
ABSTRACT
Purpose: To determine the prevalence of and risk factors for trachoma in selected local government areas (LGAs) of Kwara State, Nigeria.
Methodology: Population-based cross-sectional surveys were conducted in eight LGAs of Kwara State using Global Trachoma Mapping Project (GTMP) protocols. In each LGA, 25 villages were selected using probability-proportional-to-size sampling; 25 households were selected from each village using compact segment sampling. All residents of selected households aged ≥1 year were examined by GTMP-certified graders for trachomatous inflammation—follicular (TF) and trichiasis using the simplified trachoma grading scheme. Water, sanitation, and hygiene (WASH) data were also collected.
Results: A total of 28,506 residents were enumerated in 4769 households across the eight LGAs. TF prevalence in children aged 1–9 years ranged from 0.2% (95% CI 0.0–0.3%) to 1.3% (95% CI 0.7–2.1%), while trichiasis prevalence in persons ≥15 years was <0.2% in each LGA. Access to improved water source was the lowest in Edu (62%), while access to improved sanitation facilities was the lowest in Asa (6%) and the highest in Ilorin East (64%). Children aged 1–4 years had 0.63 (95% CI 0.40–0.99) times lower odds of having TF compared to children aged 5–9 years. Children in households with ≥5 resident 1–9-year-old children had 1.63 (95% CI 1.02–2.60) times greater odds of having TF compared to those in households with <5 resident children.
Conclusion: Trachoma is not a public health problem in Kwara State. Provision of adequate water and sanitation services should be a priority here, as a foundation for the health of the population.
Introduction
Trachoma is the principal cause of blindness of infectious origin worldwide.Citation1 In Africa, where an estimated 171 million people are at risk,Citation2 trachoma remains a significant public health problem in many areas, but until recently the district-level prevalence data necessary to prompt commitment of resources for interventions were vastly incomplete.Citation3,Citation4 The Global Trachoma Mapping Project (GTMP)Citation5 has now supported collection of those data for many more districts.
Infection of the conjunctival epithelium by particular strainsCitation6,Citation7 of the bacterium Chlamydia trachomatis stimulates a chronic inflammatory response, which may be sufficient for a diagnosis of the sign trachomatous inflammation—follicular (TF).Citation8 The principal reservoir of infection is in young children,Citation9 and this age group is therefore also most likely to have TF. Multiple infections with frequent or constant severe conjunctival inflammationCitation10–Citation12 may lead to conjunctival scarring and in-turning of the eyelashes. When misdirected eyelashes touch the eyeball, trachomatous trichiasisCitation8 is present. In some individuals, this results in irreversible visual impairment. The prevalence of trichiasis increases with age.Citation13,Citation14
There is no effective vaccine against C. trachomatis infection.Citation15 The World Health Organization (WHO) supports the use of the SAFE (surgery, antibiotics, facial cleanliness, environmental improvement) strategy against trachoma.Citation16 To achieve elimination of trachoma as a public health problem,Citation17,Citation18 community-based trichiasis surgical services should be offered wherever the prevalence of unmanaged trachomatous trichiasis in ≥15-year-olds is ≥0.2%, while the A, F, and E components of SAFE should be implemented wherever the prevalence of TF in 1–9-year-olds is ≥5%.
Nigeria is known to have a substantial burden of trachoma.Citation19–Citation25 Kwara State, in the west of the country, had a population of 2.4 million in 2006, the year for which the most recent census data are available.Citation26 Kwara State had not been previously surveyed for trachoma, and it was not known whether interventions would be required here. The purposes of this study were to estimate the district (local government area, LGA)-level prevalence of TF in 1–9-year-olds and of trichiasis in ≥15-year-olds, and to determine the proportion of households with access to improved water and sanitation facilities, in Kwara State. This information was necessary to guide appropriate implementation of the SAFE strategy.Citation27 Eight LGAs thought to have the greatest trachoma risk (due to their location to the north of the stateCitation24) were prioritized for survey implementation; decisions on whether or not to proceed with surveys in other LGAs rested on trachoma prevalence in this group of eight.
Methods
Trachoma graders and data recorders were trained and certified according to the standard operating procedures of the GTMP.Citation28 Version 2 of the GTMP training systemCitation29 was used. Grader trainees were required to pass both a slide-based test of diagnostic accuracy and a live subject-based inter-grader assessment test, while recorder trainees were required to pass an examination testing their data capture accuracy, as described previously.Citation28
In each LGA, a separate population-based prevalence survey was conducted according to the same principles and using the same systems. Details of sample-size calculation have been reported elsewhereCitation28; briefly, each survey was powered to estimate an expected TF prevalence in 1–9-year-olds of 10%, with an absolute precision of 3% and a design effect of 2.65, giving a desired minimum sample size of 1019.
Household selection
In each of the eight LGAs, 25 villages were selected using a systematic, probability-proportional-to-population-size methodology.Citation27 In selected villages, 25 households were selected using compact segment sampling.Citation30,Citation31
Data collection
All members of selected households aged ≥1 year were eligible to be included. Graders used ×2.5 magnifying loupes to examine both eyes of all consenting eligible individuals for trichiasis, TF, and trachomatous inflammation—intense (TI), defined according to the criteria of the WHO simplified grading system.Citation8 In accordance with a WHO global strategy,Citation32,Citation33 collection of water, sanitation, and hygiene (WASH) data was integrated into the survey format, with household-level WASH data generated through interviews with household members and assessment of sanitation facilities. All data were entered into the LINKS-GTMP app running on Android smartphones, which also automatically collected global positioning system coordinates for each household.Citation28 Data were uploaded to a secure cloud-based server once the phones were within range of a suitable network.Citation28,Citation34
Data analysis
Village-level proportions of children with TF were adjusted for age in 1-year age bands using 2006 census data.Citation26 Village-level proportions of adults with trichiasis were adjusted for gender and age in 5-year age bands using 2006 census data.Citation26 LGA-level prevalence was calculated as the means of the adjusted village-level proportions. Confidence intervals (CIs) were determined by bootstrapping adjusted cluster-level proportions, with replacement, over 10,000 replications.
We defined water sources and sanitation facilities as “improved” using the criteria established by the WHO/UNICEF Joint Monitoring Program (JMP) for Water Supply and Sanitation, as reported up to 2015.Citation35
Univariable and multivariable risk factor analyses were conducted using R 3.3.3 (2017; R Foundation for Statistical Computing, Vienna, Austria). We used a multilevel hierarchical model to account for clustering of TF in 1–9-year-olds at the village level. Additional adjustment for clustering at the LGA level did not significantly improve the model (likelihood ratio test (LRT), p = 0.1901). Prior to conducting multivariable analyses, we used Mantel–Haenszel tests of association to examine collinearity between explanatory variables, but this was not an absolute exclusion criterion. Univariable associations found to be statistically significant were included in the multivariable model (LRT, p < 0.10). Age and gender were included in the multivariable model a priori, and a stepwise inclusion approach was used to retain further variables in the final model if found to be statistically significant (LRT, p < 0.05).
Ethical considerations
Ethical approval was provided by the National Health Research Ethics Committee of Nigeria (NHREC/01/01/2007) and the ethics committee of the London School of Hygiene & Tropical Medicine (reference 6319). Consent was obtained verbally and documented electronically. Consent for individuals aged <15 years was given by a parent or guardian. Subjects noted to have active trachoma were given a course of 1% topical tetracycline eye ointment,Citation36 and those with trichiasis were referred to the nearest certifiedCitation37 trichiasis surgeon.
Results
A total of 28,506 residents were enumerated in 4769 households across the eight LGAs, which are shown in . In this population, 14,932 (52.4%) residents were female (). Graders examined 27,406 (96.1%) people in total; 859 (3.0%) people were absent for the examination and 238 (0.8%) people refused examination (). Of the examined individuals, 14,553 (53.1%) were female.
Table 1. Number of 1–9-year-old and number of ≥15-year-old resident, examined, absent, and refused; prevalence of trachomatous inflammation—follicular (TF); and prevalence of trichiasis; by Local Government Area (LGA), Global Trachoma Mapping Project, Kwara State, Nigeria, June and July, 2014.
Figure 1. Local Government Areas (LGAs) surveyed, and prevalence of trachomatous inflammation—follicular (TF) in 1–9-year-olds, by LGA, Global Trachoma Mapping Project, Kwara State, Nigeria, June and July, 2014.
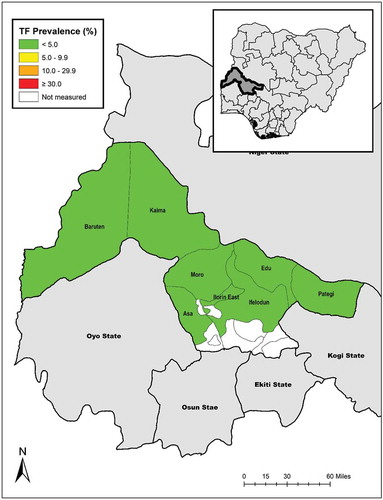
A total of 13,435 children aged 1–9 years were examined, of whom 6641 (49%) were female. The age-adjusted prevalence of TF in 1–9-year-olds ranged from 0.2% (95% CI 0.0–0.6%) in Edu to 1.3% (95% CI 0.7–2.1%) in Kaiama (, .
A total of 11,563 individuals aged ≥15 years were examined. Of those, 6732 (58%) were female. The highest age- and gender-adjusted prevalence of trichiasis in ≥15-year-olds was 0.17% (95% CI 0.0–0.3%) in Baruten. No individual examined in Edu or Kaiama had trichiasis ().
In each LGA except Baruten, over 60% of households had access to an improved source of water for face-washing within a 30-minute round trip. Household access to improved sanitation ranged from 6% in Asa to 64% in Ilorin East ().
Table 2. Household-level access to water and sanitation, by Local Government Area (LGA), Global Trachoma Mapping Project, Kwara State, Nigeria, June and July, 2014.
A histogram of TF prevalence by age in 1–9-year-olds is shown as . For the risk factor analysis with TF as the outcome variable, categorizing age dichotomously (1–4 years v 5–9 years, LRT, p = 0.047) was a better fit for the data than using 1-year age groups (LRT, p = 0.096). We therefore categorized age as 1–4 years and 5–9 years. Results of the univariable analysis are shown in .
Table 3. Univariable analysis of risk factors for trachomatous inflammation—follicular in 1–9-year-olds, Global Trachoma Mapping Project, Kwara State, Nigeria, June and July, 2014.
Figure 2. Prevalence of trachomatous inflammation—follicular (TF) by age among 1–9-year-olds, across eight surveyed Local Government Areas, Global Trachoma Mapping Project, Kwara State, Nigeria, June and July, 2014.
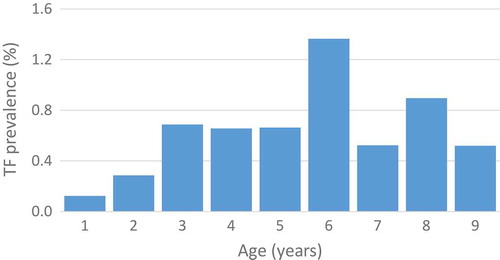
The full results of the multivariable analysis are shown in . Children aged 1–4 years had 0.63 (95% CI 0.40–0.99) times lower odds of having TF compared to children aged 5–9 years. Children in households with ≥5 children had 1.63 (95% CI 1.02–2.60) times greater odds of having TF compared to those in households with fewer than five children.
Table 4. Multivariable analysis of risk factors related to trachomatous inflammation—follicular in 1–9-year-olds, Global Trachoma Mapping Project, Kwara State, Nigeria, June and July, 2014.
Discussion
Trachoma is not a public health problem in any LGA of Kwara State. The LGA-level TF prevalence in 1–9 year-olds was <5%, and the trichiasis prevalence in ≥15-year-olds was <0.2% in each LGA surveyed. That is good news for Kwara and its people. Kogi State, which borders Kwara to the east, also enjoys prevalence of trachoma below those felt to represent a public health problem,Citation38 reinforcing the impression that deployment of the SAFE strategy for trachoma elimination may be required in the northern half of Nigeria,Citation24,Citation25,Citation39–Citation46 but not the southern half. Further trachoma mapping in Kwara State is not presently indicated.
Children aged 1–4 years examined as part of these surveys were less likely to have TF than those aged 5–9 years. The older age group includes those commencing primary school, where social interactions become more frequent, and therefore risk of ocular C. trachomatis infection from nonfamily members might be higher. However, this is pure speculation, and it is hard to understand why such hypothesized infections from classmates would not have been passed on to younger siblings. In any event, at TF prevalence as low as those recorded here, it is difficult to be certain that the follicular inflammation observed in the tarsal conjunctivae of any of our examinees was necessarily associated with C. trachomatis infection.Citation47–Citation50 We did not carry out laboratory tests for C. trachomatis.Citation51 Previous analyses of survey data from Nigeria found no significant difference in the odds of TF in school-going versus nonschool children.Citation52
In addition to the above limitation, we note that the work in Kwara State was implemented before the GTMP began to routinely collect data on the presence or absence of conjunctival scar in eyelids noted to have trichiasis; we are therefore unable to report whether the trichiasis we identified was likely to be due to trachoma or to be trichiasis of other etiologies.Citation53 In any case, the prevalence of all-trichiasis in adults was <0.2% in each LGA, so this omission does not affect our conclusion that elimination thresholds have been surpassed in this population. GTMP approaches are recognized to be of high epidemiological quality,Citation54,Citation55 and to provide an advance over the more individualized survey designsCitation56 implemented prior to the inception of the GTMP.
While most households had access to water sources to facilitate hygiene practices like keeping faces clean, access to sanitation was poor. Recent evidence has highlighted the likely importance of full community coverage and use of sanitation facilities for the elimination of trachoma.Citation57,Citation58 Until adequate sanitation services reach all communities, many will remain at risk for recrudescence of trachoma and for acquiring other infections that flourish in unsanitary environments. Greater efforts are needed here to accelerate progress on universal access to safe and sustainable water and sanitation.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the writing and content of this article.
Additional information
Funding
References
- Bourne RR, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990-2010: a systematic analysis. Lancet Glob Health. 2013;1(6):e339–49. doi:10.1016/S2214-109X(13)70113-X.
- World Health Organization. WHO Alliance for the Global Elimination of Trachoma by 2020: progress report on elimination of trachoma, 2014-2016. Wkly Epidemiol Rec. 2017;92(26):359–368.
- International Coalition for Trachoma Control. The End in Sight: 2020 INSight. Atlanta: International Coalition for Trachoma Control; 2011.
- Smith JL, Flueckiger RM, Hooper PJ, et al. The geographical distribution and burden of trachoma in Africa. PLoS Negl Trop Dis. 2013;7(8):e2359. doi:10.1371/journal.pntd.0002359.
- Solomon AW, Kurylo E. The global trachoma mapping project. Community Eye Health. 2014;27(85):18.
- Caldwell HD, Wood H, Crane D, et al. Polymorphisms in Chlamydia trachomatis tryptophan synthase genes differentiate between genital and ocular isolates. J Clin Invest. 2003;111(11):1757–1769. doi:10.1172/JCI17993.
- Hadfield J, Harris SR, Seth-Smith HMB, et al. Comprehensive global genome dynamics of Chlamydia trachomatis show ancient diversification followed by contemporary mixing and recent lineage expansion. Genome Res. 2017;27(7):1220–1229. doi:10.1101/gr.212647.116.
- Thylefors B, Dawson CR, Jones BR, West SK, Taylor HR. A simple system for the assessment of trachoma and its complications. Bull World Health Organ. 1987;65(4):477–483.
- Solomon AW, Holland MJ, Burton MJ, et al. Strategies for control of trachoma: observational study with quantitative PCR. Lancet. 2003;362(9379):198–204. doi:10.1016/S0140-6736(03)13909-8.
- West SK, Munoz B, Mkocha H, Hsieh YH, Lynch MC. Progression of active trachoma to scarring in a cohort of Tanzanian children. Ophthalmic Epidemiol. 2001;8(2–3):137–144. doi:10.1076/opep.8.2.137.4158.
- Wolle MA, Munoz BE, Mkocha H, West SK. Constant ocular infection with Chlamydia trachomatis predicts risk of scarring in children in Tanzania. Ophthalmology. 2009;116(2):243–247. doi:10.1016/j.ophtha.2008.09.011.
- Gambhir M, Basanez MG, Burton MJ, et al. The development of an age-structured model for trachoma transmission dynamics, pathogenesis and control. PLoS Negl Trop Dis. 2009;3(6):e462. doi:10.1371/journal.pntd.0000462.
- Courtright P, Sheppard J, Schachter J, Said ME, Dawson CR. Trachoma and blindness in the Nile Delta: current patterns and projections for the future in the rural Egyptian population. Br J Ophthalmol. 1989;73(7):536–540. doi:10.1136/bjo.73.7.536.
- Munoz B, Aron J, Turner V, West S. Incidence estimates of late stages of trachoma among women in a hyperendemic area of central Tanzania. Trop Med Int Health. 1997;2(11):1030–1038. doi:10.1046/j.1365-3156.1997.d01-186.x.
- Solomon AW, Mabey DC. Modeling the economic net benefit of a potential vaccination program against ocular infection with Chlamydia trachomatis. Vaccine. 2005;23(46–47):5281–5282. doi:10.1016/j.vaccine.2005.05.042.
- Francis V, Turner V. Achieving Community Support for Trachoma Control (WHO/PBL/93.36). Geneva: World Health Organization; 1993.
- World Health Assembly. Global Elimination of Blinding Trachoma. 51st World Health Assembly, Geneva, 16 May 1998, Resolution WHA51.11. Geneva: World Health Organization; 1998.
- World Health Organization. Validation of Elimination of Trachoma as a Public Health Problem (WHO/HTM/NTD/2016.8). Geneva: World Health Organization; 2016.
- Rabiu MM, Abiose A. Magnitude of trachoma and barriers to uptake of lid surgery in a rural community of northern Nigeria. Ophthalmic Epidemiol. 2001;8(2–3):181–190. doi:10.1076/opep.8.2.181.4167.
- Mpyet C, Solomon AW. Prevalence and causes of blindness and low vision in leprosy villages of north eastern Nigeria. Br J Ophthalmol. 2005;89(4):417–419. doi:10.1136/bjo.2004.048777.
- Jip NF, King JD, Diallo MO, et al. Blinding trachoma in Katsina state, Nigeria: population-based prevalence survey in ten local government areas. Ophthalmic Epidemiol. 2008;15(5):294–302. doi:10.1080/09286580802256542.
- Abdull MM, Sivasubramaniam S, Murthy GV, et al. Causes of blindness and visual impairment in Nigeria: the Nigeria national blindness and visual impairment survey. Inv Ophthalmol Vis Sci. 2009;50(9):4114–4120. doi:10.1167/iovs.09-3507.
- King JD, Jip N, Jugu YS, et al. Mapping trachoma in Nasarawa and Plateau States, central Nigeria. Br J Ophthalmol. 2010;94(1):14–19. doi:10.1136/bjo.2009.165282.
- Smith JL, Sivasubramaniam S, Rabiu MM, Kyari F, Solomon AW, Gilbert C. Multilevel analysis of trachomatous trichiasis and corneal opacity in Nigeria: the role of environmental and climatic risk factors on the distribution of disease. PLoS Negl Trop Dis. 2015;9(7):e0003826. doi:10.1371/journal.pntd.0003826.
- Mpyet C, Lass BD, Yahaya HB, Solomon AW. Prevalence of and risk factors for trachoma in Kano state, Nigeria. PLoS One. 2012;7(7):e40421. doi:10.1371/journal.pone.0040421.
- National Population Commission. 2006 Population and Housing Census of the Federal Republic of Nigeria: National and State Population and Housing Tables, Priority Tables (Volume 1). Abuja: National Population Commission; 2009.
- Solomon AW, Zondervan M, Kuper H, Buchan JC, Mabey DCW, Foster A. Trachoma Control: A Guide for Programme Managers. Geneva: World Health Organization; 2006.
- Solomon AW, Pavluck A, Courtright P, et al. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol. 2015;22(3):214–225. doi:10.3109/09286586.2015.1037401.
- Courtright P, Gass K, Lewallen S, et al. Global Trachoma Mapping Project: Training for Mapping of Trachoma (Version 2) [ Available At: http://Www.Trachomacoalition.Org/Node/357]. London: International Coalition for Trachoma Control; 2013.
- Kish L. Survey Sampling. New York: Wiley; 1965.
- Milligan P, Njie A, Bennett S. Comparison of two cluster sampling methods for health surveys in developing countries. Int J Epidemiol. 2004;33(3):469–476. doi:10.1093/ije/dyh096.
- Boisson S, Engels D, Gordon BA, et al. Water, sanitation and hygiene for accelerating and sustaining progress on neglected tropical diseases: a new Global Strategy 2015-20. Int Health. 2016;8(Suppl 1):i19–i21. doi:10.1093/inthealth/ihv073.
- World Health Organization. Water Sanitation & Hygiene for Accelerating and Sustaining Progress on Neglected Tropical Diseases: A Global Strategy 2015-2020. Geneva: World Health Organization; 2015.
- Pavluck A, Chu B, Mann Flueckiger R, Ottesen E. Electronic data capture tools for global health programs: evolution of LINKS, an Android-, web-based system. PLoS Negl Trop Dis. 2014;8(4):e2654. doi:10.1371/journal.pntd.0002654.
- World Health Organization, UNICEF. Progress on Sanitation and Drinking Water: 2015 Update and MDG Assessment. Geneva: UNICEF and World Health Organization; 2015.
- Evans JR, Solomon AW. Antibiotics for trachoma. The Cochrane Database Syst Rev. 2011;3:CD001860.
- Merbs S, Resnikoff S, Kello AB, Mariotti S, Greene G, West SK. Trichiasis Surgery for Trachoma. 2nd ed. Geneva: World Health Organization; 2015.
- Alada JJ, Mpyet C, Florea VV, et al. Prevalence of Trachoma in Kogi State, Nigeria: results of four Local Government Area-Level Surveys from the Global Trachoma Mapping Project. Ophthalmic Epidemiol. 2018;25(Sup 1):33–40. doi:10.1080/09286586.2017.1409359.
- Ramyil A, Wade P, Ogoshi C, et al. Prevalence of trachoma in Jigawa State, north-western Nigeria. Ophthalmic Epidemiol. 2015;22(3):184–189. doi:10.3109/09286586.2015.1037399.
- Mpyet C, Muhammad N, Adamu MD, et al. Trachoma mapping in Gombe State, Nigeria: results of 11 Local Government Area surveys. Ophthalmic Epidemiol. 2016;23(6):406–411. doi:10.1080/09286586.2016.1230633.
- Mpyet C, Muhammad N, Adamu MD, et al. Prevalence of trachoma in Katsina State, Nigeria: results of 34 District-Level surveys. Ophthalmic Epidemiol. 2016;23(Sup 1):55–62. doi:10.1080/09286586.2016.1236975.
- Mpyet C, Muhammad N, Adamu MD, et al. Prevalence of Trachoma in Bauchi State, Nigeria: results of 20 Local Government Area-level surveys. Ophthalmic Epidemiol. 2016;23(Sup 1):39–45. doi:10.1080/09286586.2016.1238945.
- Muhammad N, Mpyet C, Adamu MD, et al. Mapping trachoma in Kaduna State, Nigeria: results of 23 Local Government Area-level, population-based prevalence surveys. Ophthalmic Epidemiol. 2016;23(Sup 1):46–54. doi:10.1080/09286586.2016.1250918.
- Adamu MD, Mpyet C, Muhammad N, et al. Prevalence of trachoma in Niger State, North Central Nigeria: results of 25 population-based prevalence surveys carried out with the Global Trachoma Mapping Project. Ophthalmic Epidemiol. 2016;23(Sup 1):63–69. doi:10.1080/09286586.2016.1242757.
- Mpyet C, Muhammad N, Mohammed AD, et al. Prevalence of trachoma in Kano State, Nigeria: results of 44 Local Government Area-level surveys. Ophthalmic Epidemiol. 2017;24(3):195–203. doi:10.1080/09286586.2016.1265657.
- Muhammad N, Mohammed A, Isiyaku S, Adamu MD, Gwom A, Rabiu MM. Mapping trachoma in 25 local government areas of Sokoto and Kebbi states, northwestern Nigeria. Br J Ophthalmol. 2014;98(4):432–437. doi:10.1136/bjophthalmol-2013-303703.
- Solomon AW, Foster A, Mabey DC. Clinical examination versus Chlamydia trachomatis assays to guide antibiotic use in trachoma control programmes. Lancet Infect Dis. 2006;6(1):5–6; author reply 7-8. doi:10.1016/S1473-3099(05)70304-2.
- Baral K, Osaki S, Shreshta B, et al. Reliability of clinical diagnosis in identifying infectious trachoma in a low-prevalence area of Nepal. Bull World Health Organ. 1999;77(6):461–466.
- Macleod CK, Butcher R, Mudaliar U, et al. Low prevalence of Ocular Chlamydia trachomatis infection and Aactive trachoma in the Western division of Fiji. PLoS Negl Trop Dis. 2016;10(7):e0004798. doi:10.1371/journal.pntd.0004798.
- Harding-Esch EM, Edwards T, Mkocha H, et al. Trachoma prevalence and associated risk factors in The Gambia and Tanzania: baseline results of a cluster randomised controlled trial. PLoS Negl Trop Dis. 2010;4(11):e861. doi:10.1371/journal.pntd.0000861.
- Solomon AW, Peeling RW, Foster A, Mabey DC. Diagnosis and assessment of trachoma. Clin Microbiol Rev. 2004;17(4):982–1011. doi:10.1128/CMR.17.4.982-1011.2004.
- King JD, Odermatt P, Utzinger J, et al. Trachoma among children in community surveys from four African countries and implications of using school surveys for evaluating prevalence. Int Health. 2013;5(4):280–287. doi:10.1093/inthealth/iht027.
- World Health Organization Alliance for the Global Elimination of Trachoma by 2020. Second Global Scientific Meeting on Trachomatous Trichiasis. Cape Town, 4-6 November 2015 (WHO/HTM/NTD/2016.5). Geneva: World Health Organization; 2016.
- Engels D. The Global Trachoma Mapping Project: a catalyst for progress against neglected tropical diseases. Ophthalmic Epidemiol. 2016;23(sup1):1–2. doi:10.1080/09286586.2016.1257139.
- Heggen AE, Solomon AW, Courtright P. Perspectives of National Coordinators and Partners on the Work of the Global Trachoma Mapping Project. Ophthalmic Epidemiol. 2016;23(6):366–372. doi:10.1080/09286586.2016.1229795.
- Mpyet C, Kello AB, Solomon AW. Global elimination of trachoma by 2020: a work in progress. Ophthalmic Epidemiol. 2015;22(3):148–150. doi:10.3109/09286586.2015.1045987.
- Oswald WE, Stewart AE, Kramer MR, et al. Active trachoma and community use of sanitation, Ethiopia. Bull World Health Organ. 2017;95(4):250–260. doi:10.2471/BLT.16.177758.
- Garn JV, Boisson S, Willis R, et al. Sanitation and water supply coverage thresholds associated with active trachoma: modeling cross-sectional data from 13 countries. PLoS Negl Trop Dis. 2018;12:e0006110. doi:10.1371/journal.pntd.0006110.
Appendix
For the Global Trachoma Mapping Project: The Global Trachoma Mapping Project Investigators are: Agatha Aboe (1,11), Liknaw Adamu (4), Wondu Alemayehu (4,5), Menbere Alemu (4), Neal D. E. Alexander (9), Ana Bakhtiari (2,9), Berhanu Bero (4), Sarah Bovill (8), Simon J. Brooker (1,6), Simon Bush (7,8), Brian K. Chu (2,9), Paul Courtright (1,3,4,7,11), Michael Dejene (3), Paul M. Emerson (1,6,7), Rebecca M. Flueckiger (2), Allen Foster (1,7), Solomon Gadisa (4), Katherine Gass (6,9), Teshome Gebre (4), Zelalem Habtamu (4), Danny Haddad (1,6,7,8), Erik Harvey (1,6,10), Dominic Haslam (8), Khumbo Kalua (5), Amir B. Kello (4,5), Jonathan D. King (6,10,11), Richard Le Mesurier (4,7), Susan Lewallen (4,11), Thomas M. Lietman (10), Chad MacArthur (6,11), Colin Macleod (3,9), Silvio P. Mariotti (7,11), Anna Massey (8), Els Mathieu (6,11), Siobhain McCullagh (8), Addis Mekasha (4), Tom Millar (4,8), Caleb Mpyet (3,5), Beatriz Muñoz (6,9), Jeremiah Ngondi (1,3,6,11), Stephanie Ogden (6), Alex Pavluck (2,4,10), Joseph Pearce (10), Serge Resnikoff (1), Virginia Sarah (4), Boubacar Sarr (5), Alemayehu Sisay (4), Jennifer L. Smith (11), Anthony W. Solomon (1,2,3,4,5,6,7,8,9,10,11), Jo Thomson (4); Sheila K. West (1,10,11), Rebecca Willis (2,9).
Key: (1) Advisory Committee, (2) Information Technology, Geographical Information Systems, and Data Processing, (3) Epidemiological Support, (4) Ethiopia Pilot Team, (5) Master Grader Trainers, (6) Methodologies Working Group, (7) Prioritisation Working Group, (8) Proposal Development, Finances and Logistics, (9) Statistics and Data Analysis, (10) Tools Working Group, (11) Training Working Group.