
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Resilience, positive growth in contexts of stress and adversity, is shaped by social ecological factors. Among people living with HIV, resilience is associated with myriad positive health benefits and improved health-related quality of life (HR-QoL). Identifying contextual factors associated with resilience among women living with HIV (WLWH) is particularly important as this population experiences many stressors and inequalities. We examined social-ecological factors associated with resilience and its relationship with HR-QoL among WLWH. We utilized baseline survey data from a national cohort of WLWH (n = 1424) in Canada. We conducted structural equation modelling using maximum likelihood estimation methods to test the direct effects of social support and women-centred HIV care (WCHC) on resilience, and the direct effects of resilience on mental and physical HR-QoL. We also tested the indirect effects of resilience on HR-QoL via HIV disclosure concerns and economic insecurity. Participant median age was 43 years (IQR = 35–50); most participants were women of colour (29% Black; 22% Indigenous; 7% other ethnicities; 41% Caucasian). Social support and WCHC were associated with increased resilience. The direct path from resilience to mental HR-QoL was significant, accounting for the mediation effects of economic insecurity and social support. The direct path from resilience to physical HR-QoL was significant, accounting for the mediation effects of economic insecurity. Economic insecurity partially mediated the relationship between resilience and mental HR-QoL and physical HR-QoL. HIV disclosure concerns partially mediated the relationship between resilience and mental-HR-QoL. Model fit indices suggested that the model fit the data well (χ2[14] = 160.378, P < 0.001; CFI = 0.987; RMSE = 0.048 [90% CI:0.042–0.080]; SRMR = 0.036). Findings suggest social (social support) and structural (WCHC) factors increase resilience. While resilience is associated with improved HR-QoL, social (HIV disclosure concerns) and structural (economic insecurity) factors partially mediate these associations and threaten HR-QoL. Multi-level interventions can address social ecological contexts to advance resilience and HR-QoL among WLWH.
KEYWORDS:
Introduction
Social and physical ecologies contribute to resilience, conceptualized as positive growth in contexts of stress and adversity (Ungar, Citation2011). Social ecological conceptual frameworks consider the complex, dynamic interactions between persons and their social, community and structural contexts, and how these contextual factors have proximal and distal influences on health outcomes (Stokols, Citation1996). Understanding contextual factors that provide the conditions where resilience can be nurtured is particularly salient to address among women living with HIV (WLWH). WLWH experience significant adversities and stress, in part due to social-environmental contexts of stigma, discrimination, and economic insecurity (Kumar, Gruskin, Khosla, & Narasimhan, Citation2015; Logie, Ahmed, Tharao, & Loutfy, Citation2017; Loutfy et al., Citation2015).
A rich body of literature has established that resilience is associated with positive health benefits among persons living with HIV (PLWH), including viral suppression (Dale et al., Citation2014), treatment adherence (Dale et al., Citation2014), and physical and mental health dimensions of health-related quality of life (HR-QoL) (Farber, Schwartz, Schaper, Moonen, & McDaniel, Citation2000; Fumaz et al., Citation2015; McGowan et al., Citation2018). Less studies with PLWH have explored social ecological pathways to resilience and its association with HR-QoL. This reflects large knowledge gaps in the resilience research literature regarding social ecological factors – beyond individual level predictors and outcomes – that can potentiate the development and health outcomes associated with resilience (Ungar, Citation2011).
Studies that apply a social ecological lens to understanding contexts that foster resilience among PLWH have largely focused on children (Betancourt, Meyers-Ohki, Charrow, & Hansen, Citation2013; Li, Chi, Sherr, Cluver, & Stanton, Citation2015), highlighting the important role of internal, family, and community resources. These studies conceptualize resilience among children living with HIV as dynamic and longitudinal, both shaped by and shaping interactions within the environment (Betancourt et al., Citation2013; Li et al., Citation2015). Studies have also highlighted the importance of community level factors such as social support as resources to foster resilience among PLWH (Bhat et al., Citation2015; Dageid & Grønlie, Citation2015; Earnshaw, Lang, Lippitt, Jin, & Chaudoir, Citation2015; Furlotte & Schwartz, Citation2017; Garcia-Dia, DiNapoli, Garcia-Ona, Jakubowski, & O’Flaherty, Citation2013; Mo, Lau, Yu, & Gu, Citation2014; Smith, Cook, & Rohleder, Citation2017). Studies with WLWH have examined resilience as a mediator in the relationship between social support and depressive symptoms (Simoni, Huang, Goodry, & Montoya, Citation2006).
Social ecological factors that may influence pathways from resilience to HR-QoL among WLWH include HIV disclosure concerns and economic insecurity. HIV disclosure fears and concerns are linked to poorer wellbeing and quality of life (Bhat et al., Citation2015; Blalock, Mcdaniel, & Farber, Citation2002; Degroote, Vogelaers, & Vandijck, Citation2014; Fekete, Williams, Skinta, & Bogusch, Citation2016) and poor mental health outcomes among PLWH (Hernansaiz-Garrido & Alonso-Tapia, Citation2017). Conversely, Kalichman, DiMarco, Austin, Luke, and DiFonzo (Citation2003) reported an association between safe disclosure and improved quality of life among PLWH, and this study revealed social support was associated with less disclosure concerns. A knowledge gap remains regarding the relationship between resilience and HIV disclosure concerns. The role of economic insecurity in mediating associations between resilience and quality of life is also understudied with WLWH. Economic insecurity is associated with lower quality of life (Douab et al., Citation2014) and poorer mental health (Riley et al., Citation2011, Citation2012) among PLWH, and may be particularly important to examine as WLWH may experience increased levels of poverty in comparison with their HIV negative counterparts (Normén et al., Citation2005).
An underexplored source of resilience among WLWH is receiving specialized, women-centred HIV care. Carter et al. (Citation2013) suggest that women-specific HIV services may improve women’s self-worth and self-advocacy. The receipt of women-centred HIV care (WCHC) may also contribute to resilience by addressing women’s unique needs, applying a person-centred care approach, and prioritizing strengths-based principles (O’Brien et al., Citation2017) that can empower WLWH to make decisions that better manage their own care (Medeiros, Citation2017).
This study was designed to apply a social ecological perspective to understand pathways to resilience, and from resilience to HR-QoL among WLWH in Canada. We examined pathways from social (social support) and structural (WCHC) resources to resilience, and pathways from resilience to mental and physical HR-QoL through social (HIV disclosure concerns) and structural (economic insecurity) level factors.
Methods
Study setting and population
We utilized baseline survey data from a national cohort of WLWH (n = 1424) enrolled in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS) from 2013 to 2015 across three provinces (Ontario, Quebec, British Columbia). Methods are detailed elsewhere (Loutfy et al., Citation2017). Trained peer research associates (PRAs) used purposive sampling methods to recruit WLWH, including word-of-mouth, venue-based sampling from AIDS service agencies, and online listservs. Participants completed a web-based, PRA-administered survey at a location with privacy, including either at an AIDS service agency, clinic, or a participant’s home or to a lesser extent, it could have been administered by phone or Skype. All participants provided informed consent (written or oral) and received a $50 CAD participation honorarium. Research ethics board approval was obtained from: Women’s College Hospital, Simon Fraser University, University of British Columbia/Providence Health, and McGill University Health Centre. Study sites that had independent Research Ethics Boards received their own approval prior to commencing enrolment.
Data collection
Health-related quality of life (HR-QoL) was measured using the Short Form Survey (SF-12), an scale with widely established reliability and validity (Hayes, Bhandari, Kathe, & Payakachat, Citation2017; Larson, Citation2002; Ware, Kosinski, & Keller, Citation1996). Two subscales were derived from eight subdomains: mental health (vitality, social functioning, mental health and role functioning: emotional) (score range: −1.67–77.22; Cronbach ) and physical health (physical functioning, role functioning: physical, bodily pain and general health perceptions) (score range: 1.31–74.67; Cronbach
). Higher scores indicate better mental or physical HR-QoL.
Resilience, conceptualized as processes that foster the development of personal competence and self-acceptance, was assessed using the Resiliency Scale (RS-10) (score range: 18–70; Cronbach ), with higher scores indicating increased resilience (Wagnild & Young, Citation1993). This tool has established validity and reliabilty among diverse populations (Wagnild, Citation2009).
Social support and women-centred HIV care were examined as predictors of resilience. Social support was assessed by the Medical Outcomes Study Social Support Survey (MOS-SSS) (score range: 4–20, Cronbach ), a tool with established reliability and validity (Gjesfjeld, Greeno, & Kim, Citation2007; Holden, Lee, Hockey, Ware, & Dobson, Citation2014; Stewart, Citation1992). Higher scores indicate higher positive social support. Women-centred HIV care (WCHC) was measured with a six-item tool developed from an evidence-based definition of WCHC (Carter et al., Citation2013). The WCHC tool used a Likert scale from strongly disagree to strongly agree (e.g., “I think that the care I have received from my HIV doctor has been women-centred; overall, women-centred care is important to me”) (score range:6–30, Cronbach
); the tool’s reliability and validity were established in research with WLWH in Canada (Carter et al., Citation2013, Citation2017).
Potential mediators include economic insecurity and HIV disclosure concerns. Economic insecurity was measured based on an indicator that included housing insecurity and food insecurity. Housing insecurity included living in: a self-contained room, transition house, halfway house, safe house, couch surfing, outdoors on street, parks, or in a car. Stable housing was coded as including participants who lived in an apartment (own/rent) or a house (own/rent). Food insecurity was derived from three statements focused on experiences in the past 12 months: fears of running out of food; experiences with running out of food; and inability to eat balanced meals (score range: 0–6; scores of 0–1 were coded as secure and 2–6 were coded as insecure). Participants who reported never experiencing any housing insecurity or food insecurity were coded as 1 (no economic insecurity); those who reported only food insecurity but no housing insecurity were coded as 2; those who reported only housing insecurity but no food insecurity were coded as 3; and those who reported having experienced both food insecurity and housing insecurity were coded as 4. This coding of economic insecurity as a continuous variable reflects a multi-dimensional approach to poverty that examines multiple poverty indicators (food insecurity, housing insecurity) to understand the intensity of poverty (Alkire, Conconi, & Seth, Citation2014). HIV disclosure concerns were measured based on a subscale of the HIV/AIDS quality of life (HAT-QOL) scale, which contains 6 questions regarding disclosure practices among PLWH (score range: 0–24, Cronbach ), with higher score indicating more worries or fewer disclosure practices.
We examined several socio-demographic factors as covariates, including age (continuous), legal relationship status (single vs. married/common law), immigration status (Canadian citizen, landed immigrant/permanent resident, refugee, other), ethnicity (Indigenous, Black, white/Caucasian and other), education (less than high school vs. high school or higher) and years of HIV diagnosis (continuous).
Statistical analysis
We first conducted descriptive analyses of all variables for the whole sample. Unadjusted and adjusted linear regressions were used to estimate the regression coefficients of mental and physical HR-QoL, and to determine the predictors of resilience. Structural equation modelling was conducted using maximum likelihood estimation methods to test (a) the direct effects of social support and WCHC on resilience, and (b) the direct effects of resilience on mental and physical HR-QoL, and the indirect effects via economic insecurity and HIV disclosure concerns, adjusting for socio-demographic factors. Model fit was assessed using: Chi-square, Root Mean Square Error of Approximation (RMSEA) and Comparative Fit Index (CFI). A non-significance level for Chi-square of >0.05, a score of <0.05 for RMSEA with 90% confidence interval between 0.02 and 0.08, and a score greater than 0.90 for CFI indicate acceptable model fit (Mueller & Hancock, Citation2008).
Results
reports sociodemographic characteristics for the whole sample (n = 1422). The median age for the sample was 42.5 years old (IQR = 35–50). The majority of the sample (81.37%) were Canadian citizens. Approximately two-thirds (65.34%) had an annual household income less than CAD $20,000. Most participants reported currently taking antiretroviral therapy (ART) (82.63%) and having an undetectable HIV viral load (84.32%).
Table 1. Socio-demographic characteristics of women living with HIV in Canada (n = 1422) (2013–2015).
illustrates the linear regression coefficients for mental HR-QoL and physical HR-QoL among WLWH included in the analysis. Social support and WCHC scores were positively and significantly associated with resilience. Resilience was significantly and positively associated with mental HR-QoL, physical HR-QoL, and significantly and negatively associated with HIV disclosure concerns and economic insecurity. All analyses were adjusted for age, relationship status, ethnicity, immigration status, education level and years since HIV diagnosis.
Table 2. Final path model parameter estimates of resilience and health-related quality of life (mental health and physical health) among women living with HIV in Canada (2013–2015). (n = 1294)*.
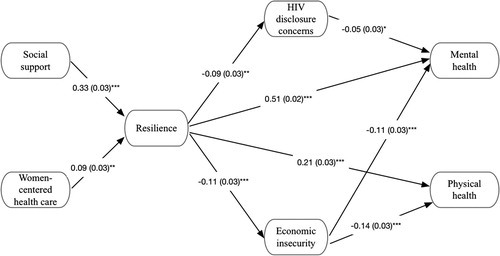
A structural equation model was tested to examine the direct and indirect effects of social support and WCHC on resilience, and resilience on mental HR-QoL and physical HR-QoL. illustrates the model with standard coefficients and the significance level of each pathway in our model. Standard coefficients indicate that with a standard deviation increase in the independent variable, the dependent variable would increase by x standard deviation, holding all other variables constant (Long & Freese, Citation2006). Results displayed in illustrates that the direct paths from social support (ß = 0.33, p < 0.001) and WCHC (ß = 0.09, p < 0.001) to resilience were significant. The direct path from resilience (ß = 0.51, p < 0.001) to mental HR-QoL was significant, accounting for the mediation effects of economic insecurity and social support. The direct path from resilience (ß = 0.21, p < 0.001 for direct effect) to physical HR-QoL was also significant, accounting for the mediation effects of economic insecurity. Economic insecurity partially mediated the relationship between resilience and both mental HR-QoL and physical HR-QoL. HIV disclosure concerns partially mediated the relationship between resilience and mental-HR-QoL. Model fit indices suggested that our model fit the data well (χ2[14] = 160.378, P < 0.001; CFI = 0.987; RMSEA = 0.048 [90% CI:0.042–0.080]; SRMR = 0.036).
Figure 1. Final path analysis results for resilience and health-related quality of life among women living with HIV in Canada (2013–2015) (n = 1294).
Discussion
Study findings demonstrate the importance of exploring multi-level factors associated with increased resilience among WLWH, as well as understanding pathways from resilience to HR-QoL. Social support and receiving WCHC predicted higher resilience, offering insight into opportunities for interventions with WLWH at community levels to foster social support. Strategies can also operate at institutional levels to integrate WCHC services into policy and practice; this will require buy-in from healthcare providers and institutions, funding to conduct training and evaluation of WCHC benefits and challenges, and the prioritization of WCHC by governments to scale-up WCHC nationally. While prior research has reported social support as a variable important to fostering resilience (e.g., Bhat et al., Citation2015; Earnshaw et al., Citation2015), to our knowledge this study is unique in contributing to the resilience literature regarding the importance of a gender-based approach to tailoring health services for WLWH.
Corroborating prior research (Farber et al., Citation2000; Fumaz et al., Citation2015; McGowan et al., Citation2018), we found that resilience was associated with improved physical and mental HR-QoL among WLWH. We found that economic insecurity did play a role in this relationship, whereby lower resilience was associated with increased economic insecurity, which in turn was associated with lower levels of mental and physical HR-QoL. Prior research with WLWH has highlighted associations between indicators of economic security and poorer wellbeing. For example, studies have reported associations between depression and: housing insecurity (Logie, Jenkinson, Earnshaw, Tharao, & Loutfy, Citation2016), food insecurity (Weiser et al., Citation2011) and low socio-economic status (Degroote et al., Citation2014). Yet economic insecurity only partially mediated the association between resilience and HR-QoL, underscoring the significant health-promoting role of resilience even in contexts of constrained economic resources.
HIV disclosure concerns reflect worry and fear of negative reactions and discrimination if one’s HIV positive serostatus is disclosed, and as such is an indicator of HIV-related stigma (Andrinopoulos et al., Citation2011; Grodensky et al., Citation2015; Turan et al., Citation2017). We found that HIV disclosure concerns partially mediated the association between resilience and mental HR-QoL. This finding aligns with prior research with PLWH that revealed associations between fears and concerns regarding disclosure of HIV status and poorer wellbeing and quality of life (Fekete et al., Citation2016) and mental health challenges (Hernansaiz-Garrido & Alonso-Tapia, Citation2017). To our knowledge the present study is unique in examining associations between resilience, HIV disclosure concerns, and HR-QoL. Our findings suggest there is an inverse relationship between resilience and HIV disclosure concerns, and that HIV disclosure concerns only partially mediate the association between resilience and mental HR-QoL. The role that resilience can play in reducing HIV disclosure concerns, and promoting HR-QoL, warrants further attention.
This study has limitations. The cross-sectional design precludes examining causation, and longitudinal studies could further explore trajectories of resilience and associated health outcomes. The purposive, non-random sample may have been biased to include women already accessing HIV care and therefore experiencing higher resilience. Conversely, we oversampled women experiencing multiple forms of marginalization, including women who use drugs, engage in sex work, young women and transgender women, and thus may have included women with less access to resources to foster resilience. The resilience measure we used, itself, was not multi-level; it simply measured personal competence and self-acceptance. To gain an understanding of pathways to, and from, different dimensions of resilience researchers could use comprehensive scales that assess not only individual aspects of resilience, but also community and contextual aspects of resilience. For instance, Liebenberg, Ungar, and Vijver’s (Citation2012) “Child and Youth Resilience Measure-28” includes three sub-scales to assess individual capacities and resources (e.g., skills, peer support), familial relationships (e.g., with primary caregiver), and contextual factors that engender feelings of belonging (e.g., spirituality, education, culture). Future studies could disentangle dimensions of resilience and their association with social ecological factors.
Conclusions
Our findings extend prior work on resilience among WLHW and have actionable implications to improve health and wellbeing among WLWH. We highlight the importance of both community factors, such as social support, and structural factors, such as WCHC (Carter et al., Citation2013; Loutfy et al., Citation2017; O’Brien et al., Citation2017), as dimensions that can be supported and integrated into policy and programme delivery to foster resilience among WLWH. There is a strong evidence base that peer support is good for WLWH in many ways (Cederbaum, Rice, Craddock, Pimentel, & Beaver, Citation2017; O’Brien et al., Citation2017; Paudel & Baral, Citation2015) and our path analyses suggests that it may be beneficial in increasing resilience, which in turn improves physical and mental HR-QoL. Our findings demonstrate that resilience is a protective factor with benefits to both physical and mental HR-QoL – yet this individual capacity of resilience interacts with social (HIV-related stigma) and structural (poverty) factors that compromise HR-QoL. Building the capacity for resilience among WLWH, while critically important and beneficial for wellbeing, must be conducted in tandem with strategies to reduce HIV-related stigma and address the root causes of economic insecurity, for WLWH to realize optimal health and opportunity.
Acknowledgements
The Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS) Research Team would like to especially thank all of the women living with HIV who participate in the research and entrust CHIWOS with their experiences of HIV treatment, care, and support. We also thank the entire national team of Co-Investigators, Collaborators, and Peer Research Associates. We would like to acknowledge the three provincial Community Advisory Boards, and the national CHIWOS Indigenous Advisory Board, CHIWOS African, Caribbean and Black Advisory Board, and our partnering organizations for supporting the study. We also acknowledge the BC Centre for Excellence in HIV for in-kind data management and analytic support.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
Data are available from the Women’s College Research Institute Women and HIV Research Programme Data Access Coordinator for researchers and students who meet the criteria for access to confidential data. The current Data Access Coordinator is Angela Underhill and she can be reached at [email protected]. The criteria for access to the confidential data includes 1) being added as a CHIWOS researcher or student to the research ethics board (REB) application and 2) signing a CHIWOS Data Sharing and Collaboration Agreement. The de-identified data set cannot be publicly shared at this point as we do not have community or REB approval to do so. Co-authorship is a requirement for data access as per the CHIWOS authorship policy (www.chiwos.ca) which includes the requirement that the ICMJE authorship criteria be met by all authors.
Additional information
Funding
References
- Alkire, S., Conconi, A., & Seth, S. (2014). Multidimensional poverty index 2014: Brief methodological note and results. Oxford, England: Oxford Poverty and Human Development Initiative.
- Andrinopoulos, K., Clum, G., Murphy, D. A., Harper, G., Perez, L., Xu, J., … Adolescent Medicine Trials Network for HIV/AIDS Interventions. (2011). Health related quality of life and psychosocial correlates among HIV-infected adolescent and young adult women in the US. AIDS Education and Prevention, 23(4), 367–381.
- Betancourt, T. S., Meyers-Ohki, S. E., Charrow, A., & Hansen, N. (2013). Annual research review: Mental health and resilience in HIV/AIDS-affected children - a review of the literature and recommendations for future research. Journal of Child Psychology and Psychiatry, 54(4), 423–444.
- Bhat, U., Cherian, A. V., Bhat, A., Chapman, H. J., Lukose, A., Patwardhan, N., … Ramakrishna, J. (2015). Factors affecting psychosocial well-being and quality of life among women living with HIV/AIDS. Nitte University Journal of Health Science, 5(4), 66.
- Blalock, A. C., Mcdaniel, J. S., & Farber, E. W. (2002). Effect of employment on quality of life and psychological functioning in patients with HIV/AIDS. Psychosomatics, 43(5), 400–404.
- Carter, A., Bourgeois, S., O’Brien, N., Abelsohn, K., Tharao, W., Greene, S., … Loutfy, M. R. (2013). Women-specific HIV/AIDS services: Identifying and defining the components of holistic service delivery for women living with HIV/AIDS. Journal of the International AIDS Society, 16, 17433. doi: 10.7448/IAS.16.1.17433
- Carter, A., Loutfy, M., de Pokomandy, A., Colley, G., Zhang, W., Sereda, P., … Kaida, A. (2017). Health-related quality-of-life and receipt of women-centered HIV care among women living with HIV in Canada. Women & Health, 163, 1–21.
- Cederbaum, J. A., Rice, E., Craddock, J., Pimentel, V., & Beaver, P. (2017). Social networks of HIV-positive women and their association with social support and depression symptoms. Women & Health, 57(2), 268–282.
- Dageid, W., & Grønlie, A. A. (2015). Measuring resilience and its association to social capital among HIV-positive South Africans living in a context of adversity. Journal of Community Psychology, 43(7), 832–848.
- Dale, S., Cohen, M., Weber, K., Cruise, R., Kelso, G., & Brody, L. (2014). Abuse and resilience in relation to HAART medication adherence and HIV viral load among women with HIV in the United States. AIDS Patient Care and STDs, 28(3), 136–143.
- Degroote, S., Vogelaers, D., & Vandijck, D. M. (2014). What determines health-related quality of life among people living with HIV: An updated review of the literature. Archives of Public Health, 72(1), 40.
- Douab, T., Marcellin, F., Vilotitch, A., Protopopescu, C., Préau, M., Suzan-Monti, M., … Spire, B. (2014). Health-related quality of life of people living with HIV followed up in hospitals in France: Comparing trends and correlates between 2003 and 2011 (ANRS-VESPA and VESPA2 national surveys). AIDS Care, 26(sup1), S29–S40.
- Earnshaw, V. A., Lang, S. M., Lippitt, M., Jin, H., & Chaudoir, S. R. (2015). HIV stigma and physical health symptoms: Do social support, adaptive coping, and/or identity centrality act as resilience resources? AIDS and Behavior, 19(1), 41–49.
- Farber, E. W., Schwartz, J. A., Schaper, P. E., Moonen, D. J., & McDaniel, J. S. (2000). Resilience factors associated with adaptation to HIV disease. Psychosomatics, 41(2), 140–146.
- Fekete, E. M., Williams, S. L., Skinta, M. D., & Bogusch, L. M. (2016). Gender differences in disclosure concerns and HIV-related quality of life. AIDS Care, 28(4), 450–454.
- Fumaz, C. R., Ayestaran, A., Perez-Alvarez, N., Muñoz-Moreno, J. A., Moltó, J., Ferrer, M. J., & Clotet, B. (2015). Resilience, ageing, and quality of life in long-term diagnosed HIV-infected patients. AIDS Care, 27(11), 1396–1403.
- Furlotte, C., & Schwartz, K. (2017). Mental health experiences of older adults living with HIV: Uncertainty, stigma, and approaches to resilience. Canadian Journal on Aging/La Revue canadienne du vieillissement, 36(2), 125–140.
- Garcia-Dia, M. J., DiNapoli, J. M., Garcia-Ona, L., Jakubowski, R., & O’Flaherty, D. (2013). Concept analysis: Resilience. Archives of Psychiatric Nursing, 27(6), 264–270.
- Gjesfjeld, C. D., Greeno, C. G., & Kim, K. H. (2007). A confirmatory factor analysis of an abbreviated social support instrument-The MOSS-SSS. Research on Social Work Practice, 18, 231–237.
- Grodensky, C. A., Golin, C. E., Jones, C., Mamo, M., Dennis, A. C., Abernethy, M. G., & Patterson, K. B. (2015). “I should know better”: The roles of relationships, spirituality, disclosure, stigma, and shame for older women living with HIV seeking support in the south. Journal of the Association of Nurses in AIDS Care, 26(1), 12–23.
- Hayes, C. J., Bhandari, N. R., Kathe, N., & Payakachat, N. (2017). Reliability and validity of the medical outcomes study short form-12 version 2 (SF-12v2) in adults with non-cancer pain. Healthcare, 5(2), e22. doi: 10.3390/healthcare5020022
- Hernansaiz-Garrido, H., & Alonso-Tapia, J. (2017). Internalized HIV stigma and disclosure concerns: Development and validation of two scales in Spanish-speaking populations. AIDS and Behavior, 21, 93–105.
- Holden, L., Lee, C., Hockey, R., Ware, R. S., & Dobson, A. J. (2014). Validation of the MOS social support survey 6-item (MOS-SSS-6) measure with two large population-based samples of Australian women. Quality of Life Research, 23(10), 2849–2853.
- Kalichman, S. C., DiMarco, M., Austin, J., Luke, W., & DiFonzo, K. (2003). Stress, social support, and HIV-status disclosure to family and friends among HIV-positive men and women. Journal of Behavioral Medicine, 26(4), 315–332.
- Kumar, S., Gruskin, S., Khosla, R., & Narasimhan, M. (2015). Human rights and the sexual and reproductive health of women living with HIV–a literature review. Journal of the International AIDS Society, 18(6S5), 20290.
- Larson, C. O. (2002). Use of the SF-12 instrument for measuring the health of homeless persons. Health Services Research, 37(3), 733–750.
- Li, X., Chi, P., Sherr, L., Cluver, L., & Stanton, B. (2015). Psychological resilience among children affected by parental HIV/AIDS: A conceptual framework. Health Psychology and Behavioral Medicine, 3(1), 217–235.
- Liebenberg, L., Ungar, M., & Vijver, F. V. D. (2012). Validation of the child and youth resilience measure-28 (CYRM-28) among Canadian youth. Research on Social Work Practice, 22(2), 219–226.
- Logie, C. H., Ahmed, U., Tharao, W., & Loutfy, M. R. (2017). A structural equation model of factors contributing to quality of life among African and Caribbean women living with HIV in Ontario, Canada. AIDS Research and Human Retroviruses, 33(3), 290–297.
- Logie, C. H., Jenkinson, J. I., Earnshaw, V., Tharao, W., & Loutfy, M. R. (2016). A structural equation model of HIV-related stigma, racial discrimination, housing insecurity and wellbeing among African and Caribbean black women living with HIV in Ontario, Canada. PloS one, 11(9), e0162826.
- Long, J. S., & Freese, J. (2006). Regression models for categorical dependent variables using stata. College Station, Texas, U.S.: Stata Press.
- Loutfy, M., de Pokomandy, A., Kennedy, V. L., Carter, A., O’Brien, N., Proulx-Boucher, K., … Greene, S. (2017). Cohort profile: The Canadian HIV women’s sexual and reproductive health cohort study (CHIWOS). PloS one, 12(9), e0184708.
- Loutfy, M., Tharao, W., Logie, C., Aden, M. A., Chambers, L. A., Wu, W., … Calzavara, L. (2015). Systematic review of stigma reducing interventions for African/black diasporic women. Journal of the International AIDS Society, 18(1), 19835.
- McGowan, J. A., Brown, J., Lampe, F. C., Lipman, M., Smith, C., & Rodger, A. (2018). Resilience and physical and mental well-being in adults with and without HIV. AIDS and Behavior, 22(5), 1688–1698.
- Medeiros, P. (2017). HIV and the health of women in New Brunswick. Journal of New Brunswick Studies/Revue d’études sur le Nouveau-Brunswick, 8, 175–192.
- Mo, P. K. H., Lau, J. T. F., Yu, X., & Gu, J. (2014). The role of social support on resilience, posttraumatic growth, hopelessness, and depression among children of HIV-infected parents in mainland China. Aids Care, 26(12), 1526–1533.
- Mueller, R. O., & Hancock, G. R. (2008). Best practices in structural equation modeling. In Best practices in quantitative methods (pp. 488–508). Thousand Oaks, CA, USA: Sage Publications .
- Normén, L., Chan, K., Braitstein, P., Anema, A., Bondy, G., Montaner, J. S., & Hogg, R. S. (2005). Food insecurity and hunger are prevalent among HIV-positive individuals in British Columbia, Canada. The Journal of Nutrition, 135(4), 820–825.
- O’Brien, N., Greene, S., Carter, A., Lewis, J., Nicholson, V., Kwaramba, G., … Loutfy, M. (2017). Envisioning women-centered HIV care: Perspectives from women living with HIV in Canada. Women’s Health Issues, 27(6), 721–730.
- Paudel, V., & Baral, K. P. (2015). Women living with HIV/AIDS (WLHA), battling stigma, discrimination and denial and the role of support groups as a coping strategy: A review of literature. Reproductive Health, 12(1), 53.
- Riley, E. D., Moore, K., Sorensen, J. L., Tulsky, J. P., Bangsberg, D. R., & Neilands, T. B. (2011). Basic subsistence needs and overall health among human immunodeficiency virus-infected homeless and unstably housed women. American Journal of Epidemiology, 174(5), 515–522.
- Riley, E. D., Neilands, T. B., Moore, K., Cohen, J., Bangsberg, D. R., & Havlir, D. (2012). Social, structural and behavioral determinants of overall health status in a cohort of homeless and unstably housed HIV-infected men. PLoS One, 7(4), e35207.
- Simoni, J. M., Huang, B., Goodry, E. J., & Montoya, H. D. (2006). Social support and depressive symptomatology among HIV-positive women: The mediating role of self-esteem and mastery. Women & Health, 42(4), 1–15.
- Smith, C., Cook, R., & Rohleder, P. (2017). Taking into account the quality of the relationship in HIV disclosure. AIDS and Behavior, 21(1), 106–117.
- Stewart, A. L. (1992). Measuring functioning and well-being: The medical outcomes study approach. Durham, North Carolina, US: Duke University Press.
- Stokols, D. (1996). Translating social ecological theory into guidelines for community health promotion. American Journal of Health Promotion, 10(4), 282–298.
- Turan, B., Hatcher, A. M., Weiser, S. D., Johnson, M. O., Rice, W. S., & Turan, J. M. (2017). Framing mechanisms linking HIV-related stigma, adherence to treatment, and health outcomes. American Journal of Public Health, 107(6), 863–869.
- Ungar, M. (2011). The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. American Journal of Orthopsychiatry, 81(1), 1–17.
- Wagnild, G. (2009). A review of the resilience scale. Journal of Nursing Measurement, 17(2), 105–113.
- Wagnild, G., & Young, H. (1993). Development and psychometric. Journal of Nursing Measurement, 1(2), 165–178.
- WareJr, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233.
- Weiser, S. D., Young, S. L., Cohen, C. R., Kushel, M. B., Tsai, A. C., Tien, P. C., … Bangsberg, D. R. (2011). Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS–. The American Journal of Clinical Nutrition, 94(6), 1729S–1739S.
