
ABSTRACT
Household economic strengthening (HES) is increasingly implemented alongside HIV programing to address economic drivers of the epidemic. The evidence base on HES for HIV outcomes is growing, and this evidence review aimed to comprehensively consolidate and synthesize the research linking 15 types of HES interventions with a range of HIV prevention and treatment outcomes. The review was conducted between November 2015 and October 2016 and consisted of an academic database search, citation tracking of relevant articles, examination of secondary references, expert consultation, and a gray literature search. Studies were included if they evaluated an HES intervention(s), reported on an HIV outcome(s), were available in English, and were relevant to low-income contexts or vulnerable populations. All evidence was assessed for quality. Over 108 citations were included and a matrix framework was used to map the evidence, linking each HES intervention with each HIV outcome, providing a precise visual depiction of the evidence base.
Given the volume of evidence, the results are presented and discussed in three papers, each focused on a different HIV outcome area. This is the first paper in the series and focuses on the 64 studies that reported HIV prevention outcomes. Conditional and unconditional cash transfers, and educational support were each associated with reductions in self-reported risk behaviors, particularly among adolescents. Food assistance in combination with other support also shows a positive trend for adolescent risk reduction. Most studies relied on self-reported behavioral data, and clinical outcomes such as HIV or other sexually transmitted infection (STI) incidence or prevalence were mostly null or underpowered, calling into question the true effectiveness of these interventions in preventing HIV. Limited evidence also supports the effectiveness of financial incentives in increasing voluntary medical male circumcision. Well-designed vocational/entrepreneurial training and savings interventions could bolster HIV prevention efforts for female sex workers, while findings are less conclusive for adolescents.
Introduction
Economic status has long been recognized as an important structural driver of the HIV epidemic (Gupta, Parkhurst, Ogden, Aggleton, & Mahal, Citation2008). Although the relationship between poverty and HIV is not linear (Kim, Pronyk, Barnett, & Watts, Citation2008), economic factors are linked to HIV risk behaviors, as well as outcomes at all stages of the HIV care and treatment cascade (Centers for Disease Control and Prevention, Citation2014). Poverty and economic insecurity can affect HIV risk by reducing negotiating power within sexual relationships (Eaton, Flisher, & Aarø, Citation2003), increasing reliance on transactional sex and sex work (Seeley et al., Citation2012), or limiting access to HIV prevention knowledge and services (Hargreaves et al., Citation2008).
Economic factors also pose barriers to HIV testing services (HTS) and routine access to care and treatment services for those who are positive, compromising the health and survival of people living with HIV (PLHIV). Transportation costs, time away from productive economic activities, and the costs of medical services are known barriers to care and treatment (Weiser et al., Citation2003). Poverty is also associated with food insecurity, which contributes to immunologic decline and reduces antiretroviral therapy (ART) adherence (Kalichman et al., Citation2014). Not accessing services and not adhering to treatment, in turn, have negative implications for onward transmission.
To address economic drivers of the epidemic, household economic strengthening (HES) initiatives are increasingly being implemented in coordination with biomedical and behavioral approaches to HIV prevention, treatment, and care. HES refers to a broad range of program approaches to improve economic wellbeing at the household level, often implemented as part of multi-sectoral interventions (Wolfe, Citation2009). The effects of HES interventions on HIV outcomes are likely mediated by structural and context-specific factors, however these interventions have the potential to mitigate economic vulnerability to HIV-related risk factors and help PLHIV overcome financial barriers to initiating and staying in care. In addition, the field of behavioral economics uses interventions that provide tangible economic rewards to influence decision-making and motivate specific prevention and treatment behaviors (Bassett, Wilson, Taaffe, & Freedberg, Citation2015; Galárraga, Genberg, Martin, Laws, & Wilson, Citation2013; Pettifor, MacPhail, Nguyen, & Rosenberg, Citation2012).
A growing body of evidence links HES interventions to HIV outcomes. This literature review was intended to comprehensively document the published and gray literature on a broad set of HES intervention types and their effects on a range of HIV outcomes. Given the volume of evidence, the review is presented in three papers, each focused on a different HIV outcome area: prevention, testing and linkage to care, and ART adherence and retention in care. This first paper in the series focuses on HIV prevention outcomes ().
Table 1. HIV outcomes assessed in full evidence review.
Methods
The methods cover the processes used for the complete review, including outcomes related to prevention, HTS and care and treatment.
Search strategy for full evidence review
The search methodology consisted of an academic database search, citation tracking of relevant articles, and an examination of existing evidence reviews for relevant primary articles. The initial search was completed using nine academic databases (PubMed, Embase, EconLit, Academic Search Premier, CINAHL Plus, Global Health, Web of Science, Campbell Collaboration, and Cochrane Library). Four consistent search strings were entered into each database using a list of HES interventions, plus terms associated with different HIV outcomes such as sexual risk behavior or ART adherence, or population groups such as orphans and vulnerable children (OVC) or female sex workers (FSW) (Appendix 1).
The literature search was conducted in November 2015 without restrictions on publication dates. Included evidence had to meet the following criteria: (1) evaluated one or more HES intervention of interest, (2) reported on at least one HIV outcome of interest, (3) available in English, and (4) relevant to low-income contexts or vulnerable populations. There were no geographic exclusion criteria, but studies conducted in high-income countries were only included in the review if the intervention and findings were relevant to low-income or otherwise vulnerable groups. Two reviewers screened titles and abstracts for inclusion; where insufficient information was available, the publication was included in the full-text review. Five percent of the abstracts (n = 160) were screened by both reviewers with 98.8% agreement in classification, and differences were resolved through consensus. Selected records then underwent a full-text review by the study author. There were no exclusion criteria based on study design. Data on study characteristics were extracted by two reviewers using a standard template.
Using a citation tracking approach, the reference sections of all selected papers were screened for additional pertinent research. An additional thirty-eight evidence reviews and policy papers identified in the initial screening were also reviewed for relevant source studies. For all primary studies identified through citation tracking, the same inclusion criteria were applied.
In July 2016, recommendations for additional evidence were solicited from experts in this field through a half-day consultative meeting. These recommendations were subsequently reviewed for inclusion. Finally, a gray literature search was conducted from September to October 2016 in which 15 websites of donors, conferences, and implementing organizations were searched using terms relevant to the review. The same inclusion criteria noted above were applied.
Study classification
We employed the Department for International Development's Assessing the Strength of Evidence methodology to appraise evidence quality from a wide range of study designs (DFID, Citation2014). This assessment tool has 20 questions grouped under seven principles of quality: conceptual framing, transparency, appropriateness, cultural sensitivity, validity, reliability, and cogency. This method was selected for its focus on development research and broad applicability. It assesses how well the study was conducted relative to the research question, and ratings are interpreted within the context of the study design and methods.
The methodology was standardized through the creation of a codebook for consistent scoring of each question (Appendix 2). Each of the 20 questions received a score of 1 (weak), 2 (moderate) or 3 (high). For each of the seven principles, the scores for each question were averaged, providing a principle score between 1 and 3. The scores for each principle were then summed, resulting in an overall quality score between 7 and 21. Studies were then rated based on pre-defined cut-off points as follows: 7.00 to 13.99 (low), 14.00 to 15.74 (medium), 15.75 to 17.49 (medium-high), and 17.50 to 21.00 (high). The rating parameters were based on average principle scores of less than 2.00 (low), 2.00 to 2.24 (medium), 2.25 to 2.49 (medium-high), and 2.50 to 3.00 (high). After two rounds of pre-testing, two reviewers completed the assessment, and 20% of the included studies, selected randomly, were reviewed jointly and discussed to support intercoder reliability. This assessment was only applied to written articles (n = 95) as there was insufficient information to complete the assessment for conference abstracts and presentations.
In addition to quality, studies were classified in terms of their direction(s) of effect. For quantitative studies, individual findings were classified as positive or negative if the results were statistically significant according to a p ≤ 0.05 threshold. Where tests of statistical significance were not conducted/presented, results were classified as null even when directional trends were strong. For qualitative studies, results were classified as positive or negative based on the qualitative data and interpretations presented.
Many studies in this review evaluated the effectiveness of integrated programs, grouping multiple HES, health, and/or social support components. The assessment of an independent relationship does not equate to attribution of the outcome to the intervention, but is an important consideration when evaluating the strength of evidence for each intervention. Therefore, studies were classified and analyzed based on whether they assessed the independent relationship between a specific HES component and the outcome(s) of interest.
Results
High level results are first presented for the complete evidence review, including studies related to prevention, HTS, and care and treatment. This is followed by a detailed discussion of results for prevention outcomes only.
Results for full evidence review
For the full evidence review the initial database search yielded 3164 unique records. Based on the abstract screening, 291 records underwent full-text review. This resulted in 56 relevant primary research studies that met inclusion criteria. Through citation tracking 91 additional full-text records were reviewed, 26 of which were included. Twenty-two additional studies were identified through participants at the consultative meeting, 16 of which met the inclusion criteria. Finally, 32 citations were identified through the gray literature search, and 10 were included. A total of 108 pieces of evidence were included in the review ().
Figure 1. PRISMA diagram on selection of studies for full review.
Study characteristics for full evidence review
Included studies were conducted in 24 countries across five continents. Variation was observed in the number of studies for each HES intervention and HIV outcome (). No studies were identified that assessed either asset transfers or microinsurance, therefore these interventions are not discussed.
Figure 2. Number of studies by HES intervention for full review.
Nearly 54% assessed a prevention outcome, including clinical outcomes, risk behaviors, and/or gender-based violence (GBV)/intimate partner violence (IPV) ().
Figure 3. Number of studies by HIV outcome for full review.
outlines the distribution of studies by quality rating
Figure 4. Number of studies by quality rating for full review.
Most studies (n = 80) were classified as having a positive direction of effect for at least one outcome, indicating they had positive findings on at least one primary indicator for that outcome, with no negative findings (though many had a mix of positive and null results across different indicators or sub-groups). Only 10% of the studies had any negative primary outcomes.
Almost half (45%) of the studies evaluated the effectiveness of integrated interventions with multiple components. Of these, few (18%) isolated the effects/associations of each intervention component, assessing both the combined and independent associations with the outcome of interest.
Evidence map
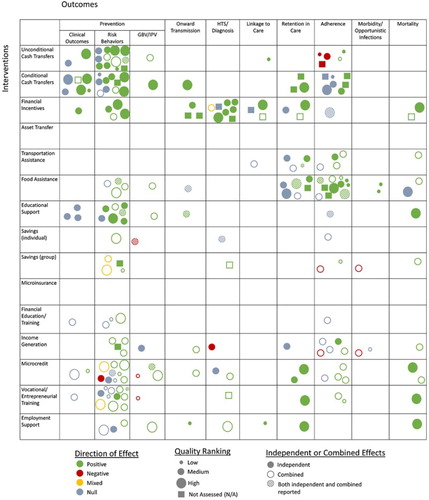
A matrix framework modeled from the International Initiative for Impact Evaluation Evidence Gap Map methodology was used to map evidence for each intervention onto each HIV outcome, creating a visual depiction of the overall evidence base (Snilstveit, Vojtkova, Bhavsar, Stevenson, & Gaarder, Citation2016) (). Each circle represents a single study and, within each cell, a study is only included once. Studies are included in multiple cells when they assessed more than one intervention or reported on multiple outcomes, or both. The characteristics mapped for each study are: study quality (represented by size), direction of effect (represented by color),Footnote1 and whether the study assessed the effects of that HES intervention independently or in combination with other program elements, or both (represented by shading). Studies with insufficient information to complete the quality assessment are depicted as squares and their size is unrelated to quality. Where multiple papers from the same study present different analyses of the same data and outcomes for an intervention-outcome pair are not substantively different, they are only captured once in the evidence map. Similarly, qualitative sub-studies that provide additional context for results previously reported are not captured in the evidence map.
Figure 5. HES and HIV outcomes evidence map for full review.
HES interventions can be classified into three categories: provision, protection, and promotion. Provision interventions directly provide economic resources to support basic needs and should target destitute households. Protection interventions help more economically stable households smooth consumption and mitigate shocks, and promotion interventions build the capacities of households capable of investing or assuming risk to grow their assets (Woller, Citation2011). The HES interventions in this review are grouped under these larger categories. Throughout this three-part series, results are presented by individual HES intervention, and are discussed in the context of these wider categories. Descriptions for each HES intervention are provided in .
Table 2. HES interventions assessed in full evidence review.
Results for prevention outcomes
Prevention outcomes were limited to clinical outcomes of HIV or sexually transmitted infection (STI) incidence or prevalence within the study population, behavioral risk factors such as self-reported condom use or partner reduction, and known vulnerabilities such as GBV or early marriage. Interventions with PLHIV aimed at disrupting onward transmission are also included. Less direct outcomes such as prevention knowledge or intentions were not included, nor were more distal outcomes such as alcohol abuse and school attendance. Most of the studies in this paper are based on self-reported measures of risk which can be susceptible to bias; this should be considered when interpreting the findings.
Given the diversity in study characteristics – geography, target group, intervention implementation, study design, sample size, outcome indicators, analysis methods, and overall study contexts – in most cases the studies in this review have only limited comparability. The summaries of literature for each intervention instead highlight patterns within these characteristics but do not seek to explicitly compare the studies. Even when the same outcome was measured, variation in these characteristics as well as different analysis methods make it difficult to directly compare effect sizes between studies. The study characteristics and effect sizes are summarized in –, providing important information when interpreting these results. Where studies included multiple HES interventions they are discussed in each relevant section. No studies with prevention outcomes included transportation assistance, so that intervention is not discussed in this paper.
Table 3. Studies of unconditional cash transfers on HIV prevention outcomes.
Table 4. Studies of conditional cash transfers on HIV prevention outcomes.
Table 5. Studies of financial incentives on HIV prevention outcomes.
Table 6. Studies of food assistance on HIV prevention outcomes.
Table 7. Studies of educational support on HIV prevention outcomes.
Table 8. Studies of savings on HIV prevention outcomes.
Table 9. Studies of financial education and training on HIV prevention outcomes.
Table 10. Studies of income generation on HIV prevention outcomes.
Table 11. Studies of microcredit on HIV prevention outcomes.
Table 12. Studies of vocational and entrepreneurial training on HIV prevention outcomes.
Table 13. Studies of employment support on HIV prevention outcomes.
Provision interventions
Unconditional cash transfers
Fourteen studies were identified that assessed unconditional cash transfers (UCTs) for HIV prevention outcomes, nine of which included government-administered transfers (). Of these, four were high quality, while three were medium-high, five were medium, and one was low quality; one was not assessed. Amounts ranged from USD 5 to USD 96 per month making them difficult to compare across contexts. Thirteen of the 14 studies assessed outcomes for adolescents, and one assessed risk among male sex workers (MSW), while none included a general adult population. The majority (n = 10) of the studies in this section assessed UCTs independently, making the evidence more compelling.
Of those focused on adolescents, six articles assessed the effects of the South African Child Support Grant and/or Foster Care Grant on adolescent risk behaviors and HIV incidence; four were from a single observational study that assessed the effects of “cash plus care”. Across all studies with adolescents, when looking at self-reported HIV risk behaviors such as sexual debut, sex frequency, condom use and number of partners, the study quality is high, and the directions of effect are positive for one or more outcome of interest, with no negative findings (Baird, Chirwa, McIntosh, & Ozler, Citation2015; Baird, Garfein, McIntosh, & Ozler, Citation2012; Cluver et al., Citation2013; Cluver, Orkin, Boyes, & Sherr, Citation2014; Cluver, Orkin, Meinck, Boyes, Yakubovich, et al., Citation2016; Cluver, Orkin, Yakubovich, & Sherr, Citation2016; DSD, SASSA, & UNICEF, Citation2012; Goodman, Kaberia, Morgan, & Keiser, Citation2014; Handa, Halpern, Pettifor, & Thirumurthy, Citation2014; Khoza et al., Citation2016; Rosenberg, Pettifor, Thirumurthy, Halpern, & Handa, Citation2014; Siaplay, Citation2012). Positive findings were seen more consistently for girls than boys.
A randomized controlled trial (RCT) conducted in Malawi also found promising clinical evidence (lower herpes simplex virus [HSV-2] and HIV prevalence in the intervention group), suggesting that the behavioral effects of UCTs could translate into lower likelihood of infection for adolescent females, though HIV incidence was not measured (Baird et al., Citation2012). However, findings of a follow-up study with the same population suggest that the effects of UCTs on sexual behaviors of adolescent females may not be sustained beyond the end of the intervention (Baird et al., Citation2015). Of the five studies that assessed UCTs in combination with different kinds of support for adolescents – including school support, food support, vocational training, income generation, agriculture training and health training – all indicate a positive result from these integrated interventions.
Only one study of UCTs was not conducted with an adolescent population. This smaller RCT with MSM in Mexico found that UCTs increased reported condom use, but there were no effects on partner reduction or on clinical outcomes of STI incidence, including HIV (Galárraga et al., Citation2017).
Conditional cash transfers
Thirteen studies provide evidence linking conditional cash transfers (CCTs) with HIV prevention, including one on prevention of mother-to-child transmission (PMTCT) (). Of these, four were high quality, while three were medium-high, three were medium, and one was low quality; two were not assessed. Eleven of the studies were based on data from RCTs, usually allowing for more direct measure of causality. Most (n = 10) also assessed CCTs independently. More than for any other intervention (n = 6 studies), clinical outcomes were assessed. Variation in the conditions – ranging from school attendance to negative STI test results – highlights the different pathways by which CCTs might influence HIV risk. For several studies, conditionality was tied to non-routine biomedical testing for HIV or STIs, which would be complicated and costly to administer in real-world settings. Like UCTs, the range of transfer amounts (USD 4–75) and variation in distribution frequency limits comparability.
Seven studies focused on an adolescent population. Five of these used experimental designs, four of which only included females. Most were conditioned on school attendance or performance, highlighting a common theory of change that keeping adolescents in school reduces HIV risk. Overall, studies with adolescents show a positive trend in reducing self-reported sexual risk behaviors such as frequent sex, unprotected sex and age-disparate sex, particularly for females (Baird et al., Citation2012; Baird, Chirwa, McIntosh, & Ozler, Citation2010; Khoza et al., Citation2016; Pettifor et al., Citation2016). In contrast, a study in Mexico with both male and female adolescents found no association between self-reported risk behaviors and CCTs comprised of cash and food and conditioned on school attendance and receipt of preventative medical care (Galárraga & Gertler, Citation2009).
Three CCT studies with adolescents assessed clinical outcomes and all used experimental designs. The study in Malawi by Baird and colleagues (Citation2012), referenced in the previous section, also found that CCTs conditioned on school attendance resulted in lower HSV-2 and HIV prevalence. Another study found CCTs conditioned on school attendance reduced self-reported IPV among females in South Africa (Pettifor et al., Citation2016), though there was no effect on HIV incidence. Another study in South Africa found CCTs conditioned on participation in a life skills program, educational performance, and HIV testing uptake reduced HSV-2 incidence among both boys and girls (Abdool Karim et al., Citation2015), but did not demonstrate impact on HIV incidence.
Among studies with adults, three papers were based on the RESPECT RCT in Tanzania, two of which also assessed clinical outcomes. They found that CCTs conditioned on negative STI test results reduced the likelihood of testing positive for STIs in younger adults, although HIV incidence was not assessed as an independent outcome (de Walque et al., Citation2012; de Walque, Dow, & Nathan, Citation2014). Initial reductions in self-reported sexual risk behaviors were not sustained after the end of the intervention (Packel, Dow, de Walque, Isdahl, & Majura, Citation2012). This is consistent with a study in Malawi that found no effect of a CCT conditioned on staying HIV-negative on adult clinical HIV status or risk behaviors after two years (Kohler & Thornton, Citation2012).
Two studies were conducted with other target populations. In the study of MSM in Mexico noted in the previous section, participants reported greater condom use as a result of CCTs conditioned on negative STI test results, but no effects were seen on STI or HIV incidence (Galárraga et al., Citation2017). Among HIV-positive pregnant women in the Democratic Republic of the Congo, CCTs conditioned on attending scheduled clinic visits and completing associated actions increased uptake and retention in PMTCT care, reducing the risk of vertical transmission (Yotebieng et al., Citation2016).
Financial incentives
Seven studies examined financial incentives and HIV prevention outcomes, all of which found positive results (). Of these, two were high quality, while one was medium-high, and three were medium quality; one was not assessed. All but one study examined financial incentives independently, providing greater confidence that the results are directly associated with the incentive. Incentive amounts ranged from USD 2.50–100, each of which incentivized unique behaviors.
An RCT in Lesotho examined a unique lottery scheme that incentivized negative test results for curable STIs, which reduced both the number of reported high risk sexual acts and HIV incidence among younger adults (Nyqvist, Corno, de Walque, & Svensson, Citation2015). Another study found that financial incentives combined with life skills education and sexual health promotion for adolescent minorities in the United States were associated with safer sex practices (Minnis et al., Citation2014).
In Kenya, three studies, two of which used experimental designs, assessed financial incentives to motivate uptake of voluntary male medical circumcision (VMMC) finding that fixed compensation amounts were effective, while a high-value lottery scheme was not (Evens et al., Citation2016; Thirumurthy et al., Citation2014; Thirumurthy et al., Citation2016). Two additional studies looked primarily at an HIV testing outcome but are included in this paper because of their focus on preventing onward transmission of the virus. The first found that incentives were associated with more pregnant women in India receiving HTS (Madhivanan et al., Citation2013); the second found incentives encouraged HIV-positive married men in Pakistan to disclose their HIV status and bring their wives in for testing, and were marginally associated with increased condom use (Khan, Qazi, Nazim, & Khan, Citation2012).
Food assistance
Seven references evaluated food assistance, all of which focus on adolescent populations and assess effects on self-reported sexual risk behaviors or sexual exploitation (). Of these, two were high quality, while one was medium-high, and four were medium quality. No food assistance studies used experimental designs or measured clinical outcomes.
Most of the evidence for this intervention comes from four papers from the same large prospective study looking at the combined effects of cash transfers, school feeding and/or food gardens as forms of “cash” assistance to adolescents in South Africa. These papers, which were also cited in the section on UCTs, found food aid was associated with lower risk behaviors in combination with other support, and independently for girls only (Cluver et al., Citation2014; Cluver, Orkin, Meinck, Boyes, Yakubovich, et al., Citation2016; Cluver, Orkin, Yakubovich, & Sherr, Citation2016). “Cash” (including school feeding) moderated the pathway from structural drivers of risk, to psychosocial problems, to HIV risk taking (Cluver, Orkin, Meinck, Boyes, & Sherr, Citation2016).
Another study in South Africa found a combined intervention, including home visits, and job support, income generating activities, and food gardens for some, was associated with lower HIV risk among former OVC (Visser, Zungu, & Ndala-Magoro, Citation2015). In contrast, a study in Mexico, also cited above under CCTs, found that bimonthly transfers in the form of food rations and financial assistance had no effect on adolescent risk (Galárraga & Gertler, Citation2009). Food assistance also did not reduce unprotected sex among HIV-positive adolescents in South Africa (Toska et al., Citation2016).
Educational support
Ten studies assessed the effects of school support on HIV outcomes and all focused on an adolescent population (). Two were high quality, while four were medium-high, and four were medium quality. All measured self-reported risk outcomes, though one was conducted with an HIV-positive population. Five studies used experimental designs and six assessed education support independently.
All but one study found at least some positive risk reduction outcomes, with no negative findings (Baird et al., Citation2010; Cho et al., Citation2017; Cluver, Orkin, Meinck, Boyes, & Sherr, Citation2016; Cluver, Orkin, Meinck, Boyes, Yakubovich, et al., Citation2016; Cluver, Orkin, Yakubovich, & Sherr, Citation2016; Hallfors et al., Citation2011; Hallfors et al., Citation2015; Luseno, Zhang, Rusakaniko, Cho, & Hallfors, Citation2015; Toska et al., Citation2016). Risk behaviors assessed include sexual debut, early marriage, pregnancy, unprotected sex, number of sexual partners, and transactional sex, among others, though there was variation among the studies in which behaviors were affected. A study, also noted in the previous section, found that school support was associated with less unprotected sex among HIV-positive adolescents in South Africa (Toska et al., Citation2016), lending further weight to the evidence for risk reduction effects, and indicating benefits may extend to reducing the risk of onward transmission.
Three studies also measured clinical outcomes. Two related studies, one of which used an experimental design, assessed HIV prevalence among adolescents in Zimbabwe and found no significant effects (Hallfors et al., Citation2015; Luseno et al., Citation2015). A third study also used an experimental design but lacked the power to detect a difference in HIV or HSV-2 incidence among adolescents in Kenya (Cho et al., Citation2017).
Protection interventions
Savings (individual and group)
Of the six savings studies identified, two focused on individual savings and four on group savings approaches (). Two savings studies were high quality, while one was medium-high, and two were medium quality; one was not assessed. Four studies were conducted with FSW and two with adolescent girls. All the studies in this section are based on combined interventions which included explicit health components, and only two studies examined the independent effects of savings: one had positive results, the other negative. Therefore, for the majority of studies, it is impossible to know whether the observed health effects were a result of the savings component, another intervention component, or the combined effects. None of the studies assessed clinical outcomes, all were based on self-reported risk factors.
The evidence from three studies with FSW, one of which used an experimental design, suggests that group or individual savings interventions combined with HIV risk reduction education/support may be protective for this population (Mantsios et al., Citation2016; Swendeman, Basu, Das, Jana, & Rotheram-Borus, Citation2009; Witte et al., Citation2015). Outcomes from a fourth study with FSW in India were less conclusive (Pillai, Bhattacharjee, Ramesh, & Isac, Citation2012).
In contrast, there were negative findings for adolescent girls in relation to sexual harassment for participants in a savings-only intervention in Uganda (Austrian & Muthengi, Citation2014). Reductions in ability to refuse sex and condom use over time were found among female adolescents in a multi-component intervention combining group savings with training on business management and reproductive health and formal microcredit in Kenya (Erulkar & Chong, Citation2005).
Financial capabilities education and training
Only three studies evaluated the effects of financial education on self-reported risk reduction (). All three used randomized designs, though one was rated as high quality, one medium-high, and one low quality. Each was conducted with a different target population: FSW, adolescents and out-of-school OVC. All three studies integrated financial education with other support, including other HES components and HIV risk reduction support, limiting any direct attribution to the financial education component.
Participation in an integrated intervention comprised of financial literacy, business development support, savings, and risk reduction training by FSW in Mongolia (also included in the saving section of this paper) was associated with fewer unprotected sex acts and fewer paying sex partners compared to risk reduction training alone (Witte et al., Citation2015). Female adolescent OVC in Zimbabwe reported reductions in risk behaviors over the period of an intervention that combined sexual health, life skills training, social support, financial literacy, and vocational training, but the results were not significantly different from controls (Dunbar et al., Citation2014). The study measured but was not powered to detect differences in HIV and HSV-2 incidence. A youth development activity in South Africa, including health and social capabilities training, and financial literacy for some, reported less risk behavior among boys in the intervention compared to controls, but tests of significance were not reported (Hallman & Roca, Citation2011).
Income generation
Six studies evaluated the effects of income generating activities (IGAs) on HIV prevention, half of which focused on adolescents (). Two of the studies in this section were medium-high quality while three were medium quality, and one was not assessed. None used a randomized design. Most of the studies assessed combined interventions, thereby limiting the direct connection between IGAs and HIV prevention outcomes. There was variation in the behavioral and structural outcomes measured and no clinical outcomes were assessed.
Youth involved in non-agricultural IGAs in Republic of Congo reported less unsafe sex (Bazika, Citation2007), while a study by Visser and colleagues, described under the food assistance section of this paper, found that a combined intervention in South Africa, including IGAs for some, was associated with lower HIV risk among former OVC in South Africa (Citation2015). Similarly, a combined HES intervention including IGAs, business and vocational training, and UCTs for OVC-headed households in Kenya was associated with lower self-reported risk among female participants but not males (Goodman et al., Citation2014).
A small study of drug-using FSW in the United States found positive associations between a combined risk reduction and IGA intervention and several risk reduction outcomes (Sherman, German, Cheng, Marks, & Bailey-Kloche, Citation2006). A qualitative study with an adult female population in Kenya reported that participation in an IGA was not protective against HIV risks, including IPV (Gnauck et al., Citation2013). A final qualitative study with an HIV-positive adult population in Kenya found an IGA plus an in-kind loan for farming inputs reduced behaviors associated with onward transmission of HIV (Zakaras et al., Citation2016).
Promotion interventions
Microcredit
Of the 10 microcredit studies identified, nine focused specifically on females (). Of these, two were high quality, while two were medium-high, four were medium, and two were low quality. Most evaluated combined interventions and only three assessed microcredit independently. Importantly, some of the interventions were designed to support highly vulnerable groups and built in protections to avoid harm, while others were less protective or flexible. GBV is associated with increased risk of HIV (Dunkle & Decker, Citation2013) and these outcomes were explored for microcredit services more than any other HES intervention.
Three papers focused on an RCT of an integrated microcredit, gender and HIV training and community mobilization intervention in South Africa, finding that participants experienced less IPV than controls (Pronyk et al., Citation2006), and women age 14–35 reported less unprotected sex (Pronyk et al., Citation2008). A third analysis from the same trial compared the integrated intervention to microcredit alone, and to a control group, finding that only the integrated intervention was associated with lower IPV while condom use outcomes were not statistically significant (Kim et al., Citation2009). Similarly, a study of adult females in Haiti found no independent association between involvement in microcredit and condom use among the full study population (Rosenberg, Seavey, Jules, & Kershaw, Citation2011).
In a qualitative study in Malawi, female fish traders reported that microcredit increased their vulnerability to HIV (MacPherson et al., Citation2015). In addition, two studies of combined sexual health and HES interventions, including microcredit, had negative findings for adolescent females. The first, was described previously and found decreases in ability to refuse sex and condom use over time in Kenya (Erulkar & Chong, Citation2005). The other found a qualitative association between participation in an HIV risk reduction, business support and microcredit intervention and higher exposure to harassment and sexual abuse in Zimbabwe (Dunbar et al., Citation2010).
Both microcredit studies with FSW found that combined interventions comprised of HIV risk reduction support and multiple HES components including microcredit, were associated with self-reported risk reduction, and one found a reduction in STI incidence though the study quality was low (Odek et al., Citation2009; Souverein et al., Citation2013). Finally, adult PLHIV in Kenya participating in a qualitative study cited in the previous section of this paper, reported reduced behaviors associated with onward transmission of HIV resulting from a combined intervention, including microcredit (Zakaras et al., Citation2016).
Vocational and entrepreneurial training
Eleven studies of vocational and entrepreneurial training measured HIV prevention outcomes (). Of these, two were high quality, while two were medium-high, four were medium, and three were low quality. These interventions were targeted at reducing risk among specific groups, including FSW (four studies) and adolescents (seven studies, five of which were delivered only to females). This evidence base is focused heavily on self-reported risk reduction outcomes.
Among adolescents, a previously described combined HES intervention including vocational training in Kenya was associated with lower reported risk among female OVC household heads, but not males (Goodman et al., Citation2014), while an RCT in Uganda found that girls in an integrated risk reduction and vocational training intervention reported lower sexual risk behaviors (Bandiera et al., Citation2012). Similarly, a combined vocational training and HIV risk-reduction intervention for youth in Uganda found reductions in sexual risk over the course of the intervention (Rotheram-Borus, Lightfoot, Kasirye, & Desmond, Citation2012). An RCT by Dunbar and colleagues described above found no significant risk reduction effects of integrated intervention for female OVC in Zimbabwe, and was underpowered to detect differences in clinical outcomes (Citation2014). Two studies described in previous sections of this paper of combined interventions with entrepreneurial training components had negative findings for adolescent females, including exposure to harassment and sexual abuse in Zimbabwe (Dunbar et al., Citation2010) and decreases in ability to refuse sex and condom use in Kenya (Erulkar & Chong, Citation2005). The two studies that independently evaluated this type of training for adolescents, one of which used an experimental design, found no independent associations or effects (Adoho, Chakravarty, Korkoyah, Lundberg, & Tasneem, Citation2014; Rotheram-Borus et al., Citation2012).
The four vocational/entrepreneurial training interventions delivered to FSW were combined with HIV prevention education, and in some cases other HES support. However, the three higher quality studies, two of which used randomized designs, found positive associations or effects on reported behaviors, including fewer sex partners, fewer paying partners, and increased condom use (Odek et al., Citation2009; Sherman et al., Citation2010; Witte et al., Citation2015). Only one small experimental study, assessed the independent effects of skills training for FSW, which found positive results for partner reduction compared to HIV education alone (Sherman et al., Citation2010). One low quality study found no association between a vocational training intervention combined with literacy, health and life skills education, and condom behaviors in this population (Lee et al., Citation2010).
Employment support
Four studies of employment support were identified (). One was high quality, while two were medium, and one was low quality. Three studies were conducted in sub-Saharan Africa and assessed risk reduction outcomes. An intervention for adolescents in South Africa, combining risk reduction with support to find work or establish a business, found reductions in IPV reported by females, but not in IPV perpetration reported by males (Jewkes et al., Citation2014). Another study in South Africa described elsewhere in this paper, found a combined intervention, including career guidance, was associated with lower HIV risk among former OVC (Visser et al., Citation2015). In contrast, an RCT assessed the independent effects of employment support for adolescents and found no association with reported condom use or partner reduction (Adoho et al., Citation2014).
The fourth study was conducted in the United States with a diverse population of PLHIV and found that use of vocational rehabilitation services was associated with less unprotected sex (Conyers & Boomer, Citation2014).
Ongoing studies
Three ongoing studies were also identified that focus on HIV prevention (). Two of these include savings services and financial services, which will bolster the evidence base for these interventions, and may allow for identification of stronger trends. One of the studies will measure STI prevalence, providing clinical evidence that is currently lacking for savings and financial capabilities.
The studies are investigating a range of combined interventions, two of which have an explicit HIV risk reduction component. However, two have factorial designs and the third is using a mixed-methods design to assess the relative contributions of intervention components and synergies between HES and HIV-specific components. Together they represent a shift from how combined HES and HIV interventions have been studied to date, since they are designed specifically to understand the contribution of the HES components to the outcomes.
Table 14. Ongoing studies of HIV prevention outcomes.
Discussion
Combining biomedical, behavioral, and structural approaches, tailored to different contexts, is essential for effective HIV prevention (Bekker, Beyrer, & Quinn, Citation2012). Increasingly, economic interventions, which work through several pathways to reduce risk, are being integrated into prevention programing. With 64 relevant pieces of research, the evidence for prevention is the strongest of the three broader outcome areas in this series. This research represents evidence from 17 countries, though over 78% of the studies were conducted in sub-Saharan Africa, compared to nearly 13% in Asia and over 9% in North America. Overall, 47% of the studies focused only on females, highlighting the disproportionate burden of HIV incidence borne by females, as well as a connection between economic insecurity and HIV risk, that is particularly salient for women and girls. By comparison only 6% of the studies focused on males, while 47% included both male and female participants. A slight majority of prevention studies (n = 33) focused on adolescent populations (of those 13 focused on female adolescents only), underscoring the importance of this population to global epidemic control. Most studies reported positive results, with only five reporting negative primary outcomes. This indicates a positive trend linking HES and HIV prevention, but could also reflect publication bias.
Most of the prevention research to date has focused on provision interventions, which are often easier to study because the causal link between intervention and outcome is more direct, and the intervention itself is generally more standardized. The strongest and most conclusive evidence for prevention also comes from provision interventions, with robust and positive results related to CCTs, UCTs, financial incentives, and educational support on risk behaviors with known linkages to HIV transmission.
Evidence for UCTs, CCTs, and education support is particularly positive in relation to adolescent risk reduction. For UCTs, positive findings were seen more consistently for girls than boys, which may be a result of the pathways through which they influence adolescent sexual behavior, such as reducing transactional sex and increasing school attendance, though only minimal data on the pathways of effects are presented in these studies. Interestingly, all 13 studies of UCTs for adolescent prevention were conducted in only three countries (South Africa, Malawi, and Kenya), which calls into question the applicability of these results in other contexts. Among CCT studies, the more consistent positive findings for adolescents compared to adults – especially when combined with the results of UCT studies – suggest an important window of opportunity in which CTs may have the greatest impact, particularly for females whose HIV risk is disproportionately higher during adolescence (Kharsany & Karim, Citation2016).
The evidence base for education support points to its effectiveness – provided either independently or in combination with other support – in reducing at least some self-reported HIV risk behaviors among vulnerable adolescents, particularly females. All the studies of food assistance evaluated integrated interventions that included educational, psychosocial, and/or economic support components, and only two were designed to assess food aid independently. This body of literature indicates, however, that the inclusion of food aid with other prevention services may support adolescent risk reduction, particularly among HIV-negative females.
Financial incentives may be particularly useful for motivating discrete or delimited behaviors. Compared to other HIV prevention outcomes, PMTCT is time-bound and linked to a well-defined set of actions and services for which financial incentives could be appropriate. The research to date is scant but indicates positive associations, and additional research is suggested. VMMC is also a natural area where financial incentives can directly influence a specific one-time behavior, and the limited evidence supports their effectiveness.
Beyond provision the evidence is far less conclusive. Studies on vocational and entrepreneurial training indicate that including this support could bolster HIV prevention efforts for FSW and possibly adolescents by reducing reliance on unsafe paid or transactional sex, though they must be designed carefully to avoid inadvertently increasing vulnerability. Studies of group and individual savings also show a protective trend for FSW. However, findings are mixed for adolescents, and while the evidence base is small, harmful gender-related outcomes warrant further investigation within this population. Given the limited comparability of the interventions themselves, varied study quality, and incongruous findings, the combination of group and individual savings forms one of the least conclusive evidence bases in this review. The evidence for IGAs suggests a positive trend, particularly in relation to female adolescent or OVC self-reported risk reduction. However, study quality is moderate and the variation in the interventions indicates these results are highly contextual. The variation in implementation, and in the behavioral and structural outcomes measured, partially account for the weak evidence bases for both IGAs and savings; however, their broad application in HIV-affected communities highlights both an opportunity and an imperative to better understand their effects on prevention outcomes through more rigorous studies.
The evidence base for microcredit is varied in quality. Of the three studies that assessed microcredit independently, only null and negative findings were reported. Interventions that integrated microcredit with other HES and health services have a more positive trend, but also include a few negative results. Results related to GBV were mixed, highlighting the complexity of microcredit programing and its potential to either mitigate or enhance risk depending on contextual factors. They point to the importance of carefully designing programs to avoid increasing women's vulnerability to HIV or GBV. For both financial capabilities education and employment support, there were small numbers of studies, varying study quality, and differences in target groups and in the overall interventions studied. Drawing conclusions in relation to these interventions is cautioned.
Only a handful of studies (n = 13) assessed clinical outcomes, while the majority relied on self-reported data which can be unreliable in relation to HIV risk behaviors (Schroder, Carey, & Vanable, Citation2003). Across all interventions where clinical data were measured, there is a trend of null and underpowered outcomes. Even for UCTs, CCTs, and education interventions, where findings for behavioral outcomes are among the strongest, the biological outcomes are far less conclusive. Of the six studies with positive clinical outcomes, only one reflects an effect on HIV incidence (Nyqvist et al., Citation2015). While nine studies measured HIV incidence, only three were powered to detect a difference between study arms and only one found this to be a statistically significant outcome. The discordance between the mostly positive self-reported behavioral outcomes and the less conclusive clinical outcomes highlights the possibility that the self-reported measures of HIV risk lack validity, or that the magnitude of effect of HES support on risk behavior is insufficient to reduce HIV incidence. The considerable funding and time required to rigorously assess HIV incidence has hindered adequate research in the HES field. However, well-powered and well-designed research is still needed to confirm whether HES can effectively contribute to HIV incidence reduction.
HES interventions can affect HIV outcomes through a myriad of potentially complex pathways. Overall, the qualitative evidence base was too limited to allow for any delineation of these causal pathways. As quantitative evidence continues to expand our understanding of which HES interventions are effective, additional qualitative and mixed-methods research is needed to understand the mechanisms of those effects.
A large proportion of the studies in this review assessed the effectiveness of integrated programs, grouping either multiple HES interventions and/or an HES intervention with health or other social interventions; most did so without being able to isolate the direct association or effect of any one intervention component. This provides evidence about what combinations of interventions are effective, but the contribution of each intervention component to the outcome(s) remains unknown.
Study limitations
Categorization into each intervention and outcome was done through thorough assessment of the context and descriptions provided in each study. Where these methodological details were limited, categorization was based on a careful assessment of available information. Although the quality assessment approach was selected for its applicability to this review, the use of a quality assessment introduces reviewer bias into the analysis. We attempted to mitigate this by creating a structured and defined codebook to minimize subjectivity for each aspect of the assessment, and two reviewers completed the assessment. Given the breadth and variation between the characteristics of studies in the review, the analytical framework that was used may not have allowed for the identification of additional trends.
Conclusions
The evidence in this review suggests that several HES interventions – particularly provision interventions such as UCTs, CCTs financial incentives and educational support – are effective in reducing self-reported HIV risk behaviors. The lack of similar positive evidence for clinical outcomes tempers the enthusiasm for these approaches and calls into question their true effectiveness in preventing HIV. Nonetheless, several high-quality studies rigorously measured and analyzed risk reduction outcomes, suggesting that these HES interventions may be an important component of risk reduction efforts in many contexts.
The comparatively limited and lower-quality evidence base for protection and promotion interventions demonstrates the need for additional research on their effectiveness for HIV prevention. As the field advances, stronger research designs are needed to understand how HES works within an integrated package of services, the causal pathways by which these interventions affect behavior change, and whether they affect clinical outcomes.
Acknowledgments
We would like to acknowledge the excellent work of Cheryl Tam, formerly of FHI 360, in screening and assessing the quality of articles included in this review. We are grateful to several FHI 360 colleagues, including Whitney Moret for her contributions to this manuscript, Allison Burns and Tamara Fasnacht for their support in the literature search, and Jenae Tharaldson for her assistance preparing the manuscript. Finally, we would like to thank the researchers, donors and practitioners who participated in the half-day consultative meeting held on July 13, 2016 for their thoughtful input and expertise on this topic. The contents are the responsibility of FHI 360 and do not necessarily reflect the views of USAID or the United States Government.
Disclosure statement
The author has no conflicts of interest to declare.
ORCID
Mandy Swann http://orcid.org/0000-0003-0348-8024
Additional information
Funding
Notes
1 Green (positive) = positive findings on one or more primary outcome of interest and no negative findings; blue (null) = no effect/association was observed on primary outcome(s) or study was under-powered; yellow (mixed) = a mix of positive and negative results on primary outcomes of interest; and red (negative) = negative findings on one or more primary outcomes of interest and no positive findings.
References
- Abdool Karim, Q., Leask, K., Kharsany, A., Humphries, H., Ntombela, F., Samsunder, N., … Abdool Karim, S. (2015). Impact of conditional cash incentives on HSV-2 and HIV prevention in rural South African high school students: Results of the CAPRISA 007 cluster randomized controlled trial; abstract TUAC0101LB. Paper presented at the 8th IAS Conference on HIV Pathogenesis, Treatment & Prevention.
- Adato, M., & Bassett, L. (2012). Social protection and cash transfers to strengthen families affected by HIV and AIDS. In M. Adato & L. Bassett (Eds.), Social protection and cash transfers to strengthen families affected by HIV and AIDS (pp. 1–3). Washington, DC: International Food Policy Research Institute.
- Adoho, F., Chakravarty, S., KorkoyahJr, D. T., Lundberg, M., & Tasneem, A. (2014). The impact of an adolescent girls employment program: The EPAG project in Liberia (Policy Research Working Paper - World Bank).
- Anema, A., Vogenthaler, N., Frongillo, E. A., Kadiyala, S., & Weiser, S. D. (2009). Food insecurity and HIV/AIDS: Current knowledge, gaps, and research priorities. Current HIV/AIDS Reports, 6(4), 224–231. doi: 10.1007/s11904-009-0030-z
- Austrian, K., & Muthengi, E. (2014). Can economic assets increase girls’ risk of sexual harassment? Evaluation results from a social, health and economic asset-building intervention for vulnerable adolescent girls in Uganda. Children and Youth Services Review, 47, 168–175. doi: 10.1016/j.childyouth.2014.08.012
- Baird, S., Chirwa, E., McIntosh, C., & Ozler, B. (2010). The short-term impacts of a schooling conditional cash transfer program on the sexual behavior of young women. Health Economics, 19, 55–68. doi: 10.1002/hec.1569
- Baird, S., Chirwa, E., McIntosh, C., & Ozler, B. (2015). What happens once the intervention ends? The medium-term impacts of a cash transfer programme in Malawi ( 3ie Grantee Final Report). New Delhi: Initiative for Impact Evaluation (3ie).
- Baird, S., Garfein, R. S., McIntosh, C. T., & Ozler, B. (2012). Effect of a cash transfer programme for schooling on prevalence of HIV and herpes simplex type 2 in Malawi: A cluster randomised trial. The Lancet, 379(9823), 1320–1329. doi: 10.1016/s0140-6736(11)61709-1
- Bandiera, O., Buehren, N., Burgess, R., Goldstein, M., Gulesci, S., Rasul, I., & Sulaiman, M. (2012). Empowering adolescent girls: Evidence from a randomized control trial in Uganda. Washington, DC: World Bank.
- Bassett, I. V., Wilson, D., Taaffe, J., & Freedberg, K. A. (2015). Financial incentives to improve progression through the HIV treatment cascade. Current Opinion in HIV and AIDS, 10(6), 451–463. doi: 10.1097/coh.0000000000000196
- Bazika, J. C. B. (2007). Effectiveness of small scale income generating activities in reducing risk of HIV in youth in the Republic of Congo. AIDS Care, 19, 23–24. doi: 10.1080/09540120601114444
- Becker, L. M., & Denicolo, P. (2012). Publishing journal articles. Los Angeles, CA: Sage.
- Bekker, L.-G., Beyrer, C., & Quinn, T. C. (2012). Behavioral and biomedical combination strategies for HIV prevention. Cold Spring Harbor Perspectives in Medicine, 2(8), a007435. doi: 10.1101/cshperspect.a007435
- Centers for Disease Control and Prevention. (2014). Understanding the HIV care continuum. Atlanta, GA: Author.
- Cho, H., Mbai, I., Luseno, W. K., Hobbs, M., Halpern, C., & Hallfors, D. D. (2017). School support as structural HIV prevention for adolescent orphans in western Kenya. Journal of Adolescent Health. doi: 10.1016/j.jadohealth.2017.07.015
- Cluver, L. D., Boyes, M., Orkin, M., Pantelic, M., Molwena, T., & Sherr, L. (2013). Child-focused state cash transfers and adolescent risk of HIV infection in South Africa: A propensity-score-matched case-control study. The Lancet Global Health, 1(6), e362–e370. doi: 10.1016/s2214-109x(13)70115-3
- Cluver, L. D., Operario, D., Lane, T., & Kganakga, M. (2012). “I can’t go to school and leave her in so much pain”: Educational shortfalls among adolescent “young carers” in the South African AIDS epidemic. Journal of Adolescent Research, 27(5), 581–605. doi: 10.1177/0743558411417868
- Cluver, L. D., Orkin, F. M., Boyes, M. E., & Sherr, L. (2014). Cash plus care: Social protection cumulatively mitigates HIV-risk behaviour among adolescents in South Africa. AIDS, 28(Suppl. 3), S389–S397. doi: 10.1097/qad.0000000000000340
- Cluver, L. D., Orkin, F. M., Meinck, F., Boyes, M. E., & Sherr, L. (2016). Structural drivers and social protection: Mechanisms of HIV risk and HIV prevention for South African adolescents. Journal of the International AIDS Society, 19(1), 20646. doi: 10.7448/IAS.19.1.20646
- Cluver, L. D., Orkin, F. M., Meinck, F., Boyes, M. E., Yakubovich, A. R., & Sherr, L. (2016). Can social protection improve sustainable development goals for adolescent health? PloS One, 11(10), e0164808. doi: 10.1371/journal.pone.0164808
- Cluver, L. D., Orkin, F. M., Yakubovich, A. R., & Sherr, L. (2016). Combination social protection for reducing HIV-risk behavior among adolescents in South Africa. Journal of Acquired Immune Deficiency Syndromes, 72(1), 96–104. doi: 10.1097/QAI.0000000000000938
- Conyers, L., & Boomer, K. B. (2014). Examining the role of vocational rehabilitation on access to care and public health outcomes for people living with HIV/AIDS. Disability and Rehabilitation, 36(14), 1203–1210. doi: 10.3109/09638288.2013.837968
- Deb, A., & Kubzansky, M. (2012). Bridging the gap: The business case for financial capability. New York, NY: Monitor Group and Citi Foundation.
- de Walque, D., Dow, W. H., & Nathan, R. (2014). Rewarding safer sex: Conditional cash transfers for HIV/STI prevention, volume 1 ( Policy Research Working Paper - World Bank). Washington, DC: World Bank.
- de Walque, D., Dow, W. H., Nathan, R., Abdul, R., Abilahi, F., Gong, E., … Medlin, C. A. (2012). Incentivising safe sex: A randomised trial of conditional cash transfers for HIV and sexually transmitted infection prevention in rural Tanzania. BMJ Open, 2(1), e000747. Retrieved from http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/448/CN-01018448/frame.html, http://bmjopen.bmj.com/content/2/1/e000747.full.pdf doi: 10.1136/bmjopen-2011-000747
- DFID. (2014). Assessing the strength of evidence. London: Author.
- DSD, SASSA & UNICEF. (2012). The South African child support grant impact assessment: Evidence from a survey of children, adolescents and their households. Pretoria: UNICEF South Africa.
- Dunbar, M. S., Kang Dufour, M.-S., Lambdin, B., Mudekunye-Mahaka, I., Nhamo, D., & Padian, N. S. (2014). The SHAZ! project: Results from a pilot randomized trial of a structural intervention to prevent HIV among adolescent women in Zimbabwe. PloS One, 9(11), e113621. doi: 10.1371/journal.pone.0113621
- Dunbar, M. S., Maternowska, M. C., Kang, M. J., Laver, S. M., Mudekunye-Mahaka, I., & Padian, N. S. (2010). Findings from SHAZ!: A feasibility study of a microcredit and life-skills HIV prevention intervention to reduce risk among adolescent female orphans in Zimbabwe. Journal of Prevention & Intervention in the Community, 38(2), 147–161, 115p. doi: 10.1080/10852351003640849
- Dunkle, K. L., & Decker, M. R. (2013). Gender-based violence and HIV: Reviewing the evidence for links and causal pathways in the general population and high-risk groups. American Journal of Reproductive Immunology, 69(Suppl. 1), 20–26. doi: 10.1111/aji.12039
- Eaton, L., Flisher, A. J., & Aarø, L. E. (2003). Unsafe sexual behaviour in South African youth. Social Science and Medicine, 56(1), 149–165. doi: 10.1016/S0277-9536(02)00017-5
- von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gotzsche, P. C., & Vandenbroucke, J. P. (2008). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Journal of Clinical Epidemiology, 61(4), 344–349. doi: 10.1016/j.jclinepi.2007.11.008
- Erulkar, A. S., & Chong, E. (2005). Evaluation of a savings & micro-credit program for vulnerable young women in Nairobi. In Promoting health, safe and productive transitions to adulthood. New York, NY: The Population Council.
- Evens, E., Lanham, M., Murray, K., Rao, S., Agot, K., Omanga, E., & Thirumurthy, H. (2016). Use of economic compensation to increase demand for voluntary medical male circumcision in Kenya: Qualitative interviews with male participants in a randomized controlled trial and their partners. Journal of Acquired Immune Deficiency Syndromes, 72(Suppl. 4), S316–S320. doi: 10.1097/QAI.0000000000001047
- Galárraga, O., Genberg, B. L., Martin, R. A., Laws, M. B., & Wilson, I. B. (2013). Conditional economic incentives to improve HIV treatment adherence: Literature review and theoretical considerations. AIDS and Behavior, 17(7), 2283–2292. doi: 10.1007/s10461-013-0415-2
- Galárraga, O., & Gertler, P. J. (2009). Conditional cash & adolescent risk behaviors: Evidence from urban Mexico. Policy Research Working Paper. Cuernavaca, Mexico: National Institute of Public Health.
- Galárraga, O., Sosa-Rubí, S. G., Kuo, C., Gozalo, P., Gonzalez, A., Saavedra, B., & Operario, D. (2017). Punto Seguro: A randomized controlled pilot using conditional economic incentives to reduce sexually transmitted infection risks in Mexico. AIDS Behavior, 21(12), 3440–3456. doi: 10.1007/s10461-017-1960-x
- Gnauck, K., Ruiz, J., Kellett, N., Sussman, A., Sullivan, M. A., Montoya, M., … Mwanthi, M. A. (2013). Economic empowerment and AIDS-related stigma in rural Kenya: A double-edged sword? Culture Health & Sexuality, 15(7), 851–865. doi: 10.1080/13691058.2013.789127
- Goodman, M. L., Kaberia, R., Morgan, R. O., & Keiser, P. H. (2014). Health and livelihood outcomes associated with participation in a community-based empowerment program for orphan families in semirural Kenya: A cross-sectional study. Vulnerable Children and Youth Studies, 9(4), 365–376. doi: 10.1080/17450128.2014.938142
- Guo, Y., Li, X., & Sherr, L. (2012). The impact of HIV/AIDS on children’s educational outcome: A critical review of global literature. AIDS Care, 24(8), 993–1012. doi: 10.1080/09540121.2012.668170
- Gupta, G. R., Parkhurst, J. O., Ogden, J. A., Aggleton, P., & Mahal, A. (2008). Structural approaches to HIV prevention. The Lancet, 372(9640), 764–775. doi: 10.1016/S0140-6736(08)60887-9
- Hallfors, D., Cho, H., Mbai, I., Milimo, B., & Itindi, J. (2012). Process and outcome evaluation of a community intervention for orphan adolescents in western Kenya. Journal of Community Health, 37(5), 1101–1109, 1109p. doi: 10.1007/s10900-012-9548-x
- Hallfors, D., Cho, H., Rusakaniko, S., Iritani, B., Mapfumo, J., & Halpern, C. (2011). Supporting adolescent orphan girls to stay in school as HIV risk prevention: Evidence from a randomized controlled trial in Zimbabwe. American Journal of Public Health, 101(6), 1082–1088. doi: 10.2105/AJPH.2010.300042
- Hallfors, D., Cho, H., Rusakaniko, S., Mapfumo, J., Iritani, B., Zhang, L., … Miller, T. (2015). The impact of school subsidies on HIV-related outcomes among adolescent female orphans. Journal of Adolescent Health, 56(1), 79–84. doi: 10.1016/j.jadohealth.2014.09.004
- Hallman, K., & Roca, E. (2011). Siyakha Nentsha: Building economic, health, and social capabilities among highly vulnerable adolescents in KwaZulu-Natal, South Africa. In Promoting healthy, safe, and productive transitions to adulthood (Vol. 4, pp. 1–4). New York, NY: The Population Council.
- Handa, S., Halpern, C. T., Pettifor, A., & Thirumurthy, H. (2014). The government of Kenya’s cash transfer program reduces the risk of sexual debut among young people age 15–25. PloS One, 9(1), e85473. doi: 10.1371/journal.pone.0085473
- Hargreaves, J. R., Bonell, C. P., Boler, T., Boccia, D., Birdthistle, I., Fletcher, A., … Glynn, J. R. (2008). Systematic review exploring time trends in the association between educational attainment and risk of HIV infection in sub-Saharan Africa. AIDS, 22(3), 403–414. doi: 10.1097/QAD.0b013e3282f2aac3
- Heise, L., Lutz, B., Ranganathan, M., & Watts, C. (2013). Cash transfers for HIV prevention: Considering their potential. Journal of the International AIDS Society, 16, 18615. doi: 10.7448/ias.16.1.18615
- Jewkes, R., Gibbs, A., Jama-Shai, N., Willan, S., Misselhorn, A., Mushinga, M., … Skiweyiya, Y. (2014). Stepping stones and creating futures intervention: Shortened interrupted time series evaluation of a behavioural and structural health promotion and violence prevention intervention for young people in informal settlements in Durban, South Africa. BMC Public Health, 14, 1325. doi: 10.1186/1471-2458-14-1325
- Johnson, J. B., Reynolds, H. T., & Mycoff, J. D. (2015). Political science research methods (8th ed., pp. 166–167). Los Angeles, CA: CQ Press.
- Kalichman, S. C., Hernandez, D., Cherry, C., Kalichman, M. O., Washington, C., & Grebler, T. (2014). Food insecurity and other poverty indicators among people living with HIV/AIDS: Effects on treatment and health outcomes. Journal of Community Health, 39(6), 1133–1139. doi: 10.1007/s10900-014-9868-0
- Khan, A., Qazi, R., Nazim, N., & Khan, A. (2012). Response to conditional cash transfers: Prevention of HIV infection in wives in Pakistan. Journal of the International AIDS Society, 15, 150.
- Kharsany, A. B. M., & Karim, Q. A. (2016). Hiv infection and AIDS in sub-Saharan Africa: Current status, challenges and opportunities. The Open AIDS Journal, 10, 34–48. doi: 10.2174/1874613601610010034
- Khoza, N., Stadler, J., MacPhail, C., Chikandiwa, A., Brahmbhatt, H., & Delany-Moretlwe, S. (2016). Exploring the consequences of cash transfers for adolescent boys and girls in inner city Johannesburg. Journal of the International AIDS Society, 19(Suppl. 5), 89.
- Kim, J., Ferrari, G., Abramsky, T., Watts, C., Hargreaves, J., Morison, L., … Pronykh, P. (2009). Assessing the incremental effects of combining economic and health interventions: The IMAGE study in South Africa. Bulletin of the World Health Organization, 87(11), 824–832. doi: 10.2471/BLT.08.056580
- Kim, J., Pronyk, P., Barnett, T., & Watts, C. (2008). Exploring the role of economic empowerment in HIV prevention. AIDS, 22(Suppl. 4), S57–S71. doi: 10.1097/01.aids.0000341777.78876.40
- Kohler, H.-P., & Thornton, R. L. (2012). Conditional cash transfers and HIV/AIDS prevention: Unconditionally promising? The World Bank Economic Review, 26(2), 165–190. Retrieved from http://wber.oxfordjournals.org/content/by/year doi: 10.1093/wber/lhr041
- Lankowski, A. J., Siedner, M. J., Bangsberg, D. R., & Tsai, A. C. (2014). Impact of geographic and transportation-related barriers on HIV outcomes in sub-Saharan Africa: A systematic review. AIDS and Behavior, 18(7), 1199–1223. doi: 10.1007/s10461-014-0729-8
- Lee, H., Pollock, G., Lubek, I., Niemi, S., O’Brien, K., Green, M., … Van Merode, T. (2010). Creating new career pathways to reduce poverty, illiteracy and health risks, while transforming and empowering Cambodian women’s lives. Journal of Health Psychology, 15(7), 982–992. doi: 10.1177/1359105310371703
- Luseno, W., Zhang, L., Rusakaniko, S., Cho, H., & Hallfors, D. (2015). Hiv infection and related risk behaviors: Does school support level the playing field between orphans and nonorphans in Zimbabwe? AIDS Care, 27(9), 1191–1195. doi: 10.1080/09540121.2015.1036726
- MacPherson, E., Sadalaki, J., Nyongopa, V., Nkhwazi, L., Phiri, M., Chimphonda, A., … Theobald, S. (2015). Exploring the complexity of microfinance and HIV in fishing communities on the shores of Lake Malawi. Review of African Political Economy, 42(145), 414–436. doi: 10.1080/03056244.2015.1064369
- Madhivanan, P., NiranjanKumar, B., Shaheen, R., Jaykrishna, P., Ravi, K., Gowda, S., … Krupp, K. (2013). Increasing antenatal care and HIV testing among rural pregnant women with conditional cash transfers to self-help groups: An evaluation study in rural Mysore, India. Journal of Sexually Transmitted Diseases, 2013, 971458. doi: 10.1155/2013/971458
- Mantsios, A., Shembilu, C., Mbwambo, J., Likindikoki, S., Beckham, S., Mwampashi, A., … Kerrigan, D. (2016). When you don’t have money, he controls you’’: Financial security, community savings groups, and HIV risk among female sex workers in Iringa, Tanzania. Journal of the International AIDS Society, 19(Suppl. 5), 155.
- Maxwell, J. A. (2012). Qualitative research design: An interactive approach (Vol. 41, pp. 39–41). Los Angeles, CA: Sage.
- Minnis, A. M., van Dommelen-Gonzalez, E., Luecke, E., Dow, W., Bautista-Arredondo, S., & Padian, N. S. (2014). Yo Puedo—A conditional cash transfer and life skills intervention to promote adolescent sexual health: Results of a randomized feasibility study in San Francisco. Journal of Adolescent Health, 55(1), 85–92. doi: 10.1016/j.jadohealth.2013.12.007
- Neuman, W. L. (2006). Social research methods: Qualitative and quantitative approaches. Boston, MA: Pearson.
- Nyqvist, M. B., Corno, L., de Walque, D., & Svensson, J. (2015). Using lotteries to incentivize safer sexual behavior: Evidence from a randomized controlled trial on HIV prevention ( Policy Research Working Paper - World Bank). Washington, DC: World Bank.
- Odek, W. O., Busza, J., Morris, C. N., Cleland, J., Ngugi, E. N., & Ferguson, A. G. (2009). Effects of micro-enterprise services on HIV risk behaviour among female sex workers in Kenya’s urban slums. AIDS and Behavior, 13(3), 449–461. doi: 10.1007/s10461-008-9485-y
- Packel, L., Dow, W. H., de Walque, D., Isdahl, Z., & Majura, A. (2012). Sexual behavior change intentions and actions in the context of a randomized trial of a conditional cash transfer for HIV prevention in Tanzania ( Policy Research Working Paper - World Bank). Washington, DC: World Bank.
- Pettifor, A., MacPhail, C., Hughes, J. P., Selin, A., Wang, J., Gómez-Olivé, F. X., … Kahn, K. (2016). The effect of a conditional cash transfer on HIV incidence in young women in rural South Africa (HPTN 068): A phase 3, randomised controlled trial. The Lancet Global Health, 4(12), e978–e988. doi: 10.1016/s2214-109x(16)30253-4
- Pettifor, A., MacPhail, C., Nguyen, N., & Rosenberg, M. (2012). Can money prevent the spread of HIV? A review of cash payments for HIV prevention. AIDS and Behavior, 16(7), 1729–1738. doi: 10.1007/s10461-012-0240-z
- Pillai, P., Bhattacharjee, P., Ramesh, B., & Isac, S. (2012). Impact of two vulnerability reduction strategies—collectivization and participation in savings activities on risk reduction among sex workers. Bangalore: Karnataka Health Promotion Trust.
- Pronyk, P. M., Hargreaves, J. R., Kim, J. C., Morison, L. A., Phetla, G., Watts, C., … Porter, J. D. H. (2006). Effect of a structural intervention for the prevention of intimate-partner violence and HIV in rural South Africa: A cluster randomised trial. The Lancet, 368(9551), 1973–1983. doi: 10.1016/S0140-6736(06)69744-4
- Pronyk, P. M., Kim, J. C., Abramsky, T., Phetla, G., Hargreaves, J. R., Morison, L. A., … Porter, J. D. H. (2008). A combined microfinance and training intervention can reduce HIV risk behaviour in young female participants. AIDS, 22(13), 1659–1665. doi: 10.1097/QAD.0b013e328307a040
- Rosenberg, M. S., Pettifor, A., Thirumurthy, H., Halpern, C. T., & Handa, S. (2014). The impact of a national poverty reduction program on the characteristics of sex partners among Kenyan adolescents. AIDS and Behavior, 18(2), 311–316. doi: 10.1007/s10461-013-0487-z
- Rosenberg, M. S., Seavey, B. K., Jules, R., & Kershaw, T. S. (2011). The role of a microfinance program on HIV risk behavior among Haitian women. AIDS and Behavior, 15(5), 911–918. doi: 10.1007/s10461-010-9860-3
- Rotheram-Borus, M. J., Lightfoot, M., Kasirye, R., & Desmond, K. (2012). Vocational training with HIV prevention for Ugandan youth. AIDS and Behavior, 16(5), 1133–1137. doi: 10.1007/s10461-011-0007-y
- Rutherford, S. (2000). The poor and their money. New Delhi: Oxford University Press.
- Schroder, K. E., Carey, M. P., & Vanable, P. A. (2003). Methodological challenges in research on sexual risk behavior: II. Accuracy of self-reports. Annals of Behavioral Medicine, 26(2), 104–123. doi: 10.1207/S15324796ABM2602_03
- Schulz, K. F., Altman, D. G., & Moher, D. (2010). CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Trials, 11, 32. doi: 10.1186/1745-6215-11-32
- Seeley, J., Watts, C. H., Kippax, S., Russell, S., Heise, L., & Whiteside, A. (2012). Addressing the structural drivers of HIV: A luxury or necessity for programmes? Journal of the International AIDS Society, 15(Suppl. 1), 1–4. doi:10.7448/IAS.19.1.20646
- Sherman, S. G., German, D., Cheng, Y., Marks, M., & Bailey-Kloche, M. (2006). The evaluation of the JEWEL project: An innovative economic enhancement and HIV prevention intervention study targeting drug using women involved in prostitution. AIDS Care, 18(1), 1–11. doi: 10.1080/09540120500101625
- Sherman, S. G., Srikrishnan, A. K., Rivett, K. A., Liu, S. H., Solomon, S., & Celentano, D. D. (2010). Acceptability of a microenterprise intervention among female sex workers in Chennai, India. AIDS and Behavior, 14(3), 649–657. doi: 10.1007/s10461-010-9686-z
- Siaplay, M. (2012). The impact of social cash transfers on young adults’ labor force participation, schooling, and sexual behaviors in South Africa. (Ph.D.), Oklahoma State University. Retrieved from https://auth.lib.unc.edu/ezproxy_auth.php?url=http://search.ebscohost.com/login.aspx?direct=true&db=ecn&AN=1404775&site=ehost-live&scope=site Available from EBSCOhost ecn database
- Snilstveit, B., Vojtkova, M., Bhavsar, A., Stevenson, J., & Gaarder, M. (2016). Evidence & gap maps: A tool for promoting evidence informed policy and strategic research agendas. Journal of Clinical Epidemiology, 79, 120–129. doi: 10.1016/j.jclinepi.2016.05.015
- Souverein, D., Euser, S. M., Ramaiah, R., Narayana Gowda, P. R., Shekhar Gowda, C., Grootendorst, D. C., … Den Boer, J. W. (2013). Reduction in STIs in an empowerment intervention programme for female sex workers in Bangalore, India: The Pragati programme. Global Health Action, 6, 22943. doi: 10.3402/gha.v6i0.22943
- Swann, M. (2018a). Economic strengthening for HIV testing and linkage to care: A review of the evidence. AIDS Care. doi: 10.1080/09540121.2018.1476665
- Swann, M. (2018b). Economic strengthening for retention in HIV care and adherence to antiretroviral therapy: A review of the evidence. AIDS Care. doi: 10.1080/09540121.2018.1479030
- Swendeman, D., Basu, I., Das, S., Jana, S., & Rotheram-Borus, M. J. (2009). Empowering sex workers in India to reduce vulnerability to HIV and sexually transmitted diseases. Social Science and Medicine, 69(8), 1157–1166. doi: 10.1016/j.socscimed.2009.07.035
- The Association for Qualitative Research. (n.d.). Qualitative research glossary. Retrieved from https://www.aqr.org.uk/glossary/
- Thirumurthy, H., Masters, S. H., Rao, S., Bronson, M. A., Lanham, M., Omanga, E., … Agot, K. (2014). Effect of providing conditional economic compensation on uptake of voluntary medical male circumcision in kenya. JAMA - Journal of the American Medical Association, 312(7), 703–711. doi: 10.1001/jama.2014.9087
- Thirumurthy, H., Masters, S. H., Rao, S., Murray, K., Prasad, R., Zivin, J. G., … Agot, K. (2016). The effects of providing fixed compensation and lottery-based rewards on uptake of medical male circumcision in Kenya: A randomized trial. Journal of Acquired Immune Deficiency Syndromes, 72(Suppl. 4), S309–S315. doi: 10.1097/QAI.0000000000001045
- Thompson, P. (2011, September 18). ‘signposting’ your journal articles and chapters. [Blog post]. Retrieved January 14, 2016, from http://patthomson.net/2011/09/18/signposting-your-journal-articles-and-chapters/
- Toska, E., Cluver, L. D., Boyes, M. E., Isaacsohn, M., Hodes, R., & Sherr, L. (2016). School, supervision and adolescent-sensitive clinic care: Combination social protection and reduced unprotected sex among HIV-positive adolescents in South Africa. AIDS and Behavior. doi: 10.1007/s10461-016-1539-y
- Visser, M., Zungu, N., & Ndala-Magoro, N. (2015). Isibindi, creating circles of care for orphans and vulnerable children in South Africa: Post-programme outcomes. AIDS Care, 27(8), 1014–1019. doi: 10.1080/09540121.2015.1018861
- Weiser, S. D., Wolfe, W., Bangsberg, D. R., Thior, I., Gilbert, P., Makhema, J., … Essex, M. (2003). Barriers to antiretroviral adherence for patients living with HIV infection and AIDS in Botswana. Journal of Acquired Immune Deficiency Syndromes, 34(3), 281–288. doi: 10.1097/00126334-200311010-00004
- Witte, S. S., Aira, T., Tsai, L. C., Riedel, M., Offringa, R., Mingway, C., … Ssewamala, F. (2015). Efficacy of a savings-led microfinance intervention to reduce sexual risk for HIV among women engaged in sex work: A randomized clinical trial. American Journal of Public Health, 105(3), e95–e102. doi: 10.2105/AJPH.2014.302291
- Wolfe, J. (2009). Household economic strengthening in Tanzania: Technical guidance for PEPFAR II programming. Washington, DC: United States Agency for International Development (DRAFT–used with permission).
- Woller, G. (2011). Livelihood and food security conceptual framework. Washington, DC: FHI 360, LIFT.
- Yotebieng, M., Thirumurthy, H., Moracco, K. E., Kawende, B., Chalachala, J. L., Wenzi, L. K., … Behets, F. (2016). Conditional cash transfers and uptake of and retention in prevention of mother-to-child HIV transmission care: A randomised controlled trial. The Lancet HIV, 3(2), e85–e93. doi: 10.1016/s2352-3018(15)00247-7
- Zakaras, J. M., Weiser, S. D., Hatcher, A. M., Weke, E., Burger, R. L., Cohen, C. R., … Dworkin, S. L. (2016). A qualitative investigation of the impact of a livelihood intervention on gendered power and sexual risk behaviors among HIV-positive adults in Rural Kenya. Archives of Sexual Behavior. doi: 10.1007/s10508-016-0828-x
Appendices
Appendix 1. Database search strings for full review
((((“HIV” OR “HIV/AIDS” OR “acquired immune deficiency syndrome” OR “acquired immunodeficiency syndrome”))) AND ((“school fees” OR “tuition payment” OR “bursaries” OR “school grants” OR “school facilitation” OR “education facilitation” OR “youth training” OR “workforce education” OR “workforce readiness” OR “economic strengthening” OR “microfinance” OR “micro-finance” OR “micro finance” OR microcredit OR microenterprise OR “micro-enterprise” OR “savings” OR “loan” OR “loans” OR “lending” OR “skills development” OR “skills building” OR “income generation” OR “income generating activity” OR “income generating activities” OR “food-for-work” OR “food for work” OR “cash-for-work” OR “cash for work” OR (“transfer” OR “transfers” AND (“cash” OR “asset”)) OR “financial incentives” OR “social protection” OR “livelihood” OR “livelihoods” OR “apprenticeship” OR (“voucher” OR “vouchers” OR “allowance” AND (“transport” OR “transportation” OR “travel”)) OR (“training” OR “trainings” OR “education” AND (“vocational” OR “entrepreneur” OR “entrepreneurship” OR “entrepreneurial” OR “finance” OR “financial”))))) AND ((“prevention” OR “prevent” OR “incidence” OR “transmission” OR “transmit” OR “acquire” OR “acquisition” OR PMTCT OR MTCT OR “behavior” OR “behaviour” OR “behaviors” OR “behaviours” OR “risk” OR “risks” OR “risky” OR “sexual activity” OR “sexual activities” OR “condom” OR “condoms” OR “male circumcision” OR “partner reduction” OR “number of partners”))
((((“HIV” OR “HIV/AIDS” OR “acquired immune deficiency syndrome” OR “acquired immunodeficiency syndrome”))) AND ((“HIV care” OR “home-based care” OR “home based care” OR “antiretroviral” OR “antiretroviral treatment” OR “ARV” OR “HAART” OR “adherence” OR “retention” OR “CD4” OR “viral load” OR “viral loads” OR “opportunistic infection” OR “opportunistic infections” OR “co-infection” OR “co-infections” OR “coinfection” OR “coinfections” OR “morbidity” OR “morbidities” OR “mortality” OR “mortalities”))) AND ((“school fees” OR “tuition payment” OR “bursaries” OR “school grants” OR “school facilitation” OR “education facilitation” OR “youth training” OR “workforce education” OR “workforce readiness” OR “economic strengthening” OR “microfinance” OR “micro-finance” OR “micro finance” OR microcredit OR microenterprise OR “micro-enterprise” OR “savings” OR “loan” OR “loans” OR “lending” OR “skills development” OR “skills building” OR “income generation” OR “income generating activity” OR “income generating activities” OR “food-for-work” OR “food for work” OR “cash-for-work” OR “cash for work” OR (“transfer” OR “transfers” AND (“cash” OR “asset”)) OR “financial incentives” OR “social protection” OR “livelihood” OR “livelihoods” OR “apprenticeship” OR (“voucher” OR “vouchers” OR “allowance” AND (“transport” OR “transportation” OR “travel”)) OR (“training” OR “trainings” OR “education” AND (“vocational” OR “entrepreneur” OR “entrepreneurship” OR “entrepreneurial” OR “finance” OR “financial”))))
((((“HIV” OR “HIV/AIDS” OR “acquired immune deficiency syndrome” OR “acquired immunodeficiency syndrome”))) AND ((“diagnosis” OR “HIV test” OR “HIV testing” OR “test results” OR “antibody test” OR “ELISA” OR “confirmatory test” OR “counselling and testing” OR “counseling and testing” OR VCT OR HTS))) AND ((“school fees” OR “tuition payment” OR “bursaries” OR “school grants” OR “school facilitation” OR “education facilitation” OR “youth training” OR “workforce education” OR “workforce readiness” OR “economic strengthening” OR “microfinance” OR “micro-finance” OR “micro finance” OR microcredit OR microenterprise OR “micro-enterprise” OR “savings” OR “loan” OR “loans” OR “lending” OR “skills development” OR “skills building” OR “income generation” OR “income generating activity” OR “income generating activities” OR “food-for-work” OR “food for work” OR “cash-for-work” OR “cash for work” OR (“transfer” OR “transfers” AND (“cash” OR “asset”)) OR “financial incentives” OR “social protection” OR “livelihood” OR “livelihoods” OR “apprenticeship” OR (“voucher” OR “vouchers” OR “allowance” AND (“transport” OR “transportation” OR “travel”)) OR (“training” OR “trainings” OR “education” AND (“vocational” OR “entrepreneur” OR “entrepreneurship” OR “entrepreneurial” OR “finance” OR “financial”))))
((((“HIV” OR “HIV/AIDS” OR “acquired immune deficiency syndrome” OR “acquired immunodeficiency syndrome”))) AND ((“orphans” OR “OVC” OR “OVCs” OR “most at risk” OR “key population” OR “key populations” OR “high risk” OR “injection drug” OR “who inject” OR IDU OR “intravenous drug” OR “needle sharing” OR PWID OR “men who have sex with men” OR “homosexual” OR MSM OR “commercial sex” OR “sex work” OR “sex worker” OR “sex workers” OR “prostitute” OR “prostitutes” OR “prostitution” OR “transactional sex” OR (“partner” OR “partners” OR “partnership” OR “partnerships” AND (“multiple” OR “concurrent”))))) AND ((“school fees” OR “tuition payment” OR “bursaries” OR “school grants” OR “school facilitation” OR “education facilitation” OR “youth training” OR “workforce education” OR “workforce readiness” OR “economic strengthening” OR “microfinance” OR “micro-finance” OR “micro finance” OR microcredit OR microenterprise OR “micro-enterprise” OR “savings” OR “loan” OR “loans” OR “lending” OR “skills development” OR “skills building” OR “income generation” OR “income generating activity” OR “income generating activities” OR “food-for-work” OR “food for work” OR “cash-for-work” OR “cash for work” OR (“transfer” OR “transfers” AND (“cash” OR “asset”)) OR “financial incentives” OR “social protection” OR “livelihood” OR “livelihoods” OR “apprenticeship” OR (“voucher” OR “vouchers” OR “allowance” AND (“transport” OR “transportation” OR “travel”)) OR (“training” OR “trainings” OR “education” AND (“vocational” OR “entrepreneur” OR “entrepreneurship” OR “entrepreneurial” OR “finance” OR “financial”))))
Appendix 2. Quality assessment codebook.
HES and HIV outcomes evidence review Evidence quality review code booka
