Abstract
Purulent pericarditis is a localized infection with a thick, fibrinous hypercellular exudate and is historically associated with a high mortality. We describe a case of purulent pericarditis due to Streptococcus agalactiae (S. agalactiae) in a 30-year-old woman with sickle cell disease who presented with fever, dyspnea, and S. agalactiae septicemia. Despite timely initiation of antibiotics, she developed a large purulent pericardial effusion requiring surgical pericardiocentesis followed by a pericardial window. At 14 months follow-up, she has remained asymptomatic without sequelae. A review of the literature contained only four patients with purulent pericarditis in sickle cell patients. We discuss the unique aspects of this case in the context of purulent pericarditis in the age of modern antibiotics and hypothesize on the pathogenesis of delayed pericardial effusion after pericarditis.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Figure 1. Chest CT without contrast Day 3: bilateral lower lung airspace disease. Additionally, there are peripheral linear/wedge-shaped opacities within the right upper and lower, as well as the left lower lobes.
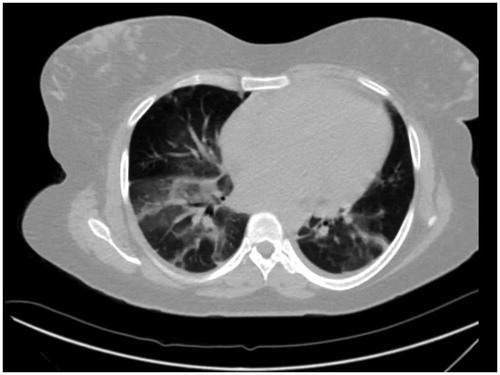
Figure 2. Chest CT with contrast Day 14: large pericardial effusion with pericardial thickening and hyper-enhancement. Bilateral pleural effusions with adjacent lower lobe atelectasis.
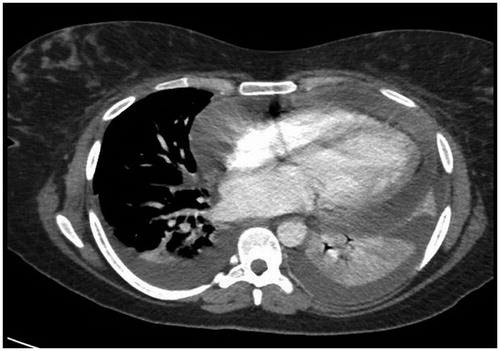
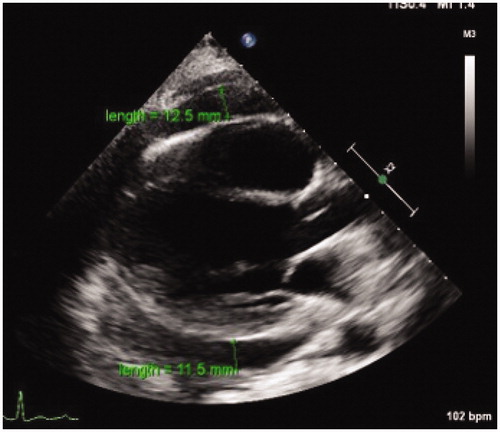
Figure 3. Trans-thoracic echocardiogram (ECHO) on Day 14: pericardial effusion.