
ABSTRACT
In the United States, 15% of HIV-positive individuals do not know their HIV serostatus. While CDC guidelines recommend HIV testing for individuals age 13–64 years, racial and ethnic minorities continue to experience delays in HIV diagnosis. We assessed providers’ perspectives on HIV testing at an urban community health center serving racial/ethnic minority populations of low socioeconomic status. We conducted five focus groups from January 2017 to November 2017 with 74 health center staff: 20 adult medicine/primary care providers, 34 community health workers (CHWs) and community health administrators, six urgent care physicians, and fourteen behavioral health providers. Study staff analyzed transcripts using a grounded theory approach and used open coding to develop themes. We identified five themes affecting HIV testing: 1) provider perception of patients’ preferences for HIV testing; 2) competing medical and social issues; 3) inter-professional communication; 4) knowledge of clinical indicators for HIV testing; and 5) knowledge of frequency of HIV testing. Primary care physicians desired mechanisms to easily identify patients for HIV testing and assistance with testing for non-English speakers. Training to improve comfort with HIV testing, integrating CHWs into routine practice, and focusing on patients’ cultural beliefs may increase HIV testing in diverse community health centers..
Introduction
In the United States, there are approximately 1.1 million people living with HIV, including 15% who are undiagnosed (Centers for Disease Control and Prevention). Nearly 40% of new HIV infections involve transmission through an individual unaware of their HIV serostatus (Centers for Disease Control and Prevention, Citation2017), which, in 2006, led the U.S. Centers for Disease Control and Prevention (CDC) to recommend that all individuals age 13–64 receive HIV testing (Branson et al., Citation2006). The U.S. Preventive Services Task Force (USPSTF) issued similar recommendations in 2013 (U.S. Preventive Services Task Force, Citation2016).
Despite the importance of routine HIV screening, racial and ethnic minorities continue to experience greater delays in diagnosis compared to non-Hispanic whites. For example, in 2015 Hispanic or Latino individuals had been infected for a median of 3.3 years before diagnosis, while non-Hispanic whites were infected 2.2 years before diagnosis (Dailey et al., Citation2017). These disparities in HIV testing cluster particularly in Blacks (Holmes et al., Citation2008), Latinos (Espinoza, Hall, Selik, & Hu, Citation2008; Holmes et al., Citation2008), and adolescents (Balaji et al., Citation2012). Foreign-born persons in the U.S. have unique vulnerabilities to delayed HIV testing (Levison, Regan, Khan, & Freedberg, Citation2017; Ojikutu, Nnaji, Sithole-Berk, Bogart, & Gona, Citation2014; Ojikutu et al., Citation2013; Prosser, Tang, & Hall, Citation2012). The achievement of the UNAIDS 90-90-90 HIV testing and treatment goals are dependent upon individuals knowing their HIV serostatus, which underscores the role of HIV testing in realizing successes throughout the HIV care continuum (Gardner, McLees, Steiner, Del Rio, & Burman, Citation2011). Several studies have shown that providers inadequately offer HIV testing in routine medical care (Arya et al., Citation2012; Ham, Huang, Gvetadze, Peters, & Hoover, Citation2016; Mills et al., Citation2011). Reasons for this inconsistence of routine testing include a variety of barriers such as time, provider or patient discomfort, lack of funding, and lack of knowledge of current testing recommendations (Centers for Disease Control and Prevention, Citation2003; Johnson, Mimiaga, Reisner, VanDerwarker, & Mayer, Citation2011; Mayer et al., Citation2016; Mimiaga, Johnson, Reisner, Vanderwarker, & Mayer, Citation2011).
Community health centers in the U.S. provide health care for nearly 1 in 6 Medicaid beneficiaries nationally (Paradise et al., Citation2017). Nearly two-thirds of health center patients in the U.S. are from racial and ethnic minority groups (Bosshart, McNamara, & Modica, Citation2011). Among community health centers, routine HIV testing is not delivered uniformly (Johnson et al., Citation2011; Mimiaga et al., Citation2011). Lack of adherence to HIV testing recommendations in community health centers could lead to under-detection of HIV infection in low income racial/ethnic minorities who bear a disproportionate burden of the disease (Centers for Disease Control and Prevention, Citation2007, Citation2010; Millett et al., Citation2012; Rosenberg, Millett, Sullivan, Del Rio, & Curran, Citation2014). Our objective was to analyze the barriers and facilitators to HIV testing at a large urban community health care center serving a multi-cultural population to improve HIV testing in this setting.
Methods
Study setting and population
We conducted focus groups and semi-structured interviews at a multi-specialty community health center that provides care for approximately 34,000 individuals and families in Suffolk County, Massachusetts, a county with the highest prevalence of HIV in the state, nearing 1% (Massachusetts Department of Public Health, Bureau of Infectious Disease and Laboratory Sciences, Citation2018). The target populations of the health center are minority and immigrant communities surrounding the health center. Two-thirds of patients are on government-sponsored insurance. The racial/ethnic profile of the patients served by the health center includes: 53% Latino; 9% Black; 3% Asian; 31% non-Hispanic White; and 4% other. Approximately 35% of health center patients are non-English language speakers.
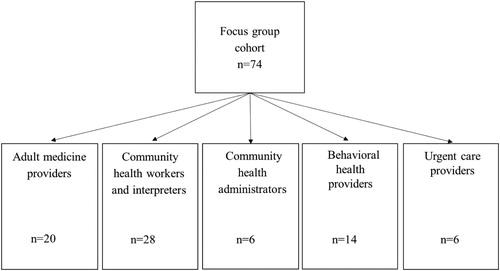
Focus groups ranged in size from 6 to 20 persons and occurred during regularly held staff meetings of the following four health center units: Adult Medicine, Community Health, Behavioral Health, and Urgent Care (). These health center units were selected because they are the primary sources of HIV testing at the health center. The Adult Medicine (n = 20) focus group was made up of primary care physicians and nurse practitioners. Community Health is composed of interpreters, community health workers (CHWs), and administrative managers. We divided this unit into three separate focus groups: we convened 28 CHWs and interpreters into two focus groups based on linguistic and cultural similarity, where possible, and community health administrators (n = 6) were interviewed in a separate focus group. The Behavioral Health (n = 14) focus group was composed of social workers, clinical psychologists, and psychiatrists. We also conducted semi-structured interviews with one medical specialty provider and one specialty clinic administrator (n = 2).
Figure 1. Study population of a qualitative study on determinants of HIV testing in a large urban community health center. Focus groups were conducted across four units: Adult Medicine, Community Health, Behavioral Health, and Urgent Care. Semi-structured interviews were conducted with an administrator and a physician from medical subspecialties.
Data collection
Focus groups and interviews occurred between January and November 2017. Interview content was standardized across groups. The interview protocol was divided into three thematic areas: (1) the current system for HIV testing; (2) barriers and facilitators for HIV testing; and (3) solutions to improve HIV testing (). All focus groups and interviews were one hour. Interviews and focus groups were conducted in English, digitally recorded, and transcribed.
Table 1. Qualitative protocol for understanding barriers and facilitators associated with HIV testing and counseling in a large community health center serving a multi-cultural population.
Data analysis
We analyzed the data using a grounded theory approach, in which theory is produced from data that has been systematically gathered, without a priori assumptions (Glaser & Strauss, Citation2017). All transcripts and audio files were analyzed independently by three researchers (AJJ, CVC, and JHL) and researchers made notes, describing emerging themes reflective of repeated individual experiences (e.g. Feeling inadequately prepared to perform HIV testing and counseling, or not having time to perform HIV counseling). These sub-themes were then grouped into themes reflective of the factors (e.g. HIV knowledge, linguistic and cultural alignment between patient and provider) and resources (e.g. Time, money, staff) that might influence uptake of HIV testing in a community health center setting. Subsequently, these themes were compared jointly among researchers who had reviewed the data independently (AJJ, DM, CVC, and JHL), and researchers resolved discrepancies through discussion. We presented preliminary results to an advisory committee comprised of representatives from each clinical unit to verify themes and enrich the data analysis. This process of “analyst triangulation” merges multiple observers to illuminate potential blind spots in the data analysis (Patton, Citation1999).
Ethical Considerations
Providers participated in focus group discussions as part of a larger quality improvement effort and were not remunerated. All participants were informed that their participation in this research study would have no bearing on their employment status or relationship with the Institution and that no identifiable information would be used. The Partners Human Research Committee (PHRC), the Institutional Review Board (IRB) of Partners HealthCare, approved this study.
Results
We identified five primary themes explaining HIV testing in this setting: (1) provider perception of patient attitudes and beliefs; (2) time and the prioritization of medical and social issues; (3) interprofessional communication; (4) clinical indicators for testing; and (5) knowledge about the importance of routine HIV testing.
Provider perception of patient attitudes and beliefs
Individuals across disciplines expressed concerns about how to address patients’ unique cultural perceptions of HIV. Many of these perceptions were based on HIV-related stigma, lack of trust in the healthcare system, and a general lack of knowledge of current HIV treatment options and efficacy. Providers uniformly expressed concern that their patients would not want HIV testing because of HIV-related stigma and the consequences of having to disclose this information within the community. CHWs agreed that HIV stigma might negatively influence a patient’s willingness to accept HIV testing: One CHW noted, “In my [Somali] culture, it’s so taboo that you just don’t bring up things [like HIV].” Common feedback from all providers was the concern that patients would fear a breach in test confidentiality and could experience discrimination in tightly knit communities. One Adult Medicine provider described an encounter with an HIV-positive patient as an example of community beliefs about HIV: “He did not want to be treated here … he did not want it somehow getting out into the community.”
Providers identified patients’ HIV-related misconceptions as a deterrent to HIV testing. For example, one CHW noted that their patients did not appreciate the possibility of good quality of life with HIV and, even more, that a common belief was that HIV was a fatal diagnosis: “For HIV … that’s a loaded word, term, thing to think about. I think [for the patient] it just automatically goes to ‘death’ … it’s a hard thing to think about.” Respondents from the CHW group acknowledged that this tendency to relate HIV infection to death was a notable trend in the immigrant and non-English language speaking patient populations served by the health center.
Addressing HIV-related misconceptions led providers to discuss the adequacy of communication about HIV. One Adult Medicine provider described how it was difficult to overcome patient concerns about HIV-related fears and stigma since providers lacked culturally and linguistically accessible health communication tools around sexual health: “How do we give the key information on [safer] sex [to people] from different cultures … and how we can talk about it?”
Providers’ awareness of this potential patient concern for test confidentiality prompted providers to use telephone-based interpreter services even if in-person interpreter services were available.
Time and the prioritization of medical and social issues
Insufficient time to conduct HIV testing and needing to prioritize more pressing medical and social issues were themes that emerged across multiple focus groups and interviews. Adult Medicine providers expressed time concerns due to engaging an interpreter (either in person or by telephone) for low-English language speaking patients. One provider noted that “you don’t have as much time if you have to use an interpreter … so [HIV counseling and testing is] something that might get left off,” and that “you routinely run into 40-minute visits if you have to use [telephone interpretation services].” Additionally, Adult Medicine providers expressed concern about routine HIV testing potentially taking away from other pressing clinical matters. One Adult Medicine provider remarked, “I’m really concerned that everything we add is going to push something out.” Providers outside of primary care also discussed the topics of prioritization of medical and social issues and the challenge of time constraints:
[Testing for HIV] may not be the first thing that crosses [primary care providers’] minds … you only have a few minutes of your visit time, and then you have to write the note. [Subspecialty provider]
You have to understand, [the] urgent care environment is not the right environment to have these long, prolonged discussions … it’s hard for us to get involved in that. We have like 50 or 60 other patients waiting to be seen. [Urgent care provider]
I could think of a lot of patients who are IV drug users and could benefit from us having conversations with them … I think we’re focused so much on psychosocial stressors that the health piece can take a backseat, frankly. [Community Health administrator]
Interprofessional communication
Participants discussed the difficulties in communicating between clinical units so that providers share in the responsibility for HIV testing. Primarily, this theme emerged during discussions regarding which clinical unit should be responsible for HIV testing, the role of referrals for HIV testing or risk reduction, and the ways that providers could communicate test results with one another.
Behavioral Health and Community Health staff discussed infrequent requests for referrals from primary care providers to discuss HIV risk behaviors. One Behavioral Health provider stated, “I have that kind of input from the providers … around hepatitis C but not [with] HIV.” Another provider agreed that primary care providers are not “passing them along for HIV-related issues.” CHWs stated interest in integrating themes around HIV risk reduction and the value of HIV testing, but that they would not unless the patient or provider prompted them. One CHW echoed this commonly felt perspective that “[we] only deal with the issue the provider wants [us] to,” and, in response to questions regarding why CHWs are not talking about HIV more often with their patients, one CHW stated that “the referrals aren’t there.”
Clinical indicators for testing
Throughout focus groups and interviews, participants shared indications for HIV testing. Most of these indications fell under the purview of three categories: (1) pregnancy, (2) hepatitis, and (3) behavioral risk (e.g. Condomless sex, injection drug use, new sexual partner). Mentioned several times throughout discussions was the opinion that pregnant patients are always tested for HIV as part of their screening. One Community Health administrator observed that although she had not come across many HIV-positive patients, the ones she had encountered were pregnant and diagnosed through screening:
Well, I’m thinking of the only cases that I’ve had … and they were pregnant. It wasn’t exactly like a referral; we learned that this was a medical issue and going on with the mom, so it was an opportunity to work with the mom because she’s having a baby.
Lastly, risk or symptom-based screening was cited as the predominant reason for testing by many providers, despite current recommendations adopting routine HIV testing. Urgent care providers emphasized using symptom-based screening, such as an AIDS-related complication, presentation for STI testing, or the request by a patient for HIV testing, noting that the urgent care setting requires a more focused clinical approach. One urgent care provider noted, however, that patients who perceived themselves as being at low risk for infection generally decline HIV testing. Therefore, low perceived risk, by either the patient or the provider, acted as a barrier to HIV testing.
Knowledge about the importance of routine HIV testing
Providers with more HIV training, either formal or informal (e.g. Education or personal experience), reported thinking about screening their patients for HIV routinely. However, this awareness of the importance of routine HIV testing was not uniformly expressed across the disciplines. One Behavioral Health participant stated, “I was seeing [two patients] more frequently than their primary care doctor and certainly didn’t think about testing them and, you know, just doing their labs.” Among Adult Medicine providers, there was also variation, with one provider remarking, “I bet you that there are a lot of people in our clinic who I’ve never screened because they’re low risk and I forget about it.”
Providers whose jobs are not directly related to HIV care reported substantially less education about HIV and seemed to be unaware of consequential changes to HIV testing guidelines that have occurred, such as the removal of written informed consent for testing in Massachusetts in 2012, as well as practice guidelines for routine testing. In a related view, one subspecialty provider posited that primary care providers must also be educated that “HIV has not gone away,” adding that although the diagnostic process and treatments have improved, the end of the HIV epidemic is still not in sight. Adult medicine providers discussed that few positive HIV test results indicated to them that HIV might not be prevalent. Similar views and questions arose with other disciplines.
Discussion
This study demonstrates factors affecting provision of HIV testing that may be unique to large multi-disciplinary community health centers with diverse patient population. While primary care providers were the principle source of HIV testing, all providers described the challenge of providing HIV testing to socially and medically complex patients, where cultural and linguistic barriers exist between patient and provider. Providers were receptive to HIV testing, however, barriers to interprofessional and multidisciplinary communication limited attaining the goal of universal HIV testing.
Our findings shed light on the persistent challenge of enhancing care for HIV prevention and treatment for minority populations, including individuals with low-English Language proficiency. However, we found that providers perspectives on patient’s HIV-related beliefs and adequate patient-provider communication were central to delivering HIV testing in this multi-cultural patient population. Integration of CHWs and interpreters into the clinical encounter may facilitate cultural and linguistic brokerage that can promote delivery of HIV testing.
The use of lay health workers to facilitate HIV testing has shown increases in HIV testing the U.S. and abroad (Kennedy, Yeh, Johnson, & Baggaley, Citation2017). Yet, despite these potential interventions, providers must still adequately address the cultural factors that influence patient HIV test acceptability. Increasingly, the literature suggests the value of “cultural humility” (or “cultural competence”), building trust with patients of diverse backgrounds (Saha, Jacobs, Moore, & Beach, Citation2010; Saha et al., Citation2013; Saha et al., Citation2011). This type of training includes implicit bias awareness or discussion of ways in which to assess patients’ cultural beliefs and integrate them into patient care.
Despite the care that may be taken by hospital systems and providers to maintain confidentiality of test results, particularly in a growing electronic medical age, these concerns continue to inform patient acceptability of HIV testing (Joseph et al., Citation2014; White et al., Citation2015). We found that providers feared that patients, especially those belonging to tightly knit ethnic groups, would be wary of HIV testing due to privacy concerns. This was particularly relevant when CHWs and interpreters were known to the patient or from the same communities. Institutional mistrust and previous experiences of discrimination may influence patient attitudes about HIV and HIV testing, and aspects of mistrust should be addressed in provider-patient encounters (Hoyt et al., Citation2012). Providers should consider emphasizing the confidentiality of test results in discussions with patients.
Provider concerns regarding time constraints remain in the foreground of barriers to routine provider-initiated HIV testing (Burke et al., Citation2007; Johnson et al., Citation2011; Mayer et al., Citation2016; Mimiaga et al., Citation2011). In addition to feeling the need to prioritize care for more prevalent diseases, such as diabetes and heart disease, providers also cited the additional time needed to provide competent care to foreign-born patients (e.g. Using a medical interpreter) as adding to the pressure to focus on matters other than HIV testing during a short visit. Integration of HIV testing into routine workflow may mitigate these problems.
Expanding routine HIV testing in community health center settings will ultimately require the skills of multiple clinical units collaborating in an integrated fashion as patients seek care across a health center. One suggested way to improve this coordination of care is the development of a testing algorithm informed by current guidelines (Branson et al., Citation2006; U.S. Preventive Services Task Force, Citation2016) as well as the development of specifications as to how providers should link positive individuals to HIV care and high-risk negative individuals to pre-exposure prophylaxis (PrEP) and other risk reduction services. This algorithm should involve the input of all clinical units, addressing questions regarding whether a single clinical unit should be responsible for HIV testing, linking newly diagnosed patients to care, and ensuring that HIV-negative individuals receive additional tests in the future. Employing a strategy to react to both negative and positive HIV test results could prevent it from becoming a “test that leads to nowhere” (El-Sadr, Gamble, & Cohen, Citation2013). Furthermore, workflow integration might include the development and implementation of alerts in the electronic medical record, soliciting medical assistants to include HIV testing as part of the routine health maintenance review, training providers to deliver brief scripts for verbal consent, and task-shifting components of HIV counseling to CHWs and interpreters.
There were several limitations of this study. Focus group discussions and interviews reflected provider perspectives of HIV testing in this community healthcare center, which may differ from actual patient experiences. The study setting was a large urban clinic, which may limit the generalizability.
Addressing the HIV testing needs of multi-cultural patient populations has broad implications. As geographic patterns of migration shift due to natural disasters, immigration policy, and employment opportunities, smaller cities and rural locations may face linguistic and cultural challenges to meet the health needs of newly arriving diverse communities (Echeniqu, Citation2018; Karimi & Kopan, Citation2018; Nathenson, Saloner, Richards, & Rhodes, Citation2016). Fully involving and leveraging the strengths of various clinical units as well as integrating testing into routine health care and provider workflow may improve routine HIV testing. This would improve HIV diagnosis and linkage of individuals to needed prevention and treatment services.
Acknowledgements
This work was supported by the National Institutes of Health (K23 MH100978, R01 AI042006), Harvard University Center for AIDS Research (P30-AI060354), a CFAR Adelante award funded by the NIH-funded Centers for AIDS Research (P30AI050409 and P30AI117970) and the U.S. National Institutes of Health, Massachusetts General Hospital Executive Committee on Community Health, and financial contributions from Harvard University and its affiliated academic health care centers. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Medical School and its affiliated academic health care centers or the National Institutes of Health.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Arya, M., Patuwo, B., Lalani, N., Bush, A. L., Kallen, M. A., Street, R. L., … Giordano, T. P. (2012). Are primary care providers offering HIV testing to patients in a predominantly Hispanic community health center? An exploratory study. AIDS Patient Care and STDs, 26(5), 256–258. doi:10.1089/apc.2011.0402.
- Balaji, A. B., Eaton, D. K., Voetsch, A. C., Wiegand, R. E., Miller, K. S., & Doshi, S. R. (2012). Association between HIV-related risk behaviors and HIV testing among high school students in the United States, 2009. Archives of Pediatrics & Adolescent Medicine, 166(4), 331–336. doi:10.1001/archpediatrics.2011.1131.
- Bosshart, J., McNamara, K., & Modica, C. (2011). Implementation of routine HIV testing in health care settings: Issues for community health centers.
- Branson, B. M., Handsfield, H. H., Lampe, M. A., Janssen, R. S., Taylor, A. W., Lyss, S. B., & Clark, J. E. (2006). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recommendations and Reports, 55(Rr-14), 1–17.
- Burke, R. C., Sepkowitz, K. A., Bernstein, K. T., Karpati, A. M., Myers, J. E., Tsoi, B. W., & Begier, E. M. (2007). Why don’t physicians test for HIV? A review of the US literature. Aids (London, England), 21(12), 1617–1624. doi: 10.1097/QAD.0b013e32823f91ff
- Centers for Disease Control and Prevention. Estimated HIV incidence and prevalence in the United States, 2010–2015.
- Centers for Disease Control and Prevention. (2003). Late versus early testing of HIV–16 Sites, United States, 2000–2003. MMWR Morbidity and Mortality Weekly Report, 52(25), 581–586.
- Centers for Disease Control and Prevention. (2007). Racial/ethnic disparities in diagnoses of HIV/AIDS–33 states, 2001–2005. MMWR Morbidity and Mortality Weekly Report, 56(9), 189–193.
- Centers for Disease Control and Prevention. (2010). Estimated lifetime risk for diagnosis of HIV infection among Hispanics/Latinos—37 states and Puerto Rico, 2007. MMWR Morbidity and Mortality Weekly Report, 59(40), 1297–1301.
- Centers for Disease Control and Prevention. (2017). Vital signs.
- Dailey, A. F., Hoots, B. E., Hall, H. I., Song, R., Hayes, D., Fulton, P., … Valleroy, L. A. (2017). Vital signs: Human immunodeficiency virus testing and diagnosis delays—United States. MMWR. Morbidity and Mortality Weekly Report, 66(47), 1300–1306. doi:10.15585/mmwr.mm6647e1.
- Echeniqu, M. (2018). Exodus: The post-hurricane Puerto Rican diaspora, Mapped.
- El-Sadr, W. M., Gamble, T. R., & Cohen, M. S. (2013). Linkage from HIV testing to care: A positive test often leads nowhere. Sexually Transmitted Diseases, 40(1), 26–27. doi:10.1097/OLQ.0b013e31827e612b.
- Espinoza, L., Hall, H. I., Selik, R. M., & Hu, X. (2008). Characteristics of HIV infection among Hispanics, United States 2003–2006. JAIDS Journal of Acquired Immune Deficiency Syndromes, 49(1), 94–101. doi:10.1097/QAI.0b013e3181820129.
- Gardner, E. M., McLees, M. P., Steiner, J. F., Del Rio, C., & Burman, W. J. (2011). The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clinical Infectious Diseases, 52(6), 793–800. doi:10.1093/cid/ciq243.
- Glaser, B. G., & Strauss, A. L. (2017). Discovery of grounded theory: Strategies for qualitative research. Piscataway, New Jersey: Routledge.
- Ham, D. C., Huang, Y. L., Gvetadze, R., Peters, P. J., & Hoover, K. W. (2016). Health care use and HIV testing of males aged 15–39 years in physicians’ offices—United States, 2009–2012. MMWR. Morbidity and Mortality Weekly Report, 65(24), 619–622. doi:10.15585/mmwr.mm6524a3.
- Holmes, L., Jr., Monjok, E., Ward, D., Garrison, O. M., Toney, E. D., Ogungbade, G., & Essien, E. J. (2008). Racial variance in rationale for HIV testing in community-based setting in the United States: Evidence from the national health interview survey. Journal of the International Association of Physicians in AIDS Care, 7(2), 61–68. doi:10.1177/1545109708315327.
- Hoyt, M. A., Rubin, L. R., Nemeroff, C. J., Lee, J., Huebner, D. M., & Proeschold-Bell, R. J. (2012). HIV/AIDS-related institutional mistrust among multiethnic men who have sex with men: Effects on HIV testing and risk behaviors. Health Psychology, 31(3), 269–277. doi:10.1037/a0025953.
- Johnson, C. V., Mimiaga, M. J., Reisner, S. L., VanDerwarker, R., & Mayer, K. H. (2011). Barriers and facilitators to routine HIV testing: Perceptions from Massachusetts community health center personnel. AIDS Patient Care and STDs, 25(11), 647–655. doi:10.1089/apc.2011.0180.
- Joseph, H. A., Belcher, L., O’Donnell, L., Fernandez, M. I., Spikes, P. S., & Flores, S. A. (2014). HIV testing among sexually active Hispanic/Latino MSM in Miami-Dade county and New York City: Opportunities for increasing acceptance and frequency of testing. Health Promotion Practice, 15(6), 867–880. doi:10.1177/1524839914537493.
- Karimi, F., & Kopan, T. (2018). There are 2,300 migrant kids spread across the US. What happens to them next?.
- Kennedy, C. E., Yeh, P. T., Johnson, C., & Baggaley, R. (2017). Should trained lay providers perform HIV testing? A systematic review to inform world health organization guidelines. AIDS Care, 29(12), 1473–1479. doi: 10.1080/09540121.2017.1317710
- Levison, J. H., Regan, S., Khan, I., & Freedberg, K. A. (2017). Foreign-born status as a predictor of engagement in HIV care in a large US metropolitan health system. AIDS Care, 29(2), 244–251. doi: 10.1080/09540121.2016.1210077
- Massachusetts Department of Public Health, Bureau of Infectious Disease and Laboratory Sciences (2018). Massachusetts HIV/AIDS Epidemiologic Profile: Regional HIV/AIDS Epidemiologic Profile of Suffolk County, Massachusetts. https://www.mass.gov/lists/hivaids-epidemiologic-profiles Published September 2018.
- Mayer, K. H., Crawford, P., Dant, L., Gillespie, S., Singal, R., Vandermeer, M., … McBurnie, M. A. (2016). HIV and hepatitis C virus screening practices in a geographically diverse sample of American community health centers. AIDS Patient Care and STDs, 30(6), 237–246. doi: 10.1089/apc.2015.0314
- Millett, G. A., Peterson, J. L., Flores, S. A., Hart, T. A., Jeffries, W. L. t., Wilson, P. A., … Remis, R. S. (2012). Comparisons of disparities and risks of HIV infection in black and other men who have sex with men in Canada, UK, and USA: A meta-analysis. The Lancet, 380(9839), 341–348. doi: 10.1016/s0140-6736(12)60899-x
- Mills, C. W., Sabharwal, C. J., Udeagu, C. C., Bocour, A., Bodach, S., Shepard, C., & Begier, E. M. (2011). Barriers to HIV testing among HIV/AIDS concurrently diagnosed persons in New York City. Sexually Transmitted Diseases, 38(8), 715–721. doi: 10.1097/OLQ.0b013e31820ead73
- Mimiaga, M. J., Johnson, C. V., Reisner, S. L., Vanderwarker, R., & Mayer, K. H. (2011). Barriers to routine HIV testing among Massachusetts community health center personnel. Public Health Reports, 126(5), 643–652. doi: 10.1177/003335491112600506
- Nathenson, R. A., Saloner, B., Richards, M. R., & Rhodes, K. V. (2016). Spanish-speaking immigrants’ access to safety net providers and translation services across traditional and emerging US destinations. The Milbank Quarterly, 94(4), 768–799. doi: 10.1111/1468-0009.12231
- Ojikutu, B., Nnaji, C., Sithole, J., Schneider, K. L., Higgins-Biddle, M., Cranston, K., & Earls, F. (2013). All black people are not alike: Differences in HIV testing patterns, knowledge, and experience of stigma between U.S.-born and non-U.S.-born blacks in Massachusetts. AIDS Patient Care and STDs, 27(1), 45–54. doi: 10.1089/apc.2012.0312
- Ojikutu, B., Nnaji, C., Sithole-Berk, J., Bogart, L. M., & Gona, P. (2014). Barriers to HIV testing in black immigrants to the U.S. Journal of Health Care for the Poor and Underserved, 25(3), 1052–1066. doi: 10.1353/hpu.2014.0141
- Paradise, J., Rosenbaum, S., Markus, A., Sharac, J., Tran, C., Reynolds, D., & Shin, P. (2017). Community health centers: Recent growth and the role of the ACA. Kaiser Family Foundation. Retrieved from https://www.kff.org/medicaid/issue-brief/community-health-centers-recent-growth-and-the-role-of-the-aca/
- Patton, M. Q. (1999). Enhancing the quality and credibility of qualitative analysis. Health Services Research, 34(5 Pt 2), 1189–1208.
- Prosser, A. T., Tang, T., & Hall, H. I. (2012). HIV in persons born outside the United States, 2007–2010. Jama, 308(6), 601–607. doi: 10.1001/jama.2012.9046
- Rosenberg, E. S., Millett, G. A., Sullivan, P. S., Del Rio, C., & Curran, J. W. (2014). Understanding the HIV disparities between black and white men who have sex with men in the USA using the HIV care continuum: A modelling study. The Lancet HIV, 1(3), e112–e118. doi: 10.1016/s2352-3018(14)00011-3
- Saha, S., Jacobs, E. A., Moore, R. D., & Beach, M. C. (2010). Trust in physicians and racial disparities in HIV care. AIDS Patient Care and STDs, 24(7), 415–420. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/20578909 doi: 10.1089/apc.2009.0288
- Saha, S., Korthuis, P. T., Cohn, J. A., Sharp, V. L., Moore, R. D., & Beach, M. C. (2013). Primary care provider cultural competence and racial disparities in HIV care and outcomes. Journal of General Internal Medicine, 28(5), 622–629. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/23307396 doi: 10.1007/s11606-012-2298-8
- Saha, S., Sanders, D. S., Korthuis, P. T., Cohn, J. A., Sharp, V. L., Haidet, P., … Beach, M. C. (2011). The role of cultural distance between patient and provider in explaining racial/ethnic disparities in HIV care. Patient Education and Counseling, 85(3), e278–e284. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/21310581 doi: 10.1016/j.pec.2011.01.012
- U.S. Preventive Services Task Force. (2016). Final update summary: Human immunodeficiency virus (HIV) infection: Screening.
- White, B. L., Walsh, J., Rayasam, S., Pathman, D. E., Adimora, A. A., & Golin, C. E. (2015). What makes me screen for HIV? Perceived barriers and facilitators to conducting recommended routine HIV testing among primary care physicians in the southeastern United States. Journal of the International Association of Providers of AIDS Care (JIAPAC), 14(2), 127–135. doi: 10.1177/2325957414524025
