
Abstract
Background. Vascular endothelial growth factor (VEGF) plays an important role in the development of diabetic retinopathy. Previous studies have suggested that angiotensin‐converting enzyme (ACE) inhibitor therapy may reduce vitreous VEGF concentration in diabetic retinopathy. Also HMG CoA reductase inhibitors (statins), known for their beneficial effects on vascular endothelium, might influence vitreous VEGF concentration in diabetic retinopathy.
Aim. Vitreous VEGF concentration of diabetic patients with proliferative retinopathy using statin therapy and/or ACE inhibitor therapy was studied.
Methods. Fifty diabetic patients with proliferative diabetic retinopathy, 21 diabetic control patients without proliferative retinopathy, and 43 non‐diabetic control subjects underwent vitrectomy. Vitreous samples were collected at the beginning of surgery, and VEGF concentration was assessed using a chemiluminescent VEGF immunoassay.
Results. Vitreous VEGF concentration was significantly higher in diabetic patients with proliferative retinopathy using statins than in those not using statins. The diabetic patients with proliferative retinopathy were divided into subgroups according to use of ACE inhibitor and/or statin medication. These groups did not differ significantly in concentration of vitreous VEGF.
Conclusions. Statin therapy is associated with high vitreous VEGF concentration in diabetic patients with proliferative retinopathy. In contrast to previous reports, ACE inhibitor use did not significantly influence vitreous VEGF concentration in these patients.
| Statins | = | HMG CoA reductase inhibitors |
| VEGF | = | vascular endothelial growth factor |
Introduction
In diabetic retinopathy, angiogenesis and increased permeability of retinal microvascular vessels are mediated through the action of vascular endothelial growth factor (VEGF). Increased concentrations of VEGF in vitreous reflect retinal VEGF production and are associated with proliferative retinopathy as well as non‐proliferative retinopathy. Several medical therapies for diabetic retinopathy have been investigated, but apart from tight glycaemic control and blood pressure control no preventive medication is hitherto introduced Citation1. The effect of intravitreal VEGF antibody therapy in severe diabetic retinopathy is under intensive investigation.
The renin‐angiotensin system is activated in the eye and high concentrations of angiotensin II in diabetic vitreous are associated with high concentrations of vitreous VEGF Citation2. A previous study has suggested that angiotensin‐converting enzyme (ACE) inhibitor use is associated with decreased concentration of vitreous VEGF in proliferative diabetic retinopathy in a dose‐dependent manner Citation3. However, the effect of ACE inhibitors on the progression of diabetic retinopathy is under debate, since a protective effect on developing proliferative retinopathy was found in an EUCLID Study Citation4 but not in other studies Citation5.
In addition to their cholesterol‐lowering effect, statins have beneficial effects on several pathologic conditions, including diabetes. The anti‐angiogenic effect of statins has been elucidated Citation6, but the action seems to be biphasic; high doses of statins being anti‐angiogenic and low therapeutic doses have been found to increase endothelial cell proliferation Citation7. Statins also reduce expression of VEGF through down‐regulation of several transcription factors involved in VEGF expression Citation8.
Both ACE inhibitors and statins are beneficial and widely used in diabetic patients; therefore, it is essential to investigate their action on VEGF in diabetic retinopathy. We hypothesized that vitreous VEGF concentrations are lower in the diabetic patients with proliferative retinopathy using statin and/or ACE inhibitor medication.
Key messages
Statin therapy is associated with increased vitreous vascular endothelial growth factor (VEGF) concentration in diabetic patients with proliferative retinopathy.
The potentially protective effect of statins on diabetic retinopathy in previous studies may not have been mediated through a decrease in vitreous VEGF.
Materials and methods
Subjects
The study population consisted of 50 diabetic patients with proliferative retinopathy, 21 diabetic control patients without proliferative retinopathy, and 43 consecutive non‐diabetic control subjects who underwent vitreous surgery in Oulu University Hospital, Oulu, Finland. Three diabetic patients had vitrectomy for both eyes; therefore the total number of eyes was 53 in diabetic patients with proliferative retinopathy group. The study was performed in accordance with the declaration of Helsinki, and the study design was approved by the Ethical Committee of The Northern Ostrobothnia Hospital District. All study subjects gave informed consent before the study. None of the diabetic patients or non‐diabetic control subjects had end stage renal failure.
The clinical characteristics of the non‐diabetic control subjects and diabetic patients are shown in . In non‐diabetic control subjects the indications for surgery were: retinal detachment (n = 17), vitreous opacities (n = 4), macular pucker (n = 8), macular hole (n = 5), prior vitreous haemorrhage (n = 7), and intra‐ocular lens luxation (n = 2). In diabetic patients without proliferative retinopathy, the indications for surgery were retinal detachment (n = 8), macular hole (n = 2), prior vitreous haemorrhage (n = 3), and diabetic maculopathy (n = 8). The patients were interviewed, and their medications, diabetic complications, and the age of diabetes onset were recorded. On the same day the ophthalmologist performed a routine preoperative eye examination including visual acuity, intra‐ocular pressure, and ocular fundus examination.
Table I. Clinical characteristics of diabetic patients and non‐diabetic control subjects. The data are expressed as means and standard deviation in parentheses, except for vitreous VEGF, which is presented as median and range.
Sample collection
Vitreous collection was performed at the beginning of the classic three‐port pars plana vitrectomy before starting intravitreal infusion with balanced salt solution. Undiluted vitreous samples (200–500 µL) were aspirated into a tuberculin syringe attached into a vitreous cutter and immediately refrigerated after collection. Vitreous was aliquoted, transferred into sterile tubes, and frozen at −70 °C.
Venous blood samples were obtained after an overnight fast on the first postoperative day. Plasma was separated out by centrifuging at +4 °C and stored at −70 °C for VEGF measurements.
Determination of vitreous VEGF concentration
Plasma and vitreous VEGF concentrations were assessed using a QuantiGlo Chemiluminescent human VEGF immunoassay (cat. no QVE00B, R&D Systems, Minneapolis, MN, USA). The assay was performed according to the manufacturer's instructions. The detection limit of the assay is 6.4 pg/mL, and the assay is linear up to 20,000 pg/mL. According to the manufacturer, the intra‐assay coefficient of variation was 4.0% and the inter‐assay coefficient of variation 7.9%.
Statistical analyses
The statistical analyses were carried out using SPSS version 14.0 (Chicago, IL, USA). The statistical difference between the means was assessed by independent samples two‐tailed Student's t‐test or analysis of variance (ANOVA), except for vitreous VEGF in which logarithmic transformation was used for comparison between two groups and Kruskal‐Wallis test for comparison between three or more groups. Linear regression analysis was used to calculate the effect of diabetes variables such as diabetes duration or glycaemic control on vitreous VEGF concentration. The data are expressed as means and standard deviations (SD) or medians and range (for skewed distributions). P‐values<0.05 were considered significant.
Results
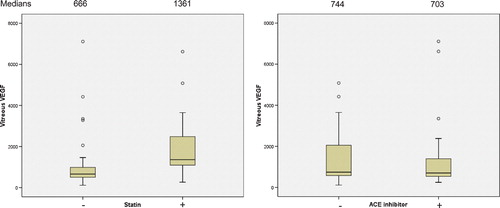
The clinical characteristics of the diabetic patients and non‐diabetic control subjects are shown in Tables and . In diabetic patients with proliferative retinopathy, there were no significant changes in fasting plasma glucose, glycated haemoglobin, diabetes duration, blood pressure, body mass index, age, or diabetes type between the users or non‐users of ACE inhibitors (ACE+ or ACE‐, respectively), or users or non‐users of statin medication (Statin+ or Statin‐, respectively) (t‐test) (data not shown). Vitreous VEGF concentration was significantly higher in the Statin+ group than the in Statin‐ group (medians 1361 pg/mL versus 666 pg/mL, P = 0.006, respectively) (), but did not differ significantly between the groups ACE+ versus ACE‐ (medians 703 versus 744, respectively, P = 0.98) (). Vitreous VEGF concentration was also higher in non‐diabetic control subjects using statins than in those not using statins (100 pg/mL versus 34 pg/mL, respectively, P = 0.001, data not shown).
Table II. Clinical characteristics of the diabetic subjects.
Figure 1 Vitreous VEGF concentration in diabetic patients with proliferative retinopathy according to statin use or ACE inhibitor use. The data are expressed as follows: black line inside the box indicating median; box between 25 and 75 percentiles; whiskers, 5 and 95 percentiles. ACE = angiotensin‐converting enzyme; VEGF = vascular endothelial growth factor.
Statin use increased vitreous VEGF levels in diabetic patients with proliferative retinopathy (). Diabetic patients without proliferative retinopathy were found to have a minor increase in vitreous VEGF concentration (), and statin users to have higher vitreous VEGF, but it did not differ significantly due to the low number of subjects (550 pg/mL, n = 11, versus 286 pg/mL, n = 10, respectively, P = 0.341) (data not shown). However, the diabetes duration and glycaemic control were significantly better in diabetic patients without proliferative retinopathy than in diabetic patients with proliferative retinopathy.
Table III. Diabetes duration, glycaemic control, blood pressure and vitreous VEGF, in non‐diabetic control subjects, diabetic patients without proliferative retinopathy, or in diabetic patients with proliferative retinopathy according to statin medication. The data are expressed as means and standard deviation for others, and vitreous VEGF as median and range. The n for vitreous VEGF is shown in parentheses. Statistical testing was done between diabetic groups with ANOVA, except for vitreous VEGF where Kruskal‐Wallis was used.
The diabetic patients with proliferative retinopathy were divided into four subgroups according to ACE inhibitor (A) or statin (S) medication: A‐/S‐, A+/S‐, A‐/S+, and A+/S+ (). The glycaemic control was slightly better, but diabetes duration longer in the A‐/S+ group, but they were not statistically significant in Kruskal‐Wallis test. The vitreous VEGF concentration was higher in groups using statins: median 2592 pg/mL in A‐/S+ group and 686 pg/mL in A‐/S‐ group (P = 0.035). Furthermore, vitreous VEGF median was 1361 pg/mL in A+/S+ group, while it was 589 pg/mL in A+/S‐ group (P = 0.045) (). The comparison between A‐/S‐ and A+/S‐ (P = 0.93) or A‐/S+ and A+/S+ groups (P = 0.309) did not reach statistical significance.
Table IV. Diabetes duration, glycaemic control, blood pressure and vitreous VEGF in diabetic patients with proliferative retinopathy in the four medication groups divided according to ACE inhibitor (A) or statin (S) medication: A‐/S‐, A+/S‐, A‐/S+ and A+/S+. The data are expressed as means and standard deviation for others, and vitreous VEGF as median and range. The n for vitreous VEGF is shown in parentheses.
The possible effect of diabetes duration or diabetes type, age, glycated haemoglobin, fasting plasma glucose, statin or ACE inhibitor use, body mass index, or blood pressure on vitreous VEGF was ruled out by performing linear regression analysis, and none of the above‐mentioned was found to have significant effect on vitreous VEGF.
Discussion
The current study shows that in diabetic patients with proliferative retinopathy using statins, the vitreous VEGF concentration was significantly higher than in those not using statin medication. This study is the first one assessing the effect of HMG CoA reductase inhibitors, statins, on vitreous VEGF concentration in diabetic patients with proliferative retinopathy, and it seems that statins have no beneficial effect in reducing VEGF production in the human diabetic eye. Previously, two clinical studies have suggested that a short‐time intervention with statins may retard the progression of diabetic retinopathy in hypercholesterolaemic patients Citation9, Citation10. However, the number of patients was low in both studies, and the study of Gordon et al. was not blinded. So far there is no clinical evidence that statins would be useful in primary or secondary prevention of diabetic retinopathy. In the light of the present results it is most likely that if a beneficial effect of statins on diabetic retinopathy would be found, it is not transmitted through a decrease in VEGF expression.
As the key regulatory element in angiogenesis, VEGF modulates endothelial cell migration and proliferation Citation11, Citation12. Though a theoretical rationale exists for statins in decreasing VEGF expression in vitro, it seems, however, that statins may even increase VEGF production in the human eye. In certain cells, statins augment VEGF expression Citation13. In a recent publication VEGF concentration in mouse retinal cell lysate was not affected by a clinically effective cholesterol‐lowering dose of pitavastatin Citation14. Statins may have biphasic effects as they seem to induce angiogenesis in vitro at low concentrations, equivalent to clinically used doses, and prevent angiogenesis at higher doses Citation6, Citation7. The enhancing effect of clinically equivalent doses of statins on angiogenesis is also present in vivo in patients with coronary heart disease Citation15. The desired statin‐induced angiogenesis in the heart would possibly be accompanied by detrimental effects in the diabetic eye. This question of potential benefit or harm of statin therapy for diabetic retinopathy patients should be solved urgently in a prospective clinical study.
Angiotensin II levels are high in the diabetic eye Citation2, and angiotensin II acts by stimulating VEGF expression and endothelial cell growth. One previous study has suggested that ACE inhibitor medication use is associated with lower concentration of vitreous VEGF in proliferative diabetic retinopathy in a dose‐dependent manner Citation3. However, in such a study the evaluation of glycaemic control is of utmost importance, since poor glycaemic control has been shown to increase VEGF expression in the diabetic retina causing blood‐retinal breakdown Citation1. The discrepancy between current results and the previous study Citation3 could probably be explained by a difference in glycaemic control between the groups in the study of Hogeboom van Buggenum et al. Citation3. They checked the glycaemic control only in a subset of patients, leaving the possibility of different glucose values in the total series. Therefore, in this study we emphasized the control of diabetes by measuring fasting plasma glucose and glycated haemoglobin in all our subjects, and the similarity in glycaemic control, duration of diabetes, or hypertension between the groups increases the reliability of our results, showing a lack of any significant effect of ACE inhibition on vitreous VEGF.
In conclusion, statin use is associated with high vitreous VEGF concentration in diabetic patients with proliferative diabetic retinopathy. However, since statins may enhance angiogenesis at clinically used doses, further studies evaluating the effect of statins and ACE inhibitors on the progression of diabetic retinopathy are warranted.
Acknowledgements
The authors wish to thank Drs Kaisu Järvinen, Ulla Lahtela, and Tapani Palosaari, who performed the vitrectomies. We are also very grateful to the staff of the Oulu University Hospital, Department of Ophthalmology for their excellent co‐operation. The skilful technical assistance of Saara Korhonen, Marja‐Leena Kytökangas, and Sari Pyrhönen is greatly appreciated. Dr Liinamaa was supported by a grant from the Eye Foundation, Helsinki, Finland and Professor Savolainen by Academy of Finland and Sigrid Juselius Foundation.
References
- Caldwell R. B., Bartoli M., Behzadian M. A., El Remessy A. E., Al Shabrawey M., Platt D. H., et al. Vascular endothelial growth factor and diabetic retinopathy: pathophysiological mechanisms and treatment perspectives. Diabetes Metab Res Rev 2003; 19: 442–55
- Funatsu H., Yamashita H., Nakanishi Y., Hori S. Angiotensin II and vascular endothelial growth factor in the vitreous fluid of patients with proliferative diabetic retinopathy. Br J Ophthalmol 2002; 86: 311–5
- Hogeboom van Buggenum I. M., Polak B. C., Reichert‐Thoen J. W., Vries‐Knoppert W. A., van Hinsbergh V. W., Tangelder G. J. Angiotensin converting enzyme inhibiting therapy is associated with lower vitreous vascular endothelial growth factor concentrations in patients with proliferative diabetic retinopathy. Diabetologia 2002; 45: 203–9
- Chaturvedi N., Sjolie A. K., Stephenson J. M., Abrahamian H., Keipes M., Castellarin A., et al. Effect of lisinopril on progression of retinopathy in normotensive people with type 1 diabetes. The EUCLID Study Group. EURODIAB Controlled Trial of Lisinopril in Insulin‐Dependent Diabetes Mellitus. Lancet 1998; 351: 28–31
- Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. UK Prospective Diabetes Study Group. BMJ 1998; 317: 713–20
- Vincent L., Chen W., Hong L., Mirshahi F., Mishal Z., Mirshahi‐Khorassani T., et al. Inhibition of endothelial cell migration by cerivastatin, an HMG‐CoA reductase inhibitor: contribution to its anti‐angiogenic effect. FEBS Lett 2001; 495: 159–66
- Weis M., Heeschen C., Glassford A. J., Cooke J. P. Statins have biphasic effects on angiogenesis. Circulation 2002; 105: 739–45
- Dichtl W., Dulak J., Frick M., Alber H. F., Schwarzacher S. P., Ares M. P., et al. HMG‐CoA reductase inhibitors regulate inflammatory transcription factors in human endothelial and vascular smooth muscle cells. Arterioscler Thromb Vasc Biol 2003; 23: 58–63
- Sen K., Misra A., Kumar A., Pandey R. M. Simvastatin retards progression of retinopathy in diabetic patients with hypercholesterolemia. Diabetes Res Clin Pract 2002; 56: 1–11
- Gordon B., Chang S., Kavanagh M., Berrocal M., Yannuzzi L., Robertson C., et al. The effects of lipid lowering on diabetic retinopathy. Am J Ophthalmol 1991; 112: 385–91
- Isner J. M., Asahara T. Angiogenesis and vasculogenesis as therapeutic strategies for postnatal neovascularization. J Clin Invest 1999; 103: 1231–6
- Kalka C., Masuda H., Takahashi T., Gordon R., Tepper O., Gravereaux E., et al. Vascular endothelial growth factor(165) gene transfer augments circulating endothelial progenitor cells in human subjects. Circ Res 2000; 86: 1198–202
- Maeda T., Kawane T., Horiuchi N. Statins augment vascular endothelial growth factor expression in osteoblastic cells via inhibition of protein prenylation. Endocrinology 2003; 144: 681–92
- Zambarakji H. J., Nakazawa T., Connolly E., Lane A. M., Mallemadugula S., Kaplan M., et al. Dose‐dependent effect of pitavastatin on VEGF and angiogenesis in a mouse model of choroidal neovascularization. Invest Ophthalmol Vis Sci 2006; 47: 2623–31
- Vasa M., Fichtlscherer S., Adler K., Aicher A., Martin H., Zeiher A. M., et al. Increase in circulating endothelial progenitor cells by statin therapy in patients with stable coronary artery disease. Circulation 2001; 103: 2885–90

