
Abstract
Purpose
Abdominal aortic calcification (AAC) assessed by using standard lateral lumbar radiographs can be graded, and composite summary scores (range, 0–24) have been shown to be highly predictive of subsequent cardiovascular morbidity and mortality in hemodialysis (HD) patients. However, few studies have sought to determine the optimal AAC score cutoff values for the prediction of mortality among HD patients.
Methods
This retrospective cohort study included 408 hemodialysis patients. AAC severity was quantified by the AAC score, which was measured by lateral lumbar radiography with complete follow-up data from January 2015 to December 2021. We used receiver operating characteristic (ROC) analysis to find the cutoff AAC value for the prediction of mortality. The Kaplan–Meier method was used to analyze all-cause and cardiovascular mortality.
Results
The cutoff calcification score for the prediction of mortality was 4.5 (sensitivity, 67.3%; specificity, 70.4%). The patients with AAC scores above 4.5 had significantly higher all-cause (log-rank p < 0.001) and cardiovascular (log-rank p < 0.001) mortality rates than those with AAC scores below 4.5. In the multivariate regression analyses, an AAC score above 4.5 was a significant factor associated with all-cause mortality (HR: 2.079, p = 0.002) and cardiovascular mortality (HR: 2.610, p < 0.001).
Conclusions
AAC is a reliable aortic calcification marker. HD patients with an AAC score > 4.5 have significantly elevated all-cause and cardiovascular mortality compared with those with an AAC score ≤ 4.5. AAC was a better predictor than cardiac valve calcification for mortality in HD patients.
Introduction
The risk of cardiovascular disease among patients with end-stage kidney disease (ESKD) is far greater than that in the general population. Among chronic kidney disease (CKD) patients treated with hemodialysis or peritoneal dialysis, cardiovascular mortality is 10 to 20 times higher than that in the general population after stratification by age, race, sex and the presence of diabetes [Citation1]. Vascular calcification (VC) has attrated increased attention as an index of CVD and as a predictor of mortality among hemodialysis (HD) patients. Vascular calcification, including aortic calcification and coronary artery calcification, is highly prevalent among dialysis patients, and disorders of mineral metabolism have been reported to be risk factors for vascular calcification [Citation2]. Cardiac valve calcification (CVC) represents a common complication and a danger signal for cardiovascular events in HD patients. Longer HD vintage and the presence of diabetes were independent risk factors for VC and CVC in HD patients from Chinese cohorts [Citation3,Citation4].
The Framingham Heart Study showed that abdominal aortic calcification (AAC) assessed by using standard lateral lumbar radiographs is a marker of subclinical atherosclerotic disease and an independent predictor of subsequent vascular morbidity and mortality [Citation5]. It was also reported that the presence of AAC is closely associated with adverse outcomes in dialysis patients [Citation6]. However, studies regarding the significant association of AAC with all-cause or cardiovascular mortality in HD patients have not reached consistent conclusions [Citation7,Citation8]. AAC can be graded, and the composite summary scores (range 0–24) provide a simple, low-cost assessment of subclinical vascular disease and have been shown to be highly predictive of subsequent cardiovascular morbidity and mortality in the general population and hemodialysis (HD) patients [Citation5,Citation9]. However, few studies have sought to determine the optimal AAC score cutoff value for the prediction of mortality among HD patients.
Accordingly, this study evaluated the clinical significance of the degree of AAC using AAC scores measured from lateral lumbar radiographs in terms of cardiac function, clinical data, biochemical assays, death, and cardiovascular death among HD patients and identified the optimal cutoff values of AAC scores for predicting outcome in HD patients.
Materials and methods
Study design
This retrospective study included HD patients at the General Hospital of Northern Theater Command. A total of 408 maintenance hemodialysis patients who had received dialysis 3 times/week for >6 months and had complete follow-up data were enrolled in the cohort from January 2015 to June 2015. HD was performed for 4 h per session using a polysulfone dialyzer and a dialysate calcium concentration of 1.5 mmol/L. The present study only included patients who were neither transplanted nor transferred to another hospital during follow-up. The exclusion criteria were (1) tumor, (2) infection within 1 month, (3) rheumatic immune disease, (4) liver cirrhosis, (5) thyroid disease, (6) Crohn’s disease, and (7) incomplete information on the AAC evaluation. A total of 582 patients received hemodialysis in our hospital, 456 patients completed the examination and evaluation of abdominal aortic calcification, and 408 patients remained according to the inclusion and exclusion criteria. The patients were followed prospectively for cardiovascular mortality or death from any cause. The follow-up data were collected until December 2021. Cardiovascular mortality was defined as death due to myocardial infarction, heart failure, sudden cardiac death, or stroke. The study protocol was approved by the Ethics Committee of General Hospital of Northern Theater Command (approval number Y (2022) 056). Written consent forms were not required because of the retrospective nature of the study.
Evaluation of abdominal aortic calcification
Between January 1, 2015, and June 30, 2015, radiographs of the left lumbar spine were acquired in the standing position. The AAC scores (total score 0–24) were graded using the method described previously by Kauppila et al. [Citation10]. X-rays were reviewed and evaluated by two physicians who had expertise in reading VC on plain radiographs and who were blinded to the clinical data.
Clinical data and biochemical assays
All clinical data of the HD patients were collected and consisted of age, dialysis vintage, sex, causes of kidney disease, medical history, height, weight, smoking status, daily average blood pressure, Kt/V, and the usage of calcium-based phosphate binders, calcium-free phosphate binders, vitamin D medications, cinacalcet and ACEI/ARB. Diabetes mellitus was defined either as a comorbid condition or as the etiology of ESKD. Hypertension was determined as blood pressure that was consistently higher than 140/90 mmHg or having been treated with hypertension medication. We defined a patient with a useful medication history as patients whose medication time exceeded 6 months when they were enrolled. Blood tests were routinely performed for each patient before the first weekly hemodialysis session within 3 months of the date of radiographs of the left lumbar spine. Assays were performed using a standard biochemical analyzer.
Echocardiography
All enrolled patients were scanned with two-dimensional-guided M-mode echocardiography, which was performed by a cardiologist who was blinded to the patient’s clinical and laboratory data. The HD patients underwent echocardiography after the first dialysis session of the week. The M-mode measurements included the left atrial dimension (LAD), left ventricular end-diastolic internal dimension (LVDd), left ventricular posterior wall thickness (LVPWT), and interventricular septal wall thickness (IVST). Left ventricular mass (LVM) was calculated by means of the Devereux formula, and the ratio of the LVM to the body surface area (BSA) was used to determine the left ventricular mass index (LVMI) [Citation11]. Left ventricular hypertrophy (LVH) was defined as LVMI > 115 g/m2 (men) and > 95 g/m2 (women) [Citation12]. The LV ejection fraction was obtained using a modified biplane Simpson’s method from apical and four-chamber views. From the mitral valve inflow velocity curve using pulsed wave Doppler, the ratio of the E wave and A wave (E/A ratio) was calculated [Citation13].
Statistical analysis
Data are presented as the mean ± standard deviation (SD) unless otherwise specified. Continuous variables were compared using Student’s t test for two groups. The Mann–Whitney U test was used for nonparametric data, and categorical variables were compared using the chi-square test as appropriate. Receiver operating characteristic (ROC) analysis was used to find the best cutoff value of AAC for mortality based on sensitivity and specificity—that is, the value that maximized the sum of the sensitivity and specificity. The Kaplan–Meier method was used for survival analysis, and the log-rank test was used to compare the survival rate differences between the patient groups according to the AAC score cutoff value. Multivariate Cox hazards analyses were performed with the results from univariate analysis to identify factors associated with mortality. In the multivariate analyses, the factors that showed p<0.05 in the univariate analysis were entered as possible factors associated with mortality. HRs were calculated using Cox proportional hazards models to estimate the relationship of AAC scores with outcome. p<0.05 was considered statistically significant. The statistical analyses were performed with SPSS, version 22.0 (SPSS for Windows, IBM Corp, USA).
Results
We recruited 408 ESKD patients with chronic HD for this study. At baseline, the patients had a mean age of 55.1 ± 13.1 years, and 61.3% (n = 250) of them were males. The proportion of patients with diabetes was 24.0% (n = 98), the proportion with hypertension was 79.7% (n = 325), and the proportion with a prior history of CVD was 14.7% (n = 60). The median value of the HD vintage was 8 (range 1–28) years. The median AAC score among these patients was 4.4 (range, 0–22). The mean follow-up duration was 43.5 ± 14.7 months (range 1–51 months). During the follow-up period, 104 (25.5%) patients died. Of these, 79 patients experienced cardiovascular death.
The ROC analysis of the baseline AAC score with respect to mortality revealed an area under the ROC curve of 0.714. The optimal cutoff value of the AAC score was 4.5 (sensitivity, 67.3%; specificity, 70.4%; ). The ROC analysis of cardiac valve calcification (CVC) with respect to mortality revealed an area under the ROC curve of 0.671. The area under the ROC curve of the AAC score was greater than that of the CVC. The patients were allocated to one of two groups using a cutoff value of 4.5: Group A (AAC score ≤ 4.5) or Group B (AAC score > 4.5). shows the comparison of patient characteristics and biochemical parameters between the two groups. Age, duration of HD, proportion of patients with diabetes, proportion of patients with cardiovascular disease, CVC, AAC score, LAD, LVMI, Ca and β2-microglobulin were significantly higher in Group B than in Group A. E/A, intact parathyroid hormone (iPTH), albumin (ALB), and uric acid (UA) were significantly lower in Group B. Kaplan–Meier analysis revealed that all-cause mortality was significantly higher in Group B (; p < 0.001). Group B also had significantly higher cardiovascular mortality than Group A (; p < 0.001).
Figure 1. Receiver operating characteristic (ROC) analysis of the baseline abdominal aortic calcification (AAC) score for mortality. The area under the ROC curve is 0.714 (95% confidence interval, 0.659–0.769, p < 0.001). The cutoff value of the AAC score is 4.5 (sensitivity 67.3%, specificity 70.4%).
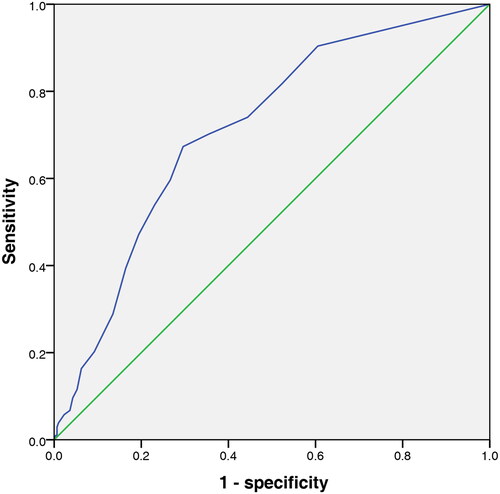
Figure 2. Kaplan–Meier analysis of all-cause and cardiovascular deaths of 408 hemodialysis patients. The blue line denotes the patients with an AAC score ≤ 4.5 (248 patients) and the green line denotes the patients with an AAC score > 4.5 (160 patients). (a) The patients with an AAC score > 4.5 had a higher death rate from all causes than those with an AAC score ≤ 4.5 (log-rank test, p < 0.001). (b) The patients with an AAC score > 4.5 had a higher death rate from cardiovascular mortality than those with an AAC score ≤ 4.5 (log-rank test, p < 0.001).
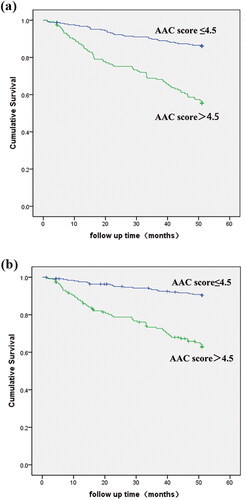
Table 1. Demographic characteristics of hemodialysis patients with AAC scores below and above 4.5.
Univariate Cox proportional hazards models were used to analyze various factors and mortality (). In addition to an AAC score >4.5, CVC, older age, the presence of diabetes, CVD, vitamin D supplementation, cinacalcet use, increased LAD, lower EF, lower hemoglobin (HGB), increased β2-microglobulin, lower triglycerides (TGs), lower ALB and lower UA were significant univariate predictors of increased all-cause mortality.
Table 2. Univariate Cox proportional hazards analysis of factors associated with all-cause and cardiovascular death in hemodialysis patients.
In the multivariate analyses, an AAC score >4.5 was a significant factor associated with all-cause mortality (hazard ratio, 2.079; 95% confidence interval, 1.299 to 3.326; p = 0.002), in addition to CVC, older age, presence of diabetes, increased LAD, lower serum Alb and lower triglycerides (). An AAC score >4.5 was also a significant factor associated with cardiovascular mortality (hazard ratio, 2.610; 95% confidence interval, 1.523 to 4.472; p < 0.001), in addition to CVC, the presence of diabetes, increased LAD, lower serum ALB and lower triglycerides. Collinearity diagnostics showed that the AAC and CVC tolerance (0.786 and 0.708) was greater than 0.10, and the variance inflation factor (1.272, and 1.413) was less than 10. Therefore, no serious collinearity problem was indicated. In the final model of all-cause mortality, an AAC score > 4.5 was compared with CVC using the partial chi-square statistic minus the predictor degrees of freedom (8.318 and 5.305 for AAC score > 4.5 and CVC, respectively) and was found to have a greater prognostic contribution. An AAC score > 4.5 was also found to have a greater contribution than CVC (11.186 and 7.467 for AAC score > 4.5 and CVC, respectively) in the final model of cardiovascular mortality.
Table 3. Multivariate Cox proportional hazards analysis of factors associated with all-cause and cardiovascular death in hemodialysis patients.
Discussion
The KDIGO guidelines suggest detecting the presence or absence of vascular calcification and valvular calcification in CKD G3a–G5D. However, previous studies did not actually compare the predictive values of AACs and CVCs regarding patient-centred end-points. Although coronary artery CT is more accurate than abdominal aortic calcification, clinical evaluation of AACs is widely available, easy to use, relatively inexpensive, involves low exposure to radiation and is noninvasive compared with coronary artery CT. The current study shows that the AAC score was associated with all-cause and cardiovascular mortality in chronic HD patients. The optimum AAC cutoff score for predicting mortality was found to be 4.5. We compared the contributions of AAC and CVC to adverse outcomes. AAC scores appeared to have a higher predictive value than CVC for all-cause and cardiovascular mortality in HD patients.
The results of the present study are consistent with previous reports in that the higher AAC (AAC score > 4.5) group was significantly older, had a longer dialysis vintage, a lower albumin level and a higher prevalence of diabetes than the lower AAC (AAC score ≤ 4.5) group. The patients with higher AACs were significantly older than those with lower AACs. The reason is that abdominal aortic calcification is indicative of advanced atherosclerosis in older patients. The serum albumin levels in the patients with higher AACs were significantly lower than those in the patients with lower AACs, indicating that the former patients were malnourished. However, the phosphorus levels did not differ between the two groups. The reason for this discrepancy is unclear but may be partially related to the fact that the use of calcium and phosphorus control medications affected the laboratory results.
Studies have shown that AAC is associated with a high incidence of cardiovascular events and mortality among HD patients [Citation6,Citation14]. CT measurement of aortic calcification is a highly reliable clinical research tool with high sensitivity and the ability to provide quantitative calcification measurements. However, CT scanning is expensive and produces more radiation than X-rays. The KDIGO guidelines suggest that lateral abdominal X-rays can be used to detect the presence of vascular calcification as a reasonable alternative to computed tomography-based imaging [Citation15]. The AAC score was first described by Kauppila et al. and it was first used by Okuno to evaluate hemodialysis patients, revealing that the presence of AAC is significantly associated with all-cause and cardiovascular mortality among HD patients [Citation6,Citation10]. Some recent studies have investigated the effect of AAC on the outcome of dialysis patients, but the results are controversial. The study of Ohya et al. reported that AAC was not a significant predictive parameter for all-cause death, but AAC was useful as a long-term prognostic indicator of cardiovascular mortality among HD patients [Citation7]. However, a Chinese retrospective observational study indicated that the presence of AAC was only significantly associated with all-cause mortality and not with cardiovascular mortality, indicating that AAC alone was not a good predictor of patient mortality in their population [Citation8]. A small number of studies have attempted to determine the optimal AAC score cutoff value for the prediction of mortality. An AAC score of 5 indicated a higher risk of mortality [Citation9], and another study showed that the cutoff calcification score for the prediction of mortality was 7.75 [Citation14]. Our study found that the optimum AAC cutoff score for predicting mortality was 4.5. The reason why earlier studies reached different conclusions than our study was that our study included a larger population with longer follow-up durations and had more covariates included than previous research. This threshold of 4.5 may be more reliable and valuable in clinical practice because it provides a direct method to identify HD patients at high risk of mortality.
The presence and degree of arterial calcification is considered to be one of the major determinants of the CVD incidence rate and mortality, and this occurs through various mechanisms. The abdominal aorta is a susceptible site for atherosclerosis and calcification. Therefore, the presence of AAC may be related to the occurrence of cardiovascular disease and patient death, and it is a very common complication in patients with ESKD [Citation16]. Arterial calcification is characterized by lesions that occur in the medial vascular wall, which exacerbates arterial stiffness and is termed arteriosclerosis in the CKD population [Citation17]. The AAC score can predict the occurrence of future CAD events in ESKD patients [Citation18]. AAC was also associated with an increased risk of congestive heart failure [Citation19]. The increased mortality caused by AAC may be due to the greater degree of generalized atherosclerosis and greater rate of occlusive lesions. Advanced aortic sclerosis with aortic calcification is associated with decreased aortic compliance, which increases the burden on the heart and increases the risk of cardiovascular death [Citation20].
Although there are reports about detecting AAC using plain abdomen X-rays in HD patients, little is reported about the estimate of abdominal aortic calcification by plain abdominal X-rays in terms of cardiac ultrasound parameters, mortality, and cardiovascular death in HD patients. This study evaluated AAC in terms of cardiac parameters, medication history, serum biochemical parameters, and clinical data with the risk of cardiovascular and all-cause mortality. After adjusting for these confounders, we found that an AAC score >4.5 predicts adverse outcomes in dialysis patients. In multivariate Cox regression, we found that cardiac ultrasound parameters, including valve calcification and LAD, were associated with mortality. Studies of CKD patients have demonstrated that valve calcification is an independent risk factor for coronary artery disease, arterial stiffness and peripheral vascular disease [Citation21,Citation22]. Experimental and clinical evidence indicates that valve calcification is an actively regulated pathophysiological process [Citation23]. The abdominal aortic calcification score correlated significantly with calcification of the aortic valve and mitral annulus in prevalent HD patients [Citation24]. The C-STRIDE study analyses showed that AAC may be associated with the risk of death for patients with CKD of any severity, while CVC is a possible risk factor for cardiovascular disease but only among those patients with mild to moderate CKD in the Chinese cohort [Citation25]. Our previous study found that CVC increased the risk of all-cause and cardiovascular mortality among HD patients [Citation26]. We sought to investigate the contributions of AAC and CVC to adverse events by using the partial chi-square statistic minus the predictor degrees of freedom [Citation27]. Our study showed that an AAC score of >4.5 appeared to better predict overall mortality in HD patients than CVC.
It is well known that elevated serum triglyceride (TG) levels are a risk factor for cardiovascular disease in the general population. However, we found that low triglycerides were significantly associated with all-cause and cardiovascular mortality in the multivariate Cox regression model. Kaplan–Meier analyses of 60 HD patients showed that serum triglycerides were higher in surviving HD patients [Citation28]. The relationship of serum TG with outcomes in patients with HD does not follow the pattern observed in the general population, and in a subset of patients, it can be paradoxical to what is expected. Although the underlying mechanisms responsible for these observations are not clear, these findings further demonstrate the limitations of serum lipid profiles in predicting outcomes in patients on HD [Citation29,Citation30].
Our study showed that smoking, hypertension, calcium-based phosphate binders, iPTH, and serum phosphate levels were not related to the risk of mortality. A previous study reported that the association of phosphate and iPTH with all-cause mortality was U-shaped, and both low and high levels have been reported as risk factors for mortality in hemodialysis patients [Citation31,Citation32]. However, in a prospective observational study conducted among French hemodialysis patients, serum P was not proven to be of predictive value for mortality by an adjusted Cox analyses [Citation33]. The reason may be that 40% of our subjects were over 60 years old, and 73% of the deceased patients were over 60 years old. However, the serum phosphorus and iPTH levels in elderly dialysis patients are not particularly high. An observational cohort study does not suggest that the calcium-free phosphate binder sevelamer is associated with superior cardiovascular safety or survival compared with calcium acetate in a routine care setting of patients 65 years or older with ESKD requiring maintenance HD from the United States Renal Data System (USRDS) [Citation34].
There are several limitations of our study. First, this was a retrospective observational cohort study at a single center. Second, we only included baseline AAC, cardiac ultrasound parameters and laboratory parameters and lacked follow-up observations of these indicators. Third, the follow-up period was relatively short. Therefore, prospective studies with longer follow-up periods are needed to support the clinical importance of AAC.
In conclusion, AAC is a reliable aortic calcification marker. HD patients with an AAC score > 4.5 have significantly elevated all-cause and cardiovascular mortality compared with those with an AAC score ≤ 4.5. AAC was a better predictor than CVC for mortality in HD patients.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee of General Hospital of Northern Theater Command (approval number Y (2022) 056).
Informed consent
The requirement to obtain written informed consent from each patient was waived because this was an observational retrospective study.
Consent for publication
All the authors agree to publish this manuscript.
Author contributions
JXB and NC conceived the study and its design, had full access to the patient records, and take responsibility for the accuracy and integrity of the data. JXB and AHZ contributed to the analysis and interpretation of the data. YPZ, KMR, ZR, CZ, and QW participated in patient inclusion and demographic data collection. All authors critically revised the drafted manuscript. The authors have read and approved the final manuscript.
Acknowledgements
The authors appreciate the support of our colleagues from the Department of Blood Purification, General Hospital of Northern Theater Command.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Datasets are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Coresh J, Longenecker JC, Miller ER, et al. Epidemiology of cardiovascular risk factors in chronic renal disease. J Am Soc Nephrol. 1999;9(12 Suppl):S24–S30.
- Chertow GM, Raggi P, Chasan-Taber S, et al. Determinants of progressive vascular calcification in haemodialysis patients. Nephrol Dial Transplant. 2004;19(6):1489–1496.
- Xiong JQ, Chen XM, Liang CT, et al. Prognosis and risk factors for cardiac valve calcification in chinese end-stage kidney disease patients on combination therapy with hemodialysis and hemodiafiltration. Ren Fail. 2022;44(1):224–232.
- He L, Yang W, Yang P, et al. Higher serum trimethylamine-N-oxide levels are associated with increased abdominal aortic calcification in hemodialysis patients. Ren Fail. 2022;44(1):2019–2027.
- Wilson PWF, Kauppila LI, O"Donnell CJ, et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation. 2001;103(11):1529–1534.
- Okuno S, Ishimura E, Kitatani K, et al. Presence of abdominal aortic calcification is significantly associated with all-cause and cardiovascular mortality in maintenance hemodialysis patients. Am J Kidney Dis. 2007;49(3):417–425.
- Ohya M, Otani H, Kimura K, et al. Vascular calcification estimated by aortic calcification area index is a significant predictive parameter of cardiovascular mortality in hemodialysis patients. Clin Exp Nephrol. 2011;15(6):877–883.
- Hong D, Wu S, Pu L, et al. Abdominal aortic calcification is not superior over other vascular calcification in predicting mortality in hemodialysis patients: a retrospective observational study. BMC Nephrol. 2013;14:120.
- Verbeke F, Van Biesen W, Honkanen E, CORD Study Investigators, et al. Prognostic value of aortic stiffness and calcification for cardiovascular events and mortality in dialysis patients: outcome of the calcification outcome in renal disease (CORD) study. Clin J Am Soc Nephrol. 2011;6(1):153–159.
- Kauppila LI, Polak JF, Cupples LA, et al. New indices to classify location, severity and progression of calcific lesions in the abdominal aorta: a 25-year follow-up study. Atherosclerosis. 1997;132(2):245–250.
- Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57(6):450–458.
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the european society of hypertension (ESH) and of the european society of cardiology (ESC). European Heart Journal. 2013;34(28):2159–2219.
- Rakowski H, Appleton C, Chan KL, et al. Canadian consensus recommendations for the measurement and reporting of diastolic dysfunction by echocardiography: from the investigators of consensus on diastolic dysfunction by. J Am Soc Echocardiogr. 1996;9(5):736–760.
- Kwon HY, Lee OH, Kim MJ, et al. The association between mortality and abdominal aortic calcification and relation between its progression and serum calcium concentration in chronic hemodialysis patients. Kidney Res Clin Prac. 2014;33(2):95–102.
- Kidney Disease: improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney Disease-Mineral and bone disorder (CKD-MBD). Kidney Inter Suppl. 2017;7(1):1–59.
- London GM, Guerin AP, Marchais SJ, et al. Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18(9):1731–1740.
- Honkanen E, Kauppila L, Wikström B, CORD study group, et al. Abdominal aortic calcification in dialysis patients: results of the CORD study. Nephrol Dial Transplant. 2008;23(12):4009–4015.
- Chen HC, Wang WT, Hsi CN, et al. Abdominal aortic calcification score can predict future coronary artery disease in hemodialysis patients: a 5-year prospective cohort study. BMC Nephrol. 2018;19(1):313.
- Walsh CR, Cupples LA, Levy D, et al. Abdominal aortic calcific deposits are associated with increased risk for congestive heart failure: the framingham heart study. Am Heart J. 2002;144(4):733–739.
- Witteman J, Grobbee D, Valkenburg HA, et al. J-shaped relation between change in diastolic blood pressure and progression of aortic atherosclerosis. Lancet. 1994;343(8896):504–507.
- Oliveira R, Okazaki H, Stinghen A, et al. Vascular calcification in chronic kidney disease: a review. J Bras Nefrol. 2013;35(2):147–161.
- Chen HC, Chou CY, Lin HJ, et al. Abdominal aortic calcification score predicts the occurrence of coronary artery disease in Middle-aged peritoneal dialysis patients. Nephrology. 2019;24(3):336–340.
- Wang Z, Jiang A, Wei F, et al. Cardiac valve calcification and risk of cardiovascular or all-cause mortality in dialysis patients: a meta-analysis. BMC Cardiovasc Disord. 2018;18(1):12.
- Kraus MA, Kalra PA, Hunter J, et al. The prevalence of vascular calcification in patients with end-stage renal disease on hemodialysis: a cross-sectional observational study. Ther Adv Chronic Dis. 2015;6(3):84–96.
- Wang L, Cheng H, Zou X, et al. Prevalence and correlates of cardiovascular calcification and its prognostic effects among patients with chronic kidney disease: results from the C-STRIDE study. Front Public Health. 2021;9:762370.
- Bai J, Zhang X, Zhang A, et al. Cardiac valve calcification is associated with mortality in hemodialysis patients: a retrospective cohort study. BMC Nephrol. 2022;23(1):43.
- Bajaj NS, Osborne MT, Gupta A, et al. Coronary microvascular dysfunction and cardiovascular risk in obese patients. J Am Coll Cardiol. 2018;72(7):707–717.
- Turkmen K, Demirtas L, Topal E, et al. Predictive value of atrial electromechanical delay on Long-Term cardiovascular outcomes in hemodialysis patients. Am J Nephrol. 2015;42(3):239–249.
- Kilpatrick RD, Mcallister CJ, Kovesdy CP, et al. Association between serum lipids and survival in hemodialysis patients and impact of race. J Am Soc Nephrol. 2007;18(1):293–303.
- Moradi H, Streja E, Kashyap ML, et al. Elevated high-density lipoprotein cholesterol and cardiovascular mortality in maintenance hemodialysis patients. Nephrol Dial Transplant. 2014;29(8):1554–1562.
- Lamina C, Kronenberg F, Stenvinkel P, et al. Association of changes in bone mineral parameters with mortality in haemodialysis patients: insights from the ARO cohort. Nephrol Dial Transplant. 2020;35(3):478–487.
- Floege J, Kim J, Ireland E, ARO Investigators, et al. Serum iPTH, calcium and phosphate, and the risk of mortality in a european haemodialysis population. Nephrol Dial Transplant. 2011;26(6):1948–1955.
- Fouque D, Roth H, Pelletier S, et al. Control of mineral metabolism and bone disease in haemodialysis patients: which optimal targets? Nephrol Dial Transplant. 2013;28(2):360–367.
- Spoendlin J, Paik JM, Tsacogianis T, et al. Cardiovascular outcomes of Calcium-Free vs Calcium-Based phosphate binders in patients 65 years or older with end-stage renal disease requiring hemodialysis. JAMA Intern Med. 2019;179(6):741–749.