
ABSTRACT
Services that aim to prevent mother-to-child HIV transmission (PMTCT) can simultaneously reduce the overall impact of HIV infection in a population while also improving maternal and child health outcomes. By taking a health equity perspective, this retrospective case control study aimed to compare the health status of under-5 children born to HIV-positive and HIV-negative mothers in Tigray Region, Ethiopia. Two hundred and thirteen HIV-positive women (cases), and 214 HIV-negative women (controls) participated through interviews regarding their oldest children. Of the children born to HIV-positive mothers, 24% had not been tested, and 17% of those who had been tested were HIV-positive themselves. Only 29% of the HIV-positive children were linked to an ART programme. Unexpectedly, exposed HIV-negative children had fewer reports of perceived poor health as compared to unexposed children. Over 90% of all the children, regardless of maternal HIV status, were breastfed and up-to-date with the recommended immunizations. The high rate of HIV infection among the babies of HIV-positive women along with their low rates of antiretroviral treatment raises serious concerns about the quality of outreach to pregnant women in Tigray Region, and of the follow-up for children who have been exposed to HIV via their mothers.
Introduction
A range of factors influences children’s health, not least of which is their parents’ own health status (CSDH, Citation2008). Maternal HIV-positive status is a particularly significant driver of child health inequities for both biological and social reasons. Biologically, children born to HIV-positive mothers have a 15% to 45% risk of acquiring HIV in the absence of treatment (WHO, Citation2018), and this can expose the child to numerous adverse health outcomes, including premature mortality (WHO, Citation2010). Socially, children born to HIV-positive mothers face a higher risk of death, as well as poorer access to education and health services, due to the death of one or both parents (Guo, Li, & Sherr, Citation2012), or inadequate nutrition (Mkwanazi, Rochat, & Bland, Citation2015).
Since an HIV diagnosis during pregnancy should lead to a woman being put on treatment, PMTCT programmes improve child health both biologically – through reducing mother-to-child transmission of HIV to below 5% – and socially, through improving maternal health. In Ethiopia, the prevention of mother-to-child transmission (PMTCT) programme was initiated in 2001. Current PMTCT guidelines (Ethiopian Federal Ministry of Health, Citation2014) follow the WHO recommendation (World Health Organization, Citation2010), whereby all pregnant and breastfeeding women receive antiretroviral therapy (ART) immediately after diagnosis, irrespective of the clinical stage of disease or CD4 count. This facilitates both a reduction in HIV-related morbidity and mortality for the woman herself, and also a reduction in the risk of her passing HIV to her baby. All infants who are born to HIV-infected mothers (i.e., HIV-exposed infants) receive antiretroviral (ARV) prophylaxis, which includes Nevirapine once daily for six weeks, after which they are tested – at six weeks of age or at the earliest opportunity thereafter – using polymerase chain reaction (PCR). Infants with a positive virological test result start ART immediately, following which they have a monthly follow up for the first six months of life, and then every three months. A confirmatory HIV test is administered at 18 months.
In 2005, there were nine PMTCT and four comprehensive ART-providing health facilities in Tigray Region in northern Ethiopia, and this had expanded to 142 PMTCT and 77 ART service-providing health facilities by 2016. This represents a coverage rate of 67% and 34% respectively in the Region. In 2009 Tigray Regional Laboratory started to provide Early Infant Diagnosis through polymerase chain reaction (PCR) HIV testing service for the region (Ethiopia Public Health Institute, Citation2017).
Substantial reductions in HIV prevalence in adult and pregnant women have been achieved since the peak in 2001. The current adult HIV prevalence in Ethiopia is considered low, 1.5% at national level, but there are also substantial variations in the rates of mother-to-child HIV transmission in different parts of Ethiopia, ranging from 15% in Dire-Dawa (Wudineh & Damtew, Citation2016) to 8.2% in Addis Ababa (Mirkuzie, Sisay, Hinderaker, Moland, & Mørkve, Citation2012; Negash & Ehlers, Citation2016). In Tigray Region, the HIV prevalence rate is 1.8%, though with wide differences by residence (4.2% in urban to 0.6% in rural) and sex (1.9% in women and 1% in men) (EDHS, Citation2016). These are caused by, among other issues, differential access to health care, and low ante-natal care (ANC) and skilled delivery coverage (Barnabas, Pegurri, Selassie, Naamara, & Zemariam, Citation2014; United Nations, Citation2015).
In spite of these low overall rates, however, there were still an estimated 33,200 pregnant women and more than 200,000 children under the age of 15 living with HIV in Ethiopia in 2013 (Federal Ministry of Health Ethiopia, Citation2014). These figures reflect the situation in a number of other African countries (Landes et al., Citation2012; Ndirangu, Newell, Tanser, Herbst, & Bland, Citation2010), where mother-to-child transmission of HIV continues to take place in spite of the availability of PMTCT services.
The post-2015 Sustainable Development Goals (SDG) agenda emphasizes equity as a cross-cutting theme for health and other development-related spheres. Child health is specifically identified in SDG 3, with targets on neonatal and under-5 mortality that, if achieved, would bring about equitably low rates of mortality among children globally (UN DSD, Citation2017). Ethiopia has identified child health inequity as an issue of concern, and has put in place strategies to address the problem in its current 2015–2020 health sector transformation plan (Mullan, Citation2016).
In order to understand the effect of policies to reduce child mortality, evaluations of services are needed in order to facilitate an informed decision-making process for health service provision based on local conditions. The aim of this paper, therefore, is to assess the health outcomes of children born to mothers (both HIV-positive and HIV-negative) enrolled in the PMTCT service in Tigray Region, Ethiopia, as a means of providing evidence for improving child health services and thereby promoting child health equity within the context of the Sustainable Development Goals.
Methods
Study design and setting
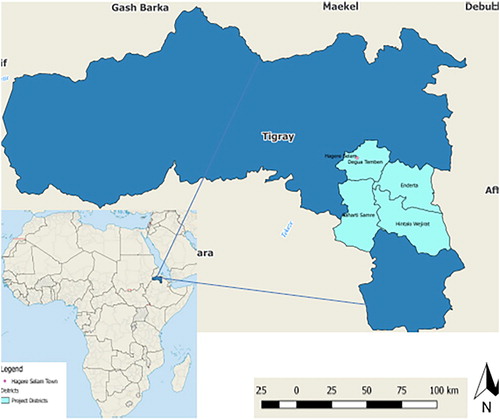
This retrospective case–control study was performed from July-August 2014 in the South-Eastern Zone of Tigray Region, North Ethiopia. The Zone comprises four administrative woredas (Districts) surrounding Mekelle, the capital of Tigray Region (), where an estimated 600,000 people live (). The people of the Zone live under broadly similar socio-economic and cultural conditions. More than 80% of the population are farmers with the remainder living in semi-urban small towns.
Figure 1. Map of Tigray Region, Ethiopia, study areas highlighted in light blue.
No woreda-specific HIV prevalence data exists in Tigray Region. However, it is known that more than half of the HIV-positive pregnant women in the Region do not receive PMTCT or enrol in ART due to low ANC and skilled delivery coverage, and also to poor linkages and adherence to ART.
There are 32 health centres, 4 primary hospitals and 72 health posts (the lowest level of health facility in the Ethiopian health system) within the South-Eastern Zone of Tigray. At health posts, preventive maternal and child services are provided, including treatment for selected diseases and HIV testing and counselling. Health centres and hospitals provide skilled delivery and PMTCT services integrated within antenatal care (ANC). In the health centres, all women are offered free HIV testing and counselling during ANC and delivery, and referral to the nearest hospitals for initiation of ART services if the infection is confirmed. Health centres provide ARV prophylaxis during ANC and delivery, as well as follow-up for mothers and exposed infants, including through the collecting and transporting of dried blood samples from HIV-exposed infants for testing at the Regional laboratory up until the age of 18 months.
Sampling methods
The South-Eastern Zone was randomly selected from among the seven Zones in Tigray Region, and all HIV-positive women who received PMTCT and enrolled in ART care in the past five years in the four woredas in the Zone were included in the study.
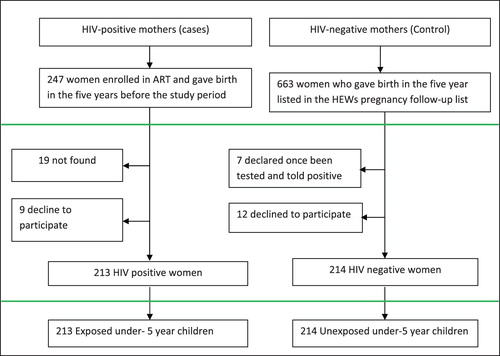
We used the ART registry in the four primary hospitals to identify HIV-positive women, the year of pregnancy, and details of their residence at kebele or village level. Simultaneously, we used the follow-up register for pregnant women at the health posts to identify HIV-negative from the same kebele and the same year of pregnancy. By combining these two datasets, it was possible to identify under-5 year children born to HIV-positive women – who would be taken as the cases – and under-5 year children born to women who had not been diagnosed with HIV, who would be taken as the control group ().
Figure 2. Sampling frame of study participants.
Data collectors contacted each of the HIV-positive mothers in order to identify all the children who had been born during the five years prior to the study (whether alive or dead at the time of interview). For the control group, households were randomly selected from the list of mothers whose most recent HIV test had been negative, ensuring a proportion of 1:1 for cases and controls. Under-5-year-old children of these mothers who had been born during the five years prior to the study (whether alive or dead) were then identified. In cases where more than one under-5 child had been born during that period, only the oldest identified child was included in the analysis.
A structured questionnaire was prepared by the first author (AA) that included items on maternal health, socio-demographic status, economic and reproductive history, child mortality and morbidity, and utilization of child health services. The questionnaire was prepared in English, translated to the local language, Tigrinya, pre-tested in a non-study area, and revised accordingly.
In each woreda, five contracted employees of the ART sites – “HIV case managers”, who are trained to ensure ART adherence and who have the contact addresses of patients for follow-up – collected the data under the supervision of an ART nurse. Data collectors and supervisors received three-day training on data collection, confidentiality, ethics, and supervision skills. Data collectors used the information collected from the ART registry to approach women at their home, and to trace the addresses of women who had changed their place of residence. In the event that the mother was deceased, the child’s caregiver was interviewed.
Data were submitted daily to supervisors and checked for completeness and quality using a checklist. Additionally, the first author and one skilled coordinator re-checked a randomly selected 10% sample of the dataset that had been approved by the supervisors on a weekly basis. Incomplete, unreliable or inappropriate data identified during checking, rechecking and during data entry were returned for clarification and/or additional information as required.
Data analysis
Data were summarized and analysed using PASW Statistics version 21.0 (SPSS Inc., Chicago, IL). Chi-square tests and Fishers exact test were used to compare the health status and other relevant variables of under-5 children born to HIV-positive and HIV-negative mothers. Bivariate and multivariate logistic regressions analyses were performed for variables with statistically significant association (p-value < .05).
Ethical considerations
The study received ethical approval from Mekelle University College of Medical Sciences and the Regional Research Review Committee of Tigray Regional Health Bureau. To protect the confidentiality of participants, data collectors were specifically selected as health professionals who are already aware of the HIV status of the study subjects, and who had already been trained to keep all such information confidential. The data collection process used verbal informed consent and respected the right of the study subjects to decline from participating.
Results
Characteristics of respondents and children
A total of 247 HIV-positive women (cases) who received PMTCT and who were currently enrolled in ART care were identified from the register. During the actual data collection, 19 (7.7%) women were not found and 9 (3.9%) declined to participate; the remainder (213/247) participated to give an overall response rate of 86.2%. Among the selected 247 HIV-negative women (controls), 12 (4.9%) declined to participate and 7 (2.8%) had, since their initial HIV-negative test, been diagnosed with HIV. These were substituted with the next, randomly assigned woman on the list. The remaining (228/247) were willing to participate, giving an overall response rate of 93%.
A total of 213 HIV-positive and 214 HIV-negative mothers participated in the study (Table1), through whom we received details of the health outcomes of 427 children (213 born to HIV-positive mothers, defined below as “exposed”; and 214 born to women without an HIV diagnosis, defined below as “unexposed”). Twenty-five mothers had more than one surviving under-5-year-old child, but only the eldest child in these cases was included in the study.
Most of the socio-economic and reproductive characteristics of cases and controls and their children were comparable, but significant differences (P < .05) were found in respondents’ age, marital status, occupation, and the number of pregnancies. HIV-positive women tended to be older, more likely to be divorced or self-employed, and have higher parity ().
Table 1. Socio-demographic, economic and reproductive characteristics of respondents by HIV status.
Child HIV status
A total of 162 (76%) out of the 213 exposed children had themselves been tested for HIV, while the remaining 51 (24%) children, of whom 46 (90.2%) were older than four weeks (and therefore eligible for HIV testing) had unknown HIV status – this was either because they had not been tested (for any of a variety of reasons), or because the mothers or caregivers did not remember if they had been tested (). Of those who had been tested, 134 (83%) were found to be HIV-negative, and 28 (17%) were HIV-positive. Only 8 (29%) of the HIV-positive children were linked to an ART programme. Delivery at home or at a health post attended by unskilled or traditional attendants, as opposed to delivery at health centre and Hospital by skilled health workers, was a significant risk factor for increased risk of HIV infection of the new-born [adj OR 3.9 (95% CI 1.7–9.1, p-.002)].
Table 2. Characteristics under-5-year-old children by child indicators.
Mortality
A total of 32 (7.5%) of the 427 babies born were reported to have died, 24 of whom had been exposed to HIV, and 8 of whom had been unexposed (). There was no significant difference in sex and age at death; however, more than 93% of the mortality occurred before 2 years of age, and 78% before the first birthday. On univariate analysis, maternal HIV-positive status, not receiving uptake of antenatal care during pregnancy, delivery at home or at health post, low maternal income status, and child’s HIV-positive status were all found to be significant risk factors for mortality (p < .01) ().
Table 3. Comparison of 24 exposed and 8 un-exposed deceased under-5-year-old children by maternal and child indicators.
However, when adjusted for maternal age, marital status, occupation, number of pregnancy, child HIV status and variables that were significant at the <.05 level in the univariate analysis, and when exposed children with unknown HIV status are removed, home or health post-delivery and HIV infection remained as significant predictors of child mortality. These contributed to six fold [adj OR 6.2 (95% CI 2.2–17.3, <.001)] and fivefold [adj OR 5.2 (95% CI 1.5–18.0, p-.009)] increases respectively ().
Table 4. Bivariate and multivariate analyses of risk factors for under-5-year-old child mortality.
Morbidity
On univariate analysis, occupation, antenatal care, place of birth and child HIV were significant risk factors (p < .03) for perceived child morbidity. When adjusted for maternal characteristics that showed asignificant difference (as in ), the following remained as significant factors for perceived poor health: HIV infection [adj OR 3.3 (95% CI 1.1–10.0, p = .03)], and delivery attended by unskilled attendants at home or at a health post [adj OR 2.9 (95% CI 1.4–6.0, p = .005).
Exposed but uninfected children are perceived to have better health status than unexposed children [adj OR 0.4 (95% CI 0.1–0.9, p = .04)]. Despite this, there was no significant difference between exposed and unexposed children with regard to those who experienced at least one episode of diarrhoea, fever or cough with fast breathing during the past two months ().
Table 5. Health status, episodes of morbidity and health service utilization surviving under-5-year-old children two months prior to the study.
Utilization of child health services
Utilization of child health services was comparable in both exposed and unexposed children. Over 92% of all HIV-exposed children and 90% of unexposed children were up-to-date with the recommended immunizations; more than 98% in both groups had been breastfed at least for some time (); and more than 60% of children in both groups (61.8% exposed and 61.2% unexposed) visited a health facility for treatment as necessary. No significant difference was found in the proportions of exposed and unexposed children making at least one visit to a health facility after adjusting for maternal variables ().
Discussion
Our study found that in spite of the well-established PMTCT programme that has been running in Tigray Region since 2001, 24% of exposed infants had unknown HIV status, which is broadly line with previous studies that have reported poor access to HIV testing and care for children in Ethiopia (Kebede, Gebeyehu, Jain, Sun, & Haubrich, Citation2014). Among those tested for HIV, 28 (17%) of the babies born to HIV-positive mothers – 11 (39.3%) of whose deliveries took place a health facility – were themselves HIV-infected. The rate of HIV in children is substantially higher than both the 5% rate achieved in South Africa (Goga et al., Citation2015 Grimwood, Fatti, Mothibi, Eley, & Jackson, Citation2012) and in other recent studies conducted in Ethiopia, where infection rates of 10% (Kassa, Citation2018) and 6% were found in Addis Ababa (Negash & Ehlers, Citation2016). Further, of these 28 children, only 8 (29%) had been linked to an ART programme. This means that more than 70% of the HIV-positive under-5-year-old children in our sample were at serious risk of disease and early death. This highlights the need for significantly improved awareness and integration of PMTCT within other home-based services.
The findings on mortality were broadly in line with expectations. Overall under-5 year child mortality in our study was consistent with the recent Ethiopian Demographic and Health Survey (DHS) (CSA, Citation2016), and mortality among children with HIV was much higher than it was among those who were not infected. Unlike many studies from the early days of national PMTCT programmes in Africa (Kuhn et al., Citation2005; Nakiyingi et al., Citation2003; Newell et al., Citation2004; Zaba et al., Citation2005) as well as from some more recent findings (Kurewa et al., Citation2010; Naniche et al., Citation2009), our findings indicate that exposure to maternal HIV alone is not a risk factor for under-5 year child mortality. However, delivery attended by an unskilled person at home or at a health post, and child HIV infection, are both significant risk factors. This is all in line with previous studies that have pointed to a higher risk of mortality among HIV-infected children (Violari et al., Citation2008), as well as research indicating that delivery in a well-equipped health institution is a predictor of improved maternal and child outcomes, regardless of maternal HIV status (Chinkhumba, De Allegri, Muula, & Robberstad, Citation2014; Moyer, Dako-Gyeke, & Adanu, Citation2013).
In spite of the high mortality rate among HIV-exposed children, it is important to note that many children, both HIV-infected and not, do survive; but in all cases, the health system needs to be responsive to the particular health and psychosocial needs of children raised in families affected by HIV. Good outcomes can be attained through provision of PMTCT services, supporting long term ART treatment for the mother, and counselling about child feeding (Lerebo, Callens, Jackson, Zarowsky, & Temmerman, Citation2014; Tura, Fantahun, & Worku, Citation2013; Wudineh & Damtew, Citation2016).
Elements of the findings relating to morbidity were also in line with expectations, with episodes of diarrhoea, fever and cough with fast breathing in our study being consistent with the latest Ethiopian DHS report (CSA, Citation2016). Further, HIV-infected children exhibited much higher levels of morbidity than the HIV-uninfected children, as expected. Viewing this through an equity lens raises questions about how the HIV-positive children could be better served by the health system, including, perhaps, through the provision of nutritional supplementation.
While previous reports indicate exposure to maternal HIV alone as a risk factor for childhood morbidity (Koyanagi et al., Citation2011; Marquez et al., Citation2014), our results showed that morbidity was significantly lower in exposed but uninfected children. This encouraging finding may be explained by the counselling that HIV-positive mothers receive during treatment follow-up and antenatal care, but it may also be a product of the co-trimoxazole prophylaxis that is provided for exposed children (Homsy et al., Citation2014; Kourtis et al., Citation2013).
The uptake of immunization services alongside good rates of breastfeeding were consistent with the findings of the Ethiopian DHS (CSA, Citation2016). Unlike one study from South Africa (Ndirangu, Bärnighausen, Tanser, Tint, & Newell, Citation2009), our study found no difference in access to child health care and services, breastfeeding, and uptake of immunization between exposed and unexposed children. These findings were to be expected given the free access to health care to all children born to HIV-positive women in the health system, the increasing acceptability of immunization, and the culture of breast feeding in Ethiopia, the latter of which is strongly supported by the Ethiopian PMTCT strategy. It could also be a result of the ongoing good health and survival of HIV-positive women enrolled in ART programmes, as this can facilitate sustaining the household income.
Limitations of the study
We acknowledge that since the data was based on self-report, some biases could have been included, either through recall bias or a reluctance of the respondents to share sensitive personal information. However, this issue should have been limited by the fact that the data collectors were trained and experienced HIV case managers, who fully understood and practised the principle of confidentiality.
Conclusion
In spite of the well-established PMTCT programme that has been running in Tigray Region since 2001, 17% of the babies born to HIV-positive mothers were themselves HIV-infected, and of these, only 29% were enrolled in an ART programme. These are poorer rates than expected, and they raise serious concerns about the quality of both outreach to pregnant women in Tigray Region, and of the follow-up of children who have been exposed to HIV via their mothers.
Viewing these findings through an equity lens provides the opportunity to ensure that the health system is more responsive to the needs of HIV-positive mothers and their children, whether infected themselves or not. Three broad areas of need have been identified: improvement in infant HIV testing; improvement in infant HIV treatment; and a reduction in infant HIV positivity rates. These issues can be addressed by enhancing the coverage of skilled delivery and PMTCT/ART services through decentralizing to health post level; integrating the follow-up of HIV-exposed children within community-level campaigns; and improving the capacity of health workers.
Data availability
Since this study involves HIV-positive individuals, the data cannot be placed in the public domain because of the risk of identity disclosure.
Acknowledgements
We thank the populations of the study woredas, the study participants, and the woreda health offices for providing permission, information and facilitation of the study. We also acknowledge the valuable input received from the reviewers.
Disclosure statement
At the time of this study, the first author (AA) was working as Deputy Head of the Tigray Regional Health Bureau.
ORCID
Atakelti Abraha http://orcid.org/0000-0002-8886-7199
Peter Byass http://orcid.org/0000-0001-5474-4361
John Kinsman http://orcid.org/0000-0003-1332-4138
Additional information
Funding
References
- Barnabas, G., Pegurri, E., Selassie, H. H., Naamara, W., & Zemariam, S. (2014). The HIV epidemic and prevention response in Tigrai, Ethiopia: A synthesis at sub-national level. BMC Public Health. doi: 10.1186/1471-2458-14-628
- Central Statistical Agency [Ethiopia] and ICF International. (2016). Demographic and health survey 2016 key indicators report.
- Chinkhumba, J., De Allegri, M., Muula, A. S., & Robberstad, B. (2014). Maternal and perinatal mortality by place of delivery in sub-Saharan Africa: A meta-analysis of population-based cohort studies. BMC Public Health, 14(1), 1014. doi: 10.1186/1471-2458-14-1014
- CSDH. (2008). Closing the gap in a generation. Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health, 246. doi: 10.1080/17441692.2010.514617
- EDHS. (2016). Ethiopia demographic and health survey 2016. Addis Ababa: Central Statistical Agency (CSA) [Ethiopia] and ICF.
- Ethiopia Public Health Institute. (2017). Ethiopia services availability and readiness assessment report. Addis Ababa.
- Federal Ministry of Health Ethiopia. (2014). Country progress report on the HIV. Addis Ababa, Ethiopia.
- Federal Ministry of Health Ethiopia. (2014). National guidelines for comprehensive HIV prevention, care and treatment. Addis Ababa.
- Goga, A. E., Dinh, T.-H., Jackson, D. J., Lombard, C., Delaney, K. P., Puren, A., … Pillay, Y. (2015). First population-level effectiveness evaluation of a national programme to prevent HIV transmission from mother to child, South Africa. Journal of Epidemiology and Community Health, 69(3), 240–248. doi: 10.1136/jech-2014-204535
- Grimwood, A., Fatti, G., Mothibi, E., Eley, B., & Jackson, D. (2012). Progress of preventing mother-to-child transmission of HIV at primary healthcare facilities and district hospitals in three South African provinces. South African Medical Journal=Suid-Afrikaanse Tydskrif Vir Geneeskunde, 102(2), 81–83.
- Guo, Y., Li, X., & Sherr, L. (2012). The impact of HIV/AIDS on children’s educational outcome: A critical review of global literature. AIDS Care – Psychological and Socio-Medical Aspects of AIDS/HIV, doi: 10.1080/09540121.2012.668170
- Homsy, J., Dorsey, G., Arinaitwe, E., Wanzira, H., Kakuru, A., Bigira, V., … Tappero, J. W. (2014). Protective efficacy of prolonged co-trimoxazole prophylaxis in HIV-exposed children up to age 4 years for the prevention of malaria in Uganda: A randomised controlled open-label trial. The Lancet Global Health, 2(12), e727–e736. doi: 10.1016/S2214-109X(14)70329-8
- Kassa, G. M. (2018). Mother-to-child transmission of HIV infection and its associated factors in Ethiopia: A systematic review and meta-analysis. BMC Infectious Diseases, doi: 10.1186/s12879-018-3126-5
- Kebede, B., Gebeyehu, A., Jain, S., Sun, S., & Haubrich, R. (2014). Delay in early infant diagnosis and high loss to follow-up among infant born to HIV-infected women in Ethiopia. World Journal of AIDS, doi: 10.4236/wja.2014.44048
- Kourtis, A. P., Wiener, J., Kayira, D., Chasela, C., Ellington, S. R., Hyde, L., … Jamieson, D. J. (2013). Health outcomes of HIV-exposed uninfected African infants. AIDS (London, England). doi: 10.1097/QAD.0b013e32835ca29f
- Koyanagi, A., Humphrey, J. H., Ntozini, R., Nathoo, K., Moulton, L. H., Iliff, P., … Grp, Z. S. (2011). Morbidity among human immunodeficiency virus-exposed but uninfected, human immunodeficiency virus-infected, and human immunodeficiency virus-unexposed infants in Zimbabwe before availability of highly active antiretroviral therapy. Pediatric Infectious Disease Journal, 30(1), 45–51. doi: 10.1097/INF.0b013e3181ecbf7e
- Kuhn, L., Kasonde, P., Sinkala, M., Kankasa, C., Semrau, K., Scott, N., … Thea, D. M. (2005). Does severity of HIV disease in HIV-infected mothers affect mortality and morbidity among their uninfected infants? Clinical Infectious Diseases, 41(11), 1654–1661. doi: 10.1086/498029
- Kurewa, E. N., Gumbo, F. Z., Munjoma, M. W., Mapingure, M. P., Chirenje, M. Z., Rusakaniko, S., & Stray-Pedersen, B. (2010). Effect of maternal HIV status on infant mortality: Evidence from a 9-month follow-up of mothers and their infants in Zimbabwe. Journal of Perinatology, 30(2), 88–92. doi: 10.1038/jp.2009.121
- Landes, M., van Lettow, M., Bedell, R., Mayuni, I., Chan, A. K., Tenthani, L., & Schouten, E. (2012). Mortality and health outcomes in HIV-infected and HIV-Uninfected mothers at 18–20 months postpartum in Zomba District, Malawi. PLoS ONE, 7(9), doi: 10.1371/journal.pone.0044396
- Lerebo, W., Callens, S., Jackson, D., Zarowsky, C., & Temmerman, M. (2014). Identifying factors associated with the uptake of prevention of mother to child HIV transmission programme in Tigray region, Ethiopia: A multilevel modeling approach. BMC Health Services Research, 14(1), 181. doi: 10.1186/1472-6963-14-181
- Marquez, C., Okiring, J., Chamie, G., Ruel, T. D., Achan, J., Kakuru, A., … Dorsey, G. (2014). Increased morbidity in early childhood among HIV-exposed uninfected children in Uganda is associated with breastfeeding duration. Journal of Tropical Pediatrics, 60(6), 434. doi: 10.1093/tropej/fmu045
- Mirkuzie, A. H., Sisay, M. M., Hinderaker, S. G., Moland, K. M., & Mørkve, O. (2012). Comparing HIV prevalence estimates from prevention of mother-to-child HIV transmission programme and the antenatal HIV surveillance in Addis Ababa. BMC Public Health, 12(1), 1113. doi: 10.1186/1471-2458-12-1113
- Mkwanazi, N. B., Rochat, T. J., & Bland, R. M. (2015). Living with HIV, disclosure patterns and partnerships a decade after the introduction of HIV programmes in rural South Africa. AIDS Care – Psychological and Socio-Medical Aspects of AIDS/HIV, doi: 10.1080/09540121.2015.1028881
- Moyer, C. A., Dako-Gyeke, P., & Adanu, R. M. (2013). Facility-based delivery and maternal and early neonatal mortality in sub-Saharan Africa: A regional review of the literature. African Journal of Reproductive Health, 17(3), 30–43. doi: 10.2307/23485710
- Mullan, Z. (2016). Transforming health care in Ethiopia. The Lancet Global Health, 4(1), e1. doi: 10.1016/S2214-109X(15)00300-9
- Nakiyingi, J. S., Bracher, M., Whitworth, J. A, Ruberantwari, A., Busingye, J., Mbulaiteye, S. M., & Zaba, B. (2003). Child survival in relation to mother’s HIV infection and survival: Evidence from a Ugandan cohort study. AIDS (London, England), 17(12), 1827–1834. doi:10.1097/01.aids.0000076274.54156.41 doi: 10.1097/00002030-200308150-00012
- Naniche, D., Bardají, A., Lahuerta, M., Berenguera, A., Mandomando, I., Sanz, S., … Menéndez, C. (2009). Impact of maternal human immunodeficiency virus infection on birth outcomes and infant survival in rural Mozambique. American Journal of Tropical Medicine and Hygiene, 80(5), 870–876. doi:10.1080/09540121.2011.579948 doi: 10.4269/ajtmh.2009.80.870
- Ndirangu, J., Bärnighausen, T., Tanser, F., Tint, K., & Newell, M.-L. (2009). Levels of childhood vaccination coverage and the impact of maternal HIV status on child vaccination status in rural KwaZulu-Natal, South Africa. Tropical Medicine & International Health, 14, 1383–1393. doi: 10.1111/j.1365-3156.2009.02382.x
- Ndirangu, J., Newell, M.-L., Tanser, F., Herbst, A. J., & Bland, R. (2010). Decline in early life mortality in a high HIV prevalence rural area of South Africa: Evidence of HIV prevention or treatment impact? Aids (London, England), 24(4), 593–602. doi: 10.1097/QAD.0b013e328335cff5
- Negash, T. G., & Ehlers, V. J. (2016). An assessment of the outcomes of prevention of mother-to-child transmission of HIV services in Addis Ababa, Ethiopia. Curationis, 39(1), 1583. doi: 10.4102/curationis.v39i1.1583
- Newell, M.-L. L., Coovadia, H., Cortina-Borja, M., Rollins, N., Gaillard, P., & Dabis, F. (2004). Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: A pooled analysis. The Lancet, 364(9441), 1236–1243. doi: 10.1016/S0140-6736(04)17140-7
- Tura, G., Fantahun, M., & Worku, A. (2013). The effect of health facility delivery on neonatal mortality: Systematic review and meta-analysis. BMC Pregnancy and Childbirth, 13(1), 18. doi: 10.1186/1471-2393-13-18
- UN DSD: Division for Sustainable Development. (2017). United Nations Partnerships for SDGs platform.
- United Nations. (2015). Countdown To Zero – Kenya. Citeseer.
- Violari, A., Cotton, M. F., Gibb, D. M., Babiker, A. G., Steyn, J., Madhi, S. A., … McIntyre, J. A. (2008). Early antiretroviral therapy and mortality among HIV-infected infants. The New England Journal of Medicine, 359(21), 2233–2244. doi: 10.1056/NEJMoa0800971
- WHO. (2010). PMTCT strategic vision 2010–2015: Preventing mother-to-child transmission of HIV to reach the UNGASS and millennium development goals.
- WHO. (2018). Mother-to-child transmission of HIV. Retrieved from http://www.who.int/hiv/topics/mtct/about/en/
- World Health Organization. (2010). Programmatic update: Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Geneva: WHO. doi:WHO/HIV/2012.6
- Wudineh, F., & Damtew, B. (2016). Mother-to-child transmission of HIV infection and its determinants among exposed infants on care and follow-up in Dire Dawa City, Eastern Ethiopia. AIDS Research and Treatment, 2016. doi: 10.1155/2016/3262746
- Zaba, B., Whitworth, J., Marston, M., Nakiyingi, J., Ruberantwari, A., Urassa, M., … Crampin, A. (2005). HIV and mortality of mothers and children. Epidemiology, 16(3), 275–280. doi: 10.1097/01.ede.0000155507.47884.43
