
Abstract
Objectives
To assess potential mesothelioma risk following inhalation of cosmetic talc, we updated previous iterations of a pooled cohort analysis, post-study statistical power analysis, and confidence interval function analysis for a pooled cohort of international cosmetic talc miners/millers given new Italian cohort data.
Methods
Five cohorts of cosmetic talc miners/millers were pooled. Expected numbers of mesotheliomas for each cohort were reported by the original authors. We based our post-study statistical power analysis on an a priori one-sided significance level of 0.05, and exact Poisson and approximate distribution probabilities. To evaluate the confidence interval function for the observed pooled mesothelioma standardized mortality ratios (SMRs), we calculated the probability for the upper 100(1–2α)% confidence limit that equals various SMRs of interest.
Results
The pooled cohorts generated a total observation time of 135,524.38 person-years. Overall, 4.14 mesotheliomas were expected (mid-value estimate), though only one case of mesothelioma has been confirmed in the pooled cohort to date. We calculated 71% and 87% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively. Our complimentary confidence interval function analysis demonstrated that the probability that the true mesothelioma SMR for the pooled cohort was at or above 2.0 or at or above 3.0 was 0.00235 and 0.00005, respectively.
Conclusions
Based on the updated results of our various analyses, the current epidemiological evidence from cosmetic talc miner/miller cohort studies continues to not support the hypothesis that the inhalation of cosmetic talc is associated with an increased risk of mesothelioma.
Introduction
Based on recent case reports and series, inhalation exposure to cosmetic talc among consumers has been implicated with the subsequent development of mesothelioma (Gordon et al. Citation2014; Emory et al. Citation2020; Moline et al. Citation2020). However, authoritative bodies, such as the International Agency for Research on Cancer (IARC) and the American Conference of Governmental Industrial Hygienists (ACGIH), have reviewed the health risks associated with exposure to inhaled talc and determined that there is no associated cancer risk, including mesothelioma. IARC specifically reported that “[t]here is inadequate evidence in humans for the carcinogenicity of inhaled talc not containing asbestos or asbestiform fibres,” such that “[i]nhaled talc not containing asbestos or asbestiform fibres is not classifiable as to its carcinogenicity (Group 3)” (IARC Citation2010, p. 412). ACGIH designates talc “containing no asbestos” as “A4 – Not Classifiable as a Human Carcinogen” (American Conference of Governmental Industrial Hygienists [ACGIH] Citation2010, p. 1).
Cosmetic-grade talc (herein referred to as cosmetic talc) is widely regarded as “relatively pure” talc (Hildick-Smith Citation1976; IARC Citation1987; Zazenski et al. Citation1995; American Conference of Governmental Industrial Hygienists [ACGIH] Citation2001, p. 1; Citation2010; IARC Citation2010; Fiume et al. Citation2015; Drechsel et al. Citation2018). The Cosmetic, Toiletry, and Fragrance Association (CTFA), now known as the Personal Care Products Council (PCPC), noted that cosmetic talc “consists typically of 90% hydrated magnesium silicate” (CTFA Citation1976 b), while ACGIH more recently reported that talc used in cosmetics and pharmaceuticals is >98% and >99% pure, respectively (ACGIH Citation2010). Cosmetic talc is comprised of plates of a crystalline hydrated silicate of magnesium and, on occasion, other silicates, such as non-asbestiform serpentine or amphibole (e.g., anthophyllite and tremolite) minerals at low levels (Lightfoot et al. Citation1972; Pooley Citation1972, Citation1976; Rubino et al. Citation1976; Boundy et al. Citation1979; Rubino et al. Citation1979; Selevan et al. Citation1979; Parkes Citation1982; Wegman et al. Citation1982; Wergeland et al. Citation1990; Wild et al. Citation2002; Coggiola et al. Citation2003; Pira et al. Citation2017; Wergeland et al. Citation2017; Fordyce et al. Citation2019; Ciocan et al. Citation2022).
Of critical importance when determining potential health risks following the inhalation of cosmetic talc is the habit (i.e., asbestiform vs. non-asbestiform) of any potentially present amphibole minerals. As noted, the low levels of amphibole minerals occasionally present in cosmetic talc are most commonly found in their non-asbestiform habit (Zoltai Citation1979; Agency for Toxic Substances and Disease Registry [ATSDR] Citation2001; Strohmeier et al. Citation2010), which, from a human health risk perspective, is a relatively benign form of mineral, specifically when compared to the known health risks, including mesothelioma, associated with sufficient and prolonged exposures to asbestiform amphiboles (Consumer Product Safety Commission [CPSC] Citation1988; American Thoracic Society [ATS] Citation1990; OSHA Citation1992; ATSDR Citation2001; Addison and McConnell Citation2008; Gamble and Gibbs Citation2008; Mossman Citation2008; Williams et al. Citation2013; Mossman Citation2018).
Since 1976, the cosmetic industry has relied upon the J4-1 analytical method to determine the potential presence of asbestiform minerals in talc; this method incorporates X-ray diffraction (XRD) to detect the presence or absence of amphibole mineral, followed sequentially by optical microscopy and dispersion-staining color to determine potential fibrous morphology, if the mineral is in fact detected in the initial XRD step (CTFA Citation1976 b, Citation1976a). The U.S. Pharmacopeia (USP) has also published an analytical method to determine the “absence of asbestos” in talc used for pharmaceutical applications using either the infrared spectroscopy (IR) technique or XRD as a first step, and then optical microscopy if either of these two initial procedures returns a positive result (i.e., tremolite or serpentine minerals are detected) in order to confirm the potential presence of asbestos fibers (USP Citation2007, Citation2020). Additional efforts to develop analytical methods that can reliably identify potential asbestos fibers in talc are underway by the Talc Methods Expert Panel associated with the USP, as well as a federal Interagency Working Group, which made a white paper publicly available in December of 2021 (IWGACP Citation2021).
Analytical testing of cosmetic talc used in consumer products or from the source mines themselves has been conducted using various microscopic methods to evaluate and quantify the potential presence of asbestiform minerals (Cralley et al. Citation1968; Lewin Citation1972; Snider et al. Citation1972; Weissler Citation1973; Rohl and Langer Citation1974; Rohl et al. Citation1976; Kennedy Citation1979; Paoletti et al. Citation1984; Blount Citation1991; Mattenklott Citation2007; Gordon et al. Citation2014; Anderson et al. Citation2017; Ilgren et al. Citation2017; Pierce et al. Citation2017; Fitzgerald et al. Citation2019; Delgado et al. Citation2020; Stoiber et al. Citation2020; USFDA Citation2021; Ciocan et al. Citation2022). Although there are instances in which amphibole minerals were reportedly detected in the cosmetic talc samples, the analytical methods used in these studies were not always capable of distinguishing the amount, type, and habit of the minerals (asbestiform vs. non-asbestiform), and it was subsequently recognized that the results had limited reliability (USFDA Citation1971; Caneer Citation1973; Eiermann Citation1973; Weissler Citation1973; Krause Citation1977; Rohl and Langer Citation1979; Swanson Citation1986; Addison and Langer Citation2000; IARC Citation2010; Lee and Van Orden Citation2015).
Although there are no epidemiological studies of cosmetic talcum powder product end-users, to the best of our knowledge, cosmetic talc miners and millers can be used as an example of a reasonable proxy to assess mesothelioma risk of consumers, since these workers are known to have been exposed to high levels of cosmetic talc. Prior to this publication, we identified four cohort studies and subsequent updates of cosmetic talc miners and millers in five countries, including Italy (Rubino et al. Citation1976; Citation1979; Coggiola et al. Citation2003; Pira et al. Citation2017), Norway (Wergeland et al. Citation1990; Citation2017), France (Wild et al. Citation2002), Austria (Wild et al. Citation2002), and the United States-Vermont (Selevan et al. Citation1979; Fordyce et al. Citation2019). Overall, only one possible case of mesothelioma (with prior asbestos exposure noted on the death certificate) was reported in the Vermont cohort (Fordyce et al. Citation2019). Therefore, the epidemiological evidence from the cosmetic talc miner/miller cohort studies does not support the hypothesis that cosmetic talc exposures are associated with an increased risk of mesothelioma.
A criticism of these cohort studies was that the statistical power of any given study alone was too low to adequately ascertain a clinically significant risk of mesothelioma. However, as we have demonstrated in various prior publications, pooling the cohort data has generally resulted in good post-study statistical power to detect a true increase in risk (Finley et al. Citation2017; Marsh et al. Citation2019a; Ierardi and Marsh Citation2020). Indeed, in our most recent post-study statistical power analysis, we found that the pooled cohorts, with 130,514 person-years of observation across five cohorts and a mid-value estimate of 3.34 expected cases of mesotheliomas, had 59% and 78% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively (Ierardi and Marsh Citation2020). We additionally found that post-study statistical power was maintained after restricting the pooled cohort to workers who had a latency period of 30 or greater years (Marsh et al. Citation2019a).
As a complement to our post-study power calculations, we also conducted a confidence interval function analysis of the pooled cosmetic talc miner/miller cohort data to determine whether various hypothesized mesothelioma risks were consistent with the observed cohort data (Marsh and Ierardi Citation2020). Using the mid-value estimate of expected number of cases available at the time of publication (3.34), we determined that the probability (α) that the true mesothelioma SMR was at or above 2.0 or at or above 3.0 was 0.0096 and 0.0005, respectively, indicating that a mesothelioma SMR of 2.0 or greater was not compatible with the observed pooled data. This finding provided further support for the conclusion that cosmetic talc exposure is not associated with an elevated risk of mesothelioma.
Since the publication of our most recent post-study power analysis (Ierardi and Marsh Citation2020) and complimentary confidence interval function analysis (Marsh and Ierardi Citation2020), an update to the Italian cohort was published (Ciocan et al. Citation2022). Thus, the purpose of the current study was to update our pooled cohort analysis, post-study statistical power analysis, and confidence interval function analysis to include the updated Italian data.
Methods
Pooled cohort analysis
The expected numbers of mesothelioma deaths for each cohort have been explicitly reported by the authors of the original studies; these values were therefore used in the current study to estimate the total number of expected mesotheliomas in the pooled cohort (). As noted previously (Ierardi and Marsh Citation2020), the Vermont cohort was the only cohort for which a range of possible expected values was provided (Fordyce et al. Citation2019, Citation2020). Thus, we conducted the post-study statistical power analysis using all three estimates provided for the Vermont cohort in order to account for any potential uncertainties in expected values associated with this cohort.
Table 1. Most recent cohort studies included in an updated pooled analysis of pleural cancers/mesotheliomas associated with employment as a cosmetic talc miner or miller.
Post-study statistical power analysis
The same methodology for the pooled post-study statistical power analysis used in our prior publications (Finley et al. Citation2017; Marsh et al. Citation2019a; Ierardi and Marsh Citation2020) was again used in this study. Our aim, which was to address the question of whether the pooled cosmetic talc miner and miller cohort studies provided sufficient power to detect a statistically significant elevated risk of mesothelioma among these workers, also remained the same. Our post-study statistical power analysis focused on detecting only elevated mesothelioma risks, since reduced risk of mesothelioma resulting from exposure to cosmetic talc is an implausible event. We therefore entered into our pooled analysis with the a priori alternative hypothesis (HA) that the relative risk (RR; estimated using SMRs or incidence ratios) for mesothelioma among cosmetic talc miners and millers would be greater than that expected in the corresponding general reference populations (i.e., HA: RR > 1.0), and used a 5% one-sided significance test to test the null hypothesis (H0) of no excess risk (i.e., H0: RR = 1.0).
Exact Poisson distribution probabilities from Breslow and Day (Citation1987) and approximate power values based on the normal distribution-based method of Beaumont and Breslow (Citation1981) were used for our power calculations. As explained by Marsh and Ierardi (Citation2020), “[u]nlike exact power values, which may not increase monotonically with small numbers, approximate values increase monotonically with increasing numbers of expected cases” (Marsh and Ierardi Citation2020, p. 2).
Confidence interval function analysis
In order to incorporate observed risk estimates and their variances, which are not accounted for in post-study power calculations, we evaluated the confidence interval function for the observed pooled mesothelioma SMRs, and calculated the probability (α) for the upper 100(1–2α)% confidence limit that equals various SMRs of interest (1.5, 2.0, 2.5, 3.0). A more detailed explanation of these methods and calculations can be found in our previous publication (Marsh and Ierardi Citation2020).
Results
Pooled cohort analysis
Ciocan et al. (Citation2022) recently updated a mortality analysis of cosmetic talc miner and millers from Italy with an additional seven years of follow-up. Twenty-seven men were added to the cohort from the prior update by Pira et al. (Citation2017) for a total of 1,749 workers who contributed 64,349.38 person-years of observation; thus, 5,010.38 person-years were added in this update. The total observation time for all five pooled cohorts is now 135,524.38 person-years ().
Ciocan et al. (Citation2022) did not observe any deaths due to pleural cancer (expected = 2.8). Two cases of peritoneal cancer were identified, though these cases did not result in any significantly elevated risk (expected = 1.4; SMR = 1.43; 95% confidence interval [CI]: 0.17, 5.15). Specifically regarding these cases of peritoneal cancer, Ciocan et al. (Citation2022) explained that following a “detailed review of the medical records, … the specific causes of the two deaths from peritoneal cancer were one peritoneal carcinomatosis and one retroperitoneal tumor” (Ciocan et al. Citation2022, p. 2). Additionally, Ciocan et al. (Citation2022) noted that they excluded 172 subjects from their analysis because their age at death was older than 85. However, they stated, “[t]here were no deaths from either pleural or peritoneal cancer among the subjects deceased after the 85th birthday, who were excluded in the analysis” (Ciocan et al. Citation2022, p. 2-3). The authors did not report any deaths due to mesothelioma in their cohort or among those individuals aged 85+.
For the pooled cohort, total expected values for mesothelioma are now 3.97, 4.14, or 4.40, depending on the value used for the Vermont cohort (). SMRs of 0.252 (90% CI: 0.013, 1.19), 0.242 (90% CI: 0.012, 1.15), and 0.227 (90% CI: 0.012, 1.08) were calculated given these expected values and one observed case of mesothelioma from the Vermont cohort (). As in our prior pooled analysis (Ierardi and Marsh Citation2020), none of these SMRs was elevated above the null value of 1.00.
Table 2. Statistical power for SMR calculated after study completion and the probability estimate available from the observed dataa.
Post-study statistical power analysis
The results of the post-study statistical power analysis for various SMRs of interest are summarized in . One observed case of mesothelioma and a range of expected values of mesothelioma for the pooled cohort were used, as described above. Using the mid-value estimate of 4.14 for the expected number of mesothelioma cases, the pooled cohorts now have 71% and 87% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively (). Comparable statistical post-study power was calculated using the lower- (3.97) and upper-bound (4.40) expected value estimates (). Furthermore, and as we have previously noted (Marsh et al. Citation2019a; Ierardi and Marsh Citation2020), there are some irregular patterns in certain post-study power values with increasing SMRs of interest and across the three expected numbers. This counterintuitive result is due to the small number of events and the discrete nature of the Poisson probability distribution; using approximate post-study power values results in monotonically increasing numbers ().
Confidence interval function analysis
Using the updated mid-value estimate of expected number of mesothelioma cases from the pooled cohorts (4.14), the probability (α) that the true mesothelioma SMR was at or above 2.0 or at or above 3.0 was 0.00235 and 0.00005, respectively ( and ). also shows very low probabilities of observing 2.0- or 3.0-fold elevations in mesothelioma risk were found using the lower- (3.97) and upper-bound (4.40) estimates of expected cases.
Figure 1. Confidence interval function for SMR estimate = 0.242 derived from pooled cosmetic talc miner/miller cohort studies.
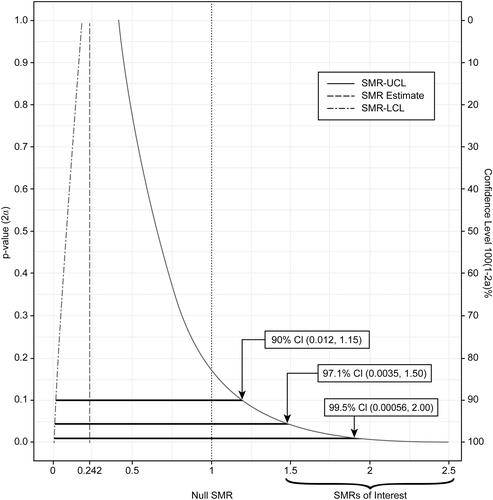
Table 3. Selected 100(1–2α)% confidence intervals from confidence interval function analysis, SMR point estimate = 1/4.14a = 0.242.
Discussion
As noted above, various analytical testing of cosmetic talcs has been performed by numerous investigators over time. The U.S. Food and Drug Administration (FDA) specifically has conducted analyses of cosmetic talcs used in consumer products for more than 50 years, up through as recently as 2021. Consistent with the other findings, the results of these FDA analyses indicate that there is no widespread issue of detectable asbestos in talc-containing consumer products (Lewin Citation1972; Eiermann Citation1973, Citation1976; Weissler Citation1973; Kennedy Citation1979; USFDA Citation2021). Yet concern as to this potential issue periodically resurfaces despite risk assessments performed by FDA and other investigators indicating that there is no increased risk of asbestos-related disease associated with the routine use of cosmetic talcum powder products, even assuming up to 0.1% asbestos content in cosmetic talc as a “worst-case” scenario (Brown Citation1985; Swanson Citation1986; Burns et al. Citation2019, p. 2272). Thus, our study represents a systematic and robust approach to address these concerns using a weight-of-evidence approach that incorporates the most current and relevant epidemiological literature in three unique types of analyses.
As we noted in Marsh and Ierardi (Citation2020), observed risk estimates and their variances are not accounted for in post-study power calculations. Thus, a confidence interval function analysis in this case allows us to effectively incorporate this observed data by evaluating the extent to which various alternative SMRs of interest are compatible with the observed risk of mesothelioma among the pooled cohort of international cosmetic talc miners and millers, and is a major strength of this study. We therefore updated our confidence interval function analysis using the new findings of Ciocan et al. (Citation2022) and determined that the probability that the true value of the SMR was 2.0 or greater was only 0.24% and 3.0 or greater was only 0.005%. These remarkably low probabilities indicate that SMRs for mesothelioma greater than 2.0 are not compatible with the observed data from the pooled cohort of cosmetic talc miners and millers, and provide further support for the conclusion that inhalation of cosmetic talc is not associated with an elevated risk of mesothelioma.
The results of our post-study power analysis warrant some discussion as well. In the initial analysis by Finley et al. (Citation2017), the pooled cohorts (which did not include the Vermont cohort) had 67% and 84% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively. An updated analysis (which included additional follow-up data for the Italian and Norwegian cohorts, but still did not include the Vermont cohort) had 62% and 79% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively (Marsh et al. Citation2019a). And, finally, our most recent prior analysis (which, for the first time, did include the Vermont cohort) had 59% and 78% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively (Ierardi and Marsh Citation2020). Lower- and upper-bound estimates of expected mesothelioma deaths did not materially alter the calculated post-study power.
The post-study statistical power calculated in the current study is greater than that calculated in our prior analyses due to the inclusion of updated Italian cohort data, which is the largest cosmetic talc miner/miller cohort in both number of subjects and person-years of observation, as well as longest duration of follow-up (a total of 74 years). Specifically, an additional 0.8 expected cases of pleural cancer among the Italian cohort were reported (2.8 by Ciocan et al. (Citation2022) vs. 2.0 by Pira et al. (Citation2017)), ultimately bolstering our calculated post-study power values, which is an additional strength of this study. While the post-study power values in the current study are indeed greater than those calculated in our prior analyses, the results are consistent and therefore continue to support the conclusion that there is no positive association between cosmetic talc exposure and risk of mesothelioma.
Furthermore, as noted, we previously conducted a latency analysis, and found that our post-study power calculations were effectively maintained among cosmetic talc miners and millers with a latency period of 30 or more years (observation time from first employment) (Marsh et al. Citation2019a). The update of the Italian cohort can only help to improve the number of person-years or percentage of person-years in the 30+ year latency group; thus, we would expect that our previous results from the latency analysis would not change materially given the newly available Italian cohort data.
Ierardi et al. (Citation2021) recently performed a weight-of-evidence assessment of Sir Bradford Hill’s guidelines for causal inference, which quantitatively evaluated cosmetic talc as a cause of mesothelioma. As part of the assessment of several guidelines, the mesothelioma risk of the cosmetic talc miners/millers was considered. The results of the current study support the original guideline justifications provided by Ierardi et al. (Citation2021), in particular that there is a deficit in mesothelioma risk (SMR = 0.242; 90% CI: 0.012, 1.15) among the pooled cosmetic talc miner/miller cohorts. This finding is not surprising given that the source mines where these workers were employed did not contain detectable asbestos and may only contain non-asbestiform amphibole and serpentine minerals, if any at all (Lightfoot et al. Citation1972; Pooley Citation1972, Citation1976; Rubino et al. Citation1976; Boundy et al. Citation1979; Rubino et al. Citation1979; Selevan et al. Citation1979; Parkes Citation1982; Wegman et al. Citation1982; Wergeland et al. Citation1990; Wild et al. Citation2002; Coggiola et al. Citation2003; Pira et al. Citation2017; Wergeland et al. Citation2017; Fordyce et al. Citation2019; Ciocan et al. Citation2022). Indeed, as Ierardi et al. (Citation2021) explain in their causal assessment, analogous occupational exposures to non-asbestiform minerals among the Homestake gold miners in South Dakota and the taconite iron ore miners in Minnesota do not result in an increased risk of mesothelioma in these workers. Experimental rodent studies also demonstrate that high doses of either inhaled or injected cosmetic talc do not produce an increase in mesothelioma (Ierardi et al. Citation2021). These epidemiological and toxicological findings are consistent with the current weight of evidence that non-asbestiform minerals do not possess biological activity, as indicated above, and reinforce the results of our current analyses, which used the most up-to-date cosmetic talc miner/miller cohort data available in the published literature.
Limitations
As noted, our current analyses have been updated by an additional 5,010.38 person-years from the Italian cohort, which only represents an approximate 4% increase in the total number of person-years of observation from our most recent update (Ierardi and Marsh Citation2020). While this increase in person-years may seem small and unlikely to impact our findings, it, in fact, greatly influences the total number of expected cases of mesothelioma, which have increased by nearly 24% since our previous update; yet, no additional cases of mesothelioma were identified. In addition, the numbers of expected cases of mesothelioma for each cohort used in our analyses were reported directly by the original authors of each study, and incorporate both national and regional rates, as indicated in . We have previously discussed the appropriateness of using regional rates (Marsh et al. Citation2019a, Citation2019b). Since the identification of unexposed referent populations is not logical, regional populations represent very similar groups of people to the miners/millers such that these comparisons are the most valid given the available data.
Additionally, the Italian cohort is the largest and oldest of the cosmetic talc miner/miller cohorts with a majority (approximately 77%) of the cohort now deceased (Ciocan et al. Citation2022), and many of the individuals who are still alive are entering older age groups where mesothelioma rates are higher (Moolgavkar et al. Citation2009, Citation2017; Boffetta et al. Citation2018). Thus, if cosmetic talc exposures among this, or any, miner/miller cohort were truly associated with an increased mesothelioma risk, then it is very likely that mesothelioma would have already developed in the individuals belonging to the older age groups. Naturally, one cannot determine causes of death for individuals in any of the cohorts who have unknown causes of death or were lost to follow-up. However, none of the cohorts suffered from an unacceptably high rate of loss to follow-up or unknown causes of death and, therefore, would not have affected our results. Indeed, the Norwegian cohort entailed the greatest combined total percentage of cohort members who were either lost to follow-up or died from an unknown cause of death (approximately 11% of the total cohort), with the other cohorts ranging from approximately 1% (Austrian) to approximately 10% (Italian).
Evolving International Classification of Diseases (ICD) codes for mesothelioma could potentially impact disease ascertainment and, as a result, our current findings. Yet, any under-ascertainment of cases in the cosmetic talc miner/miller cohorts would tend to balance out in the reference populations over time since the same classification codes would have been used for both groups in any given time period, and so it is therefore unlikely that these evolving ICD codes had any significant impact on our analyses. Further, Fordyce et al. (Citation2019), for example, conducted a thorough review of the death certificates for the Vermont cohort using ICD-5 through −10. Although, to the best of our knowledge, the authors did not perform the same review process for the referent population (the scale of which makes this an unfeasible undertaking, but, if anything, would only result in the identification of additional cases of mesothelioma, thereby increasing the referent population death rate and the total expected number of cohort deaths and, ultimately, reducing any potential SMR estimate), Fordyce et al. (Citation2019) only identified one confirmed death from mesothelioma, suggesting that under-ascertainment of mesothelioma deaths is unlikely to uniformly occur across the cohorts. We therefore maintain that the current analyses were performed using the best available cohort data, which indicate that exposure to cosmetic talc does not lead to an increased mesothelioma risk.
Conclusion
According to the most currently available data, the five pooled cosmetic talc miner/miller cohorts from Italy, Norway, France, Austria, and Vermont now comprise a total of 4,178 men (135,524.38 person-years of observation), and, based on the mid-value estimate of 4.14 expected mesotheliomas among the pooled cohort, the pooled SMR is 0.242 (90% CI: 0.012, 1.15). Based on this observed SMR, the probability that the true value of the SMR was 2.0 or greater was only 0.24%. Additionally, when this mid-value estimate is used in our post-study statistical power analysis, we calculated 71% and 87% post-study power to detect a 2.5-fold or greater and a 3.0-fold or greater increase in mesothelioma, respectively. Thus, the results of our various analyses of the pooled cohort allow us to continue to conclude that the current epidemiological evidence from the cosmetic talc miner and miller cohort studies does not support the hypothesis that inhalation of cosmetic talc is associated with an increased risk of mesothelioma.
Acknowledgments
The authors extend our appreciation to our colleague, Amanda Burns, for her helpful comments on the draft manuscript, as well as our thanks to Michael Tyson (Cardno now Stantec) for his graphic design assistance with the figure.
Disclosure statement
All of the authors are employed by Cardno ChemRisk now Stantec, a consulting firm that provides scientific advice to the government, corporations, law firms, and various scientific/professional organizations. GMM is also Professor Emeritus of Biostatistics and Epidemiology, and Founding Director, Center for Occupational Biostatistics and Epidemiology at the University of Pittsburgh, Graduate School of Public Health. This manuscript was prepared and written exclusively by the authors, and no external funding was received for this study. No organizations other than Cardno ChemRisk now Stantec were aware of the preparation of this manuscript, and no other organizations other than Cardno ChemRisk now Stantec reviewed any part of this manuscript prior to its submission for publication. Both AMI and GMM have been retained as defense experts in cosmetic talc-related litigation.
References
- [ACGIH] American Conference of Governmental Industrial Hygienists 2001. TLV for Talc. Cincinnati, OH: American Conference of Governmental Industrial Hygienists.
- [ACGIH] American Conference of Governmental Industrial Hygienists 2010. TLV for Talc. Cincinnati, OH: American Conference of Governmental Industrial Hygienists.
- Addison J, Langer AM. 2000. Draft Comments on the NTP Draft Report on Carcinogens Background Document for Talc Asbestiform and Non-Asbestiform. November 2000. Yorkshire: John Addison Consultancy.
- Addison J, McConnell EE. 2008. A review of carcinogenicity studies of asbestos and non-asbestos tremolite and other amphiboles. Regul Toxicol Pharmacol. 52(1 Suppl):S187–S199.
- Anderson EL, Sheehan PJ, Kalmes RM, Griffin JR. 2017. Assessment of health risk from historical use of cosmetic talcum powder. Risk Anal. 37(5):918–929.
- [ATS] American Thoracic Society 1990. Health effects of tremolite. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, June 1990. American Review of Respiratory Disease. 142(6 Pt 1):1453–1458.
- [ATSDR] Agency for Toxic Substances and Disease Registry 2001. Toxicological Profile for Asbestos. September 2001. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service, Agency for Toxic Substances and Disease Registry.
- Beaumont JJ, Breslow NE. 1981. Power considerations in epidemiologic studies of vinyl chloride workers. Am J Epidemiol. 114(5):725–734.
- Blount AM. 1991. Amphibole content of cosmetic and pharmaceutical talcs. Environ Health Perspect. 94:225–230.
- Boffetta P, Malvezzi M, Pira E, Negri E, La Vecchia C. 2018. International analysis of Age-Specific Mortality Rates From Mesothelioma on the Basis of the International Classification of Diseases, 10th Revision. J Glob Oncol. 4:1–15.
- Boundy MG, Gold K, Martin K, Jr. Burgess WA, Dement JA. 1979. Occupational exposures to non-asbestiform talc in Vermont. In: Lemen R, Dement JM, editors. Dusts and Disease. Park Forest South, IL: Pathotox Publisher Inc.; p. 356–378.
- Breslow NE, Day NE. 1987. Statistical methods in cancer research. Volume II–The design and analysis of cohort studies. IARC Sci Publ. (82):1–406.
- Brown R. 1985. Memo from QRAC (Quantitative Risk Assessment Committee) to W. Gary Flamm, Ph.D. (Director, Office of Toxicological Sciences - Food and Drug Administration), RE: Asbestos in Talc. Dated June 6, 1985.
- Burns AM, Barlow CA, Banducci AM, Unice KM, Sahmel J. 2019. Potential airborne asbestos exposure and risk associated with the historical use of cosmetic talcum powder products. Risk Anal. 39(10):2272–2294.
- Caneer WT. 1973. Internal Memo from W. T. Caneer (Colorado School of Mines Research Institute) to W. H. Ashton (Colorado School of Mines Research Institute), RE: Meeting with Bowling Green State University Geological Staff. Dated June 8, 1973.
- Ciocan C, Pira E, Coggiola M, Franco N, Godono A, La Vecchia C, Negri E, Boffetta P. 2022. Mortality in the cohort of talc miners and millers from Val Chisone, Northern Italy: 74 years of follow-up. Env Res. 203:111865.
- Coggiola M, Bosio D, Pira E, Piolatto PG, La Vecchia C, Negri E, Michelazzi M, Bacaloni A. 2003. An update of a mortality study of talc miners and millers in Italy. Am J Ind Med. 44(1):63–69.
- [CPSC] Consumer Product Safety Commission 1988. Consumer Product Safety Commission. Briefing package of the CPSC Office of the Secretary on a Petition to Ban Play Sand with Non-Asbestiform Tremolite. Washington, D.C.: U.S. Product Safety Commission.
- Cralley LJ, Key MM, Groth DH, Lainhart WS, Ligo RM. 1968. Fibrous and mineral content of cosmetic talcum products. Am Ind Hyg Assoc J. 29(4):350–354.
- [CTFA] Cosmetic, Toiletry, and Fragrance Association 1976a. CFTA Method J 4-1. Asbestiform Amphibole Minerals in Cosmetic Talc. Part I: X-Ray Diffraction Method, Part II: Optical Microscopy and Dispersion-Staining Method. Washington, D.C.: The Cosmetic, Toiletry, and Fragrance Association.
- [CTFA] Cosmetic, Toiletry, and Fragrance Association 1976b. CTFA Specification: Cosmetic Talc, revised October 7, 1976. The Cosmetic, Toiletry, and Fragrance Association.
- Delgado R, Fernandez-Gonzalez MV, Gzouly M, Molinero-Garcia A, Cervera-Mata A, Sanchez-Maranon M, Herruzo M, Martin-Garcia JM. 2020. The quality of Spanish cosmetic-pharmaceutical talcum powders. Appl Clay Sci. 193:105691.
- Drechsel DA, Barlow CA, Bare JL, Jacobs NF, Henshaw JL. 2018. Historical evolution of regulatory standards for occupational and consumer exposures to industrial talc. Regul Toxicol Pharmacol. 92:251–267.
- Eiermann HJ. 1973. Summary and Comments on Analyses for Asbestos in Cosmetic Talc Products. October 1, 1973.
- Eiermann HJ. 1976. Internal Memo from Heinz J. Eiermann (U.S. FDA - Director, Division of Cosmetics Technology) to Robert M. Schaffner (U.S. FDA - Associate Director for Technology), RE: Asbestos in Talc. Dated March 18, 1976.
- Emory TS, Maddox JC, Kradin RL. 2020. Malignant mesothelioma following repeated exposures to cosmetic talc: A case series of 75 patients. Am J Ind Med. 63(6):484–489.
- Finley BL, Benson SM, Marsh GM. 2017. Cosmetic talc as a risk factor for pleural mesothelioma: A weight of evidence evaluation of the epidemiology. Inhal Tox. 29(4):179–185.
- Fitzgerald S, Harty E, Joshi TK, Frank AL. 2019. Asbestos in commercial indian talc. Am J Ind Med. 62(5):385–392.
- Fiume MM, Boyer I, Bergfeld WF, Belsito DV, Hill RA, Klaassen CD, Liebler DC, Marks JG, Jr., Shank RC, Slaga TJ, et al. 2015. Safety Assessment of Talc as Used in Cosmetics. Int J Toxicol. 34(1 Suppl):66S–129S.
- Fordyce TA, Leonhard MJ, Mowat FS, Moolgavkar SH. 2019. A 37-year update on mortality patterns in an expanded cohort of Vermont talc miners and millers. J Occup Environ Med. 61(11):916–923.
- Fordyce TA, Leonhard MJ, Mowat FS, Moolgavkar SH. 2020. Letter to the Editor: Egilman et. al.'s misrepresentation of the Fordyce et al. (2019) Vermont talc miners and millers cohort study update. J Occup Env Med. 62(1):e19–e21.
- Gamble JF, Gibbs GW. 2008. An evaluation of the risks of lung cancer and mesothelioma from exposure to amphibole cleavage fragments. Regul Toxicol Pharmacol. 52(1 Suppl):S154–S186.
- Gordon RE, Fitzgerald S, Millette J. 2014. Asbestos in commercial cosmetic talcum powder as a cause of mesothelioma in women. Int J Occup Environ Health. 20(4):318–332.
- Hildick-Smith GY. 1976. The biology of talc. Br J Ind Med. 33(4):217–229.
- [IARC] International Agency for Research on Cancer 1987. Talc. IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans: Silica and Some Silicates. Lyon: International Agency for Research on Cancer; p. 185–224.
- [IARC] International Agency for Research on Cancer 2010. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Volume 93: Carbon Black, Titanium Dioxide, and Talc. Lyon, France: International Agency for Research on Cancer.
- Ierardi AM, Marsh GM. 2020. Absence of mesothelioma risk maintained in an expanded international cohort of cosmetic talc miners and millers. Inhal Toxicol. 32(6):257–264.
- Ierardi AM, Urban A, Marsh GM. 2021. A quantitative weight of evidence assessment of Hill's guidelines for causal inference for cosmetic talc as a cause of mesothelioma. Tox Appl Pharm. 417:115461.
- Ilgren EB, Sartorio C, Hoskins JA. 2017. Analysis of an authentic historical Italian cosmetic talc sample - Further evidence for the lack of cancer risk. EP. 6(2):6–33.
- Interagency Working Group on Asbestos in Consumer Products [IWGACP] 2021. White Paper: IWGACP Scientific Opinions on Testing Methods for Asbestos in Cosmetic Products Containing Talc. Dated December, 2021.
- Kennedy D. 1979. Memo from Donald Kennedy (Commission of Food and Drugs) to Sidney M. Wolfe, M.D, and Mr. Benjamin Gordon (Public Citizen) RE: Letter from Sidney M. Wolfe and Mr. Benjamin Gordon Dated August 4, 1978, Discussing Talc Carcinogenesis (With Attachments). Dated January 11, 1979.
- Krause JB. 1977. Mineralogical characterization of cosmetic talc products. J Toxicol Environ Health. 2(5):1223–1226.
- Lee R, Van Orden D. 2015. Letter To The Editor RE, Gordon R, Fitzgerald S, Millette J. 2014. Asbestos in commercial cosmetic talcum powder as a cause of mesothelioma in women. Int J Occup Environ Health. 20(4):318–332.
- Lewin SZ. 1972. Memo from Seymour Z. Lewin (Professor of Chemistry, New York University) to Dr. Alfred Weissler (Acting Director, Division of Colors and Cosmetics Technology, Office of Product Technology, Food and Drug Administration), RE: Lewin's Final Analytical Results on the Mineral Compositions of 102 Examples of Standard, Commercial Products Containing Talc (With Attachment). Dated August 3, 1972.
- Lightfoot J, Kingston GA, Pooley FD. 1972. An Examination of Italian Mine Samples and Relevant Powders. Cardiff, UK: Cardiff University.
- Marsh GM, Ierardi AM, Benson SM, Finley BL. 2019a. Occupational exposures to cosmetic talc and risk of mesothelioma: An updated pooled cohort and statistical power analysis with consideration of latency period. Inhal Tox. 31(6):213–223.
- Marsh GM, Ierardi AM. 2020. Confidence interval function analysis to evaluate the risk of mesothelioma among an expanded international cohort of cosmetic talc miners and millers. Regul Toxicol Pharmacol. 115:104696.
- Marsh GM, Ierardi AM, Benson SM, Finley BL. 2019b. Response to letters regarding “Occupational exposures to cosmetic talc and risk of mesothelioma: An updated pooled cohort and statistical power analysis with consideration of latency period". Inhal Toxicol. 31(11-12):387–391.
- Mattenklott M. 2007. Asbestos in Talc Powders and Soapstone - The Present State. Accessed October 13, 2017: http://www.dguv.de/medien/ifa/de/pub/grl/pdf/2009_108.pdf.
- Moline J, Bevilacqua K, Alexandri M, Gordon RE. 2020. Mesothelioma associated with the use of cosmetic talc. J Occup Environ Med. 62(1):11–17.
- Moolgavkar SH, Chang ET, Mezei G, Mowat FS. 2017. Chapter 3, Epidemiology of mesothelioma. In: Testa JR, editor. Asbestos and mesothelioma current cancer research. Cham, Switzerland: Springer; p. 43–72.
- Moolgavkar SH, Meza R, Turim J. 2009. Pleural and peritoneal mesotheliomas in SEER: age effects and temporal trends, 1973–2005. Cancer Causes Control. 20(6):935–944.
- Mossman BT. 2008. Assessment of the pathogenic potential of asbestiform vs. nonasbestiform particulates (cleavage fragments) in in vitro (cell or organ culture) models and bioassays. Regul Toxicol Pharmacol. 52(1 Suppl):S200–S203.
- Mossman BT. 2018. Mechanistic in vitro studies: What they have told us about carcinogenic properties of elongated mineral particles (EMPs). Tox Appl Pharm. 361:62–67.
- [OSHA] Occupational Safety and Health Administration. 1992. 29 CFR Parts 1910 and 1926: Occupational Exposure to Asbestos, Tremolite, Anthophyllite and Actinolite; Final Rule. Fed. Reg. 57(110):24310–24331. June 8, 1992.
- Paoletti L, Caiazza S, Donelli G, Pocchiari F. 1984. Evaluation by electron microscopy techniques of asbestos contamination in industrial, cosmetic, and pharmaceutical talcs. Regul Toxicol Pharmacol. 4(3):222–235.
- Parkes WR. 1982. Occupational Lung Disorders. 2nd ed. Boston: Butterworths.
- Pierce JS, Riordan AS, Miller EW, Gaffney SH, Hollins DM. 2017. Evaluation of the presence of asbestos in cosmetic talcum products. Inhal Toxicol. 29(10):443–456.
- Pira E, Coggiola M, Ciocan C, Romano C, La Vecchia C, Pelucchi C, Boffetta P. 2017. Mortality of talc miners and millers from Val Chisone, Northern Italy: An updated cohort study. J Occup Environ Med. 59(7):659–664.
- Pooley FD. 1972. Report of the Examination of Rock Samples from the Vermont Mine. UK: Department of Mineral Exploitation, Cardiff University.
- Pooley FD. 1976. Letter from Dr. F.D. Pooley, Department of Mineral Exploitation, University College, Cardiff, to Dr. R.E. Shapiro, Ph.D., Epidemiology Unit, HFF-108, Department of Health, Education & Welfare, Public Health Service, Food and Drug Administration, Washington, D.C. Dated March 9, 1976. Cardiff: University College.
- Rohl AN, Langer AM. 1974. Identification and quantitation of asbestos in talc. Environ Health Perspect. 9:95–109.
- Rohl AN, Langer AM. 1979. Fibrous mineral content of consumer talc-containing products. In: Lemen R, Dement JM, editors. Dusts and Disease. Park Forest South, IL: Pathotox Publishers; p. 393–403.
- Rohl AN, Langer AM, Selikoff IJ, Tordini A, Klimentidis R, Bowes DR, Skinner DL. 1976. Consumer talcums and powders: mineral and chemical characterization. J Toxicol Environ Health. 2(2):255–284.
- Rubino GF, Scansetti G, Piolatto G. 1979. Mortality and morbidity among talc miners and millers in Italy. In: Lemen R, Dement JM, editors. Dusts and Disease: Proceedings of the Conference on Occupational Exposures to Fibrous and Particulate Dust and Their Extension into the Environment. Park Forest South, IL: Pathotox Publishers; p. 357–363.
- Rubino GF, Scansetti G, Piolatto G, Romano CA. 1976. Mortality study of talc miners and millers. J Occup Med. 18:186–193.
- Selevan SG, Dement JM, Wagoner JK, Froines JR. 1979. Mortality patterns among miners and millers of non-asbestiform talc: preliminary report. J Environ Pathol Toxicol. 2(5):273–284.
- Snider DW, Pfeiffer DE, Mancuso JJ. 1972. Asbestosform impurities in commerical talcum powders. Compass of Sigma Gamma Epsilon. 49:65–67.
- Stoiber T, Fitzgerald S, Leiba NS. 2020. Asbestos contamination in talc-based cosmetics: An invisible cancer risk. Environ Health Insights. 14:117863022097655. 1178630220976558.
- Strohmeier BR, Huntington JC, Bunker KL, Sanchez MS, Allison K, Lee RJ. 2010. What is asbestos and why is it important? Challenges of defining and characterizing asbestos. Int Geol Rev. 52(7-8):801–872.
- Swanson JW. 1986. Memo from J.W. Swanson (Acting Associate Commissioner for Regulatory Affairs - U.S. Food and Drug Administration) to Mr. Phillippe Douillet, RE: Docket Number 1982P-404, Denying a November 8, 1983, Petition Requesting that Cosmetic Talc be Labeled with an Asbestos Warning Statement (Includes Enclosures/Talc Documents). Dated July 11, 1986.
- U.S. Food and Drug Administration [USFDA] 1971. FDA Meeting Minutes-Asbestos in Cosmetic Talc. August 3, 1971 - Washington, D.C.
- U.S. Food and Drug Administration [USFDA] 2021. Talc. Retrieved Jan. 31, 2022 from: https://www.fda.gov/cosmetics/cosmetic-ingredients/talc. Silver Spring, MD: U.S. Food and Drug Administration (USFDA).
- U.S. Pharmacopeia [USP] 2007. US Monographs: Talc. Retrieved Nov. 24, 2020 from: http://ftp.uspbpep.com/v29240/usp29nf24s0_m80360.html#. Rockville, MD: U.S. Pharmacopeia.
- U.S. Pharmacopeia [USP] 2020. FAQs: Modernization of the USP Talc Monograph. Retrieved Nov. 24, 2020 from: https://www.usp.org/frequently-asked-questions/talc-monograph. Rockville, MD: U.S. Pharmacopeia.
- Wegman DH, Peters JM, Boundy MG, Smith TJ. 1982. Evaluation of respiratory effects in miners and millers exposed to talc free of asbestos and silica. Br J Ind Med. 39(3):233–238.
- Weissler A. 1973. Internal Memo from Alfred Weissler Ph.D. (Acting Director- Division of Color Technology, U.S. Food and Drug Administration) to Dr. Robert M. Schaffner (Director - Office of Technology, U.S. Food and Drug Administration), RE: Summary and Comments on Prof. Lewin's Analytical Results for Asbestos in Talc (Enclosures Included - Final Report: X-Ray Powder Diffraction Analyses of Commerical Cosmetic Powders). Dated July 31, 1973.
- Wergeland E, Andersen A, Berheim A. 1990. Morbidity and mortality in talc-exposed workers. Am J Ind Med. 17(4):505–513.
- Wergeland E, Gjertsen F, Vos L, Grimsrud TK. 2017. Cause-specific mortality and cancer morbidity in 390 male workers exposed to high purity talc, a six-decade follow-up. Am J Ind Med. 60(9):821–830.
- Wild P, Leodolter K, Refregier M, Schmidt H, Zidek T, Haidinger G. 2002. A cohort mortality and nested case-control study of French and Austrian talc workers. Occup Environ Med. 59(2):98–105.
- Williams C, Dell L, Adams R, Rose T, Van Orden D. 2013. State-of-the-science assessment of non-asbestos amphibole exposure: Is there a cancer risk? Environ Geochem Health. 35(3):357–377.
- Zazenski R, Ashton WH, Briggs D, Chudkowski M, Kelse JW, MacEachern L, McCarthy EF, Nordhauser MA, Roddy MT, Teetsel NM. 1995. Talc: Occurrence, characterization, and consumer applications. Regul Toxicol Pharmacol. 21(2):218–229.
- Zoltai T. 1979. Asbestiform and acicular mineral fragments. Ann NY Acad Sci. 330(1 Health Hazard):621–643.