
ABSTRACT
Clinical Relevance
Vision Bus Aotearoa is a fully equipped mobile eye health clinic designed to provide a novel platform for undergraduate optometry clinical training, community eye health research and deliver services to underserved communities.
Background
Aotearoa New Zealand has inequitable access to eye health care. Vision Bus Aotearoa aims to work in partnership with communities to provide comprehensive mobile primary eye health care services while training optometry students, and integrating community eye health research.
Methods
A description is provided of the governance model which has been involved throughout the project.
Results
The process of vehicle manufacture, clinical set-up, funding models and service delivery are described. The aims of the project are detailed in terms of optometry teaching, clinical services in partnership with communities, and research integration and implementation.
Conclusion
Vision Bus Aotearoa represents a valuable opportunity to deliver mobile eye health care to historically underserved communities, enhance undergraduate optometry teaching and to provide a unique platform for community eye health research.
Introduction
A fundamental goal of Aotearoa New Zealand’s (hereafter referred to as New Zealand) Health Strategy is to ensure equitable access to health and disability care for all. New Zealand is a signatory to the United Nation’s Sustainable Development Goals, which have an overarching aim to leave no one behind.Citation1 Poor eye health has a negative impact on quality of life, reduces mobility and mental health and increases the risk of mortality.Citation2 In contrast, improving eye health contributes to advancing several Sustainable Development Goals,Citation2,Citation3 including the goal related to health and well-being. Unfortunately, there is currently a lack of policy commitment in New Zealand to improve access to eye health care.Citation4
Therefore, people in New Zealand face barriers to accessing eye health care including older/younger people,Citation5 people of Māori and Pacific ethnicity,Citation6 those with long travel distances,Citation7 and those living with disability.
Te Tiriti o Waitangi (Treaty of Waitangi) guarantees Māori the same right to health as other New Zealanders.Citation8 These rights are currently not being met including for eye health. Māori have higher rates of diabetic retinopathy,Citation9 and present for cataract surgery with worse visual acuity, and at a younger age compared to other New Zealanders,Citation6 and also experience inequitable access to pre-school vision screening.Citation10 These findings demonstrate a need to prioritise eye health services for Māori communities, and to address underlying factors such as discrimination to improve delivery of culturally safe services.Citation11 Further, the limited scope of published research in the area of access to eye health care in New Zealand indicates the need for more research.
To comprehensively address eye health care in New Zealand, the entire system needs to be considered. An eye care situational assessment in Aotearoa was completed in early 2022 using a tool developed by the World Health Organisation.Citation12 The subsequent report highlighted several areas of eye health services that require strengthening within New Zealand’s health system, with particular weaknesses identified in leadership and governance, access, financing and information.
In 2021, it was announced that the New Zealand health system would reform to two central agencies, Health NZ and the Māori health authority by July, 2022. In the previous model, there were 20 district health boards across New Zealand which independently managed regional service provision. In some district health boards there was no permanent ophthalmology service, and programmes such as diabetic retinopathy screening were delivered using different models between regions.Citation13 The current transformation of the New Zealand health system provides a valuable opportunity for eye health care to be integrated into the new structure. The New Zealand health system does not currently fund primary eye health care setting it apart from similar economies, which tend to at the very least, universally fund children, those with disabilities and older people.Citation14
The School of Optometry and Vision Science (SOVS) at the University of Auckland is the only optometry educator in New Zealand, with an annual graduating class of about 60 students who can work in Australia and New Zealand upon graduation. An ongoing objective within the SOVS strategic plan is to expand community eye health research and promote public health optometry.
Vision Bus Aotearoa is a mobile optometry clinic, recently launched by SOVS. The project has funding for five years and has three objectives:
to be a teaching platform, allowing students enrolled in their final year of the Bachelor of Optometry programme to experience working within a diverse range of clinical and community settings.
to deliver clinical services to historically underserved communities. In addition to addressing access barriers, this activity will demonstrate the scope of primary eye care services to wider communities, improve general eye health literacy and promote optometry as a career to school-aged children, particularly those of Māori/Pacific ethnicity who are vastly underrepresented in the profession
to enable community-based research, including population-based surveys, and evaluation as a model of service delivery that could be replicated in other parts of New Zealand
Mobile eye health services are common internationally, delivering vision screeningCitation15 and primary eye health care,Citation16 through to ophthalmology services including surgery.Citation17 Self-contained mobile eye health services have been used to deliver eye care in a range of settings including routine care in highly deprived urban areas,Citation18 remote communitiesCitation17,Citation19 and in disaster stricken areas.Citation20 Services have also been delivered to target specific conditions such as the Finnish glaucoma vanCitation19 and diabetic retinal screening in New Zealand.Citation21 The Fred Hollows Foundation New Zealand has a mobile eye clinic delivering eye health care in Fiji, and cataract surgery is performed on a mobile surgical bus in New Zealand.Citation22
Paediatric populations are commonly targeted through mobile eye health services. Examples include mobile eye/ear screening of Indigenous preschool children in Australia,Citation15 and provision of full eye examinations and treatment following vision screening in schools.Citation18,Citation23 Delivering care in this way has been shown to increase follow-up rates and adherence to spectacle wear in school-aged children.
Initially, Vision Bus Aotearoa is providing services across the Auckland region, home to one-third of New Zealand’s population. In the future, the intention is for services to expand into other regions, including Northland, where travel distances to optometry are the furthest in the country.Citation7
Vision Bus Aotearoa will remove financial barriers by providing all services and make spectacles available to those needing them, at no cost to the user. Such services are funded through existing government subsidies and several complementary philanthropically supported schemes running in parallel to the Vision Bus Aotearoa project.
The bus was delivered to SOVS on February 1st 2022, and officially launched on June 10th 2022. In this article, the process of delivering the bus from its inception to its completed manufacture is described. Details of the intended use of the service, and how it will be integrated into the Bachelor of Optometry curriculum as a teaching platform are given, along with an overview of how research will be integrated into the service is provided.
Methods
Governance
An advisory group was formed to manage the project, which includes academic and professional SOVS staff (research, clinical, teaching) (including JB, AC, RW, AG, VM, SD, GP), technical and information technology advisors and the donors. This group meets quarterly and initially focused on overseeing the vehicle commission/manufacture, equipment purchase, and recruitment of staff. With the vehicle now delivered, the group’s activity has shifted towards marketing, evaluation of prospective research that would use the bus and upcoming community-based activities. As the project moves towards delivering eye health services in communities, the intention is that the advisory group will primarily focus on the longer term sustainability of the initiative.
From a governance standpoint, the Vision Bus Aotearoa is considered as an offshoot of the main SOVS clinic located at the Grafton Campus of the University of Auckland.
From an administration standpoint, the Vision Bus Aotearoa project has benefited from unbudgeted support from SOVS academic and professional staff to manage and execute the project (including project management), additional as-required funding (at school, faculty and university level) to cover unanticipated costs, and on central and local faculty support to provide both staff to develop philanthropic initiatives and direct financial support, e.g. by absorbing depreciation costs for the vehicle. The importance of these elements should be considered at a planning stage, were a similar enterprise to be undertaken independently.
Results
Bus design
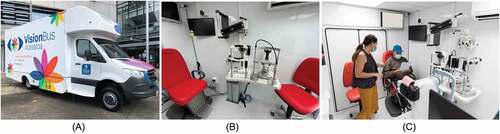
The vehicle is built on a Mercedes Springer VS30 chassis (8 m long by 2.4 m wide x 3.12 m height) () and was manufactured in Hamilton, New Zealand (Action Manufacturing Ltd). It has a rear lift to allow for wheelchair access. This model was chosen to allow adequate space for the required clinical set-up, while only requiring a standard New Zealand driving licence to operate on public roads, so permitting the optometrist to be the primary driver of the vehicle. The vehicle has a generator, and can also be externally powered where available. An air conditioning unit provides heating/cooling and fresh air circulation.
Figure 1. A: (left pane, photo credit: Rob Jacobs), external image of the Vision Bus Aotearoa, B: (middle pane), image of a vision testing lane, C: (right pane) the imaging table in the centre of the testing lanes.
Information technology capacity on the vehicle includes Wi-Fi (4 G), and a local server to store information from local computers and imaging devices. Secure backup of this local information to university storage systems is performed weekly. Clinical records are entered directly into a patient management system, and all referrals/orders/reporting is delivered electronically to maintain a paper-free environment.
The bus has two fully equipped 3 metre testing lanes () each including an electronic visual acuity chart (Frey CP-600P), phoroptor (Reichert), slit lamp (Takagi 4ZL with tonometer and teaching tube), and topographer/anterior segment imaging system (Medmont Meridia Pro).
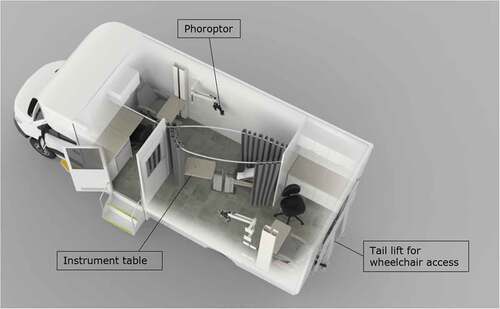
Between the two lanes there is a moveable table for shared imaging equipment (). This table can be configured to suit the patient group and at any time can hold two of: an OCT/retinal camera (Nidek RS-330), retinal camera (diabetic retinal screening grade, Canon), table-top auto-refractor/keratometer/pachymeter/non-contact tonometer (Nidek TONOREF3), ocular biometer (LenStar) and visual field machine (Humphrey Matrix 800). Fiso patient chairs and instrument tables have been fitted. A fridge is available for the storage of diagnostic pharmaceuticals ().
Figure 2. Floor plan of Vision Bus Aotearoa (image credit: Action Manufacturing).
Clinical equipment was chosen based on size, the ability to withstand motion and integration with the overall setup. Custom moulded hard covers (Roadmaster Case Ltd) were manufactured for all equipment to restrict motion whilst the vehicle was in transit.
A range of handheld and paediatric vision testing equipment is available, including iCare tonometers, pachymeters, paediatric visual acuity charts, binocular indirect ophthalmoscopes (Heine), retinoscope/ophthalmoscope (Keeler), a hand-held slit lamp (Sun Kingdom LS-1B) and hand-held auto-refractors/photo-screeners (Welch Allyn Spot photo-screener),
Dispensing of spectacles is undertaken on the bus, with dispensing equipment (Takagi vertometers, pupillometers, frame heaters and tools for adjustments) and a small range of adult/paediatric frames on display. Orders are placed electronically, and are delivered to patients at the same location as their examination, generally within two weeks.
Funding model of the Vision Bus Aotearoa project
The manufacture and refit of the vehicle, clinical equipment, vehicle running expenses (fuel, servicing, maintenance) and core staffing costs were funded by a large philanthropic donation to SOVS ().
Table 1. Costs ($NZ) of the Vision Bus Aotearoa (in kind costs not included). Annual costs have been averaged over the 5-year project term.
The core staff include:
An optometrist employed as a Professional Teaching Fellow with primary responsibility of teaching of optometry students including the supervision of clinical care, and primary oversight of the service delivery.
A project coordinator responsible for scheduling bus activities and day-to-day administration and reporting of bus service.
A Professional Teaching Fellow (education focused clinical academic): Kaiāwhina. This is a holistic Māori health role offering cultural support to the project and associated communities. Their primary responsibility is to ensure that Māori health and appropriate practice is at the centre of how the service is delivered.
Support for academic, technical, marketing, fleet management and IT staff/services is funded through the University of Auckland, as is a part-time project manager and provision of parking, security and depreciation for the vehicle and information technology infrastructure.
Funding model of service delivery
All services and appliances delivered on/through the bus project are provided at no cost to those using the service. Where subsidies are available to the patient (e.g. through limited government subsidies (children under 16, https://enable.co.nz/services/subsidy-funding-services/childrens-spectacle-subsidy/), Māori health funding, private medical insurance or employer contributions these will be claimed by the Vision Bus Aotearoa project to accurately evaluate this service and the unmet need of those using it.
Where research projects are involved, research funding may be required to staff the service; the expectation is that future projects will budget for Vision Bus Aotearoa costs at the grant proposal stage to allow for accurate costing of a contribution towards running costs.
Following the official launch of the bus in June 2022, further donations will be sought to expand the services the bus can provide. The longer term aspiration is to acquire funding to extend the project beyond 5 years.
Teaching and clinical activities
To achieve the teaching objective, final year (Part V) BOptom students will be rostered to deliver eye care under the supervision of a registered optometrist. Students will complete an associated e-log with ICD-10 coding to describe clinical exposures.
The bus will provide clinical services 4 days per week to allow 1 day for servicing of the vehicle and administration tasks for the optometrist. Two students will be scheduled to undertake supervised examinations each day, with an additional student scheduled for imaging/dispensing activities when available. Students will each complete up to 6 full eye examinations per day. Scheduling capacity will be limited by community organisation hours (e.g. schools have a 6 hour day), and space limitations within the vehicle.
Partnerships with local providers will be established, including clear referral pathways with public ophthalmology services where further assessment is required.
Research activities
Primary eye health services are almost exclusively provided in the private sector in New Zealand, with historically little support (at a health policy level) for alternative models to improve access for underserved groups.Citation24 One of the reasons for this lack of policy support is the absence of population-level data on eye health or vision impairment, which would likely uncover disparities similar to those observed in an Australian national eye health survey in 2016.Citation25
Vision Bus Aotearoa will provide a platform to perform population-based eye health surveys, allowing mobile data collection in a range of regional communities.
A lack of data also limits our ability to identify unmet need in paediatric groups, particularly for conditions with variable population prevalence and increasing incidence such as myopia. New Zealand is also known to have a high prevalence of keratoconus, with recent evidence suggesting that Māori adolescents have a higher prevalence of this condition compared to other New Zealanders.Citation26 There is currently a lack of coordination between paediatric eye health services, with children anecdotally not accessing care recommended following vision screening. Integration of school-based eye care is currently a research theme within SOVS, and the Vision Bus Aotearoa allows us to test the efficacy of delivering comprehensive eye care on site at the child’s school.
Ongoing evaluation of the bus as a model to deliver accessible community-based eye care will be continuing and will include assessment of health economic aspects of eye health care delivery to inform policy change. Stakeholder evaluation will also be collected throughout the project to gain feedback about the model from the perspective of users (optometry students, patients and their families, partner organisations).
Community partnership
SOVS maintains a long-standing teaching-led school vision screening programme that tests up to 4,500 children annually (school years 1–13) in low-mid decile schools (a multi-factor measure which indicates the school roll consists of families living with higher levels of deprivation). Approximately 17% of children fail the vision screening, primarily due to refractive error.Citation27 A key partnership for Vision Bus Aotearoa will be to provide comprehensive eye examinations at schools for children that have failed a vision screening.
Partnerships will also be established with Māori health providers such as marae (traditional Māori meeting house) based general practitioners to deliver services to people with vision/eye health concerns identified by primary health providers. In time the intention is to also establish partnerships with residential care facilities.
Another community partnerships is with the Mangere Refugee Resettlement Centre based in South Auckland, where refugees arriving in New Zealand will spend time before settling around the country.
Promotion of optometry as a future health profession choice
An advantage of school visits being the key activity for Vision Bus Aotearoa is that it allows a diverse range (age, location) of school students to learn more about tertiary study, particularly optometry and allied health. Internationally, studies have demonstrated that schools in areas of high-socioeconomic deprivation tend to struggle with providing opportunities for students to experience health-related work experience placements.Citation28
A parallel project involving Vision Bus Aotearoa aims to increase exposure to optometry among Māori and Pacific students by partnering with a group of Auckland high schools which have traditionally had low rates of tertiary enrolments. A group of senior students will be offered an opportunity to get involved with school vision screening, have an eye examination and hear more about the role of optometrists from a range of alumni in New Zealand and around the Pacific.
Discussion
Vision Bus Aotearoa is a direct response to the inequities in New Zealand eye health care. It is recognised that the project is insufficient to solve this problem in isolation from other efforts to address the large unmet need across the country. Because this project is also a teaching platform, the expected capacity each year is up to 3,000 full eye examinations. The number of partnerships with community providers established will be rationalised to retain the quality of the service. With time and additional funding for staff, the bus may be used in the evening/weekend to expand the services provided. A further benefit of the Bus is to raise awareness of (a) the services available (to community members) and (b) the unmet need for services, and potential solutions (in terms of an innovative service delivery model) to policy-makers.
Vision Bus Aotearoa will provide primary eye care within schools. Evidence is increasingly demonstrating the value of delivering eye care in partnership with schools,Citation29 and the low adherence with community provider referrals following vision screening at schools.Citation30 Referral pathways and follow-up care will need to be established including for myopia management, contact lens fitting and specialised assessment of ocular health, binocular vision or formal diagnosis of colour vision deficiency.
Where clinics are delivered to older groups of adults with higher levels of required follow-up care, referral to local providers or the University clinic in central Auckland will be required. A known barrier to accessing services is the lack of optometry providers in some communities,Citation7 meaning relationship building with local general practice clinics will be essential to ensure that referral pathways are appropriate.
Vision Bus Aotearoa provides a reference design and costing for others considering a mobile eye health service. Other potential mobile providers would be the public health system, private ophthalmology, charitable eye heath organisations, optometrists delivering services with targeted social impact (such as https://mrfoureyes.co.nz/) or larger optometry chains wanting to extend practice locations. Mobile eye health services could be targeted towards providing certain services; particularly in remote communities. Previously, this model has been successful for mobile diabetic retinal screening in Northland.Citation21
An important determinant in people accessing eye care is being able to do so in a way which is culturally safe; putting the onus on the healthcare provider to ensure they are sufficiently competent to deliver appropriate care. Training in cultural safety is essential so healthcare practitioners are aware of their own responsibilities in identifying ways in which their practice may make patients feel comfortable while engaged with their service.Citation31 Embedding self-reflection in undergraduate training programmes is a way of preparing clinicians for future practice. The bus will expose undergraduate optometry students to a diverse range of clinical and community settings, and allow them to experience delivering eye care in a way which is designed to remove access barriers (published 6 Nov).Citation32 Of particular importance will be highlighting the obligations and benefits of partnership with Māori community providers. This aligns with the University of Auckland’s strategic plan for 2025 and vision for 2030; Taumata Teitei.Citation33 This plan highlights the need for partnership with communities, creating a future ready workforce and research-informed curriculum.
Vision Bus Aotearoa presents a unique opportunity to prepare future New Zealand optometrists for a career in primary eye health care that encompasses both community partnerships and evidence-based practice. With ongoing advances in scope of practice for optometrists, and an increasing acknowledgement of the central role optometry must play in collaborative eye health care, there has never been a better time to explore different models of practice. The Vision Bus Aotearoa objectives of teaching, community partnership and research offers the chance to highlight the right of all New Zealanders to experience optimal eye health.
Acknowledgments
We thank Peter and Rae Fehl, the donors that made the Vision Bus Aotearoa a reality. Also thanks to Helen and Barbara Blake for their donation, allowing the formation of the community spectacle fund. We wish to acknowledge Kumuda Setty and Essilor, for their ongoing support and provision of lenses and fitting services. We gratefully acknowledge Sunix Vision for providing trial software and support, Tim Way from OIC and Robert Nyenkamp from Optimed NZ for their major contribution to the design and for advice on instrumentation, to Andrew Cho, digital solutions architect and to Sam Elias for IT support. Thank you to Action Manufacturing for providing a collaborative approach to vehicle manufacture. We also acknowledge the numerous other people from within SOVS and around the University that support this project, particularly Johanna Beattie for her ongoing involvement across the initiative. Thanks to Amie Straker for her support with project management. Thanks to Telusila Vea for her continued support as a community coordinator, and Kristine Hammond/Emily Benefer for their ongoing support with dispensing. Finally, many thanks to Fionna Urlich for her role in coordinating all aspects of the Vision Bus Aotearoa and providing a high level of support to the staff involved.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Trade NZFAa. Sustainable development goals. [cited 2022 April 08]. Available from: https://www.mfat.govt.nz/en/peace-rights-and-security/our-work-with-the-un/sustainable-development-goals/#bookmark1 .
- Burton MJ, Ramke J, Marques AP, et al. The lancet global health commission on global eye health: vision beyond 2020. Lancet Glob Health 2021 Feb 20; 9:e489–551. DOI:10.1016/S2214-109X(20)30488-5.
- Zhang JH, Ramke J, Jan C, et al. Advancing the sustainable development goals through improving eye health: a scoping review. Lancet Planet Health 2022 Feb 28; 6:e270–280. DOI:10.1016/S2542-5196(21)00351-X.
- Silwal P, Watene R, Cowan C, et al. Eye care in Aotearoa New Zealand 2022: Eye care situation analysis tool (ECSAT). Auckland: University of Auckland; 2022. DOI:10.17605/OSF.IO/R75ZS.
- Findlay R, Black J, Anstice N, et al. The prevalence of refractive error and visual impairment among New Zealand children in a community with significant socioeconomic disadvantage: is current preschool vision screening effective? N Z Med J 2020 April 24; 133:33–41.
- Chilibeck C, Mathan JJ, Ng SG, et al. Cataract surgery in New Zealand: access to surgery, surgical intervention rates and visual acuity. N Z Med J 2020 Oct 30; 133:40–49.
- Ramke JZ, Wilson J, Lee O, et al. Geographic access to eye health services in Aotearoa New Zealand: which communities are being left behind?. Submitted to CXO for special edition (public health optometry and indigenous eye health). 2022.
- Reid P. Structural reform or a cultural reform? Moving the health and disability sector to be pro-equity, culturally safe, Tiriti compliant and anti-racist. N Z Med J 2021 May 21; 134:7–10.
- Papali’i-Curtin AT, Dalziel DM. Prevalence of diabetic retinopathy and maculopathy in Northland, New Zealand: 2011-2012. N Z Med J 2013 Oct 26; 126:20–28.
- Findlay R, Hamm L, Anstice N, et al. Vision screening in New Zealand pre-school children: Is it equitable?. J Paediatr Child Health. 2021 Oct; 57 (10):1594–1599. DOI:10.1111/jpc.15548. Epub 2021 May 10. PMID: 33969914.
- Espiner E, Paine SJ, Weston M, et al. Barriers and facilitators for Maori in accessing hospital services in Aotearoa New Zealand. N Z Med J 2021 Dec 03; 134:47–58.
- World Health Organisation. Eye Care Situation Analysis Tool (ECSAT). Geneva; 2019.
- Chang LY, Lee AC, Sue W. Prevalence of diabetic retinopathy at first presentation to the retinal screening service in the greater Wellington region of New Zealand 2006-2015, and implications for models of retinal screening. N Z Med J 2017 Feb 17; 130:78–88.
- Goodman LB, Tousignant JM, Keay B, et al. How should NZ implement the “Eye Health Check” for older adults to maximise the potential to reduce vision impairment? A scoping review. 2021.
- Elliott G, Smith AC, Bensink ME, et al. The feasibility of a community-based mobile telehealth screening service for aboriginal and torres strait islander children in Australia. Telemed J E Health 2010 Nov 03; 16:950–956. DOI:10.1089/tmj.2010.0045.
- Satto LH, Meneghim R, Hirai FE, et al. Impact of a mobile unit on access to eye care in Sao Paulo, Brazil. Arq Bras Oftalmol 2021 Jan 21; 84:51–57. DOI:10.5935/0004-2749.20210009.
- Tan IJ, Wu XN, Dobson LP, et al. Rural pre-operative cataract assessment on the lions outback vision Van. Clin Exp Ophthalmol 2017 Oct 22; 45:410–412. 2016. DOI:10.1111/ceo.12866
- Alvi RA, Justason L, Liotta C, et al. The eagles eye mobile: assessing its ability to deliver eye care in a high-risk community. J Pediatr Ophthalmol Strabismus 2015 March 24; 52:98–105. DOI:10.3928/01913913-20150216-02.
- Hautala N, Hyytinen P, Saarela V, et al. A mobile eye unit for screening of diabetic retinopathy and follow-up of glaucoma in remote locations in northern Finland. Acta Ophthalmol 2009 June 06; 87:912–913. DOI:10.1111/j.1755-3768.2009.01570.x.
- Oshima CR, Yuki K, Uchida A, et al. The vision Van, a mobile eye clinic, aids relief efforts in tsunami-stricken areas. Keio J Med 2012 March 14; 61:10–14. DOI:10.2302/kjm.61.10.
- Jagadish P, Dalziel D. Discharge outcomes of patients referred to specialist eye clinic from diabetic retinopathy screening in Northland (2014-15). N Z Med J 2017 Feb 17; 130:89–93.
- Sheck L, Riley A, Wilson GA. Is a mobile surgical bus a safe setting for cataract surgery? A four-year retrospective study of intraoperative complications. Clin Exp Ophthalmol 2012 June 15; 40:330–331. 2011. DOI:10.1111/j.1442-9071.2011.02615.x
- Griffith JF, Wilson R, Cimino HC, et al. The use of a mobile van for school vision screening: results of 63 841 evaluations. Am J Ophthalmol 2016 Dec 02; 163:108–114 e101. DOI:10.1016/j.ajo.2015.11.026.
- Ministry of Health. Strategic frameworks. Wellington: Ministry of Health; 2021.
- Foreman J, Keel S, Dunn R, et al. Sampling methodology and site selection in the National Eye Health Survey: an Australian population-based prevalence study. Clin Exp Ophthalmol 2017 Dec 09; 45:336–347. DOI:10.1111/ceo.12892.
- Papali’i-Curtin AT, Cox R, Ma T, et al. Keratoconus prevalence among high school students in New Zealand. Cornea 2019 July 25; 38:1382–1389. DOI:10.1097/ICO.0000000000002054.
- Black J. Visual impairment and refractive error in Auckland school children ( MPH thesis). University of Auckland, Auckland; 2021.
- Southgate E, Kelly BJ, Symonds IM. Disadvantage and the ‘capacity to aspire’ to medical school. Med Educ 2015 Dec 30;49: 73–83. DOI:10.1111/medu.12540.
- Evans JR, Morjaria P, Powell C. Vision screening for correctable visual acuity deficits in school-age children and adolescents. Cochrane Database Syst Rev 2018 Feb 16; 2: CD005023. DOI:10.1002/14651858.CD005023.pub3.
- Shakarchi AF, Collins ME. Referral to community care from school-based eye care programs in the United States. Surv Ophthalmol 2019 March 13; 64: 858–867. DOI:10.1016/j.survophthal.2019.04.003.
- Curtis E, Jones R, Tipene-Leach D, et al. Why cultural safety rather than cultural competency is required to achieve health equity: a literature review and recommended definition. Int J Equity Health 2019 Nov 16; 18:174. DOI:10.1186/s12939-019-1082-3.
- Anstice NS, Alam K, Armitage JA, et al. Leaders in Indigenous Optometry Education Network. Developing culturally safe education practices in optometry schools across Australia and Aotearoa New Zealand. Clin Exp Optom. 2022 Nov; 6:1–9. DOI:10.1080/08164622.2022.2136514. Epub ahead of print. PMID: 36336833.
- University of Auckland. Taumata Teitei. Vision 2030 and Strategic Plan 2025. 2021.