
ABSTRACT
Caregiver satisfaction has the potential to promote equity for children living with HIV, by influencing health-seeking behaviour. We measured dimensions of caregiver satisfaction with paediatric HIV treatment in Nigeria, and discuss its implications for equity by conducting facility-based exit interviews for caregivers of children receiving antiretroviral therapy in 20 purposively selected facilities within 5 geopolitical zones. Descriptive analysis and factor analysis were performed. Due to the hierarchical nature of the data, multilevel regression modelling was performed to investigate relationships between satisfaction factors and socio-demographic variables. Of 1550 caregivers interviewed, 63% (95% CI: 60.6–65.4) reported being very satisfied overall; however, satisfaction varied in some dimensions: only 55.6% (53.1–58.1) of caregivers could talk privately with health workers, 56.9% (54.4–59.3) reported that queues to see health workers were too long, and 89.9% (88.4–91.4) said that some health workers did not treat patients living with HIV with sufficient respect. Based on factor analysis, two underlying factors, labelled Availability and Attitude, were identified. In multilevel regression, the satisfaction with availability of services correlated with formal employment status (p < .01), whereas caregivers receiving care in private facilities were less likely satisfied with both availability (p < .01) and attitude of health workers (p < .05). State and facility levels influenced attitudes of the health workers (p < .01), but not availability of services. We conclude that high levels of overall satisfaction among caregivers masked dissatisfaction with some aspects of services. The two underlying satisfaction factors are part of access typology critical for closing equity gaps in access to HIV treatment between adults and children, and across socio-economic groups.
Introduction
Globally, there are over 2.4 million children living with HIV who do not receive HIV treatment and care (UNAIDS, Citation2014b). Most of these children reside in sub-Saharan Africa where a persistent gap in access to antiretroviral therapy (ART) between adults and children constitutes a major inequity in the global HIV response (UNAIDS, Citation2014b). In 2014, less than one-third of children living with HIV received life-saving ART compared to 40% for adults and 66% for pregnant women among the 21 Global Plan priority countries (UNAIDS, Citation2014a). In Nigeria, only 12% of children living with HIV receive treatment and care which is among the lowest rates of ART coverage in the world (UNAIDS, Citation2014a, Citation2014b). Prominent among the factors related to this low coverage are limitations in policy and health systems infrastructure, such as limited decentralization of services, inadequate child-friendly Antiretroviral (ARV) formulations and ineffective case-finding strategies (McNairy et al., Citation2013). Most of these factors to date have focused primarily on the supply side (care provision) with little consideration for the demand side, for instance, caregivers’ perspectives on the quality of paediatric HIV services.
Prior studies indicate that primary caregivers play a major role in recognizing children’s needs and ensuring that their children enter and remain in health care (Cook et al., Citation2004; Logan & King, Citation2002). Parents’ satisfaction with the health services their children receive has been shown to influence utilization, length of service usage and to enhance relationships with healthcare providers (Cook et al., Citation2004). In the health sector, the definition of client satisfaction is anchored to the fulfilment of the individual’s desire for and expectations of health care (Kravitz, Citation1998). Zemencuk, Feightner, Hayward, Skarupski, and Katz (Citation1998) defined the patients’ desires as their perception of needing a given element of care. It is increasingly recognized that viewing health care “through patients” eyes’ is ethically and professionally imperative as the core purpose of health systems is to also help patients achieve their desires and expectations (Kravitz, Citation1998). In Nigeria, caregiver satisfaction with non-ART-related child health services was previously reported to vary among public health facilities (Iloh et al., Citation2013). However, in the provision of paediatric HIV services, there is a paucity of literature on caregiver satisfaction with HIV services for their children. This is one of the missing links for fully understanding the drivers of low coverage of paediatric ART and poor retention.
Few studies in health care have examined the relationship between caregiver satisfaction and equity in HIV care. In the business sector, however, many such studies abound with diverse findings on the relationship between customer satisfaction and equity (Fisk & Young, Citation1985). In developed countries, several studies have reported that utilization of health services in general hospital settings, after controlling for healthcare needs, promoted horizontal equity – meaning equal access for equal needs regardless of socio-economic differences (Lostao, Blane, Gimeno, Netuveli, & Regidor, Citation2014). Building on these studies, it can be postulated that satisfied caregivers are likely to improve utilization of services for their children living with HIV irrespective of their socio-economic differences resulting in equitable treatment access and outcomes.
In this study, we measured dimensions of caregiver satisfaction with HIV care services provided to their HIV-positive children in Nigeria, and assessed the relationship of underlying satisfaction factors with caregiver characteristics. To the best of our knowledge, this is the first study that assesses caregiver satisfaction with paediatric HIV and care. We anticipate that the findings may contribute significantly to the existing literature. The aim was to understand the implications of caregiver satisfaction on equity for their children and suggest how their perspectives on paediatric HIV treatment could be addressed within national HIV strategic planning and policy dialogues.
Methods
The study was multi-centre and facility-based that included exit interviews for caregivers of children living with HIV and receiving ART in selected facilities in Nigeria. This was conducted as part of larger paediatric HIV assessment supported by United Nations Children Fund and the World Health Organization. It was carried out in collaboration with the HIV/AIDS Division of the Federal Ministry of Health and members of the Paediatric sub-Committee of the National ART Task Team drawn from the academia and partner organizations. The eligibility criteria included a primary caregiver (a parent or member of the family) residing with and caring for the child aged less than 15 years living with HIV who visited the ART facility for a scheduled clinical appointment. ART facilities routinely kept updated appointment registers and folders containing medical records of children receiving HIV treatment and care. Based on Nigeria’s ART guidelines, the clinical appointments are scheduled to monitor clinical and immunological response to ART, screen for tuberculosis, track adherence, monitor adverse drug reactions and relevant laboratory parameters depending on each client’s condition.
Sampling and data sources
Purposive sampling was used to select a total of 20 public and private facilities offering paediatric ART services from 5 states (Anambra, Bayelsa, Benue, Kano and Lagos). These represented a mixture of high and low HIV burden in five geopolitical zones. The list of facilities was drawn from the Nigerian Health Facility Directory, and sorted by key domains for wide representation. These included urban/rural location, and facility level and ownership (public/private [for-profit and not-for-profit such as faith-based]).
We used records of clinic appointments from the selected facilities to estimate the number of caregivers to be enrolled for exit interviews. Using PASS 12 software®, (NCSS, Kaysville, Utah, USA, 2012) and adjusting for 20% non-response rate, a sample size of 1500 caregivers was required. This was then distributed proportionally to the population size of the facilities based on the number of patients ever enrolled in paediatric HIV treatment and care. A systematic selection of caregivers was done in each facility by randomly selecting the first caregiver using Excel “Rand” function followed by every third individual in the appointment register.
A structured questionnaire adapted from the 13-item patient satisfaction tool (Chimbindi, Barnighausen, & Newell, Citation2014) was used to collect information for assessing caregiver satisfaction with paediatric HIV treatment focusing on perceptions and evaluation of treatment received. This patient questionnaire has been validated in sub-Saharan African settings and has been used previously for patients receiving HIV treatment (Lyatuu, Msamanga, & Kalinga, Citation2008; Paddock, Veloski, Chatterton, Gevirtz, & Nash, Citation2000). The adaptation involved the caregivers’ responses regarding HIV treatment on behalf of their children. The questions were adapted to elicit caregiver perceptions on overall satisfaction, staff–caregiver communications, staff attitudes, privacy, confidentiality, staffing and amenities. The adaptation of the patient questionnaire used for caregivers was based on the premise that primary caregivers, particularly parents, have major role in recognizing their children’s needs and have strong impact on children’s use of ART medication. It was also presumed that caregiver perceptions and expectations of services provided to their children do have major influence on access and adherence to paediatric HIV treatment.
Outcomes and data analysis
The main outcome of the study was caregiver satisfaction and its underlying factors. Socio-demographic data associated with satisfaction factors included age, sex, marital status, level of education, employment, income status and facility ownership. Most of these are individual patient-level factors that have been found to influence patient satisfaction in previous studies (Quintana et al., Citation2006).
Descriptive analysis of the dimensions of caregiver satisfaction was performed, followed by a factor analysis with oblique rotation using the Promax method to identify underlying factors that explain satisfaction data. The oblique rotation was used based on the theoretical assumptions that the factors for patient satisfactions are correlated. In line with Kaiser criteria, those factors with eigenvalue >1.00 were retained after factor analysis. The rotated factor loadings were tabulated and a Scree plot was generated to visualize those factors with eigenvalue greater than 1.00. Retained factors were labelled based on the weights and number of loadings. Additionally, due to the hierarchical nature of data collected, of individuals nested within facilities and states, we performed a multilevel regression modelling to establish the relationship between the satisfaction factors identified and socio-demographic variables at statistical significance of α < 0.05. Random-effect equations were used to measure the variations at facility and state levels. All statistical analyses were completed using STATA version IC 11 (StataCorp LP, College Station, TX, USA, 2012).
Ethical considerations
Ethical clearance for the study was granted by National Health Research Ethics Committee of Nigeria (NHREC). Formal requests and approvals to visit facilities and perform exit interviews were also granted by the Federal and State Ministries of Health. Informed consents signed by the study participants were obtained before the exit interviews. Confidentiality of information from the caregivers was assured by removal of personal identifiers.
Results
A total of 1550 caregivers were interviewed, of which 1386 (89.4%) attended public facilities and 973 (62.8%) attended tertiary-level facilities providing paediatric HIV treatment and care. The socio-demographic characteristics of the caregivers are presented in . Most caregivers were females (1333 [86.1%]) with the median age of 33 years [interquartile range (IQR): 28–39], married, and over 62% earned less than NGN 18,000 per month.
Table 1. Socio-demographic characteristics of caregivers.
In total, 63.0% (95% CI: 60.6–65.4%) of caregivers were overall very satisfied, but the level of satisfaction among particular dimensions varied widely as depicted in .
Table 2. Dimensions of caregiver satisfaction.
Communication and health worker attitude
Most respondents (93.8%) reported that health workers fully discussed HIV treatment of their children with them; yet, only two-thirds found it easy to tell the health workers if they missed giving medication to their children. Despite the majority disagreeing that it was a problem that health workers did not speak caregivers’ language, approximately one-fifth thought that health workers were too busy to listen to their children’s problems. Similarly, almost 90% of caregivers agreed that some health workers did not treat patients living with HIV with sufficient respect. In contrast, almost 94% of respondents agreed that they, as caregivers, were treated with respect.
Privacy, confidentiality, staffing and services
The majority of respondents (90%) agreed that patient information was kept confidential in the health facilities they visited; however, only 55.6% reported that they were able to talk with the doctors or nurses in private. Additionally, approximately 57% of respondents admitted that the queues to see a health worker for services were too long. A similar proportion (57.3%) would have preferred to see a nurse in a nearby clinic than to travel further to see a doctor (32.2%) to access HIV services for their children. In order to improve services in the health facilities, most respondents suggested shorter queues (81.7%), making more health workers available to clients (80.2%), making health facilities cleaner (60.7%) and provision of better patient amenities such as waiting rooms or toilets (69.8%).
In the factor analysis of caregiver satisfaction, two underlying factors with eigenvalue above 1.00 were retained (). These two factors accounted for 93.8% of total variance in caregiver satisfaction. shows the factor loadings for each satisfaction variable. Based on factor loadings, we labelled Factor 1 as availability of services and Factor 2 as attitude of health workers. The labels capture the contents of different satisfaction variables that load heavily on the two retained factors.
Figure 1. Scree plot of eigenvalues.
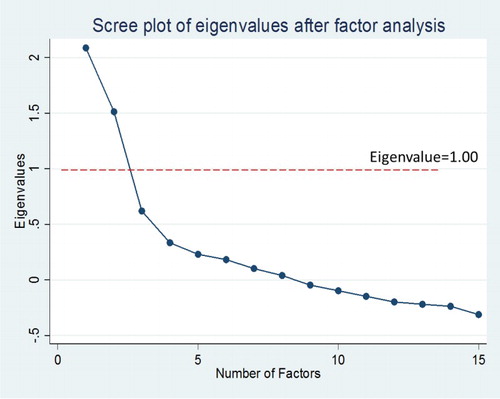
Table 3. Factor loadings after oblique rotation.
In multilevel regression modelling (), the level of satisfaction with availability of services had a positive association with formal employment status (p < .05), whereas those caregivers who received care in private facilities were less likely to be satisfied with both availability of services (p < .01) and attitude of health workers (p < .05). Analysis of random-effect parameters was used to measure the variations at facility and state levels and showed that states and facility levels did not influence the association between the levels of satisfaction with availability of services (p > .05), but had significant association with the attitude of the health workers (p < .01). The level of satisfaction was not associated with age, sex, marital status or income.
Table 4. Socio-demographic factor associated with caregiver satisfaction.
Discussion
Caregiver satisfaction with paediatric HIV services has the potential to influence access and outcomes of HIV, hence the importance of this study. In Nigeria, provision of high-quality care for children living with HIV was shown to improve outcomes by lowering loss to follow-up and decreasing mortality (Ojikutu et al., Citation2014). Despite this, there is limited evidence on the utility of caregiver satisfaction data in policy formulations in sub-Saharan Africa.
Our study found that approximately two-thirds of caregivers, while very satisfied overall with treatment offered to their children living with HIV, showed substantial variations in the levels of satisfaction regarding aspects of staff attitude, privacy, availability of services and waiting time to see health workers due to the long queues. This is consistent with previous studies that indicated that a high level of overall satisfaction masked substantial dissatisfaction with particular aspects of services (Chimbindi et al., Citation2014). It also confirmed findings of other studies that found waiting times due to long queues to be a main determinant of patient satisfaction (Dansky & Miles, Citation1997).
The finding that most caregivers preferred a nurse in a nearby facility rather than travelling further to see a doctor supports the need for a national policy on decentralization of paediatric HIV treatment and care in Nigeria. At the time of this study, paediatric ART was initiated only at secondary or tertiary levels of care. The potential effect of decentralization of services on increasing access to paediatric HIV services has been well documented (Fayorsey et al., Citation2013). Similarly, caregivers overwhelmingly preferred shorter queues and providing additional health workers, highlighting important strategies for improving paediatric HIV services. This is consistent with a study in Bangladesh that found a reduction in waiting time as more important to clients seeking for healthcare services (Mendoza Aldana, Piechulek, & al-Sabir, Citation2001). A preference for more health workers also reflects the limitation of current policy in Nigeria that only allows initiation of paediatric HIV treatment by medical doctors or specialist paediatricians. This underscores the need for task shifting in paediatric HIV services that could improve HIV services as observed in other countries (Kredo, Adeniyi, Bateganya, & Pienaar, Citation2014).
This study identified availability and attitude as the main factors underlying caregiver satisfaction. These factors are in agreement with two of the five dimensions of “access” taxonomy, proposed by Penchansky and Thomas (Citation1981). Later in Citation1984, Thomas and Penchansky described the relationship of satisfaction with access to services, further supporting the hypothesis that patients’ beliefs and perception are important determinants of health behaviour. Thus, the low levels of caregiver satisfaction with availability and attitude observed in this study might partly explain the reported low coverage of paediatric HIV treatment in Nigeria. The findings in this study are also consistent with other studies that identified provider behaviour, particularly respect and politeness, as the most powerful predictors of client satisfaction (Mendoza Aldana et al., Citation2001).
This study also demonstrated that only formal employment and receiving services in private health facility influenced the two underlying factors. A meta-analysis reported by Hall and Dornan (Citation1990) concluded that socio-demographic characteristics are at best a minor predictor of satisfaction. Other studies have also shown inconsistent relationships between patient socio-demographic characteristics and satisfaction (Jackson, Chamberlin, & Kroenke, Citation2001). The finding of a positive relationship between formal employment and the level of satisfaction on availability of services may be explained by the fact that formal employees are participants of the National Health Insurance Scheme (NHIS) that covers parents and up to 4 children under the age of 18 years in Nigeria (Mohammed, Sambo, & Dong, Citation2011). Similarly, other studies in Nigeria have indicated that formal employment was a strong predictor of willingness to pay for HIV care, as out-of-pocket payments in health is over 90% (Mbachu, Enabulele, Nwudele, Alegu, & Anwara, Citation2015; Odeyemi & Nixon, Citation2013). The inverse relationship between satisfaction and private facilities is likely due to unmet expectation of caregivers for the services in private facilities. This finding is in line with the “discrepancy model” of patient satisfaction by Fox and Storms (Citation1981) arguing that satisfaction is entirely relative, and defined in large part by the perceived discrepancy between a patient’s expectation and actual experience.
The findings on caregiver satisfaction have implications for the equity for children living with HIV receiving life-saving treatment. We have demonstrated that the underlying satisfaction factors, availability and health workers attitude, are critical dimensions of access to services. Improving access to paediatric HIV services is essential for closing the equity gap in access to ART between adults and children. The improved access and retention will likely improve equitable treatment outcomes between rich and poor, as income status did not influence our satisfaction data. Improved access across population groups will also reduce the possibility of “inverse inequity”, as suggested by Cesar Victora, where wealthier individuals benefit first from new and better interventions (Hargreaves, Davey, & White, Citation2013). In this study, we did not investigate the relationship between satisfaction and treatment outcomes – a future research question requiring further elucidation.
We also hypothesized that the influence of formal employment on satisfaction is most likely due to the access to Health Insurance Scheme which extends the coverage of care to children. This re-emphasizes the importance and need for universal health coverage, which has been shown to promote equity (Atun et al., Citation2013). Conversely, studies in the business sector have also shown that the relationship between satisfaction and equity is bi-directional with evidence indicating that perceived unfairness in service provision has led to customer dissatisfaction (Fisk & Young, Citation1985). A limitation of this study, however, is that we did not determine whether there were differences in the quality of services provided by selected facilities or states even though the levels of facility and state had significant influence on the attitude of health workers.
Acknowledgements
The authors would like to thank the members of Nigeria paediatric HIV assessment team, National HIV/AIDS and Sexually Transmitted Infection Control Program (NASCP) of the Federal Ministry of Health, UNICEF, and the World Health Organization for their support and contributions. Special gratitude goes to Drs Dorothy Mbori-Ngacha (UNICEF New York) and Chewe Luo (UNICEF New York) for their leadership throughout the assessment process. Authors’ contributions: Data analysis and first draft of the manuscript was developed by DC and extensively reviewed by LU, CA, DA, EO and CO. The field data collection was coordinated by EA, LU and CA while the rest of the co-authors led study teams in the states and reviewed the manuscript.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Atun, R., Aydin, S., Chakraborty, S., Sumer, S., Aran, M., Gurol, I., … Akdag, R. (2013). Universal health coverage in Turkey: Enhancement of equity. The Lancet, 382(9886), 65–99. doi:10.1016/S0140-6736(13)61051-X
- Chimbindi, N., Barnighausen, T., & Newell, M. L. (2014). Patient satisfaction with HIV and TB treatment in a public programme in rural KwaZulu-Natal: Evidence from patient-exit interviews. BMC Health Services Research, 14, 32. doi:10.1186/1472-6963-14-32
- Cook, J. A., Fitzgibbon, G., Burke-Miller, J., Mulkern, V., Grey, D. D., Heflinger, C. A., … Kelleher, K. (2004). Medicaid behavioral health care plan satisfaction and children’s service utilization. Health Care Financing Review, 26(1), 43–55.
- Dansky, K. H., & Miles, J. (1997). Patient satisfaction with ambulatory healthcare services: Waiting time and filling time. Hospital & Health Services Administration, 42(2), 165–177.
- Fayorsey, R. N., Saito, S., Carter, R. J., Gusmao, E., Frederix, K., Koech-Keter, E., … Abrams, E. J. (2013). Decentralization of pediatric HIV care and treatment in five sub-Saharan African countries. Journal of Acquired Immune Deficiency Syndromes, 62(5), e124–e130. doi: 10.1097/QAI.0b013e3182869558
- Fisk, R., & Young, C. (1985). Disconfirmation of equity expectations: Effects on consumer satisfaction with services. Advances in Consumer Research, 12, 340–345.
- Fox, J. G., & Storms, D. M. (1981). A different approach to sociodemographic predictors of satisfaction with health care. Social Science & Medicine A, 15(5), 557–564.
- Hall, J. A., & Dornan, M. C. (1990). Patient sociodemographic characteristics as predictors of satisfaction with medical care: A meta-analysis. Social Science & Medicine, 30(7), 811–818. doi: 10.1016/0277-9536(90)90205-7
- Hargreaves, J. R., Davey, C., & White, R. G. (2013). Does the ‘inverse equity hypothesis’ explain how both poverty and wealth can be associated with HIV prevalence in sub-Saharan Africa? Journal of Epidemiology & Community Health, 67(6), 526–529. doi:10.1136/jech-2012-201876
- Iloh, G., Ofoedu, J., Njoku, P., Okafor, G., Amadi, A., & Godswill-Uko, E. (2013). Satisfaction with quality of care received by patients without national health insurance attending a primary care clinic in a resource-poor environment of a tertiary hospital in Eastern Nigeria in the era of scaling up the Nigerian formal sector health insurance scheme. Annals of Medical and Health Sciences Research, 3(1), 31–37. doi:10.4103/2141-9248.109471
- Jackson, J. L., Chamberlin, J., & Kroenke, K. (2001). Predictors of patient satisfaction. Social Science & Medicine, 52(4), 609–620. doi: 10.1016/S0277-9536(00)00164-7
- Kravitz, R. (1998). Patient satisfaction with health care: Critical outcome or trivial pursuit? Journal of General Internal Medicine, 13(4), 280–282. doi: 10.1046/j.1525-1497.1998.00084.x
- Kredo, T., Adeniyi, F. B., Bateganya, M., & Pienaar, E. D. (2014). Task shifting from doctors to non-doctors for initiation and maintenance of antiretroviral therapy. Cochrane Database Systematic Review, 7, CD007331. doi:10.1002/14651858.CD007331.pub3
- Logan, D. E., & King, C. A. (2002). Parental identification of depression and mental health service use among depressed adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 41(3), 296–304. doi:10.1097/00004583-200203000-00009
- Lostao, L., Blane, D., Gimeno, D., Netuveli, G., & Regidor, E. (2014). Socioeconomic patterns in use of private and public health services in Spain and Britain: Implications for equity in health care. Health & Place, 25, 19–25. doi:10.1016/j.healthplace.2013.09.011
- Lyatuu, M. B., Msamanga, G. I., & Kalinga, A. K. (2008). Clients’ satisfaction with services for prevention of mother-to-child transmission of HIV in Dodoma Rural district. East African Journal of Public Health, 5(3), 174–179.
- Mbachu, C, Enabulele F, Nwudele T, Alegu S, Anwara K, & Obinna, O. (2015). Willingness to Pay for Antiretroviral drugs among HIV/AIDS clients in Ebonyi state, Nigeria Paper presented at the iHEA World Congress, Milan. Abstract retrieved from https://ihea2015.abstractsubmit.org/presentations/13970/
- McNairy, M. L., Lamb, M. R., Carter, R. J., Fayorsey, R., Tene, G., Mutabazi, V., … Abrams, E. J. (2013). Retention of HIV-infected children on antiretroviral treatment in HIV care and treatment programs in Kenya, Mozambique, Rwanda and Tanzania. Journal of Acquired Immune Deficiency Syndromes, 62(3), e70–81. doi:10.1097/QAI
- Mendoza Aldana, J., Piechulek, H., & al-Sabir, A. (2001). Client satisfaction and quality of health care in rural Bangladesh. Bull World Health Organ, 79(6), 512–517.
- Mohammed, S., Sambo, M. N., & Dong, H. (2011). Understanding client satisfaction with a health insurance scheme in Nigeria: Factors and enrollees experiences. Health Research Policy and Systems, 9, 20. doi:10.1186/1478-4505-9-20
- Odeyemi, I. A., & Nixon, J. (2013). Assessing equity in health care through the national health insurance schemes of Nigeria and Ghana: A review-based comparative analysis. International Journal for Equity in Health, 12, 9. doi:10.1186/1475-9276-12-9
- Ojikutu, B., Higgins-Biddle, M., Greeson, D., Phelps, B. R., Amzel, A., Okechukwu, E., … Hirschhorn, L. R. (2014). The association between quality of HIV care, loss to follow-up and mortality in pediatric and adolescent patients receiving antiretroviral therapy in Nigeria. PLoS One, 9(7), e100039. doi:10.1371/journal.pone.0100039
- Paddock, L. E., Veloski, J., Chatterton, M. L., Gevirtz, F. O., & Nash, D. B. (2000). Development and validation of a questionnaire to evaluate patient satisfaction with diabetes disease management. Diabetes Care, 23(7), 951–956. doi: 10.2337/diacare.23.7.951
- Penchansky, R., & Thomas, J. W. (1981). The concept of access: Definition and relationship to consumer satisfaction. Medical Care, 19(2), 127–140. doi: 10.1097/00005650-198102000-00001
- Quintana, J. M., Gonzalez, N., Bilbao, A., Aizpuru, F., Escobar, A., Esteban, C., … Thompson, A. (2006). Predictors of patient satisfaction with hospital health care. BMC Health Services Research, 6, 102. doi:10.1186/1472-6963-6-102
- Thomas, J. W., & Penchansky, R. (1984). Relating satisfaction with access to utilization of services. Medical Care, 22(6), 553–568. doi: 10.1097/00005650-198406000-00006
- UNAIDS. (2014a). 2014 Progress report on the global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive. Geneva: Author.
- UNAIDS. (2014b). The gap report. Geneva: Author.
- Zemencuk, J. K., Feightner, J. W., Hayward, R. A., Skarupski, K. A., & Katz, S. J. (1998). Patients’ desires and expectations for medical care in primary care clinics. Journal of General Internal Medicine, 13(4), 273–276. doi: 10.1046/j.1525-1497.1998.00080.x
