
ABSTRACT
Nearly 80 million people have been forcibly displaced by persecution, violence, and disaster. Displaced populations, including refugees, face health challenges such as resource shortages, food and housing insecurity, violence, and disrupted social support. People living with HIV in refugee settings have decreased engagement with HIV services compared to non-refugee populations, and interventions are needed to enhance linkage to care. However, designing health interventions in humanitarian settings is challenging. We used Intervention Mapping (IM), a six-step method for developing theory- and evidence-based health interventions, to design a program to increase linkage to HIV care for refugees and Ugandan nationals in Nakivale Refugee Settlement in Uganda. We engaged a diverse group of stakeholders (N = 14) in Nakivale, including community members and humanitarian actors, in an interactive workshop focusing on IM steps 1–4. We developed a chronic care program that would integrate HIV care with services for hypertension and diabetes at accessible community sites, thereby decreasing stigma around HIV treatment and improving access to care. IM provided an inclusive, efficient method for integrating community members and program implementers in the intervention planning process, and can be used as a method-driven approach to intervention design in humanitarian settings.
Introduction
Uganda is home to 1.4 million refugees, the third largest refugee population in the world (UNHCR, Citation2020). Displaced populations, including refugees, face particular health challenges: prior and ongoing trauma including sexual and gender-based violence, impoverishment and food insecurity, unstable and unsafe housing, destruction of infrastructure, the presence of military forces and armed groups, eroded social support, and disrupted behavioral norms (IASC Task Force on HIV/AIDS in Emergency Settings, Citation2003; UN Food and Agriculture Organization, Citation2010; UNHCR, Citation2017). In this challenging context, there is rapid spread of infectious diseases, including sexually transmitted infections such as HIV, and inadequate management of chronic health issues (IASC Task Force on HIV/AIDS in Emergency Settings, Citation2003).
Designing health interventions in humanitarian settings is difficult and complex, and empiric evidence from non-emergency settings may not be generalizable. Both the performance of health systems and the health behaviors of individual people are altered by the challenges of the humanitarian context. Furthermore, the experience of displaced people varies by country of origin, and it evolves over time and space – from the acute emergency, to transit through unsafe territories, to residence in camps, to assimilation into a host population or longer-term refugee settlement (Wirtz et al., Citation2013).
The data on designing optimal health interventions for humanitarian settings are relatively sparse; data collection is difficult, and research has often been deprioritized in favor of quick implementation of life-saving interventions (UNHCR, Citation2002). However, with growing recognition that program efficacy is critically important to the populations affected by crises, and that well-intentioned aid programs can have adverse consequences, there has been increased emphasis on monitoring and evaluation of health interventions (UNHCR, Citation2002).
Lessons have emerged. Organizations must coordinate their efforts in order to address gaps and avoid duplication in services, and at-risk groups including women, children, and mobile populations may need specific programming (IASC Task Force on HIV/AIDS in Emergency Settings, Citation2003). Additionally, the target populations, local and national governments, and supporting organizations should be involved in resource allocation and program design to ensure that interventions are culturally appropriate and acceptable to the target populations, without perpetuating discrimination and stereotypes (IASC Task Force on HIV/AIDS in Emergency Settings, Citation2003; UN Food and Agriculture Organization, Citation2010).
Designing interventions to improve HIV care cascade outcomes for displaced populations is crucial for achieving UNAIDS treatment targets (UNAIDS Programme Coordinating Board, Citation2020). The steps in the HIV care cascade are HIV testing, linkage to care, initiation of antiretroviral therapy (ART), suppression of viral load, and retention in care (Gardner et al., Citation2011). In Nakivale Refugee Settlement in Uganda, 6850 people (70% of whom were refugees) were voluntarily tested for HIV from March 2013 to October 2014. The HIV prevalence among refugees was 2% and the prevalence among Ugandans was 9%, compared to a Ugandan national prevalence of 6.0% in 2016 (Uganda AIDS Commission, Citation2017). Of the people who tested positive for HIV, only 54% linked to care within 90 days after diagnosis (O’Laughlin et al., Citation2017), compared to 74% in another Ugandan cohort (Billioux et al., Citation2017) and 61% overall for sub-Saharan Africa (Sharma et al., Citation2015). This suggests that there may be particular barriers to engaging with HIV care in the refugee settlement. None of the following demographic variables were significantly associated with linkage to care: gender, age, refugee status, country of origin, residence in Nakivale, distance from clinic, years living in Nakivale, relationship status, education level, knowledge about HIV, or prior negative HIV test (O’Laughlin et al., Citation2016). This suggests that engagement with HIV care may be associated with more complex factors, such as mental health and substance use, HIV stigma and social support, or migration patterns and resettlement policies.
Intervention Mapping (IM) is a method for developing health promotion programs (Bartholomew et al., Citation1998; Bartholomew Eldredge et al., Citation2016) that builds on previous health intervention models (Green et al., Citation2005; Kirby, Citation2001) to bridge across theory, empiric evidence, and practical implementation. Its iterative step-by-step approach facilitates stakeholder participation throughout the intervention planning process (Bartholomew Eldredge et al., Citation2016). IM has been used in diverse settings to design interventions for reducing sexually transmitted infections and improving adherence to treatment (Côté et al., Citation2008; Mkumbo et al., Citation2009). Few studies have attempted to quantify the effect of IM on the efficacy of health interventions, but one systematic review concluded that programs designed using the IM approach had better uptake compared to control programs (Garba & Gadanya, Citation2017).
Based on the adaptability, efficacy, and emphasis on participation of diverse stakeholders, we selected IM as a method for designing a program to enhance linkage to HIV care for individuals newly diagnosed with HIV in Nakivale Refugee Settlement.
Methods
Overview of IM steps
A working group of stakeholders is selected to participate in the six-step intervention planning process (). In Step 1, a needs assessment is performed to characterize the health problem that will be addressed by the intervention. The health problem is described according to the PRECEDE model, which is an established framework for assessing health needs and applying theories to health interventions () (Green et al., Citation2005). In Step 2, the goals of the intervention are established. In Step 3, theory-based change methods and practical applications are selected. In Step 4, program materials are designed and piloted. In Step 5, a plan is developed for adoption, implementation, and maintenance of the intervention. In Step 6, indicators and measures are selected to assess the intervention (Bartholomew Eldredge et al., Citation2016).
Figure 1. Logic model of the problem of untreated HIV (Step 1). The logic model of the problem of untreated HIV, as described by the Intervention Mapping working group in Nakivale Refugee Settlement. From right to left, the ways in which untreated HIV affects quality of life and health (Phases 1 and 2); the behavioral and environmental factors which contribute (Phase 3); and the behavioral and environmental determinants of those factors (Phase 4).
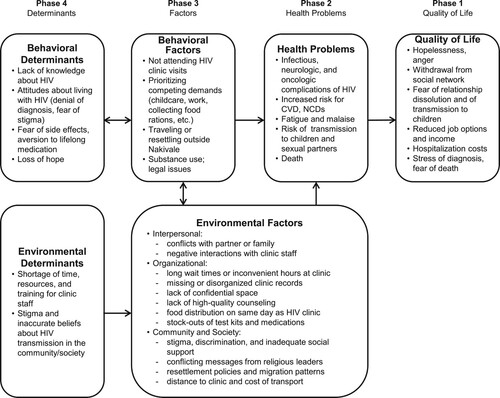
Table 1. Six steps of Intervention Mapping (adapted from Bartholomew et al., Citation2016).
Application of IM in Nakivale Refugee Settlement
Study setting
Nakivale Refugee Settlement in Uganda hosts over 100,000 refugees from the Democratic Republic of the Congo, Somalia, Burundi, Rwanda, and other countries (UNHCR, Citation2019). There are four health centers in the settlement, which are attended by refugees and Ugandan nationals living in and around Nakivale. As part of an ongoing prospective research study, a research team collaborates with Medical Teams International (the implementing partner for health care delivery in Nakivale) to offer free HIV testing, counseling, and treatment. Clients who are diagnosed with HIV are referred to the weekly HIV clinic.
IM workshop
In this study, IM was used to design a program to address the health problem of untreated HIV in Nakivale. For the needs assessment (Step 1), we conducted a literature review on the factors that affect linkage to care in Uganda and in sub-Saharan Africa (Jain et al., Citation2021; Pell et al., Citation2019; Rentsch et al., Citation2018; Sabapathy et al., Citation2018; Sanga et al., Citation2018; Seeley et al., Citation2018), and reviewed findings from an ongoing prospective research study of routine clinic-based HIV testing in Nakivale (O’Laughlin et al., Citation2017, Citation2013, Citation2014, Citation2016, Citation2018).
Next, a diverse working group of stakeholders was purposively selected to participate in a one-day IM workshop in January 2019, led and facilitated by our research team. There were 14 participants, including representatives from Medical Teams International, the United Nations High Commissioner for Refugees (UNHCR), the American Refugee Committee (ARC), and Tutapona (a local non-governmental organization). Participants also included church leaders, community members, and researchers. Several participants were refugees (from Rwanda, Ethiopia, and the Democratic Republic of the Congo), and at least one was living with HIV. During the stakeholder workshop, we focused on IM steps 1 through 4 (), as has been described in previous literature (Corbie-Smith et al., Citation2010; Wolfers et al., Citation2007). We used small-group breakout sessions and large-group discussions to generate and refine ideas for each IM step. After the workshop, we presented the findings to additional stakeholders for feedback and revisions.
Results
Step 1: Logic model of the problem
Based on published literature, data from ongoing research in Nakivale, and participants’ experiences, the working group described in detail the health problem of untreated HIV in Nakivale. Participants produced a logic model of the problem of untreated HIV (), using the PRECEDE framework for assessing health needs (Bartholomew Eldredge et al., Citation2016; Green et al., Citation2005).
The working group enumerated the ways that HIV causes secondary health problems and reduces people’s quality of life (, Phases 1 and 2). They identified the primary behavioral and environmental factors that prevent people living with HIV (PLHIV) from engaging with medical care (, Phase 3). Some factors identified were specific to the refugee setting: for example, in Nakivale, food distribution and HIV clinic sometimes occur on the same day, which prevents clients from attending clinic. Additionally, some religious leaders in Nakivale counsel that HIV can be cured through prayer or alternative healing methods, which discourages participation in care. Resettlement policies and migration patterns make continuity of care difficult for the refugees living in Nakivale.
Finally, the working group examined behavioral and environmental determinants, or, the factors causing individual and environmental actors to engage in behaviors that prevent linkage to HIV care (, Phase 4). In terms of behavioral determinants, the working group emphasized that lack of knowledge about HIV and attitudes about living with HIV – including denial of the diagnosis and fear of anticipated stigma – are major reasons for avoiding health care.
Environmental determinants identified by the working group included a shortage of resources and training for clinic staff, which may contribute to inadequate skills and self-efficacy to provide high-quality, empathic care for PLHIV. On the community and society levels, deeply ingrained stigma and inaccurate beliefs about HIV transmission cause people to discriminate against their family members and neighbors with HIV.
Step 2: Program outcomes and objectives
Program outcomes
Behavioral and environmental outcomes are health-promoting behaviors and conditions that would facilitate PLHIV in engaging with HIV care. The working group selected one primary behavioral outcome: individuals who are newly diagnosed with HIV will attend HIV clinic. They selected three primary environmental outcomes:
HIV clinics are accessible to clients in their communities.
Clinic staff provide high-quality, empathic care to clients with HIV.
Clients can access supportive social networks.
Performance objectives, determinants, and change objectives
For each of the behavioral and environmental outcomes, the working group developed performance objectives, determinants, and change objectives. Performance objectives are specific actions that must take place in order for the behavioral or environmental outcome to happen. Determinants are the reasons why individuals and environmental actors would complete the performance objectives. Change objectives describe what must change relative to each determinant in order to accomplish the performance objectives ().
Table 2. Matrices of Change Objectives (Step 2).
The working group emphasized that the problem of insufficient resources, including stock-outs of medications and diagnostic tests, inadequate clinic space for confidential counseling, and overburdened clinic staff – was a major barrier to achieving performance objectives. The group agreed that this problem was highly important, but difficult to solve with a single intervention. Therefore, they brainstormed strategies for using existing resources more effectively. For example, to address the problem of overburdened clinic staff, the working group suggested supporting the staff with social events and workshops to prevent burnout and foster empathy for clients.
Step 3: Program design
In Step 3, the working group developed the basic features of the intervention. They used an existing taxonomy (Bartholomew Eldredge et al., Citation2016) to select change methods and practical applications for each change objective (). They found that some change objectives could be accomplished using overlapping methods and applications, and grouped those together in . For example, the change objectives concerning the attitudes and values of clinic staff (C.1 to C.4) could all be addressed by improving staff support and training workshops, so these objectives were grouped together in .
Table 3. Change Methods and Practical Applications (Step 3).
To guide the working group discussion, the research team provided background information on interventions that have been successful in improving HIV care in other settings, including integrated HIV/NCD programs (Garrib et al., Citation2018; Haldane et al., Citation2018; Watt et al., Citation2017) and adherence clubs (Bateman, Citation2013; Wilkinson, Citation2013). HIV/NCD programs integrate HIV care with management of non-communicable diseases (NCDs) including diabetes and hypertension. These programs aim to reduce the stigma associated with HIV by treating HIV alongside other chronic diseases (Garrib et al., Citation2018). Another type of intervention, adherence clubs, are groups of clients with HIV who meet every 1–4 months in community- or clinic-based sites, facilitated by lay health workers who perform clinical assessments, counsel about treatment and adherence, and distribute ART. This intervention aims to improve social support (Mukumbang et al., Citation2019) and retention in HIV care (Bock et al., Citation2019; Grimsrud et al., Citation2016; Hanrahan et al., Citation2019; Luque-Fernandez et al., Citation2013; Sharp et al., Citation2019; Tsondai et al., Citation2017).
With this evidence base in mind, the working group brainstormed several practical applications that would be feasible in Nakivale. An HIV clinic could be combined with other services (e.g., diabetes and hypertension management) in order to increase the perceived benefits of HIV care and reduce HIV stigma. Groups of PLHIV could meet for education sessions and social support. Staff training could be supplemented by educational methods such as role-play and empathy training, as well as burnout prevention strategies. Additionally, some strategies that are already used in Nakivale, such as posttest HIV counseling and involvement of lay health workers and expert clients, could be optimized to accomplish additional change objectives.
Step 4: Program production
In Step 4, the working group refined the practical applications from Step 3 into cohesive program components. The intervention described was community-based chronic care teams, or “C-3 teams,” in which clients would receive counseling and medications for HIV, diabetes, and hypertension at accessible, confidential community sites, such as schools or churches. Clients would be enrolled in the program immediately after diagnosis in order to facilitate linkage to care. They would receive services for diabetes and hypertension in addition to HIV, in order to increase the perceived benefit of the clinic (O’Laughlin et al., Citation2013). Additionally, the integration of HIV care with that of other chronic diseases would reduce HIV-related stigma (Garrib et al., Citation2018).
In addition to the primary intervention, there would be two additional program components. First, the staff members for C-3 teams would undergo extensive training including role-plays and guided practice of posttest counseling. They would learn principles of motivational interviewing and participate in empathy training. They would also demonstrate knowledge about HIV management, and practice delivering this information in a client-centered style. Second, there would be a workshop for community leaders to use their leadership role to increase knowledge about HIV and foster empathy for PLHIV in their communities.
Discussion
Despite the unprecedented number of refugees and other forcibly displaced people in the world today (UNHCR, Citation2020), there is a scarcity of published literature on the best practices for designing health interventions in refugee contexts (Abuhaloob et al., Citation2018; Palic & Elklit, Citation2011; Purgato et al., Citation2018; Thompson et al., Citation2018; Williams & Thompson, Citation2011). In a humanitarian setting in which resources are scarce and the sociopolitical situation is complex, it is essential to carefully consider the feasibility, impact, and acceptability of a proposed intervention before implementing it. A broad network of stakeholders, especially the future program participants, must be included in the planning process to ensure it is tailored to the context. IM provides a structured approach for including numerous stakeholders in designing a rigorous, evidence-based health intervention.
We used IM to design a program aimed at enhancing linkage to HIV care in Nakivale Refugee Settlement, Uganda. In an intensive workshop, a cross-disciplinary working group designed a program of “C-3 teams” to provide community-based, integrated health care to people with HIV, hypertension, and diabetes. This program would enhance engagement in HIV care by improving access, reducing stigma, and enhancing social support for participants.
We identified several lessons in applying IM methodology to the refugee context. First, it is crucial to incorporate the firsthand experience of numerous stakeholders in developing an intervention for this setting because the published evidence about refugee populations is relatively sparse. Second, given that there are numerous partner organizations and multiple levels of permissions involved in health care implementation in refugee settlements (in Nakivale, Medical Teams International, UNHCR, the Ministry of Health, and others), it is critical to actively seek participation and buy-in from these organizations in order to successfully implement an intervention. Third, in the refugee setting there can be rapid turnover in staff and leadership, which introduces challenges when planning and implementing long-term projects with local partners.
Another challenge of planning an intervention for HIV care in a refugee setting is the frequent change in guidelines and policies. For example, when data collection on HIV testing in Nakivale began in 2013 (O’Laughlin et al., Citation2014), the standard of care for HIV management was to base ART eligibility on physical exam findings and CD4 count. In 2016, the guidelines changed to a test-and-treat strategy, initiating all people with HIV on ART regardless of CD4 count. It is not known whether this change in treatment guidelines affected linkage to HIV care in Nakivale (O’Laughlin et al., Citation2017).
Though the IM method fosters participation from diverse stakeholders, specific efforts may be needed to promote inclusivity. In our workshop, participants had different cultural backgrounds, ages, occupations, and fluency in English (which was the working group’s common language). To create a collaborative environment, we explicitly discussed the perspective and strengths of each participant. For example, one participant was a Congolese pastor who had limited English fluency compared to other participants, but was empowered to participate because the group recognized his valuable contributions as a religious provider and community leader.
Our study is limited by the absence of two notable perspectives from the working group: Ugandan nationals living in Nakivale, and Somali refugees. In Nakivale, as in other humanitarian settings, there is a complex landscape of power and vulnerability (Bjørkhaug, Citation2020). The Ugandan participants in the IM workshop worked for humanitarian and government organizations; they were in positions of relative power in the settlement. Conversely, the Ugandans who live in Nakivale are vulnerable to eviction from their land, yet also benefit from the health and education services provided for refugees, thus facing complex challenges and motivations. Additionally, Somali refugees tend to be more economically prosperous than other groups and conflicts can arise between those communities (Bjørkhaug, Citation2020). Prior to implementation of the proposed intervention, feedback from these groups should be obtained.
Of note, there are many refugees living in Kampala, Uganda’s capital. The refugee population living in urban settings is distinct from those in the settlements: though they may have access to more employment opportunities, they do not have access to the services offered for refugees, and if they do not return periodically to the settlements for “verification” of their refugee status and residence in Uganda, they may lose their benefits altogether. Additionally, rates of transactional sex are high for refugees living in Kampala (Logie et al., Citation2020). It is not known whether refugees living in urban areas face the same barriers in linkage to HIV care as those living in the refugee settlements.
Intervention Mapping is an inclusive, efficient approach to intervention design that can be applied in the time- and resource-limited conditions of the humanitarian setting. In Nakivale Refugee Settlement, this method allowed stakeholders and community members to design a feasible intervention to promote linkage to HIV care based on a detailed discussion of the causes and consequences of untreated HIV.
Acknowledgements
The authors acknowledge the contributions of the working group who participated in the Intervention Mapping workshop in Nakivale, and to the following individuals who provided feedback on the proposed intervention: Masereka Simon, Ndariho Jackson, Namakula Priscilla, Kaddu Elinah, Neema Alphonsine, Kansiime Henry, and Ekolu Abraham. We thank the Medical Teams International (MTI) health clinic staff in Nakivale Refugee Settlement and the MTI leadership in Uganda for making this work possible. We thank our collaborators from the United Nations High Commissioner for Refugees (UNHCR), and the members of the Refugee Desk Office and the Office of the Prime Minister of Uganda for their support.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abuhaloob, L., Carson, S., Richards, D., & Freeman, R. (2018). Community-based nutrition intervention to promote oral health and restore healthy body weight in refugee children: A scoping review. Community Dental Health, 35(2), 81–88. https://doi.org/10.1922/CDH_4188Abuhaloob08
- Bartholomew Eldredge, L. K., Markham, C. M., Ruiter, R. A., Fernandez, M. E., Kok, G., & Parcel, G. S. (2016). Planning health promotion programs: An Intervention Mapping approach (4th ed.). Jossey-Bass & Pfeiffer Imprints, Wiley.
- Bartholomew, L. K., Parcel, G. S., & Kok, G. (1998). Intervention Mapping: A process for developing theory and evidence-based health education programs. Health Education & Behavior, 25(5), 545–563. https://doi.org/10.1177/109019819802500502
- Bateman, C. (2013). MSF again paves the way with ART. South African Medical Journal, 103(2), 71. https://doi.org/10.7196/SAMJ.6666
- Billioux, V. G., Chang, L. W., Reynolds, S. J., Nakigozi, G., Ssekasanvu, J., Grabowski, M. K., Ssekubugu, R., Nalugoda, F., Kigozi, G., Kagaayi, J., Serwadda, D., Gray, R. H., Wawer, M. J., & the Rakai Health Sciences Program (2017). Human immunodeficiency virus care cascade among sub-populations in Rakai, Uganda: An observational study. Journal of the International AIDS Society, 20(1), 21590. https://doi.org/10.7448/IAS.20.1.21590
- Bjørkhaug, I. (2020). Revisiting the refugee–host relationship in Nakivale Refugee Settlement: A dialogue with the Oxford Refugee Studies Centre. Journal on Migration and Human Security, 8(3), 266–281. https://doi.org/10.1177/2331502420948465
- Bock, P., Gunst, C., Maschilla, L., Holtman, R., Grobbelaar, N., Wademan, D., Dunbar, R., Fatti, G., Kruger, J., Ford, N., Hoddinott, G., & Meehan, S. (2019). Retention in care and factors critical for effectively implementing antiretroviral adherence clubs in a rural district in South Africa. Journal of the International AIDS Society, 22(10). https://doi.org/10.1002/jia2.25396
- Corbie-Smith, G., Akers, A., Blumenthal, C., Council, B., Wynn, M., Muhammad, M., & Stith, D. (2010). Intervention Mapping as a participatory approach to developing an HIV prevention intervention in rural African American communities. AIDS Education and Prevention, 22(3), 184–202. https://doi.org/10.1521/aeap.2010.22.3.184
- Côté, J., Godin, G., Garcia, P. R., Gagnon, M., & Rouleau, G. (2008). Program development for enhancing adherence to antiretroviral therapy among persons living with HIV. AIDS Patient Care and STDs, 22(12), 965–975. https://doi.org/10.1089/apc.2008.0124
- Garba, R. M., & Gadanya, M. A. (2017). The role of Intervention Mapping in designing disease prevention interventions: A systematic review of the literature. PLOS ONE, 12(3), e0174438. https://doi.org/10.1371/journal.pone.0174438
- Gardner, E. M., McLees, M. P., Steiner, J. F., del Rio, C., & Burman, W. J. (2011). The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clinical Infectious Diseases, 52(6), 793–800. https://doi.org/10.1093/cid/ciq243
- Garrib, A., Birungi, J., Lesikari, S., Namakoola, I., Njim, T., Cuevas, L., Niessen, L., Mugisha, K., Mutungi, G., Mghamba, J., Ramaiya, K., Jaffar, S., Mfinanga, S., & Nyirenda, M. (2018). Integrated care for human immunodeficiency virus, diabetes and hypertension in Africa. Transactions of The Royal Society of Tropical Medicine and Hygiene. https://doi.org/10.1093/trstmh/try098
- Green, L. W., Kreuter, M. W., & Green, L. W. (2005). Health program planning: An educational and ecological approach (4th ed.). McGraw-Hill.
- Grimsrud, A., Lesosky, M., Kalombo, C., Bekker, L.-G., & Myer, L. (2016). Implementation and operational research: Community-based adherence clubs for the management of stable antiretroviral therapy patients in Cape Town, South Africa. Journal of Acquired Immune Deficiency Syndromes, 71(1), e16–e23. https://doi.org/10.1097/QAI.0000000000000863
- Haldane, V., Legido-Quigley, H., Chuah, F. L. H., Sigfrid, L., Murphy, G., Ong, S. E., Cervero-Liceras, F., Watt, N., Balabanova, D., Hogarth, S., Maimaris, W., Buse, K., McKee, M., Piot, P., & Perel, P. (2018). Integrating cardiovascular diseases, hypertension, and diabetes with HIV services: A systematic review. AIDS Care, 30(1), 103–115. https://doi.org/10.1080/09540121.2017.1344350
- Hanrahan, C. F., Schwartz, S. R., Mudavanhu, M., West, N. S., Mutunga, L., Keyser, V., Bassett, J., & Van Rie, A. (2019). The impact of community- versus clinic-based adherence clubs on loss from care and viral suppression for antiretroviral therapy patients: Findings from a pragmatic randomized controlled trial in South Africa. PLOS Medicine, 16(5), e1002808. https://doi.org/10.1371/journal.pmed.1002808
- IASC Task Force on HIV/AIDS in Emergency Settings. (2003). Guidelines for HIV/AIDS interventions in emergency settings. Inter-Agency Standing Committee. https://www.refworld.org/docid/3d94756a2.html
- Jain, K., Mshweshwe-Pakela, N. T., Charalambous, S., Mabuto, T., & Hoffmann, C. J. (2021). Enhancing value and lowering costs of care: A qualitative exploration of a randomized linkage to care intervention in South Africa. AIDS Care, 31(4), 481–488. https://doi.org/10.1080/09540121.2018.1503636
- Kirby, D. (2001). Emerging answers: Research findings on programs to reduce teen pregnancy. ERIC Clearinghouse.
- Logie, C. H., Okumu, M., Mwima, S., Hakiza, R., Abela, H., & Kyambadde, P. (2020). Gender, transactional sex, and HIV prevention cascade engagement among urban refugee and displaced adolescents and youth in Kampala, Uganda. AIDS Care, 1–7. https://doi.org/10.1080/09540121.2020.1861181
- Luque-Fernandez, M. A., Van Cutsem, G., Goemaere, E., Hilderbrand, K., Schomaker, M., Mantangana, N., Mathee, S., Dubula, V., Ford, N., Hernán, M. A., & Boulle, A. (2013). Effectiveness of patient adherence groups as a model of care for stable patients on antiretroviral therapy in Khayelitsha, Cape Town, South Africa. PLoS ONE, 8(2), e56088. https://doi.org/10.1371/journal.pone.0056088
- Mkumbo, K., Schaalma, H., Kaaya, S., Leerlooijer, J., Mbwambo, J., & Kilonzo, G. (2009). The application of Intervention Mapping in developing and implementing school-based sexuality and HIV/AIDS education in a developing country context: The case of Tanzania. Scandinavian Journal of Public Health, 37(2_suppl), 28–36. https://doi.org/10.1177/1403494808091345
- Mukumbang, F. C., van Wyk, B., Van Belle, S., & Marchal, B. (2019). “At this [adherence] club, we are a family now”: A realist theory-testing case study of the antiretroviral treatment adherence club, South Africa. Southern African Journal of HIV Medicine, 20(1). https://doi.org/10.4102/sajhivmed.v20i1.922
- O’Laughlin, K., Kasozi, J., Rabideau, D., Parker, R., Mulogo, E., Faustin, Z., Greenwald, K., Doraiswamy, S., Walensky, R., & Bassett, I. (2017). The cascade of HIV care among refugees and nationals in Nakivale Refugee Settlement in Uganda. HIV Medicine, 18(7), 513–518. https://doi.org/10.1111/hiv.12476
- O’Laughlin, K. N., Kasozi, J., Walensky, R. P., Parker, R. A., Faustin, Z. M., Doraiswamy, S., Owino, C. O., & Bassett, I. V. (2014). Clinic-based routine voluntary HIV testing in a refugee settlement in Uganda. Journal of Acquired Immune Deficiency Syndromes, 67(4), 409–413. https://doi.org/10.1097/QAI.0000000000000317
- O’Laughlin, K. N., Rabideau, D. J., Kasozi, J., Parker, R. A., Bustamante, N. D., Faustin, Z. M., Greenwald, K. E., Walensky, R. P., & Bassett, I. V. (2016). Predictors of HIV infection: A prospective HIV screening study in a Ugandan refugee settlement. BMC Infectious Diseases, 16(1). https://doi.org/10.1186/s12879-016-2021-1
- O’Laughlin, K. N., Rouhani, S. A., Faustin, Z. M., & Ware, N. C. (2013). Testing experiences of HIV positive refugees in Nakivale Refugee Settlement in Uganda: Informing interventions to encourage priority shifting. Conflict and Health, 7(1), 2. https://doi.org/10.1186/1752-1505-7-2
- O’Laughlin, K. N., Rouhani, S. A., Kasozi, J., Greenwald, K. E., Perkons, N. R., Faustin, Z. M., Bassett, I. V., & Ware, N. C. (2018). A qualitative approach to understand antiretroviral therapy (ART) adherence for refugees living in Nakivale Refugee Settlement in Uganda. Conflict and Health, 12(1). https://doi.org/10.1186/s13031-018-0145-1
- Palic, S., & Elklit, A. (2011). Psychosocial treatment of posttraumatic stress disorder in adult refugees: A systematic review of prospective treatment outcome studies and a critique. Journal of Affective Disorders, 131(1–3), 8–23. https://doi.org/10.1016/j.jad.2010.07.005
- Pell, C., Reis, R., Dlamini, N., Moyer, E., & Vernooij, E. (2019). “Then her neighbour will not know her status”: How health providers advocate antiretroviral therapy under universal test and treat. International Health, 11(1), 36–41. https://doi.org/10.1093/inthealth/ihy058
- Purgato, M., Gross, A. L., Betancourt, T., Bolton, P., Bonetto, C., Gastaldon, C., Gordon, J., O’Callaghan, P., Papola, D., Peltonen, K., Punamaki, R.-L., Richards, J., Staples, J. K., Unterhitzenberger, J., van Ommeren, M., de Jong, J., Jordans, M. J. D., Tol, W. A., & Barbui, C. (2018). Focused psychosocial interventions for children in low-resource humanitarian settings: A systematic review and individual participant data meta-analysis. The Lancet Global Health, 6(4), e390–e400. https://doi.org/10.1016/S2214-109X(18)30046-9
- Rentsch, C. T., Wringe, A., Machemba, R., Michael, D., Urassa, M., Todd, J., Reniers, G., & Zaba, B. (2018). Linkage to care and antiretroviral therapy initiation by testing modality among individuals newly diagnosed with HIV in Tanzania, 2014-2017. Tropical Medicine & International Health, 23(12), 1384–1393. https://doi.org/10.1111/tmi.13153
- Sabapathy, K., Hensen, B., Varsaneux, O., Floyd, S., Fidler, S., & Hayes, R. (2018). The cascade of care following community-based detection of HIV in sub-Saharan Africa: A systematic review with 90-90-90 targets in sight. PLOS ONE, 13(7), e0200737. https://doi.org/10.1371/journal.pone.0200737
- Sanga, E. S., Mukumbang, F. C., Mushi, A. K., Olomi, W., Lerebo, W., & Zarowsky, C. (2018). Processes and dynamics of linkage to care from mobile/outreach and facility-based HIV testing models in hard-to-reach settings in rural Tanzania. Qualitative findings of a mixed methods study. AIDS Research and Therapy, 15(1). https://doi.org/10.1186/s12981-018-0209-8
- Seeley, J., Bond, V., Yang, B., Floyd, S., MacLeod, D., Viljoen, L., Phiri, M., Simuyaba, M., Hoddinott, G., Shanaube, K., Bwalya, C., de Villiers, L., Jennings, K., Mwanza, M., Schaap, A., Dunbar, R., Sabapathy, K., Ayles, H., Bock, P., … Fidler, S. (2018). Understanding the time needed to link to care and start ART in seven HPTN 071 (PopART) study communities in Zambia and South Africa. AIDS and Behavior. https://doi.org/10.1007/s10461-018-2335-7
- Sharma, M., Ying, R., Tarr, G., & Barnabas, R. (2015). Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature, 528(7580), S77–S85. https://doi.org/10.1038/nature16044
- Sharp, J., Wilkinson, L., Cox, V., Cragg, C., van Cutsem, G., & Grimsrud, A. (2019). Outcomes of patients enrolled in an antiretroviral adherence club with recent viral suppression after experiencing elevated viral loads. Southern African Journal of HIV Medicine, 20(1). https://doi.org/10.4102/sajhivmed.v20i1.905
- Thompson, C. T., Vidgen, A., & Roberts, N. P. (2018). Psychological interventions for post-traumatic stress disorder in refugees and asylum seekers: A systematic review and meta-analysis. Clinical Psychology Review, 63, 66–79. https://doi.org/10.1016/j.cpr.2018.06.006
- Tsondai, P. R., Wilkinson, L. S., Grimsrud, A., Mdlalo, P. T., Ullauri, A., & Boulle, A. (2017). High rates of retention and viral suppression in the scale-up of antiretroviral therapy adherence clubs in Cape Town, South Africa. Journal of the International AIDS Society, 20, 21649. https://doi.org/10.7448/IAS.20.5.21649
- Uganda AIDS Commission. (2017). Uganda HIV/AIDS country progress report July 2016 to June 2017. http://www.unaids.org/sites/default/files/country/documents/UGA_2018_countryreport.pdf
- UN Food and Agriculture Organization. (2010). Gender-based violence and livelihood interventions: Focus on populations of humanitarian concern in the context of HIV. https://www.refworld.org/docid/58bd54964.html
- UNAIDS Programme Coordinating Board. (2020). Annotated Outline of the Global AIDS Strategy 2021-2026. UNAIDS. https://www.unaids.org/sites/default/files/PCB47__Annotated_Outline_Strategy_EN.pdf
- UNHCR. (2002). Evaluation of humanitarian assistance in emergency situations. https://www.refworld.org/docid/4ff54d962.html
- UNHCR. (2017). UNHCR Global Report. http://reporting.unhcr.org/sites/default/files/gr2017/pdf/GR2017_English_Full_lowres.pdf
- UNHCR. (2019, May). Uganda refugee response monitoring: Settlement fact sheet Nakivale. UNHCR operational portal refugee situations. https://data2.unhcr.org/en/documents/download/63282
- UNHCR. (2020, June). UNHCR figures at a glance. https://www.unhcr.org/en-us/figures-at-a-glance.html
- Watt, N., Sigfrid, L., Legido-Quigley, H., Hogarth, S., Maimaris, W., Otero-García, L., Perel, P., Buse, K., McKee, M., Piot, P., & Balabanova, D. (2017). Health systems facilitators and barriers to the integration of HIV and chronic disease services: A systematic review. Health Policy and Planning, 32(suppl_4), iv13–iv26. https://doi.org/10.1093/heapol/czw149
- Wilkinson, L. S. (2013). ART adherence clubs: A long-term retention strategy for clinically stable patients receiving antiretroviral therapy. Southern African Journal of HIV Medicine, 14(2), 48–50. https://doi.org/10.4102/sajhivmed.v14i2.77
- Williams, M. E., & Thompson, S. C. (2011). The use of community-based interventions in reducing morbidity from the psychological impact of conflict-related trauma among refugee populations: A systematic review of the literature. Journal of Immigrant and Minority Health, 13(4), 780–794. https://doi.org/10.1007/s10903-010-9417-6
- Wirtz, A. L., Glass, N., Pham, K., Aberra, A., Rubenstein, L. S., Singh, S., & Vu, A. (2013). Development of a screening tool to identify female survivors of gender-based violence in a humanitarian setting: Qualitative evidence from research among refugees in Ethiopia. Conflict and Health, 7(1), 13. https://doi.org/10.1186/1752-1505-7-13
- Wolfers, M. E., van den Hoek, C., Brug, J., & de Zwart, O. (2007). Using Intervention Mapping to develop a programme to prevent sexually transmittable infections, including HIV, among heterosexual migrant men. BMC Public Health, 7(1). https://doi.org/10.1186/1471-2458-7-141
