
ABSTRACT
Purpose: To determine the need or otherwise for establishment of a trachoma elimination program in Gombe State, Nigeria, by estimating the population-based prevalence of trachoma in each Local Government Area (LGA) of Gombe.
Methods: Using a multi-stage, systematic, random, and quasi-random sampling approach and Global Trachoma Mapping Project support, we selected 25 clusters in each LGA. In each cluster, we selected 25 households and all consenting residents aged 1 year and older were examined for trachomatous inflammation–follicular (TF) and trichiasis, using the World Health Organization simplified grading scheme.
Results: No LGA in Gombe State had a TF prevalence ≥5% in 1–9-year-olds. All LGAs had trichiasis prevalences above the elimination threshold and should be targeted for community-based delivery of trichiasis surgery. Only three LGAs had household-level improved wash water access of greater than 80%. Access to improved sanitation facilities was also poor as household access to improved sanitation facilities was above 80% in only one LGA.
Conclusion: A trachoma program focused on delivery of trichiasis surgery is required in Gombe. Improvements in water and sanitation, through engagement with other sectors, are necessary.
Introduction
Trachoma is responsible for 4% of overall blindness in Nigeria, with the north-eastern part of the country having the highest burden.Citation1 There are fewer than five years until the agreed target date for the global elimination of trachoma as a public health problem.Citation2 The World Health Organization (WHO) recommends the SAFE (Surgery for trichiasis; Antibiotics to clear infection; Facial cleanliness and Environmental improvement to reduce transmission) strategy for the elimination of trachoma.Citation2 Implementation of the SAFE strategy has led to considerable decline of trachoma in various countries.Citation3,Citation4 It is therefore important that countries suspected of being trachoma-endemic document where trachoma is a problem, at district level, and determine what aspects of the SAFE strategy require implementation. To reach this decision, trachoma programs need to know the prevalence of trachomatous inflammation–follicular (TF) in children aged 1–9 years, and the prevalence of trachomatous trichiasis in adults aged 15 years and older, in each suspected-endemic district. Gombe State is located in the north-eastern part of Nigeria and borders Yobe, Kano and Jigawa States, where trachoma has been documented as requiring intervention.Citation5–Citation7 However, there is no trachoma elimination program in Gombe State, in part because the district-level prevalences of trachoma, which might justify the establishment of such a program, have not been estimated.
We sought to determine the district (Local Government Area, LGA) level prevalence of TF and trichiasis in Gombe, so that the government and its partners can determine whether a trachoma elimination program is required. This was undertaken as part of the Global Trachoma Mapping Project (GTMP).
Materials and methods
Sample size calculations, field team training and certification protocols, data collection procedures, data processing and analysis techniques all followed GTMP standards, which have been previously published.Citation8 In Gombe State, each LGA formed an evaluation unit, and we estimated an average of two children aged 1–9 years per household; 25 clusters each of 25 households therefore put >1222 children in the sampling frame per LGA. In each selected household, all residents aged 1 year and older were invited to be examined by GTMP-certified graders for TF, trachomatous inflammation—intense, and trichiasis. As elsewhere, we also collected data on household-level access to water and sanitation, using a combination of questioning of adult residents and direct observation.
Ethics
Examination protocols were explained by field teams to prospective participants in a language they understood, and verbal consent for enrolment and examination was obtained, as most survey subjects could neither read nor write. Each adult provided individual consent while heads of households gave consent on behalf of minors. Consent was documented in the LINKS applicationCitation9 by research teams. Persons with clinical evidence of active trachoma were given two tubes of 1% tetracycline eye ointment, and they or their carer were told how to apply it. Participants with trichiasis were referred to the nearest trained trichiasis surgeon for free lid surgery. In between examinations, graders used an alcohol-based hand sanitizer to clean their hands. Protocols were approved by the National Health Research Ethics Committee of Nigeria (NHREC/01/01/2007), and the Ethics Committee of the London School of Hygiene & Tropical Medicine (reference 6319). The Gombe State Ministry of Health gave administrative permission to conduct the surveys.
Sampling
A total of 25 villages (clusters) were selected from a sampling frame which consisted of a list of all the villages in each LGA, using a probability-proportional-to-size technique. Each selected village was further subdivided into existing subunits (wards), one of which was randomly selected; in the selected ward, 25 households were selected using the random walk, despite its epidemiological drawbacks.Citation6,Citation10 A household was defined as all individuals normally resident together and eating from the same pot.
Survey definitions
The WHO simplified grading scheme was used.Citation11 Data on household-level access to water and sanitation were collected using standard GTMP protocols.Citation8
Data handling
Data were cleaned and analyzed following the standard GTMP techniques.Citation8 The GTMP data manager analyzed the data using pre-specified algorithms to control for age and sex of those recruited, and the number of individuals examined in each cluster. We calculated the trichiasis backlog in each LGA by multiplying the prevalence estimate in persons aged 15 years and older by 0.56 of the total population per LGA (as determined in the most recent census), because 56% of the Nigerian population is aged 15 years or older.Citation12 Further data analyses presented here were carried out in Epi Info version 7.0 (Centers for Disease Control and Prevention, Atlanta, GA, USA).
Results
Field teams examined 39,377 participants between November and December 2013. A further 5202 residents were absent, while 763 residents refused examination. The age range of study participants ranged from 1 to 100 years ().
Table 1. Age and sex distribution of participants, Global Trachoma Mapping Project, Gombe State, 2013.
Across the 11 LGAs, we examined 15,374 children aged 1–9 years (7488 females and 7886 males); 606 children were absent and 449 refused examination. The state-wide crude TF prevalence in 1–9-year-olds was 0.5% (95% confidence interval, CI, 0.4–0.7%); there was no statistically significance difference in the TF prevalence between females (0.7%, 95% CI 0.5–0.9%) and males (0.4%, 95% CI 0.3–0.6%), with an odds ratio (females:males) of 1.5 (95% CI 1.0–2.4; χCitation2 = 3.4, p = 0.06).
A total of 20,165 persons aged 15 years and older were examined (12,390 females and 7775 males). In this age group, 3325 people were absent on the day of examination, and 292 refused examination. The state-wide crude trichiasis prevalence was 3.2% (95% CI 2.9–3.4%). The prevalence in females (3.4%, 95% CI 3.1–3.8%) was higher than in males (3.2%, 95% CI 2.9–3.4%), but there was no statistically significant difference between these prevalences; the female:male odds ratio was 0.9 (95% CI 0.8–1.0; χCitation2 = 1.7,p = 0.2).
LGA-level age-adjusted prevalences of TF in children aged 1–9 years are shown in and , and age- and sex-adjusted trichiasis prevalences in persons aged 15 years and older are shown in and .
Table 2. Local Government Area-level prevalences of trachomatous inflammation–follicular (TF) and trichiasis, Global Trachoma Mapping Project, Gombe State, 2013.
Figure 1. Prevalence of trachomatous inflammation–follicular (TF) in 1–9-year-old children, by Local Government Area, Global Trachoma Mapping Project, Gombe State, 2013.
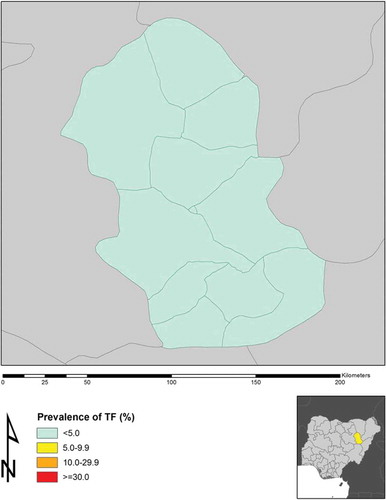
Figure 2. Prevalence of trichiasis in adults ≥15 years, by Local Government Area, Global Trachoma Mapping Project, Gombe State, 2013.
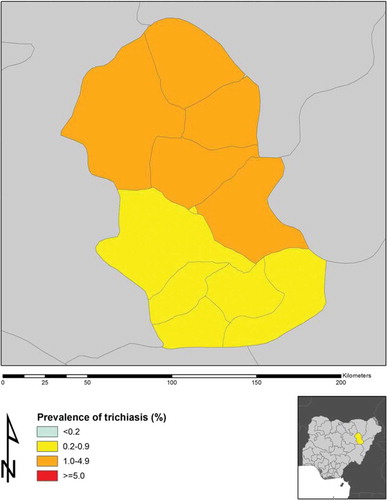
None of the LGAs had a TF prevalence >5%, but each LGA had a trichiasis prevalence above 0.2% in adults (equivalent to >1:1000 total populationCitation13), which requires intervention.
The estimated population of Gombe State is 2,365,040, and the trichiasis backlog is a little less than 20,000 individuals. Setting aside incident trichiasis, over 17,000 persons require trichiasis surgery to attain the elimination prevalence target for trichiasis in the state (). The LGAs with the greater trichiasis problem are located across the northern part of Gombe ().
Table 3. Local Government Area-level estimates of trichiasis surgery backlog, Global Trachoma Mapping Project, Gombe State, 2013.
Access of households to water and sanitation facilities ranged widely across the state. Access to improved water for hygiene purposes ranged from 14% in Kwami to 72% in Gombe LGA, while access to improved latrine facilities ranged from 8% in Balanga to 80% in Dukku ().
Table 4. Household access to wash water and improved latrines by Local Government Area, Global Trachoma Mapping Project, Gombe State, 2013.
Discussion
Trachoma appears to be a disappearing disease in Gombe State, considering that none of the LGAs had TF prevalences in children at or above the 5% elimination threshold set by WHO. This is similar to the picture in neighboring Bauchi State, where only two LGAs qualify for one round of mass azithromycin administration, but contrast with the picture in the northern neighboring state of Yobe, which has an active trachoma problem.Citation5,Citation10 However, inadequate access to improved water and sanitation facilities in some Gombe LGAs needs to be rectified, to help prevent possible recrudescence of active trachoma there.Citation14 To sustain the process of eliminating trachoma (and for other wide ranging benefits to the local population)Citation14,Citation15 there is a need for governments, water and sanitation agencies and other partners to prioritize provision of these facilities in Balanga, Nafada, Shongom and Kwami LGAs in particular, while improving on rather better circumstances noted in the other LGAs.
None of the LGAs qualified for mass drug administration of azithromycin for trachoma elimination pur-poses.Citation16 However, the prevalence of trichiasis is above the elimination threshold across Gombe, and there is a need to plan community-based eyelid surgery in order to clear the backlog of trichiasis cases. All LGAs require eyelid surgery interventions, but priority should be given to the five northern LGAs of Nafada, Funakaye, Dukku, Kwami, and Yamaltu/Deba, which border Yobe, a state in which trichiasis prevalence is high.Citation5 To attain elimination of trachoma from Gombe State, the emphasis should be on training and equipping eyelid surgeons, then deploying them to perform community-based surgery. Those with trichiasis normally reside in remote villages and do not have access to surgical services located in cities.Citation17 Surgical training should follow guidelines established by WHO.Citation18 If the trachoma program is to be successful in overcoming the trichiasis problem in Gombe, a system for finding patients with trichiasis through village promotion efforts will be required.Citation19 Emphasis must also be placed on supervision and support of trichiasis surgeons to ensure high productivity and delivery of a high quality service.Citation20
Gombe State would benefit from a trachoma program that delivers trichiasis surgery to the nearly 20,000 residents who need it to save their vision. In addition, improvements in water and sanitation are required.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This study was principally funded by the Global Trachoma Mapping Project (GTMP) grant from the United Kingdom’s Department for International Development (ARIES: 203145) to Sightsavers, which led a consortium of non-governmental organizations and academic institutions to support ministries of health to complete baseline trachoma mapping worldwide. The GTMP was also funded by the United States Agency for International Development (USAID) through the ENVISION project implemented by RTI International under cooperative agreement number AID-OAA-A-11-00048, and the END in Asia project implemented by FHI360 under cooperative agreement number OAA-A-10-00051. A committee established in March 2012 to examine issues surrounding completion of global trachoma mapping was initially funded by a grant from Pfizer to the International Trachoma Initiative. AWS was a Wellcome Trust Intermediate Clinical Fellow (098521) at the London School of Hygiene & Tropical Medicine. None of the funders had any role in project design, in project implementation or analysis or interpretation of data, in the decisions on where, how or when to publish in the peer reviewed press, or in preparation of the manuscript.
Additional information
Funding
References
- Kyari F, Murthy GVS, Sivsubramaniam S, et al. Nigeria National Blindness and Visual impairment study group. Prevalence of blindness and visual impairment in Nigeria: The National Blindness and Visual Impairment Survey. Invest Ophthalmol Visual Sci 2009;50:2033–2039.
- World Health Assembly. Global elimination of blinding trachoma. 51st World Health Assembly, Geneva, 16 May 1998, Resolution WHA51.11. Geneva: World Health Organization, 1998.
- Ferriman A. Blinding trachoma almost eliminated from Morocco. BMJ 2001;323(7326):1387.
- Ngondi J, Onsarigo A, Matthews F, et al. Effect of 3 years of SAFE (surgery, antibiotics, facial cleanliness, and environmental change) strategy for trachoma control in southern Sudan: a cross-sectional study. Lancet 2006;368(9535):589–595.
- Mpyet C, Ogoshi C, Goyol M. Prevalence of trachoma in Yobe state, north eastern Nigeria. Ophthalmic Epidemiol 2008;15:303–307.
- Mpyet C, Muhammad N, Mohammed A, et al. Prevalence of trachoma in Kano state, Nigeria: results of 44 district-level surveys. Ophthalmic Epidemiol (manuscript submitted for publication).
- Ramyil A, Wade P, Ogoshi C, et al. Prevalence of trachoma in Jigawa state, Northwestern Nigeria. Ophthalmic Epidemiol 2015;22:184–189.
- Solomon AW, Pavluck A, Courtright P, et al. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol 2015;22:214–225.
- Pavluck A, Chu B, Mann Flueckiger R, et al. Electronic data capture tools for global health programs: evolution of LINKS, an Android-, web-based system. PLoS Negl Trop Dis 2014;8:e2654.
- Mpyet C, Muhammad N, Adamu MD, et al. Prevalence of trachoma in Bauchi state, Nigeria: results of 20 local government area level surveys. Ophthalmic Epidemiol 2016. DOI:10.1080/09286586.2016.1238945
- Thylefors B, Dawson CR, Jones BR, et al. A simple system for the assessment of trachoma and its complications. Bull World Health Organ 1987;65:477–483.
- National Population Commission. 2006 population and housing census of the Federal Republic of Nigeria: national and state population and housing tables, priority tables (volume 1). Abuja: National Population Commission, 2009.
- World Health Organization. Report of the 2nd global scientific meeting on trachoma, Geneva, 25–27 August, 2003. Geneva: World Health Organization, 2003.
- Boisson S, Engels D, Gordon BA, et al. Water, sanitation and hygiene for accelerating and sustaining progress on neglected tropical diseases: a new Global Strategy 2015–20. Intl Health 2016;8(Suppl. 1):i19–i21.
- United Nations General Assembly. Resolution adopted by the General Assembly on 25 September 2015 (A/70/L.1). Transforming our world: the 2030 agenda for sustainable development. New York: United Nations, 2015.
- Solomon AW, Zondervan M, Kuper H, et al. Trachoma control: a guide for program managers. Geneva: World Health Organization, 2006.
- Bowman R, Sey O, Alexander N, et al. Should trichiasis be offered in the village? A community-randomised controlled trial of village vs community health center-based surgery. Trop Med Intl Health 2000;5:528–533.
- Merbs S, Resnikoff S, Kello AB, et al. Trichiasis surgery for trachoma (2nd ed). Geneva: World Health Organization, 2015.
- Mahande M, Tharaney M, Kirumbi E, et al. Uptake of trichiasis surgical services in Tanzania through two village based approaches. Br J Ophthalmol 2007;91:139–142.
- Lewallen S, Mahande M, Tharaney M, et al. Surgery for trachomatous trichiasis: findings from a survey of trichiasis surgeons in Tanzania. Br J Ophthalmol 2007;91:143–145.
Appendix
The Global Trachoma Mapping Project Investigators are: Agatha Aboe (1,11), Liknaw Adamu (4), Wondu Alemayehu (4,5), Menbere Alemu (4), Neal D. E. Alexander (9), Berhanu Bero (4), Simon J. Brooker (1,6), Simon Bush (7,8), Brian K. Chu (2,9), Paul Courtright (1,3,4,7,11), Michael Dejene (3), Paul M. Emerson (1,6,7), Rebecca M. Flueckiger (2), Allen Foster (1,7), Solomon Gadisa (4), Katherine Gass (6,9), Teshome Gebre (4), Zelalem Habtamu (4), Danny Haddad (1,6,7,8), Erik Harvey (1,6,10), Dominic Haslam (8), Khumbo Kalua (5), Amir B. Kello (4,5), Jonathan D. King (6,10,11), Richard Le Mesurier (4,7), Susan Lewallen (4,11), Thomas M. Lietman (10), Chad MacArthur (6,11), Colin Macleod (3,9), Silvio P. Mariotti (7,11), Anna Massey (8), Els Mathieu (6,11), Siobhain McCullagh (8), Addis Mekasha (4), Tom Millar (4,8), Caleb Mpyet (3,5), Beatriz Muñoz (6,9), Jeremiah Ngondi (1,3,6,11), Stephanie Ogden (6), Alex Pavluck (2,4,10), Joseph Pearce (10), Serge Resnikoff (1), Virginia Sarah (4), Boubacar Sarr (5), Alemayehu Sisay (4), Jennifer L. Smith (11), Anthony W. Solomon (1,2,3,4,5,6,7,8,9,10,11), Jo Thomson (4); Sheila K. West (1,10,11), Rebecca Willis (2,9).
Key: (1) Advisory Committee, (2) Information Technology, Geographical Information Systems, and Data Processing, (3) Epidemiological Support, (4) Ethiopia Pilot Team, (5) Master Grader Trainers, (6) Methodologies Working Group, (7) Prioritisation Working Group, (8) Proposal Development, Finances and Logistics, (9) Statistics and Data Analysis, (10) Tools Working Group, (11) Training Working Group.