010053
- Marazziti, D., Di Nasso, E., Masala, I., Baroni, S., Abelli, M., Mengali, F., Mungai, F., & Rucci, P. (2003). Normal and obsessional jealousy: A study of a population of young adults. European Psychiatry, 18(3), 106–111. https://doi.org/10.1016/S0924-9338(03)00024-5
- Margolin, G. (1981). A behavioural systems approach to morbid jealousy. Clinical Psychology Review, 1(4), 469–487. https://doi.org/10.1016/0272-7358(81)90028-3
- Marks, M., & De Silva, P. (1991). Multi-faceted treatment of a case of morbid jealousy. Sexual and Marital Therapy, 6(1), 71–78. https://doi.org/10.1080/02674659108408356
- Morley, S. (2010). Single case methods in clinical psychology: A practical guide. Taylor and Francis.
- Mullen, P. E. (1990). Morbid jealousy and the delusion of infidelity. In R. Bluglass, & P. Bowden (Eds.), Principles and practice of forensic psychiatry (pp. 823–834). Churchill Livingstone.
- Mullen, P. E., & Maack, L. H. (1985). Jealousy, pathological jealousy and aggression. In D. P. Farrington, & J. Gunn (Eds.), Aggression and Dangerousness (pp. 103–126). Wiley.
- Network for Research on Experiential Psychotherapies. (2003). Change Interview. http://www.experiential-researchers.org/instruments/elliott/hat.html.
- Nicklas, L. B., Dunbar, M., & Wild, M. (2010). Adherence to pharmacological treatment of non-malignant chronic pain: The role of illness perceptions and medication beliefs. Psychology and Health, 25(5), 601–615. https://doi.org/10.1080/08870440902783610
- Ortigue, S., & Bianchi-Demicheli, F. (2011). Intention, false beliefs and delusional jealousy: Insights from the right hemisphere for neurological patients and neurological studies. Medical Science Monitor, 17(1), 1–11. https://doi.org/10.12659/MSM.881314
- Parker, R. I., & Vannest, K. J. (2009). An improved effect size for single case research: NonOverlap of All Pairs (NAP). Behavior Therapy, 40(4), 357–367. https://doi.org/10.1016/j.beth.2008.10.006
- Pollock, P H. (1996). Clinical issues in the cognitive analytic therapy of sexually abused women who commit violence offences against their partners. British Journal of Medical Psychology, 69(2), 117–127.
- Pollock, P. H., Broadbent, M., Clarke, S., Dorrian, A. J., & Ryle, A. (2001). The Personality Structure Questionnaire (PSQ): A measure of the multiple self-states model of identity disturbance in cognitive analytic therapy. Clinical Psychology and Psychotherapy, 8(1), 59–72. https://doi.org/10.1002/cpp.250
- Potter, S. (2020). Therapy with a map – A cognitive analytic approach to helping relationships. Pavilion Publishing.
- Ryle, A. (2007). Investigating the phenomenology of borderline personality disorder with the states description procedure: Clinical implications. Clinical Psychology and Psychotherapy, 14, 329–341. https://doi.org/10.1002/cpp.543
- Ryle, A., Beard, H., & Marlowe, M. J. (1995). Cognitive analytic therapy of borderline personality disorder: Theory, practice and the clinical and research uses of the self-states sequential diagram. International Journal of Short-Term Psychotherapy, 10, 21–34.
- Ryle, A., & Kellett, S. (2018). Cognitive analytic therapy. In J. W. Livesley, & R. Larstone (Eds.), Handbook of personality disorders: Theory, research, and treatment (pp. 489–512). Guilford Press.
- Ryle, A., & Kerr, I. B. (2002). Introducing cognitive analytic therapy. Principles and practice. John Wiley.
- Salvini, A., Faccio, E., Mininni, G., Romaioli, D., Cipolletta, S., & Castelnuovo, G. (2012). Change in psychotherapy: A dialogical analysis single-case study of a patient with bulimia nervosa. Frontiers in Psychology, 3, 546. https://doi.org/10.3389/fpsyg.2012.00546
- Scruggs, T. E., & Mastropieri, M. A. (1998). Summarizing single-subject research. Issues and applications. Behaviour Modification, 22(3), 221–242. https://doi.org/10.1177/01454455980223001
- Seaman, M. (1979). Pathological jealousy. Psychiatry, 42(4), 351–361. https://doi.org/10.1080/00332747.1979.11024038
- Shadish, W. R., & Sullivan, K. J. (2011). Characteristics of single-case designs used to assess intervention effects. Behaviour Research Methods, 43(4), 971–980. https://doi.org/10.3758/s13428-011-0111-y
- Silva, J. A., Ferrari, M. M., Leong, G. B., & Penny, G. (1998). The dangerousness of persons with delusional jealousy. Journal of the American Academy of Psychiatry and the Law, 26(4), 607–623.
- Singh, S. K., Bhandari, S. S., & Singh, P. K. (2017). Phenomenology and predisposing factors of morbid jealousy in a psychiatric outdoor: A cross-sectional, descriptive study. Journal of Psychiatry and Allied Sciences, 8(2), 129–135. https://doi.org/10.5958/2394-2061.2017.00008.8
- Stieger, S., Preyss, A. V., & Voracek, M. (2012). Romantic jealousy and implicit and explicit self-esteem. Personality and Individual Differences, 52(1), 51–55. https://doi.org/10.1016/j.paid.2011.08.028
- Stravogiannis, A. L. d. C., Kim, H. S., Sophia, E. C., Sanches, C., Zilberman, M. L., & Tavares, H. (2018). Pathological jealousy and pathological love: Apples to apples or apples to pears? Psychiatry Research, 259, 562–570. https://doi.org/10.1016/j.psychres.2017.11.029
- Tarrier, N., Beckett, R., Harwood, S., & Bishay, N. (1990). Morbid jealousy: A review and cognitive–behavioural formulation. British Journal of Psychiatry, 157(3), 319–326. https://doi.org/10.1192/bjp.157.3.319
- Tate, R. L., Perdices, M., Rosenkoetter, U., Shadish, W., Vohra, S., Barlow, D. H., Horner, R., Kazdin, A., Kratochwill, T., McDonald, S., Sampson, M., Shamseer, L., Togher, L., Albin, R., Backman, C., Douglas, J., Evans, J. J., Gast, D., Manolov, R., … Wilson, B. (2016). The single case reporting guideline in behavioural interventions (SCRIBE) 2016 statement. Journal of School Psychology, 56, 133–142. https://doi.org/10.1016/j.jsp.2016.04.001
- Teisman, M. (1979). Jealousy: Systematic problem solving with couples. Family Process, 18(2), 151–160. https://doi.org/10.1111/j.1545-5300.1979.00151.x
- Wendt, O. (2009). Calculating effect sizes for single-case experimental designs: An overview and comparison. Paper presented at the 9th Annual Campbell Collaboration Colloquium, Oslo, Norway.
- Wenger, R., Roy, A. R. K., Gorman, K. R., & Ferguson, K. (2018). Attachment, relationship communication style and the use of jealousy induction techniques in romantic relationships. Personality and Individual Differences, 129, 6–11. https://doi.org/10.1016/j.paid.2018.02.033
- White, G. L., & Mullen, P. E. (1989). Jealousy: Theory, research, and clinical strategies. Guilford.