
Abstract
This study was designed to evaluate the role of urinary and serum carbohydrate antigen 19-9 (CA19-9) as a biomarker in the assessment of patients with ureteral stone. A total of 38 patients with ureteral stone and hydronephrosis who underwent transurethral lithotripsy (TUL) (Group A) and 24 age-matched healthy controls (Group B) were evaluated in this study. Urinary and serum CA19-9 concentrations were measured in group A patients before TUL as well as 4 and 8 weeks following the operation. Urinary and serum CA19-9 concentrations were also measured in group B participants. Median concentration of urinary and serum CA19-9 was 34.0 and 15.0 kU/L in group A patients and 16.1 and 5.3 kU/L in group B, respectively (p < 0.001). Medians of CA19-9 concentration in urine and serum reduced to 12.5 and 4.5 kU/L 8 weeks after TUL (p < 0.001). Following successful TUL and hydronephrosis resolution, a significant decline was detected in serum and urinary CA19-9. We also noted that duration of ureteral obstruction was associated with serum and urinary CA19-9 concentrations, suggesting the potential role of this marker in predicting renal damage associated with urinary tract obstruction and determining the appropriate timing of interventions.
Introduction
Carbohydrate antigen 19-9 (CA19-9) is a 36-kDa serum glycolipid, which is used extensively as a tumor marker both in the diagnosis and follow-up of the patients with pancreatic or gastrointestinal cancers. A variety of tissues including the stomach, colon, gall bladder, pancreas, bronchial tree, endometrium, salivary glands and prostate express this marker in normal conditions.Citation1–3 Elevated concentrations of CA19-9 has been reported in nonmalignant conditions such as diabetes mellitus, hepatobiliary or pancreatic complications as well as pulmonary diseases.Citation4–6 Elevation of serum and urinary CA19-9 concentrations has also been reported in several benign urological conditions associated with urinary tract obstruction and hydronephrosis.Citation7–10 Furthermore, this marker might be a potential predictor of renal injuries associated with obstructive uropathies.Citation10,Citation11
Ureteral stones may be presented with colicky pains, dysuria and hematuria. Ultrasound-detected hydronephrosis has also been reported in approximately 90% of patients with ureterolithiasis.Citation12 The indication and appropriate timing of intervention in patients with ureteral stone have not been defined clearly. The management of patients with ureterolithiasis may be affected by the duration of symptoms. Although the length of time a stone has been in the ureter may be a potential predictor for the loss of renal function, several other factors including the degree of obstruction are also relevant factors. Few studies have evaluated the role of biomarkers in early detection of renal injury.Citation13 CA19-9 which is elevated in patients with obstructive hydronephrosis might be a potential marker in determining renal injury associated with ureteral obstruction in patients with ureteral stones.
We conducted this study to assess the correlation between CA19-9 concentrations and obstruction due to ureterolithiasis and to assess the potential of CA19-9 in predicting renal damage associated with obstructive hydronephrosis.
Materials and methods
In this prospective study, 62 patients were evaluated during the two-year study period. The patients with history of malignancy, liver and pancreatic diseases, diabetes mellitus, urinary tract infection and any other conditions which might affect serum CA19-9 concentrations were excluded from enrollment. The study participants were divided into two groups. Group A included 38 patients with colicky pain and distal ureteral stone and group B consisted of 24 age-matched healthy controls. Serum creatinine, blood urea nitrogen, urinary and serum CA19-9 concentration were measured in all the study participants. CA19-9 was measured using chemiluminescence method and the diagnosis of ureteral stone was confirmed with ultrasonography and/or abdominopelvic CT scan in group A patients. Interval between initiation of symptoms and treatment was recorded in all the patients. Successful TUL without ureteral stenting was performed in 33 of 38 patients. Ultrasonography was performed postoperatively and revealed no evidence of ureteral stone and hydronephrosis four weeks after TUL. Reevaluation of urinary and serum CA 19-9 was performed 4 and 8 weeks postoperatively in patients who underwent successful TUL. All the patients provided written informed consent and institutional review board approved the study.
Statistical analysis was performed using SPSS version 19 (SPSS Inc., Chicago, IL). T test and paired T test were applied to compare quantitative data. When the data were not normally distributed according to the Kolmogorov–Smirnov test, we applied Wilcoxon or Mann–Whitney U test. Qualitative data were compared using chi square test. p values of less than 0.05 were considered as statistically significant. Moreover, ROC curve analysis was performed to assess the sensitivity and specificity of serum and urinary CA19-9 in the diagnosis of ureteral stone.
Results
A total of 62 patients including 39 (62.9%) males and 23 (37.1%) females were enrolled in the study. The study participants consisted of 38 patients with ureteral stone (group A) and 24 frequency age-matched healthy controls (Group B). Mean age was 38.0 ± 14.6 and 32.7 ± 13.2 in group A and B participants respectively (p = 0.165). Mean serum creatinine and blood urea nitrogen was within the reference interval in all participants and did not differ between the study groups significantly. As shown in , preoperative serum and urinary CA19-9 concentrations were significantly higher in group A patients compared to healthy controls (p < 0.001, Mann–Whitney test). A median interval of 14 days (ranging from 4 to 180 days) was noted between initiation of symptoms and performing TUL. Pearson correlation coefficients did reveal significant correlation between serum (r = 0.710, p < 0.001) and urinary CA19-9 (r = 0.799, p < 0.001) and duration of obstruction (). The patients were further divided into two groups based on the duration of obstruction. Those who underwent TUL more than 2 weeks after initiation of symptoms had significantly higher serum and urinary CA19-9 concentrations (). Nevertheless we did not find a significant association between serum and urinary CA19-9 and severity of hydronephrosis. Four weeks after TUL, the median concentration of serum and urinary CA19-9 decreased to 4.7 and 13.4 kU/L in 33 patients who underwent successful TUL respectively (p < 0.001, Wilcoxon test). Although not statistically significant, further decline to 4.5 kU/L and 12.5 kU/L was also noted in serum and urinary CA19-9 concentrations 8 weeks after TUL respectively ().
Figure 1. Scatter plots show the correlation between serum (A) and urinary (B) carbohydrate antigen 19-9 concentration and duration of obstruction in patients with ureteral stone.
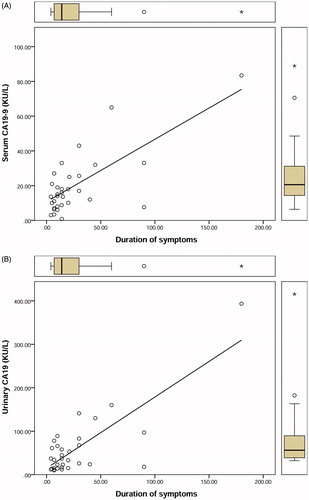
Figure 2. Box plots show the difference in serum (A) and urinary (B) carbohydrate antigen 19-9 concentration in patients with ureteral obstruction lasting <14 days compared to >14 days.
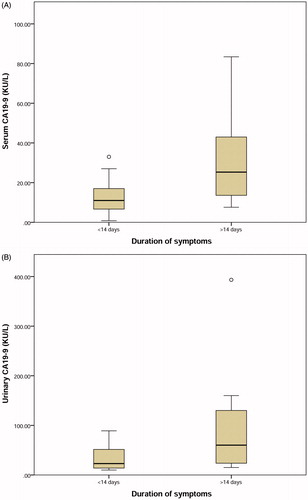
Table 1. Serum and urinary carbohydrate antigen 19-9 levels in study groups (values are shown in median [interquartile range]).
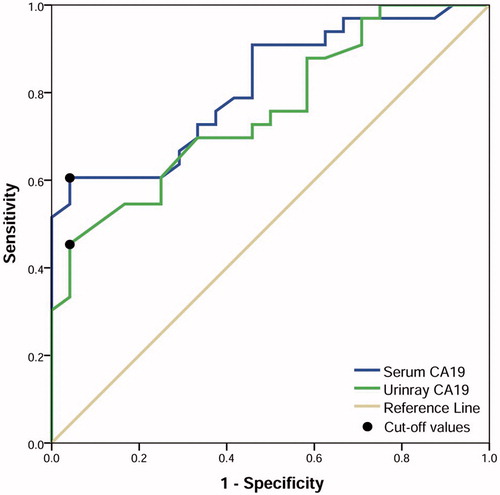
ROC curve analysis was performed to determine optimal cut off value, sensitivity and specificity of serum and urinary CA19-9 concentrations in detecting ureteral obstruction. Optimal cutoff values were reported considering a high specificity and positive likelihood ratio, which may be helpful in detecting renal injuries associated with ureteral obstruction. For serum CA19-9 at cut off value of 13.4 kU/L, we noted a sensitivity and specificity of 60.6% and 95.8% respectively (positive likelihood ratio = 14.5). Moreover, sensitivity and specificity of urinary CA19-9 concentration at reference value of 37.1 kU/L was 45.5% and 95.8% respectively with a positive likelihood ratio of 10.9 ().
Figure 3. Receiver operating characteristic curve analysis of serum and urinary carbohydrate antigen 19-9 for detecting obstructive hydronephrosis in patients with ureteral stone.
Discussion
CA19-9 is widely used as a tumor marker in diagnosis and follow-up of various cancers. However, serum and urinary concentrations of this biomarker may also increase in several nonmalignant conditions. In this study we showed statistically higher concentrations of CA19-9 both in urine and serum of patients with hydronephrosis due to ureteral stones. Concentrations of this marker returned to reference values after a successful TUL and resolution of the hydronephrosis, which highlights the potential role of this marker in evaluating surgery outcomes. Similar reports also showed significant elevation of serum and urinary CA19-9 in patients with benign hydronephrosis. Aybek et al. in a study evaluated serum and urinary CA19-9 in 54 patients with nonmalignant hydronephrosis and 23 healthy controls. They showed higher concentrations of CA19-9 both in serum and urine of patients with hydronephrosis, compared to healthy controls. However, neither serum nor urine CA19-9 predicted complete obstruction of the urinary tract.Citation7 Suzuki et al. showed an increase in the concentration of serum CA19-9 in patient with hydronephrosis and this increment was correlated with urinary tract infections, bilateral hydronephrosis, proteinuria, severity of obstruction, and grade of hydronephrosis. They also showed a correlation between serum CA19-9 and renal dysfunction.Citation10 In another study, this group hypothesized that changes in CA19-9 either in serum or urine after hydronephrosis resolution might be the most clinically useful parameter in the diagnosis of malignant from benign hydronephrosis.Citation9 There are also a couple of case reports on this subject. Inamoto et al. reported a patient with a giant hydronephrosis in right kidney associated with a high CA19-9 concentration both in the patient’s serum and bloody fluid drained from the nephrostomy.Citation14 Meyer et al. also reported a case with prolonged partial staghorn calculus in right kidney associated with severe hydronephrosis and loss of function. They reported a high serum CA19-9 concentration in this patient which declined to reference values after nephrectomy.Citation15 In another study Kutlu et al. evaluated 50 cases of ureteral stones and divided them into two groups based on the presence of hydronephrosis. They did not find any significant correlation between serum CA19-9 concentrations and presence of hydronephrosis. However, it should be considered that hydronephrosis is not a constant finding associated with ureteral stones and absence of hydronephrosis does not necessarily exclude obstruction in patients with ureteral stones.Citation16 Furthermore hydronephrosis is not necessarily accompanied with obstruction. Differentiating between obstructed and non-obstructed dilated pyelocaliceal systems which are associated with renal damage might be challenging. Atar et al. in a recent study reported the role of urine CA19-9 concentration in discriminating between obstructive and non-obstructive hydronephrosis in patients with unilateral antenatal hydronephrosis. They also revealed a significant decline in urine CA19-9 after pyeloplasty.Citation17 In another report, Kajbafzadeh et al. revealed an elevated concentrations of CA19-9 in serum and urine of patients with ureteropelvic junction obstruction and a significant decrease in CA19-9 concentrations after corrective surgery.Citation11 In patients with ureteropelvic junction obstruction, dilation of pyelocaliceal system, albeit non-obstructive, may persist even after the corrective surgery. Decrease in serum and urine CA19-9 concentrations in these patients after pyeloplasty, brings this hypothesis to mind that elevated serum and urinary CA19-9 concentrations is seen in patients with obstructive hydronephrosis which might be associated with renal damage.
Urothelium of renal pelvis normally secretes a certain amount of CA19-9. In addition the epithelium of renal tubules has shown positive staining for CA19-9 in immunohistochemical assays.Citation15 Inflammation and nonmalignant proliferation of these tissues result in increased production of this glycolipid. Moreover, obstruction in urinary tracts and subsequent decline in clearance of the marker, leads to higher concentrations of CA19-9 in serum.Citation18
CA19-9 concentrations greater than 37 kU/L are assumed to be abnormal. However, this cut off does not seem to be useful in benign conditions such as ureterolithiasis. Atar et al. reported urinary CA19-9 concentration of 15.6 kU/L as optimal cut off value for diagnosis of obstructive hydronephrosis in patients with ureteropelvic junction obstruction.Citation17 Moreover, Kajbafzadeh et al. in their study of patients with ureteropelvic junction obstruction showed that optimal cut off values for serum and urinary CA19-9 are 13.2 and 30.6 kU/L respectively.Citation11 Our results are similar to pervious findings and we showed that cut off values of 13.4 and 37.1 kU/L for serum and urinary CA19-9 are optimal for detecting obstructive hydronephrosis. Since specificities of our reported cutoff points are remarkably high, serum and urinary concentrations of this marker might be used as an adjunct to imaging techniques to confirm the diagnosis of ureteral obstruction secondary to ureteral stone. Since, elevated concentrations of CA19-9 are also seen in several other conditions such as diabetes mellitus, hepatobiliary diseases, pancreatic diseases and pulmonary complications,Citation4–6 these overlaps must be taken into account at the time of interpreting the results.
Our results did not show any correlation between serum and urinary CA19-9 concentrations and severity of hydronephrosis. However, this finding does not preclude the association between CA19-9 concentration and severity of obstruction. Severity of hydronephrosis in ultrasonography at the onset of renal colicky pains or referral of the patients is not necessarily an appropriate representative of obstruction and subsequent renal damage. Ureteral stones might have different positions within the ureter and move in urinary tract over their course of passage, therefore, the severity of hydronephrosis may alter. However, the time elapsed from the initiation of symptoms in patients with ureterolithiasis could be a better index for predicting the degree of renal damage.Citation7,Citation11 In the present study, for the first time a statistically significant relationship was found between symptom duration and CA19-9 serum and urinary concentrations. Our results support this hypothesis that significant elevations in CA19-9 may be related to more severe renal damages and thus needs a more urgent therapeutic intervention.
Our results revealed that serum and urinary CA 19-9 might have a potential role in the diagnosis of ureteral obstruction. This clinically applicable method may also increase the sensitivity and specificity of detecting ureteral obstruction especially when imaging modalities are inconclusive. Moreover, we noted higher CA19-9 concentration in patients with longer duration of ureteral obstruction. This finding supports the association between serum and urinary CA19-9 concentrations and renal damage and shows that this marker may be of value in predicting renal damage associated with urinary tract obstruction and determining the appropriate timing of intervention in patients with ureteral stone. Further studies with larger number of patients are necessary to confirm the role of serum and urinary CA19-9 in predicting renal damage in patients with urinary tract obstruction.
Disclosure statement
The authors declare no competing interests.
References
- Kilis-Pstrusinska K, Szajerka U, Zwolinska D. Unspecific increase of tumor markers in a girl with nephrotic syndrome and ovarian teratoma. Renal Fail. 2013;35:654–656.
- Atkinson BF, Ernst CS, Herlyn M, Steplewski Z, Sears HF, Koprowski H. Gastrointestinal cancer-associated antigen in immunoperoxidase assay. Cancer Res. 1982;42:4820–4823.
- Malaguarnera G, Giordano M, Paladina I, et al. Markers of bile duct tumors. World J Gastrointest Oncol. 2011;3:49–59.
- Ohshio G, Manabe T, Watanabe Y, et al. Comparative studies of DU-PAN-2, carcinoembryonic antigen, and CA19-9 in the serum and bile of patients with pancreatic and biliary tract diseases: Evaluation of the influence of obstructive jaundice. Am J Gastroenterol. 1990;85:1370–1376.
- Uygur-Bayramicli O, Dabak R, Orbay E, et al. Type 2 diabetes mellitus and CA 19-9 levels. World J Gastroenterol. 2007;13:5357–5359.
- Kodama T, Satoh H, Ishikawa H, Ohtsuka M. Serum Levels of CA19-9 in patients with nonmalignant respiratory diseases. J Clin Lab Anal. 2007;21:103–106.
- Aybek H, Aybek Z, Sinik Z, Demir S, Sancak B, Tuncay L. Elevation of serum and urinary carbohydrate antigen 19-9 in benign hydronephrosis. Int J Urol. 2006;13:1380–1384.
- Lopes RI, Denes FT, Bartolamei MG, et al. Serum and urinary values of CA 19-9 and TGFss1 in a rat model of partial or complete ureteral obstruction. Eur J Pediatr Surg. 2015;25:513–519.
- Suzuki K. Elevation of serum and urinary carbohydrate antigen 19–9 in benign hydronephrosis. Int J Urol. 2007;14:668–669.
- Suzuki K, Muraishi O, Tokue A. The correlation of serum carbohydrate antigen 19–9 with benign hydronephrosis. J Urol. 2002;167:16–20.
- Kajbafzadeh A-M, Elmi A, Talab SS, Emami H, Esfahani SA, Saeedi P. Urinary and serum carbohydrate antigen 19–9 as a biomarker in ureteropelvic junction obstruction in children. J Urol. 2010;183:2353–2360.
- Moak JH, Lyons MS, Lindsell CJ. Bedside renal ultrasound in the evaluation of suspected ureterolithiasis. Am J Emerg Med. 2012;30:218–221.
- Daggulli M, Utangac MM, Dede O, et al. Potential biomarkers for the early detection of acute kidney injury after percutaneous nephrolithotripsy. Renal Fail. 2016;38:151–156.
- Inamoto T, Itoh S, Azuma H, Katsuoka Y, Takasaki N. Giant hydronephrosis with increased carbohydrate antigen 19–9 both in serum and fluid. Hinyokika Kiyo. 2004;50:485–488.
- Meyer A, Kausch I, Krüger S, Fetscher S, Böhle A, Jocham D. Elevation of CA 19–9 in giant hydronephrosis induced by a renal calculus. Urology. 2004;63:381–382.
- Kutlu O, Celik O, Koksal IT, Yigit S, Danisman A. Serum carbohydrate antigen 19-9 levels in patients with unilateral hydronephrosis due to urinary lithiasis. Minerva Urol Nefrol. 2012;64:217–221.
- Atar A, Oktar T, Kucukgergin C, et al. The roles of serum and urinary carbohydrate antigen 19–9 in the management of patients with antenatal hydronephrosis. J Pediatr Urol. 2015;11:133.e1–133.e5.
- Ito S, Gejyo F. Elevation of serum CA19-9 levels in benign diseases. Intern Med. 1999;38:840–841.