
Abstract
The authors of this study inquire about the association between handgrip strength (HGS) and the risk of falls in physically active older women. A cross-sectional study was conducted on 135 women between 50 and 90 years of age who were referred for the follow-up evaluations of HGS using dynamometry and the Tinetti scale to determine the risk of falls. The mean age was 68.8 ± 8.5 years. A total of 31.9% of women had a high risk of falls, and 55% reported five or more falls in the past six months. In addition, our results indicated that grip strength decreases as risk of falls increases (minimal risk = 42.8, 95% confidence interval [CI]: 39.8, 45.8; moderate risk = 31.3, 95% CI: 29.1, 33.5; high risk = 21.9, 95% CI: 19.3, 24.6). It should be considered that in physically active women aged over 50 years, the grip strength could be a predictor of falls and risk of falls. Evaluation of grip strength is a low-cost type of assessment that can be included as a part of physical tests.
Since the end of the 20th century, demographic change has been characterized by a decrease in mortality and a transition of fertility, which has had a significant impact on the population’s aging process. The aging process is accompanied by sensory, neurological and musculoskeletal deterioration, which increases the risk of falls, events that are considered the second leading cause of death due to unintentional injuries (World Health Organization (WHO), Citation2017; WHO, Citation2016). According to WHO, an estimated 424,000 people worldwide die each year due to falls, and more than 80% of these deaths are reported in low- and middle-income countries. Furthermore, 37.3 million falls occur each year, the severity of which requires medical attention. Although research on the subject of falls during the aging process is significant, falls are still considered an important cause of functional loss and lower quality of life among those aged over 65 years. Authors of previous studies have estimated that the annual fall rate ranges from 33% to 42% among individuals in this age group, and 5% will require hospital care for fractures. In addition, one in three individuals will die in the course of a year after a bone lesion in such cases (Sousa et al., Citation2017; World Health Organization (WHO), Citation2016).
Therefore, it is important to identify and treat the factors that can increase the risk of falls, such as malnutrition, multimorbidity, sleep disorders, gait disturbance, functional disability, cognitive impairment, consumption of psychotropic medication, physical inactivity and sarcopenia, which is characterized by a reduction in muscle mass and function. Sarcopenia is also associated with a decrease in functional performance and an increase in morbidity and mortality in an older adult (OA) population (Cruz-Jentoft et al., Citation2010; Massy-Westropp et al., Citation2011; Rantanen et al., Citation2000).
According to the consensus of the European Working Group on Sarcopenia in Older People (EWGSOP), the measurement of handgrip strength (HGS) dynamometry is a simple and recommended method for assessing strength in the clinical practice due to its strong association with the muscle strength of the lower extremities and the cross-sectional area of the calf muscle. Despite the above, this test is not commonly included in the physical checkup of older people (Mathiowetz, Citation2002; Mijnarends et al., Citation2013).
From the literature review, it was found that older men and women with poor HGS are more likely to report fall-related fractures (Balogun et al., Citation2017; Iolascon & Moretti, Citation2018; Langeard et al., Citation2019). In addition, an association between poor HGS and an increased risk of falling as well as falls has been found in older men but not in older women (Confortin et al., Citation2018; Van Ancum et al., Citation2018). Furthermore, based on certain results, a high fall risk in older women engaged in high levels of physical activity (PA) has been found (van Nieuwpoort et al., Citation2018). Considering the aforementioned observation and the gap in the literature where the type of association between the risk of falls, falls in the last six months and grip strength in physically active OA women has been described, the present study was carried out.
Materials and methods
A cross-sectional study was conducted on 135 women aged 50–90 years out of 320 OA (both male and female) participating in an exercise program developed in Colombia. The physical exercise program is carried out twice a week for a duration of one hour. In the exercise program, the focus lies on improving strength along with bodyweight, endurance, flexibility, agility and balance. A total of 18 women were excluded; 12 of them were unable to complete the test appropriately, four did not adhere to the PA recommendations of 150 minutes/week of moderate-to-vigorous PA and two were less than 50 years old.
Data collection
Comprehensive evaluations were carried out at the senior centers by two professionals, a physiotherapist and a physical educator, with at least 12 years of experience. The recruitment of participants was done from August to November 2018.
Handgrip strength
The HGS assessment expressed in Kg/F was performed using the Jamar dynamometer (Hydraulic Hand Dynamometer), which is currently the gold standard for measuring maximal grip strength, and a range of 5.0 to 6.5 kg may be reasonable estimates of clinically important changes in grip strength (Bohannon, Citation2019b; Bohannon et al., Citation2006). The participants were asked to stand with the shoulders adducted and without rotation, with the elbow flexed at 90°, with the forearm and wrist in neutral position with an extension between 0° and 30° and with an ulnar deviation of 0°–15°. A total of three maximal contractions were made in each hand, and the highest of the three attempts was recorded. Both hands were measured alternately, with a break of approximately one minute between measurements of the same hand (Bohannon, Citation2019; Bohannon et al., Citation2006). Based on previous studies, the maximum value achieved using either hand was used as a summary measure of the isometric strength of the hand and forearm muscles of a person (Roberts et al., Citation2011; Steiber, Citation2016).
Anthropometric measurements
Weight (kg) was measured using a digital scale with an accuracy of 100 grams (Tanita 679 F), and height (m) was measured using a stadiometre (SECA 213). Body mass index (BMI) was calculated as follows: BMI = weight/height2.
Questionnaires
The sociodemographic and clinical questionnaire was used to gather personal and clinical information, including age, education, marital status, occupation, socioeconomic status, presence/absence of current physical disability and cardiovascular risk factors such as acute myocardial infarction, smoking, high blood pressure, history of cardiovascular death in any first-degree relative, dyslipidemia, diabetes and high-density lipoproteins greater than 60 mg/dl (Riebe et al., Citation2018). In addition, participants were asked about the number of falls in the last six months, and the response was categorized as follows: None, 1 or 2, 3 to 5 and greater than 5.
The Tinetti scale was used to determine the risk of falls. This test has a sensitivity of 70% and a specificity of 52% (Raîche et al., Citation2000). In the Colombian population, the inter- and intra-rater reliability was between 0.4–0.6 and 0.6–0.8, respectively, and the Cronbach’s alpha was 0.91 (Rodríguez Guevara & Luz Helena, Citation2012). The Tinetti scale is composed of nine items that evaluate balance and seven items that evaluate gait. The answers were rated 0 when the person was not able to perform the requested movement, 1 when the participant performed the task with compensatory movements and 2 when the person performed the task without difficulty (Di Fabio & Seay, Citation1997). The maximum score for balance was 16, and it was 12 for walking. The classification of the scale was as follows: 1) minimum risk of fall (> 25); 2) moderate risk of fall (19–24) and high risk of fall (< 19) (Di Fabio & Seay, Citation1997; Rodríguez Guevara & Luz Helena, Citation2012).
Ethical consideration
It was ensured that all procedures conformed to the ethical standards of the responsible human committee and were in accordance with the guidelines of the World Medical Association and the Declaration of Helsinki. This study was approved by the research committee of the Faculty of Physical Culture, Sport and Recreation of the University of Santo Tomas-Bucaramanga. The ethical principles of confidentiality, beneficence, non-maleficence, autonomy and justice were respected. The study objectives, design and risks/benefits were explained to the participants, and written informed consent was obtained before the evaluation.
Statistical analysis
The distribution of the data was assessed using the Shapiro–Wilk test. Since age and HGS were observed to be normally distributed, descriptive statistics were presented as means with standard deviation. The remaining categorical variables were presented as numbers of cases and percentages. The three categories of the risk of falling and the four categories of the number of falls in the past six months were used to compare the mean HGS. There were statistically significant differences among categories when the 95% confidence intervals did not overlap.
The association between HGS and high risk of falling (high vs. moderate/minimum risk of falling) as well as HGS and falls in the past six months (no fall vs. at least one fall) were evaluated using univariate and multivariate logistic regression. Manual backward selection was then used to obtain the main effects models, starting with a model where all the independent variables were included. Model fitness was assessed using the Linktest and the Hosmer-Lemeshow goodness-of-fit test. Multicollinearity was evaluated using variance inflation factors (< 5 for all variables). Using the main effects models, the adjusted predicted probabilities of high fall risk and fall in the past six months at representative values of HGS were plotted. The statistical analyses were performed using Stata 16.0 (Stata Corp LCC, College Station, TX, USA). The significance level was set to α = 0.05.
Results
The general characteristics of the sample are reported in . The mean age was 68.8 ± 8.5 years, 76.8% of the research participants were employees, 63.0% were from an urban area, 52.2% belonged to the middle/high socioeconomic strata, 49.3% reported hypertension, 31.9% had a high risk of falls and 55% reported five or more falls in the past six months.
Table 1. General characteristics of the study population.
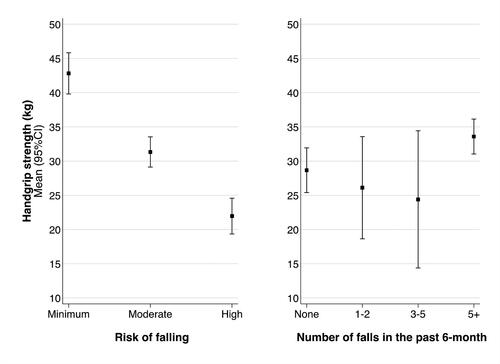
From , it can be seen that there were statistically significant differences in the mean HGS among the three levels of risk of falls. Thus, the mean HGS decreased as the risk of falls increased (minimum risk = 42.8, 95% CI: 39.8, 45.8; moderate risk = 31.3, 95% CI: 29.1, 33.5; high risk = 21.9, 95% CI: 19.3, 24.6). There were no significant differences in the mean HGS by number of falls in the past six months (none = 28.7, 95% CI: 25.4, 31.9; 1–2 falls = 26.1, 95% CI: 18.6, 33.6; 3–5 falls = 24.4, 95% CI: 14.4, 34.4; > 5 falls = 33.6, 95% CI: 31.0, 36.1).
Figure 1. Handgrip strength by risk of falling (left) and number of falls in the past six months (right).
In the univariate and multivariate analysis, HGS was found to be associated with high fall risk () and falls in the past six months (). Based on the adjusted predicted probabilities (), it was found that as HGS increases, the probability of high fall risk and the probability of falls in the past six months tends to decrease, and this trend is steeper in the case of high fall risk.
Figure 2. Adjusted predicted probability of high risk of falling (left) and of fall in the past six months (right) at representative values of handgrip strength (kg force).
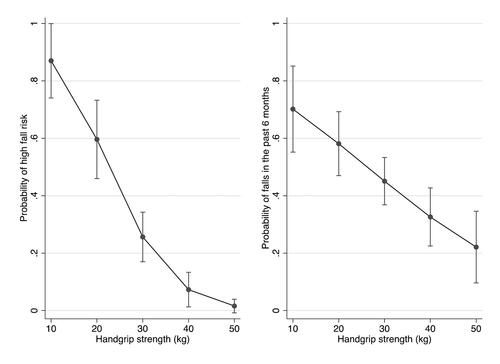
Table 2. Factors associated to high risk of falling.
Table 3. Factors associated with falls in the past six months.
Discussion
From the present study, the researchers found that in physically active women over 50 years of age, grip strength could be a predictor of falls and risk of falls.
Most previous studies were found to indicate an association between age and reduced muscle mass and function (sarcopenia) (Cruz-Jentoft et al., Citation2019; Marzetti et al., Citation2017; Pahor et al., Citation2009). The literature was found to suggest that the HGS slowly begins to decrease as age advances, obtaining a peak of greater strength between 30 and 50 years and then gradually decreasing (Cauley et al., Citation1987; Crosby et al., Citation1994). Additionally, grip strength has been mentioned as a good indicator of total muscle strength, which is key to identifying frailty and sarcopenia, conditions that have been found to compromise functionality and increase falls, fractures, institutionalisations and deaths (Cauley et al., Citation1987; Crosby et al., Citation1994; Cruz-Jentoft et al., Citation2019; Marzetti et al., Citation2017; Pahor et al., Citation2009; Studenski et al., Citation2014).
The results of the HGS obtained in the current study were above the mean of those in the meta-analysis conducted by Bohannon et al. (Citation2006), who normalized the data by age and measured the HGS with a Jamar dynamometer according to the recommendations of the American Society of Hand Therapists using relevant data from 12 studies with a total of 3,317 subjects. The differences in the results may be due to the fact that the respondents of the present study participate in programs that promote regular physical exercise.
Low grip strength has been shown to be a predictor of loss of balance and falls (Arvandi et al., Citation2018; Balogun et al., Citation2017; Bohannon, Citation2003; Citation2019a; Confortin et al., Citation2018; Giampaoli et al., Citation1999; Iolascon & Moretti, Citation2018; Langeard et al., Citation2019; Lusardi et al., Citation2017; Van Ancum et al., Citation2018), especially up to 79 years of age (Moreira et al., Citation2018). However, little information was found in the literature on this type of prediction in physically active adult women. Overall, the literature was found to indicate that physically active older women have a lower risk of falls (Sherrington et al., Citation2020). Despite the above, van Nieuwpoort et al. (Citation2018) reported that falls are more frequent in older women who are more active and those with low insulin-like growth factor (IGF-1) values, which is related to lower grip strength (van Nieuwpoort et al., Citation2018). These authors analyzed the PA in terms of time spent on PA in minutes per day during the previous two weeks without specifying whether the population participated in some physical exercise modality. In addition to ≥150 minutes of weekly PA, the literature has been found to suggest the importance of implementing multi-component programmes that target improvement, for example, of both strength and balance, which appear to be particularly effective in reducing falls in older women (Sherrington et al., Citation2020). The participants of our study were recruited from a multimodal program, which may be one of the possible reasons why their strength condition behaved as a predictor of falls.
The handgrip muscle strength test is considered an economical and simple measurement of muscle function with good psychometric properties (Beaudart et al, Citation2016). There also exists a large body of scientific knowledge where its predictive value on health outcomes among OA is described. However, its use has been limited to research studies, with little application in clinical practice (Cruz-Jentoft & Sayer, Citation2019; Sayer, Citation2010). Among the possible factors limiting the use of handgrip muscle strength tests, poor training in dynamometer use and organizational factors (e.g., lack of or limited time for patient assessment and a limited number of health care professionals) are the most important in low-resource settings (Ibrahim et al., Citation2018).
Based on our results, we recommend the routine use of HGS measurement in older women regardless of their age and PA level to identify women at great risk of poor health outcomes in a timely manner. Hence, clinicians and researchers could tailor early interventions to reduce the number of falls and their subsequent complications.
Finally, we suggest that future studies focus on evaluating the effectiveness of training and educational strategies in implementing the HGS test as a routine measurement, estimating its cost-effectiveness and identifying barriers and facilitators to its use in different contexts and population groups.
Limitations of the study
Although the Tinetti scale has been shown to have a lower predictive value compared to others of its kind (Moreira et al., Citation2018), it was used since it is the only one that has been validated in the older Colombian population (Rodríguez Guevara & Luz Helena, Citation2012). Other factors that must be considered when interpreting the results of the study are the lack of control for confounding variables such as drug intake and eating habits.
Conclusion
Although the grip strength values in the population evaluated were not found to be low, the importance of assessing HGS among physically active women over 50 years of age is perceived to identify people at risk of falls in a practical way.
Acknowledgements
The authors would like to thank the Faculty of Physical Culture, Sports and Recreation of the University Santo Tomás, for its support and backing during this present investigation. AAF would like to acknowledge the Fonds de recherche du Québec – Santé, Canada that fund her postdoctoral training program.
Disclosure statement
The authors reports no conflicts of interest in this work.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
References
- Arvandi, M., Strasser, B., Volaklis, K., Ladwig, K. H., Grill, E., Matteucci Gothe, R., Horsch, A., Laxy, M., Siebert, U., Peters, A., Thorand, B., & Meisinger, C. (2018). Mediator effect of balance problems on association between grip strength and falls in older adults: Results from the KORA-age study. Gerontology & Geriatric Medicine, 4, 2333721418760122. https://doi.org/10.1177/2333721418760122
- Balogun, S., Winzenberg, T., Wills, K., Scott, D., Jones, G., Aitken, D., & Callisaya, M. L. (2017). Prospective associations of low muscle mass and function with 10-year falls risk, incident fracture and mortality in community-dwelling older adults. The Journal of Nutrition, Health & Aging, 21(7), 843–848. https://doi.org/10.1007/s12603-016-0843-6
- Beaudart, C., McCloskey, E., Bruyère, O., Cesari, M., Rolland, Y., Rizzoli, R., Araujo de Carvalho, I., Amuthavalli Thiyagarajan, J., Bautmans, I., Bertière, M.-C., Brandi, M. L., Al-Daghri, N., Burlet, N., Cavalier, E., Cerreta, F., Cherubini, A., Fielding, R., Gielen, E., Landi, F., … Cooper, C. (2016). Sarcopenia in daily practice: assessment and management. BMC Geriatrics, 16(1), 170. https://doi.org/10.1186/s12877-016-0349-4
- Bohannon, R. W. (2003). Grip strength: A summary of studies comparing dominant and nondominant limb measurements. Perceptual and Motor Skills, 96(3 Pt 1), 728–730. https://doi.org/10.2466/pms.2003.96.3.728
- Bohannon, R. W. (2019a). Grip strength: An indispensable biomarker for older adults. Clinical Interventions in Aging, 14, 1681–1691. https://doi.org/10.2147/CIA.S194543
- Bohannon, R. W. (2019b). Minimal clinically important difference for grip strength: A systematic review. Journal of Physical Therapy Science, 31(1), 75–78. https://doi.org/10.101589/jpts.31.75.
- Bohannon, R. W., Peolsson, A., Massy-Westropp, N., Desrosiers, J., & Bear-Lehman, J. (2006). Reference values for adult grip strength measured with a Jamar dynamometer: a descriptive meta-analysis. Physiotherapy, 92(1), 11–15. https://doi.org/10.1016/j.physio.2005.05.003
- Cauley, J. A., Petrini, A. M., LaPorte, R. E., Sandler, R. B., Bayles, C. M., Robertson, R. J., & Slemenda, C. W. (1987). The decline of grip strength in the menopause: relationship to physical activity, estrogen use and anthropometric factors. Journal of Chronic Diseases, 40(2), 115–120. https://doi.org/10.1016/0021-9681(87)90062-2
- Confortin, S. C., Danielewicz, A. L., Antes, D. L., Ono, L. M., d’Orsi, E., & Barbosa, A. R. (2018). Association between chronic diseases and handgrip strength in older adults residents of Florianópolis - SC, Brazil. Associação entre doenças crônicas e força de preensão manual de idosos residentes em Florianópolis – SC, Brasil. Ciencia & Saude Coletiva, 23(5), 1675–1685. https://doi.org/10.1590/1413-81232018235.19742016
- Crosby, C. A., Wehbé, M. A., & Mawr, B. (1994). Hand strength: Normative values. The Journal of Hand Surgery, 19(4), 665–670. https://doi.org/10.1016/0363-5023(94)90280-1
- Cruz-Jentoft, A. J., Baeyens, J. P., Bauer, J. M., Boirie, Y., Cederholm, T., Landi, F., Martin, F. C., Michel, J. P., Rolland, Y., Schneider, S. M., Topinková, E., Vandewoude, M., & Zamboni, M. (2010). Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age and Ageing, 39(4), 412–423. https://doi.org/10.1093/ageing/afq034
- Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., Cooper, C., Landi, F., Rolland, Y., Sayer, A. A., Schneider, S. M., Sieber, C. C., Topinkova, E., Vandewoude, M., Visser, M., & Zamboni, M. (2019). Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
- Cruz-Jentoft, A. J., & Sayer, A. A. (2019). Sarcopenia. Lancet (London, England), 393(10191), 2636–2646. https://doi.org/10.1016/S0140-6736(19)31138-9
- Di Fabio, R. P., & Seay, R. (1997). Use of the "fast evaluation of mobility, balance, and fear" in elderly community dwellers: validity and reliability. Physical Therapy, 77(9), 904–917. https://doi.org/10.1093/ptj/77.9.904
- Giampaoli, S., Ferrucci, L., Cecchi, F., Lo Noce, C., Poce, A., Dima, F., Santaquilani, A., Vescio, M. F., & Menotti, A. (1999). Hand-grip strength predicts incident disability in non-disabled older men. Age and Ageing, 28(3), 283–288. https://doi.org/10.1093/ageing/28.3.283
- Ibrahim, K., May, C. R., Patel, H. P., Baxter, M., Sayer, A. A., & Roberts, H. C. (2018). Implementation of grip strength measurement in medicine for older people wards as part of routine admission assessment: identifying facilitators and barriers using a theory-led intervention. BMC Geriatrics, 18(1), 79. https://doi.org/10.1186/s12877-018-0768-5
- Iolascon, G., & Moretti, A. (2018). The relationship between serum IGF-1, handgrip strength, physical performance and falls in elderly men and women. Journal of Laboratory and Precision Medicine, 3, 103–103. https://doi.org/10.21037/jlpm.2018.12.05
- Langeard, A., Pothier, K., Chastan, N., Marcelli, C., Chavoix, C., & Bessot, N. (2019). Reduced gait and postural stability under challenging conditions in fallers with upper limb fracture. Aging Clinical and Experimental Research, 31(4), 483–489. https://doi.org/10.1007/s40520-018-0992-z
- Lusardi, M. M., Fritz, S., Middleton, A., Allison, L., Wingood, M., Phillips, E., Criss, M., Verma, S., Osborne, J., & Chui, K. K. (2017). Determining risk of falls in community dwelling older adults: A systematic review and meta-analysis using posttest probability. Journal of Geriatric Physical Therapy (2001), 40(1), 1–36. https://doi.org/10.1519/JPT.0000000000000099
- Marzetti, E., Calvani, R., Tosato, M., Cesari, M., Di Bari, M., Cherubini, A., Collamati, A., D’Angelo, E., Pahor, M., Bernabei, R., & Landi, F. (2017). Sarcopenia: An overview. Aging Clinical and Experimental Research, 29(1), 11–17. https://doi.org/10.1007/s40520-016-0704-5
- Massy-Westropp, N. M., Gill, T. K., Taylor, A. W., Bohannon, R. W., & Hill, C. L. (2011). Hand Grip Strength: age and gender stratified normative data in a population-based study. BMC Research Notes, 4(1), 127. https://doi.org/10.1186/1756-0500-4-127
- Mathiowetz, V. (2002). Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occupational Therapy International, 9(3), 201–209. https://doi.org/10.1002/oti.165
- Mijnarends, D. M., Meijers, J. M., Halfens, R. J., ter Borg, S., Luiking, Y. C., Verlaan, S., Schoberer, D., Cruz Jentoft, A. J., van Loon, L. J., & Schols, J. M. (2013). Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. Journal of the American Medical Directors Association, 14(3), 170–178. https://doi.org/10.1016/j.jamda.2012.10.009
- Moreira, N. B., Rodacki, A., Pereira, G., & Bento, P. (2018). Does functional capacity, fall risk awareness and physical activity level predict falls in older adults in different age groups? Archives of Gerontology and Geriatrics, 77, 57–63. https://doi.org/10.1016/j.archger.2018.04.002
- Pahor, M., Manini, T., & Cesari, M. (2009). Sarcopenia: Clinical evaluation, biological markers and other evaluation tools. The Journal of Nutrition, Health & Aging, 13(8), 724–728. https://doi.org/10.1007/s12603-009-0204-9
- Raîche, M., Hébert, R., Prince, F., & Corriveau, H. (2000). Screening older adults at risk of falling with the Tinetti balance scale. Lancet (London, England), 356(9234), 1001–1002. https://doi.org/10.1016/S0140-6736(00)02695-7
- Rantanen, T., Harris, T., Leveille, S. G., Visser, M., Foley, D., Masaki, K., & Guralnik, J. M. (2000). Muscle strength and body mass index as long-term predictors of mortality in initially healthy men. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 55(3), M168–M173. https://doi.org/10.1093/gerona/55.3.M168
- Riebe, D., Ehrman, J., Liguori, G., & Magal, M. (2018). American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription (10th ed.). Wolters Kluwer.
- Roberts, H. C., Denison, H. J., Martin, H. J., Patel, H. P., Syddall, H., Cooper, C., & Sayer, A. A. (2011). A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age and Ageing, 40(4), 423–429. https://doi.org/10.1093/ageing/afr051
- Rodríguez Guevara, C., & Luz Helena, L. (2012). Validez y confiabilidad de la Escala de Tinetti para población colombiana. Revista Colombiana de Reumatología, 19(4), 218–233. http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0121-81232012000400004&lng=en&tlng=es. https://doi.org/10.1016/S0121-8123(12)70017-8
- Sayer, A. A. (2010). Sarcopenia. BMJ (Clinical Research ed.), 341, c4097. https://doi.org/10.1136/bmj.c4097
- Sherrington, C., Fairhall, N., Kwok, W., Wallbank, G., Tiedemann, A., Michaleff, Z. A., Ng, C., & Bauman, A. (2020). Evidence on physical activity and falls prevention for people aged 65+ years: systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. International Journal of Behavioral Nutrition and Physical Activity, 17(1), 144. https://doi.org/10.1186/s12966-020-01041-3
- Sousa, L. M., Marques-Vieira, C. M., Caldevilla, M. N., Henriques, C. M., Severino, S. S., & Caldeira, S. M. (2017). Risk for falls among community-dwelling older people: systematic literature review. Risco de quedas em idosos residentes na comunidade: revisão sistemática da literatura. Revista Gaucha de Enfermagem, 37(4), e55030. https://doi.org/10.1590/1983-1447.2016.04.55030
- Steiber, N. (2016). Strong or weak handgrip? Normative reference values for the german population across the life course stratified by sex, age, and body height. PLoS One, 11(10), e0163917. https://doi.org/10.1371/journal.pone.0163917
- Studenski, S. A., Peters, K. W., Alley, D. E., Cawthon, P. M., McLean, R. R., Harris, T. B., Ferrucci, L., Guralnik, J. M., Fragala, M. S., Kenny, A. M., Kiel, D. P., Kritchevsky, S. B., Shardell, M. D., Dam, T. T., & Vassileva, M. T. (2014). The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. The Journals of Gerontology: Series A, 69(5), 547–558. https://doi.org/10.1093/gerona/glu010
- Van Ancum, J. M., Pijnappels, M., Jonkman, N. H., Scheerman, K., Verlaan, S., Meskers, C., & Maier, A. B. (2018). Muscle mass and muscle strength are associated with pre- and post-hospitalization falls in older male inpatients: a longitudinal cohort study. BMC Geriatrics, 18(1), 116. https://doi.org/10.1186/s12877-018-0812-5
- van Nieuwpoort, I. C., Vlot, M. C., Schaap, L. A., Lips, P., & Drent, M. L. (2018). The relationship between serum IGF-1, handgrip strength, physical performance and falls in elderly men and women. European Journal of Endocrinology, 179(2), 73–84. https://doi.org/10.1530/EJE-18-0076
- World Health Organization (WHO). (2016, January). Falls. https://www.who.int/news-room/fact-sheets/detail/falls
- World Health Organization (WHO). (2017, January). Ageing. https://www.who.int/ageing/en/