
ABSTRACT
Objective:
Determine the feasibility, acceptability, and preliminary effectiveness of financial incentives to motivate re-engagement in HIV care in Shinyanga, Tanzania.
Methods:
Out-of-care people living with HIV (PLHIV) were identified from medical records in four clinics and home-based care providers (HBCs) from April 13, 2018 to March 3, 2020. Shinyanga Region residents, ≥18 years, who were disengaged from care were randomized 1:1 to a financial incentive (∼$10 USD) or the standard of care (SOC), stratified by site, and followed for 180 days. Primary outcomes were feasibility (located PLHIV who agreed to discuss the study), acceptability (enrollment among eligibles), and re-engagement in care (clinic visit within 90 days).
Results:
HBCs located 469/1,309 (35.8%) out-of-care PLHIV. Of these, 215 (45.8%) were preliminarily determined to be disengaged from care, 201 (93.5%) agreed to discuss the study, and 157 eligible (100%) enrolled. Within 90 days, 71 (85.5%) PLHIV in the incentive arm re-engaged in care vs. 58 (78.4%) in the SOC (Adjusted Risk Difference [ARD] = 0.08, 95% CI: −0.03, 0.19, p = 0.09). A higher proportion of incentivized PLHIV completed an additional (unincentivized) visit between 90–180 days (79.5% vs. 71.6%, ARD = 0.10, 95% CI: −0.03, 0.24, p = 0.13) and remained in care at 180 days (57.8% vs. 51.4%, ARD = 0.07, 95% CI: −0.09, 0.22, p = 0.40).
Conclusions:
Short-term financial incentives are feasible, acceptable, and have the potential to encourage re-engagement in care, warranting further study of this approach.
KEYWORDS:
Introduction
Adherence to antiretroviral therapy (ART) and retention in care are critical to achieving viral suppression and the UNAIDS 95-95-95 goals (World Health Organization, Citation2003). Although ART access has dramatically increased in the treatment as prevention (TasP) era, suboptimal adherence continues to impede progress (Joint United Nations Programme on HIV/AIDS, Citation2019; Kalinjuma et al., Citation2020; UNAIDS, Citation2020); only 58% of people living with HIV (PLHIV) in eastern and southern Africa are virally suppressed (Joint United Nations Programme on HIV/AIDS, Citation2019), and a large study in sub-Saharan Africa demonstrated that more than one-third of PLHIV were not retained in care five years after ART initiation (Kelly et al., Citation2019). Despite these challenges, few studies have focused on retention in the TasP era, particularly among PLHIV who disengaged from care (Kelly et al., Citation2019).
Disengagement from care is a complex process which likely begins with competing daily demands that result in missed clinic visits and evolves into a reluctance to return to the clinic and a weakened sense of connectedness to care (Ware et al., Citation2013). Theories from psychology and economics indicate that financial incentives have the potential to overcome this reluctance and motivate engagement in care (Loewenstein et al., Citation2007; Tversky & Kahneman, Citation1974) and have demonstrated efficacy for other HIV outcomes including adherence and viral suppression (El-Sadr et al., Citation2017; Galárraga & Sosa-Rubí, Citation2019; Yotebieng et al., Citation2016). Building on this theoretical and empirical foundation, the objective of our pilot study was to determine the feasibility, acceptability, and preliminary effectiveness of combining standard tracing procedures with a financial incentive to motivate re-engagement in HIV care.
Methods
Trial design and ethics
We conducted a 2-arm parallel randomized controlled trial in Shinyanga, Tanzania. Participants were enrolled from April 13, 2018 to March 3, 2020 (with follow-up through August 30, 2020). Ethical approval was obtained by the Committee for Protection of Human Subjects at the University of California, Berkeley and the Tanzanian National Institute for Medical Research. Written informed consent was obtained from all study participants. Participants who were unable to sign their name could provide a thumbprint/mark on the consent form. The trial was pre-registered (clinicaltrials.gov: NCT03454373) and is presented using the CONSORT guidelines (Schulz et al., Citation2010).
Participants
Lists of all lost-to-follow-up PLHIV from medical records at four clinics (two hospitals, one clinic, and one dispensary) and home-based care providers (HBCs) serving clinic catchment areas were used to identify out-of-care PLHIV who were previously in care. Potential participants were traced by HBCs following recommended procedures from the President’s Emergency Plan for AIDS Relief (PEPFAR) and the Ministry of Health to ensure that the intervention could seamlessly and sustainably integrate into real-world government procedures. After ascertaining care status, HBCs recruited PLHIV who were: (1) residing within Shinyanga Region; (2) aged 18 years or older; and (3) disengaged from care, defined as not attending a clinic appointment for ≥ 28 days since their last scheduled appointment, consistent with 2019 PEPFAR definitions (PEPFAR, Citation2019).
Randomization and masking
Participants were individually randomized in a 1:1 ratio, stratified by site, to the intervention or standard of care (SOC) after providing consent. Randomization was initially conducted using Qualtrics (Qualtrics, Citation2020); however, unequal random allocation was detected midway through enrollment due to a technical issue. An improved process was implemented to randomize participants using permuted block sizes of 2 and 4. The code was developed and executed at the University of California, Berkeley using Stata version 15.1 (StataCorp, Citation2017). Randomization assignments were disclosed to research assistants after consent.
Procedures
Participants in the SOC arm received standard services according to Tanzania’s National Guidelines for the Management of HIV (Ministry of Health and Social Welfare, Citation2009; National AIDS Control Programme, Citation2017), including in-person home-based counseling from HBCs to return to care and the offer to schedule an HIV care visit. Participants in the incentive arm received standard services plus 22,500 TZS (∼$10 USD), delivered through digital mobile money services or in cash when participants did not have a mobile phone or a mobile money account. Half of the incentive was provided at enrollment (unconditional upon clinic attendance) and half was provided after a completed clinic visit within 90 days (conditional upon clinic attendance, confirmed by medical record review). Partial payment was provided upfront to mitigate economic barriers including transport costs, as evidence has shown that poor adherence is associated with poverty, stigma, and a lack of motivation (Bukenya et al., Citation2019; Geng et al., Citation2016; Roura et al., Citation2009; Young et al., Citation2014). The incentive amount, selected in collaboration with local stakeholders, the Ministry of Health, and clinic staff, was determined to be sufficient for multiple roundtrip clinic visits and small enough to avoid undue coercion.
In-person surveys were conducted in Kiswahili at baseline to assess individual and household characteristics, including food security (from the Household Food Insecurity Access Scale (Coates et al., Citation2007), work status (adapted from the Demographic and Health Survey (Ministry of Health, Community Development, Gender, Citation2016), and reasons for disengagement from care. At 90 days, phone surveys were conducted to assess clinic attendance, experiences re-engaging in care, and motivation for re-engagement. Medical record reviews were conducted at 90 and 180 days to verify scheduled and attended visits at the clinic(s).
Outcomes
The pre-registered (Wharton University of Pennsylvania Credibility Lab, Citationn.d.) primary outcomes were: (1) feasibility, including (i) the proportion of potentially out-of-care PLHIV who were successfully located and (ii) the proportion of located, potentially out-of-care PLHIV who agreed to discuss the study; (2) acceptability, defined as the proportion of located, potentially out-of-care PLHIV who were eligible and agreed to participate; and (3) initial re-engagement in care, defined as the proportion of participants with a documented HIV care visit within 90 days of enrollment. Preliminary re-engagement status was determined from the phone survey and verified with medical records. Secondary outcomes (not pre-registered) included the proportion of PLHIV who completed a documented, unincentivized visit after receiving the second half of the incentive (between 90–180 days) and the proportion of PLHIV in care at 180 days, defined as <28 days since their last scheduled visit. Among participants who re-engaged in care by 90 days, we report the most common reasons listed for re-engagement.
Sample size and statistical analysis
The sample size was informed by our team’s previous study (unpublished) in Shinyanga where 45% of out-of-care PLHIV initiated care within 90 days of HBC interaction. We estimated that enrolling 144 PLHIV (72 per arm) provided 80% power to detect at least a 23-percentage point difference in engagement between treatment arms (alpha = 0.05).
Descriptive statistics were used to assess balance of participant characteristics by treatment arm at baseline and the outcomes of acceptability and feasibility. Re-engagement in care at 90 days, engagement between 90–180 days, and retention at 180 days were estimated with an intent-to-treat analysis (ITT). Risk differences (RD) with 95% CIs were calculated using generalized linear models with a binomial distribution and identity link. Pre-registered adjusted models controlled for factors imbalanced at baseline. Statistical analyses were conducted using R version 4.0.2 (R Core Team, Citation2020).
Results
In total, 469 (36%) PLHIV were located by HBCs, of which 215 (45%) were preliminarily determined to be out of care and 201 (93%) agreed to discuss the study. After screening for eligibility, 157 consented (100% of eligibles) (). Participants were followed for 180 days, with follow-up concluding in August 2020.
Figure 1. Study profile. Study population for analysis of primary outcomes.
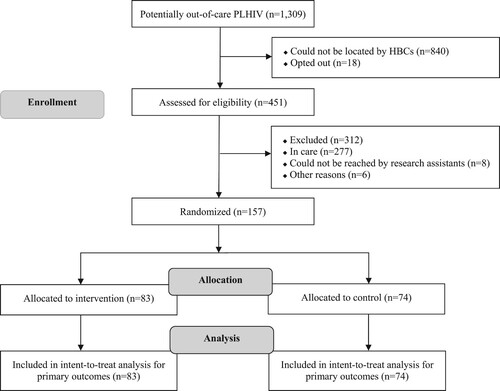
At baseline, 101 (64%) of participants were female, 100 (64%) completed primary school, and 123 (78%) were working. The mean age was 38 years (). Sex, severe food insecurity, educational status, language, and site were imbalanced and included in adjusted models ().
Table 1. Socio-demographic characteristics of study participants at baseline.
Table 2. Summary of the effects of financial incentives on re-engagement in care within 3 months, engagement between 3–6 months, and retention in care at 6 months.
In the unadjusted analysis, there was no statistical difference in re-engagement between study arms (). The incentive arm had a non-significantly higher proportion of PLHIV with a clinic visit at 90 days compared to the SOC (85.5% vs. 78.4%, RD = 0.07, 95% CI: −0.05, 0.19, p = 0.24, ). The incentive arm also had a non-significantly higher proportion who completed an additional visit between 90–180 days, after the incentive period (79.5% vs. 71.6%, RD = 0.08, 95% CI: −0.05, 0.21, p = 0.24), and higher retention at 180 days (57.8%, vs. 51.4%, RD = 0.06, CI: −0.09, 0.22, p = 0.43). Adjusted models showed larger estimates after accounting for baseline imbalances; however, these results remained non-significant ().
At 90 days, participants who re-engaged in care were asked about the main factors that influenced their decision. Among the 144 participants reached (91.7%), 33.0% reported wanting to improve their health/feeling in poor health and 25.1% reported having more time to attend the clinic. Some indicated that encouragement from research staff and nurses was a motivating factor (5.6%). Participants in the incentive arm also highlighted receiving money from the study (12.7%) as a primary reason for seeking care.
Discussion
This pilot study reveals that incorporating small incentives into routine tracing procedures is feasible and acceptable for out-of-care PLHIV who were previously in care. While non-significant at the 5% level, the point estimates and range of possible effect sizes provide preliminary signal that financial incentives may have the potential to motivate re-engagement among out-of-care PLHIV. Retention in care waned across both groups by 180 days; however, the intervention group remained in care after the incentive period at higher levels than the SOC, suggesting that motivation continues after incentives end, as has been found in other studies (McCoy et al., Citation2017). These results build on previous studies demonstrating that incentives can bolster linkage to HIV care (Linnemayr et al., Citation2017; McNairy et al., Citation2017; Solomon et al., Citation2014); however, until now, no studies have focused on incentives for out-of-care PLHIV.
Notably, re-engagement and retention were also high in the SOC arm, with more than 75% returning to care within 90 days. This finding may be related to engagement with supportive personnel throughout the study period, as encouragement from the research team and nurses was identified by participants in both arms as a factor for seeking care. Similar effects were found in a study among adolescent PLHIV in South Africa, where improved retention was associated with kind and supportive clinic staff (Cluver et al., Citation2018). In our study, however, it is impossible to disentangle the effects of HBCs from research staff, warranting future research to understand the effectiveness and cost-effectiveness of home visits alone on re-engagement.
This study has several strengths. This was the first study to target out-of-care PLHIV, a group critical to reducing onward transmission, to assess whether incentives are feasible, acceptable, and influence re-engagement in care. Second, the two-installment incentive was designed to mitigate widely established structural barriers and to increase motivation to seek care. Third, we used rigorous Ministry-recommended procedures in collaboration with HBCs, a key part of the Tanzanian HIV workforce, to locate out-of-care PLHIV, trace participants who were unreachable for phone surveys, and verify self-reported outcomes with medical records. Only a small percentage of potentially out-of-care PLHIV were located through tracing procedures, and not all of those who were located were out of care. This suggests that medical records are often out-of-date and include inaccurate contact information and care statuses, highlighting the challenges of identifying disengaged PLHIV.
This study also has limitations. We were insufficiently powered to detect small differences between groups, as our intent was to pilot the intervention in preparation for a larger study. In the future, a larger effectiveness trial based on this pilot will provide sufficient power to detect small effect sizes. Subsequent studies could also consider increasing the magnitude or duration of the incentive to bolster the effect size, which has been successful in other contexts (Silverman et al., Citation2019). However, increasing incentive size and duration has important tradeoffs with sustainability and scalability. Our study sample also only included individuals who were known to be out of care from HBCs and clinic records. The full care history of each participant was not recorded at enrollment; therefore, it is uncertain whether the intervention had differential effects for individuals who were disengaged from care for longer periods. Additionally, the pre-specified definition of acceptability may have partially conflated acceptability and participation since individuals may have chosen to participate for reasons other than acceptability (e.g., need for financial support). However, the amount of the cash transfer was specifically designed to avoid coercion. Lastly, generalizability is limited as the most marginalized and disenfranchized PLHIV were likely not located by HBCs and included in our study.
Overall, the findings from our study indicate that short-term financial incentives are feasible, acceptable, and have the potential to modestly encourage out-of-care PLHIV to re-engage in care. Although these findings were measured with significant uncertainty, our results suggest that research among a larger sample is warranted to further examine the effectiveness of this approach.
Word count: 2,108.
Acknowledgements
The authors would like to acknowledge and thank the local research team at Health for a Prosperous Nation, the home-based care providers, and study participants.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bukenya, D., Mayanja, B. N., Nakamanya, S., Muhumuza, R., & Seeley, J. (2019). What causes non-adherence among some individuals on long term antiretroviral therapy? Experiences of individuals with poor viral suppression in Uganda. AIDS Research and Therapy, 16(1), 2. doi:10.1186/s12981-018-0214-y
- Cluver, L., Pantelic, M., Toska, E., Orkin, M., Casale, M., Bungane, N., & Sherr, L. (2018). Stacking the odds for adolescent survival: health service factors associated with full retention in care and adherence amongst adolescents living with HIV in South Africa. Journal of the International AIDS Society, 21(9), e25176–e25176. doi:10.1002/jia2.25176
- Coates, J., Swindale, A., & Bilinsky, P. (2007). Household Food Insecurity Access Scale (HFIAS) for measurement of food access: indicator guide. Version, 3, 29. https://www.fantaproject.org/sites/default/files/resources/HFIAS_ENG_v3_Aug07.pdf
- El-Sadr, W. M., Donnell, D., Beauchamp, G., Hall, H. I., Torian, L. V., Zingman, B., Lum, G., Kharfen, M., Elion, R., Leider, J., Gordin, F. M., Elharrar, V., Burns, D., Zerbe, A., Gamble, T., & Branson, B. (2017). Financial incentives for linkage to care and viral suppression among HIV-positive patients: A randomized clinical trial (HPTN 065). JAMA Internal Medicine, 177(8), 1083–1092. doi:10.1001/jamainternmed.2017.2158
- Galárraga, O., & Sosa-Rubí, S. G. (2019). Conditional economic incentives to improve HIV prevention and treatment in low-income and middle-income countries. The Lancet HIV, 6(10), e705–e714. doi:10.1016/S2352-3018(19)30233-4
- Geng, E. H., Odeny, T. A., Lyamuya, R., Nakiwogga-Muwanga, A., Diero, L., Bwana, M., Braitstein, P., Somi, G., Kambugu, A., Bukusi, E., Wenger, M., Neilands, T. B., Glidden, D. V., Wools-Kaloustian, K., Yiannoutsos, C., & Martin, J. (2016). Retention in care and patient-reported reasons for undocumented transfer or stopping care among HIV-infected patients on antiretroviral therapy in Eastern Africa: Application of a sampling-based approach. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 62(7), 935–944. doi:10.1093/cid/civ1004
- Joint United Nations Programme on HIV/AIDS. (2019). UNAIDS Data 2019. https://www.unaids.org/sites/default/files/media_asset/2019-UNAIDS-data_en.pdf
- Kalinjuma, A. V., Glass, T. R., Weisser, M., Myeya, S. J., Kasuga, B., Kisung’a, Y., Sikalengo, G., Katende, A., Battegay, M., Vanobberghen, F., & Group, K. S. (2020). Prospective assessment of loss to follow-up: incidence and associated factors in a cohort of HIV-positive adults in rural Tanzania. Journal of the International AIDS Society, 23(3), e25460–e25460. doi:10.1002/jia2.25460
- Kelly, N., Maokola, W., Mudasiru, O., & McCoy, S. I. (2019). Interventions to improve linkage to HIV care in the era of “treat all” in sub-saharan africa: A systematic review. Current HIV/AIDS Reports, 16(4), 292–303. doi:10.1007/s11904-019-00451-8
- Linnemayr, S., Stecher, C., & Mukasa, B. (2017). Behavioral economic incentives to improve adherence to antiretroviral medication. AIDS (London, England), 31(5), 719–726. doi:10.1097/QAD.0000000000001387
- Loewenstein, G., Brennan, T., & Volpp, K. G. (2007). Asymmetric paternalism to improve health behaviors. JAMA, 298(20), 2415–2417. doi:10.1001/jama.298.20.2415
- McCoy, S. I., Njau, P. F., Fahey, C., Kapologwe, N., Kadiyala, S., Jewell, N. P., Dow, W. H., & Padian, N. S. (2017). Cash vs. food assistance to improve adherence to antiretroviral therapy among HIV-infected adults in Tanzania. AIDS (London, England), 31(6), 815–825. doi:10.1097/QAD.0000000000001406
- McNairy, M. L., Lamb, M. R., Gachuhi, A. B., Nuwagaba-Biribonwoha, H., Burke, S., Mazibuko, S., Okello, V., Ehrenkranz, P., Sahabo, R., & El-Sadr, W. M. (2017). Effectiveness of a combination strategy for linkage and retention in adult HIV care in Swaziland: The Link4Health cluster randomized trial. PLOS Medicine, 14(11), e1002420. doi:10.1371/journal.pmed.1002420
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), & ICF. (2016). Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16.
- President’s Emergency Plan for AIDS Relief (PEPFAR). (2019). Monitoring, evaluation, and reporting indicator reference guide.
- Qualtrics. (2020).
- R Core Team. (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing.
- Roura, M., Busza, J., Wringe, A., Mbata, D., Urassa, M., & Zaba, B. (2009). Barriers to sustaining antiretroviral treatment in Kisesa, Tanzania: A follow-up study to understand attrition from the antiretroviral program. AIDS Patient Care and STDs, 23(3), 203–210. doi:10.1089/apc.2008.0129
- Schulz, K. F., Altman, D. G., & Moher, D. (2010). CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ, 340 :c332. doi:10.1136/bmj.c332.
- Silverman, K., Holtyn, A. F., Rodewald, A. M., Siliciano, R. F., Jarvis, B. P., Subramaniam, S., Leoutsakos, J.-M., Getty, C.-A., Ruhs, S., Marzinke, M. A., & Fingerhood, M. (2019). Incentives for viral suppression in people living with HIV: A randomized clinical trial. AIDS and Behavior, 23(9), 2337–2346. doi:10.1007/s10461-019-02592-8
- Solomon, S. S., Srikrishnan, A. K., Vasudevan, C. K., Anand, S., Kumar, M. S., Balakrishnan, P., Mehta, S. H., Solomon, S., & Lucas, G. M. (2014). Voucher incentives improve linkage to and retention in care among HIV-infected drug users in Chennai, India. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 59(4), 589–595. doi:10.1093/cid/ciu324
- StataCorp. (2017). Stata statistical software: release 15. StataCorp LP.
- The United Republic of Tanzania. Ministry of Health and Social Welfare. National AIDS Control Programme. (2009). National guidelines for home based care services in Tanzania. February.
- The United Republic of Tanzania. Ministry of Health, Community Development, Gender, Elderly, and Children. National AIDS Control Programme. (2017). National guidelines for the management of HIV and AIDS. 6th edition (October).
- Tversky, A., & Kahneman, D. (1974). Judgment under uncertainty: Heuristics and biases. Science, 185(4157), 1124 LP –1131. doi:10.1126/science.185.4157.1124
- UNAIDS. (2020). Global HIV & AIDS Statistics - 2020 fact sheet. UNAIDS. https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf
- Ware, N. C., Wyatt, M. A., Geng, E. H., Kaaya, S. F., Agbaji, O. O., Muyindike, W. R., Chalamilla, G., & Agaba, P. A. (2013). Toward an understanding of disengagement from HIV treatment and care in sub-saharan Africa: A qualitative study. PLOS Medicine, 10(1), e1001369. doi:10.1371/journal.pmed.1001369
- Wharton University of Pennsylvania Credibility Lab. (n.d.). AsPredicted. http://www.aspredicted.org
- World Health Organization. (2003). Adherence to long term therapies. Evidence for action. World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf?sequence=1&isAllowed=y
- Yotebieng, M., Thirumurthy, H., Moracco, K. E., Edmonds, A., Tabala, M., Kawende, B., Wenzi, L. K., Okitolonda, E. W., & Behets, F. (2016). Conditional cash transfers to increase retention in PMTCT care, antiretroviral adherence, and postpartum virological suppression: A randomized controlled trial. Journal of Acquired Immune Deficiency Syndromes (1999), 72 Suppl 2(Suppl 2), S124–S129. doi:10.1097/QAI.0000000000001062
- Young, S., Wheeler, A. C., McCoy, S. I., & Weiser, S. D. (2014). A review of the role of food insecurity in adherence to care and treatment among adult and pediatric populations living with HIV and AIDS. AIDS and Behavior, 18 Suppl 5(0 5), S505–S515. doi:10.1007/s10461-013-0547-4
