
Abstract
People with mobility impairments have reported that improving their walking is one of the most important goals of their rehabilitation. Novel robotic technologies using powered exoskeletons for the lower limb could potentially offer efficient and less labour-intensive approaches to rehabilitation with shorter recovery times. To gather users’ and carers’ perspectives of assistive device use to provide information to design personalised and safe mobility rehabilitation technology. Semi-structured interviews were carried out with people with experience of mobility impairments. Iterative data collection was used to gather information about the social phenomena surrounding patient interaction and requirements for assistive devices for mobility impairments. Cycles of continuous data collection and thematic analysis using a theoretical, semantic approach was used to develop key themes within the data. We interviewed eight people: six people with mobility impairments and two carers. We identified five main themes: relationship with assistive technology, requirements for assistive technology, function and goal setting, personal factors to assistive device use and psychosocial factors to assistive device use. There was variability in the importance placed on each theme, particularly in the trade-off between the function and comfort of assistive technology. Patients emphasised the need for assistive technology to be personalised; they reported the ability to stand, control spasticity and involvement in community roles as key goals of their rehabilitation. These results highlight the variation in requirements for assistive technology between people with different mobility impairments; individuals’ experiences are unique and future prototypes need to account for different levels of impairments and personal goals. These findings will also inform the user evaluation stage of assistive device testing. The acceptability of assistive devices is dependent upon a number of factors, including personalisation, comfort and function. Future pilot studies should gather qualitative data to determine the acceptability of actual device use.
1. Introduction
People with mobility impairments have reported that ambulatory recovery is one of the main aims of their rehabilitation therapy irrespective of the time post-injury [Citation1,Citation2]. This project addresses the growing needs of older or disabled people to live with independence and dignity. Currently, of the 11.6 million disabled people living in the UK, 6.5 million have problems with mobility. Patients utilise Assistive and Rehabilitation Technology (ART) to support and improve their mobility. ART can include walking aids, wheelchairs, hoists or any other device to assist user movement and function. The use of ART is often efficacious but not effective; for example, poor acceptability due to ill-fitting orthoses can contribute to further injury and a negative impact on patient dignity.
Studies of people living with spinal cord injury have shown the use of assistive technology to improve mobility is one of their main health and life priorities [Citation3]. Pilot studies assessing the safety and feasibility of static and ambulatory robotic technology have frequently used numerical rating scales to assess user evaluation [Citation4,Citation5]; whilst appearing to quantify acceptability to users, its apparent simplicity ignores the complexity of users’ experiences and does not conform to the latest standards of user centred design [Citation6].
Published articles describing the development of ART have frequently focussed on the mechanical feasibility of device use, rather than patient acceptability or quantifying functional improvement. Attempts to gather users’ opinions have employed informal opinion or non-validated questionnaires as methods of data collection; there is a lack of substantial qualitative data that outline the true perspective of the needs of patients using ART, which limits personalised modifications to feasibility-tested devices [Citation4,Citation7,Citation8]. Difficulties donning/doffing and adjusting devices whilst wearing, further emphasise the need for future assistive devices to be more user-friendly [Citation7].
This study is part of a wider project to explore novel materials and techniques for ART, for example wearable soft robotics, to improve patients’ mobility and independence. The study aims to address the lack in qualitative literature with a detailed exploration into patients’ and carers’ perspectives of ART as a whole, to provide clinicians and engineers with the necessary user requirements before device development. It is important to note the fundamental role of carers in facilitating the use of assistive technology in users, therefore this study has also intended to capture the prerequisites for carer use of ART also.
2. Methods
Since there is a lack of information on patient perspective of assistive technology, this study aimed to gather a rich understanding from patients who use ART and their carers through semi-structured interviews [Citation9]. An iterative study design with cycles of simultaneous collection and constant comparison of data, ensured that data were refined so to allow new and existing themes to develop [Citation10,Citation11].
2.1. Setting
This study was undertaken within the Academic Department of Rehabilitation Medicine at the University of Leeds. Interviews took place within the university premises on the campus. Where participants were unable to attend the university, due to transport limitations or other difficulties as a result of their disabilities, the study investigators attended patients’ homes to carry out interviews.
2.2. Recruitment and sampling
Maximum variation sampling, a purposive sampling technique, was used to sample a wide a range of perspectives in order to capture the broadest set of data and experiences [Citation12]. Using typical and extreme cases allows studies to establish greater insight into a social phenomenon due to different approaches [Citation12]. Any issues which are noted within the data are constantly compared with other perspectives for similarities and differences [Citation10]. This allows the researcher to better identify common themes within the sample participants’ responses. [Citation12]. This was used in combination with theoretical sampling, to allow the research team to sample those who were believed would add a new perspective to those already represented [Citation10,Citation12]. Interviews were ceased at the point of qualitative data saturation; new interviews only served to confirm rather than add to existing theories generated by past interviews [Citation10,Citation13].
The inclusion criteria for participation in the study was that patients must (i) have a disability that affects their mobility and (ii) currently be using some sort of ART to support or improve their mobility. Participants were excluded from the study if they were (i) under the age of 18, (ii) unable to consent to interview and (iii) unable to complete an interview that would last up to approximately 60 min. Carers of those who fit the eligibility criteria were also invited to be present at interview for patient support, with both participant and carer informed consent. When carers were present in the interview, they were included in the full interview and questions were addressed to both participants. Both sets of perspectives on the use of ART were included in analyses.
Participants were recruited from those who expressed interest to the study investigators, as a result numerous media campaigns over the past year; media strategies included a press release on the university website, radio appearances, local newspaper publications and regional television news appearances. The study aimed to recruit 6 to 8 participants. It was anticipated that this sample size would be necessary to achieve data saturation [Citation14].
2.3. Data collection
The study’s aim was to gather the patients’ perspectives of ART to support or improve mobility; the use of observations or questionnaires would not have gathered sufficient depth of information that spoken data would [Citation15]. Semi-structured interviews were used in order to allow co-production of knowledge; flexible interviewing helped themes to develop more naturally and allowed the participant to also lead the interview where appropriate [Citation16–18].The content of each interview and focus group was directed by a topic guide [Box], which was enhanced with additional prompts based on themes that arose from the ideas of previous participants.
2.4. Analysis
Analysis was within the interpretivist paradigm; this study used thematic analysis in order to identify and analyse patterns within the interview and focus group data [Citation9,Citation11]. The analysis method used mirrors that which has been adopted by Sansam et al. in reviewing clinicians’ perspectives of decision making [Citation15]. Organisation and initial coding of the data was performed using QSR NVivo 10 analysis software. Interviews were audio-recorded and transcribed in verbatim. Each of the interview transcripts were coded by the interviewer (LH) and reviewed by a second researcher (RJOC). In order to ensure reliability, prospective themes and sub-themes were discussed amongst the research team to review any inconsistencies in thematic structure. Codes were reviewed in a systematic fashion across the data set.
The study classified themes in accordance with the definition by Braun and Clarke [Citation11] that a theme is “something important about the data in relation to the research question, and represents some level of patterned response or meaning within the data set.” Once initial themes were noted, they were reviewed in relation to both coded extracts and the entire data set to generate a map of analysis [Citation11]. This thematic map was developed and refined in an iterative process to produce the themes and sub-themes. Each theme was refined in order to generate clear names, which described succinctly that group of data [Citation11].
2.5. Ethical considerations
This study was granted ethical approval by the University of Leeds, School of Medicine Research Ethics Committee (MREC15-078). Participants were able to withdraw prior to or during interviews and focus groups. However, due to the nature of focus groups, it would not have been possible to withdraw any contributions already provided. The nature of the project meant that questions were asked about how a participant’s health condition impacts on their life, however these were not intended to be intrusive. If participants became distressed or felt uncomfortable in discussing sensitive topics, they were given the opportunity to stop. Eligible participants provided feely given, informed consent for the collection and use of data via information sheets and consent forms following expression of interest, receipt of ethical approval.
A data management plan was written in accordance with the University data management policy, to ensure that data remained protected and confidential. Secure, encrypted university drives were used to store transcription data, whilst consent forms were kept in secure, locked cabinets within university premises. Actual, digital audio recordings were destroyed. Only LH and ROC had access to non-anonymised data. Data were anonymised such that any potentially identifiable information, such as names, places or other identifying information were removed. Sensitive personal data such as political opinions or religious beliefs were also removed. Participants’ names were removed and participants were labelled using codes.
3. Results
3.1. Participants
Of the 8 participants recruited, 4 were male and 4 were female. They were all of white, British ethnic origin. Participants’ ages ranged from 25 to 82. Interviews lasted between 33 and 59 min; one of the participants required a shorter interview due to fatigue associated with their health condition. Patients had a variety of mobility impairments; they have been categorised as done by previous clinical studies assessing rehabilitation robotics ().
Table 1. Interview participant demographic information.
3.2. Themes and Sub-themes
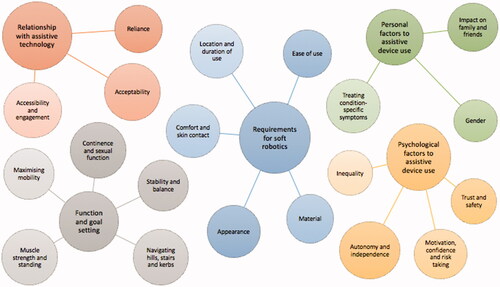
The results generated 5 themes and 20 sub-themes ().
Figure 1. Final thematic map.
3.2.1. Relationship with assistive and rehabilitation technology for mobility
3.2.1.1. Reliance
Participants expressed clear concerns surrounding the necessity of assistive technology in their lives. Whilst they felt that the use of ART was largely advantageous in maintaining function, they felt that activities of daily living were almost entirely dependent on the use of a walking stick, wheelchair or hoist in those with more severe impairments:
“People are telling me to get a wheelchair and scooter…I said it won’t be helpful if I get one of them. I won’t get back out.”
Patients were also apprehensive about the idea that over-reliance could result in a “point of no return”; they worried that they may become so reliant on the help of aids that their body would lose the ability carryout certain manoeuvres. Patients with declining lower limb function, who relied on the ability to stand up or push themselves with their upper limbs, were also apprehensive over losing upper limb function.
3.2.1.2. Acceptability
Patient and carers provided differing perspectives on the tolerability of device use, and described a tension between the acceptability of ART in their lives which is in tension with the increase in accessibility provided by the technology. Most users were so reliant on their aids that they expressed a disdain. Carers often felt like the use of devices represented a loss of control:
“We’ve tried out various different slings ‘cause when that hoist first arrived I felt very antagonistic towards it. I felt it was a labelling moment…a loss of control for both of us.”
“Any possibility of an assistive device that might in the future increase my mobility and confidence and remove the need for aids yeah I would welcome with open arms”
3.2.1.3. Accessibility and engagement
Some participants spoke of ART in a positive light; aids facilitated them in partaking in community engagement, social occasions and general activities of daily living:
“The advantages of the wheelchair, of course, [are] that I can go to places and meet people and attend activities, which would otherwise be ruled out because of distances involved as far as the sticks are concerned”
Comparisons were made between different assistive aids; users preferred to have the comfort of wheelchairs for longer distances, whilst sticks facilitated mobility in more compact environments.
Users identified the need for a device to be operated with one hand as a key design feature, in order to be accessible to a wider audience, such as those with hemiparesis. They also pointed out that this would facilitate them in using their devices, whilst being able to do other things such as shake someone’s hand, hold a cup of tea or a baby.
3.2.2. Requirements for assistive and rehabilitation technology for mobility
3.2.2.1. Appearance
Participants were often concerned over public opinion of ART, but not the appearance of their disability. Users did not require robotics to make their gait appear more ‘normal’, but preferred the use of something inconspicuous. Many called for a garment, which could be worn underneath normal clothing:
“I wouldn’t want it to be obvious because you don’t’ want people looking and staring at you thinking [they’ve] got those special trousers on.”
They highlighted the trade-off between a device that was discrete enough to avoid judgement, but also something was obvious enough for people around them to provide an alert to others around them to give them more time or space. Ultimately, participants expressed the superiority of function over appearance.
3.2.2.2. Ease of use
Both users and carers alike stressed the amount of time it takes to get dressed and fit to ART. They articulated a need for something which is easy to don and doff independently; they emphasised how dexterity issues make ART difficult to use in the bathroom specifically. A carer highlighted the fact that they themselves would have to find them easy to use:
“You know, my own mobility will change…so need to kind of look at how the carer could get those trousers [one type of ART mentioned by this participant during the interview] on when the person being cared for would not be able to do what we can do.”
Participants stressed the need for something which is easy to carry, not too heavy to wear and pack whilst travelling. The majority of participants prioritised function over device weight:
“The clothing which polar explorers wear… to enable them to survive temperatures of -32 °C - if they can wear it so can I.”
With regard to the incorporation of a battery pack, participants talked about the trade-off between something which required less power for regular every day-use, and more power for one-off, longer distances.
3.2.2.3. Material
Participants described a variety of materials as appropriate, ranging from “lycra that stretches” and “neoprene” to “Velcro” and “football shirts”. It became apparent that ART needs to be flexible to participants’ own body shapes. After describing the capability of the technology, participants agreed that they would like material to replace where body profile has been lost.
The majority of users thought the trousers should be washable; either something that was self-cleaning or a device that comprised an inner and outer layer, a removable washable part inside the robotic component.
3.2.2.4. Comfort and skin contact
There were contrasting views regarding the need for comfort. Participants with less severe mobility impairments prioritised comfort over function. The use of electrical stimulation was generally accepted, although some who had used FES in the past found it uncomfortable:
“You always socialise [and] make your own terms with discomfort”
“If it worked but it was uncomfy, I wouldn’t wear it.”
Many users raised the issue of whether the skin-contact garment would be too warm. They expressed the need for it to regulate temperature or be breathable in order to control sweating.
Participants varied in terms of sensory ability; those lacking temperature perception required help with that. Others preferred something which was heated, to combat the cold sensations associated with their condition.
3.2.2.5. Location and duration of use
Different participants described a need for soft robotics at different times during the day; generally it was agreed that users would need some time not wearing them, such as sitting down and relaxing in the house:
“I’d use it all the time. I’d use it everywhere.”
Some participants expressed a specific need for them during the night, to keep them in one position whilst sleeping.
3.2.3. Function and goal setting
Based on the contexts and requirements described above by participants, a varied spectrum of goals that ART might help participants to achieve were identified. These were associated with increasing function – some were specific and high-achieving, others were more general:
“I set myself very high goals…to walk into Marks and Spencer’s without any aids, buy a shirt and walk out again.”
3.2.3.1. Continence and sexual function
Patients and carers both described the need for assistance with personal functions. Many required help with getting to the toilet unassisted:
“I could envisage a moment where we could return to, with help, being able to stand and swivel and sit on the loo, that’d be number one. Stand. Swivel. Sit.”
Others expressed the loss of sexual intercourse in their lives due to their partner’s disability. Carers identified how a soft robotic device might assist in providing comfort and support during sex:
“I would like to be able to make love to my wife again.”
3.2.3.2. Stability and balance
Users placed emphasis on the essential role of ART in providing stability and minimising falls. The majority of participants needed a device to counteract problems with balance and a fear of falling. Patients described a device that could either prevent harm associated with falls or the fall itself:
“I’m walking a bit like a ballet dancer across the surface ready to put the sticks down if I felt I was going”
Some participants described a need for trunk and postural stability as well as something for the lower limbs, to help with fatigue associated with remaining upright.
3.2.3.3. Navigating hills, stairs and kerbs
The majority of participants described difficulty navigating inclines, whilst walking and also self-propelling in a wheelchair:
“Anything that’s slightly inclined becomes a problem.”
Participants identified strength, balance and foot-drop as the main barriers to being able to perform these movements. Often, attempts to manage kerbs resulted in falls:
“I tried to go up a kerb yesterday and I just didn’t make it.”
Regardless, users frequently identified these functions as “ultimately worth the risk” and felt that ART could help them achieve a “victory to walk upstairs”.
3.2.3.4. Muscle strength and standing
Participants frequently described the potential role of aART to give extra assistance and power during standing. They identified soft robotics as a better alternative to riser-recliner chairs:
“I find it difficult to get up from a chair, if this chair didn’t have arms I would not be able to get up from it”
Carers explained the difficulty in trying to get their partner up from a seat and out of bed, or transfer between chairs; users with more severe impairments often required at least two physiotherapists to assist with standing:
“So getting out of bed, everything you took for granted, or I took for granted…you’ll realise now how hard it is.”
Participants identified lack of muscle strength as a key factor in becoming fatigued; they felt that a robot would give extra power and therefore more stamina to be active for longer.
3.2.3.5. Maximising mobility
Participants identified walking further and walking faster as the main goals of their rehabilitation; users with more severe impairments welcomed the idea of a device that enabled walking at all:
“Well I really want to walk again…that’s the main thing”
Some Participants, particularly stroke survivors, pointed out the need for reference gait patterns to account for the non-affected leg as well as their paretic side; the two legs would have to work in cooperation with one another.
3.2.4. Personal factors to assistive device use
Participants emphasised the need for soft robotics to be personalised to their unique needs and impairments:
“The factor which determines the success that kind of innovative product is how deep your understanding is of the customers’ needs, in- depth understanding not just superficial. If you can transplant the technology into everyday patient experience terms you’ve got the jackpot”
3.2.4.1. Impact on family and friends
Participants described family and friends to be “very sympathetic, understanding and supportive” of their individual needs, but at times felt burdening:
“Everywhere I go I have someone with me.”
They felt that the use of an assistive soft robotic device would enable them to live more independently, without the need for someone to help them to go to the toilet, get out of bed or walk unaided:
“I’ll try anything that helps get her independence back that’s the biggest thing in the world for anyone who’s had a stroke relying on anybody else to do things for you.”
Carers identified a lack of knowledge when returning home from acute care; they found it difficult to transition to a new way of life and learn how to use ART and other devices.
3.2.4.2. Gender
Participants were vocal over the need for the smart trousers to be gender specific. They identified from a fashion and continence point of view that the device would have to come in two different forms, in addition to different sizes:
“A woman is a different shape to a guy so possibly a male version and a female version the legs could be the same it’s just the body part would have to be different.”
3.2.4.3. Treating condition-specific symptoms
Participants often voiced concerns over issues related to their health condition or disability specifically. They felt that the robotic socks could be used to help circulatory problems and treat swelling in the lower limbs and ankles. Previous use of ART often made swelling worse because it was too restrictive:
“A device that could massage for you, keeping the blood flow”
Participants also identified that soft robotics could be used to alleviate spasticity – specifically a need for something to combat involuntary movements in their limbs. They described these movements as embarrassing and uncomfortable, affecting their stability:
“We’ve tried fastening it down and if you fasten it down it literally fights it and then goes into contraction and wrestles with everything so something that could hold that in place, whether it’s a suit… would be awesome”
3.2.5. Psychosocial factors to assistive device use
3.2.5.1. Autonomy and independence
Participants gave contrasting views as to whether they would like a device that they had control of, or a device that controlled them; most agreed that it would be beneficial to have the option of both, dependent on the severity of mobility impairment.
Carers explained that “one way of [users] exerting control when [one] has not got any, is to refuse”; this is often misinterpreted by health professional as a lack of acceptability. They expressed patients need to have a choice over these sorts of opportunities:
“If you had something in built in that would correct you, then that wouldn’t stop you from doing what you wanted to do”
ART users frequently that aids could do more to facilitate their independence in terms of mobility; they described a soft robotic suit that would allow them to go out on their own.
3.2.5.2. Trust and safety
Participants gave varied opinions over whether to trust a device completely, develop trust gradually or not at all:
“[The] proof of the pudding would be in the using wouldn’t it.”
Participants frequently expressed concerns over the idea of the soft robotics failing or breaking down; they suggested that a safety mechanism would have to be in place to prevent losing control or falling over. Carers explained that they would rather trust themselves before trusting a robotic device:
“I’d be careful about making sure there’d be somebody available to be alongside her and probably for a start I’d want that to be me.”
3.2.5.3. Motivation, confidence and risk-taking
Participants generally believed that no matter how advanced the technology, the motivation to improve and see functional differences was their responsibility:
“I think overcoming limitations and using my poor old body to the maximum extension is the way to keep going it is very important to me to remain affective and stable.”
They often described ART as just as important in assisting their confidence as function; sometimes users avoided taking risks associated with mobility due to a lack of confidence:
“Mentally it gives me a feeling of confidence, and functionally its stops my foot [from] rolling…so it makes it easier for me to walk.”
3.2.5.4. Inequality
Some users described a sense of inequality surrounding their disability and use of ART in the eye of the public:
“I felt a sense of inequality not exactly embarrassment but inequality…what I was saying may have been filtered through a slight amount of cynicism and unbelief, this guy is in a wheelchair what does he know.”
They felt that the use of discrete ART may help reduce this stigma.
4. Discussion
This study has identified five main themes that are important design considerations in the development of new ART for mobility impairments: relationship with ART, requirements for ART, function and goal setting, personal factors to assistive device use and psychosocial factors in ART use. Participants frequently highlighted trade-offs in the design of an assistive device, particularly regarding whether they prioritised function over comfort or appearance. Whilst it seemed that appearance was not a limiting aspect, comfort was a crucial factor in determining user acceptability.
This study is limited in that only a small number of people could be interviewed and the ethnically homogeneous composition of the group. However, it was felt that this number of interviews was the best possible trade-off between gaining enough of a comprehensive overview of perspectives and an ethically-appropriate sample size. Single author coding was performed due to the nature of this individual project; using more than one researcher to code and analyse the data would have further minimised any potential for bias. Bias was reduced to some extent by having a second reviewer (RJOC), who reviewed the themes at certain points during data analysis.
This study has added to previous qualitative research, which have used simple questionnaires and numerical rating scales as methods of data collection. It is not possible to draw comparisons between previous qualitative studies, due to their lack of participant text and quotes. Whilst quantification of phenomena may be useful in providing a summary of qualitative information, the application solely of numbers in this type of research should be used with caution; creative triangulation methods using both types of data may have added to the understanding and validity of these complex phenomena [Citation19]. Future clinical studies with prototypes of ART should aim to quantitatively and qualitatively assess the acceptability and improvement of ambulatory function [Citation20].
The acceptability of ART is dependent upon a number of factors, including personalisation, comfort and function. Future pilot studies must seek to gather qualitative data, increasing the diversity of the participants recruited to reflect the composition of the populations that use ART to determine the acceptability of actual device use.
Acknowledgements
The research reported in this publication was supported by the National Institute for Health Research (NIHR) Devices for Dignity MedTech Co-operative. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Ditunno P, Patrick M, Stineman M, et al. Who wants to walk? Preferences for recovery after SCI: a longitudinal and cross-sectional study. Spinal Cord. 2008;46(7):500–506.
- Simpson LA, Eng JJ, Hsieh JT, Spinal Cord Injury Rehabilitation Evidence Scire Research Team, et al. The health and life priorities of individuals with spinal cord injury: a systematic review. J Neurotrauma. 2012;29(8):1548–1555.
- Cushman LA, Scherer MJ. A pilot study of perceived needs of persons with new spinal cord injury. Psychol Rep. 2002;90(3 Pt 2):1153–1160.
- Jezernik S, Colombo G, Keller T, et al. Robotic orthosis lokomat: a rehabilitation and research tool. Neuromodulation. 2003;6(2):108–115.
- Kolakowsky-Hayner SA, Crew J, Moran S, et al. Safety and feasibility of using the EksoTM bionic exoskeleton to aid ambulation after spinal cord injury. J Spine. 2013;2013:1–8.
- Culmer PR, Brooks PC, Strauss DN, et al. An instrumented Walking-Aid to assess and retrain gait. IEEE/ASME Trans Mechatron. 2014;19(1):141–148.
- Zeilig G, Weingarden H, Zwecker M, et al. Safety and tolerance of the ReWalk™ exoskeleton suit for ambulation by people with complete spinal cord injury: a pilot study. J Spinal Cord Med. 2012;35(2):96–101.
- Esquenazi A, Talaty M, Packel A, et al. The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am J Phys Med Rehabil. 2012;91(11):911–921.
- Gray DE. Doing research in the real world. London: Sage; 2013.
- Lingard L, Albert M, Levinson W. Grounded theory, mixed methods, and action research. BMJ. 2008;337(aug07_3):a567.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
- Kuper A, Lingard L, Levinson W. Critically appraising qualitative research. BMJ. 2008;337(aug07_3):a1035.
- Patton MQ. Qualitative research. New Jersey, USA: Wiley Online Library; 2005.
- Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179–183.
- Sansam K, O'Connor RJ, Neumann V, et al. Clinicians' perspectives on decision making in lower limb amputee rehabilitation. J Rehabil Med. 2014;46(5):447–453.
- King N, Horrocks C. Interviews in qualitative research. London: Sage; 2010.
- Britten N. Qualitative research: qualitative interviews in medical research. BMJ. 1995;311(6999):251–253.
- DiCicco‐Bloom B, Crabtree BF. The qualitative research interview. Med Educ. 2006;40(4):314–321.
- Malterud K. Qualitative research: standards, challenges, and guidelines. The Lancet. 2001;358(9280):483–488.
- Onwuegbuzie AJ, Leech NL. On becoming a pragmatic researcher: the importance of combining quantitative and qualitative research methodologies. Int J Soc Res Methodol. 2005;8(5):375–387.