
ABSTRACT
Currently, the management of comorbidities and polypharmacy in HIV-infected patients requires a coordinated action, with special focus on gender differences. Observational, cross-sectional study was conducted to study the HIV population from Menorca (Illes Balears). Adult HIV-positive individuals on antiretroviral treatment attending the pharmacy service from Hospital Mateu Orfila (Menorca) were included. In a single visit, demographical and clinical characteristics, comorbidities and cotreatments were collected. Anticholinergic burden (Drug Burden Index, DBI), drug-to-drug interactions (BOT PLUS database) and symptoms associated with HIV treatment (HIV-SI index) were assessed. A total of 223 patients were included, 68.2% men, with a median age of 53.00 (44.50–58.00) years, median BMI of 24.07, 47.73% smokers and 9.90% drug consumers. Women had more advanced stages of the disease and significantly more symptoms (cough and anxiety) versus men (p = .033 and p = .048, respectively). Moreover higher exposures to anticholinergic drugs (DBI 0.51 vs. 0.27) were reported, together with more frequency of drug-to-drug interactions (57.7% vs. 37.5%; p = .005) that increased with age. Red interactions were more frequently reported in PI (2.69%), NNRTIs (1.92%) and booster drugs (1.92%). These results support the need to implement specific measures for the management of HIV-infected women and tools to assess polypharmacy and risk of drug-to-drug interactions.
1. Introduction
Currently, there are more than 38 million people living with HIV worldwide (www.unaids.org), with new diagnoses attributable to male-male sex increasing in most high-income countries (Sullivan et al., Citation2014).
Antiretroviral treatment has enabled HIV-infected persons to live with chronic infection (Lucas & Nelson, Citation2015), with long-term survival approaching that of the general population (Akbari et al., Citation2019), particularly in patients without risk factors on a successful highly active antiretroviral therapy (HAART) (Obel et al., Citation2011).
Due to aging, HIV individuals are suffering an increased number of comorbidities, occurring at higher rates than in patients without HIV for any given age (Wing, Citation2016). Comorbidities, polypharmacy and drug-to-drug interactions (DDIs) have become an important challenge, particularly in older HIV-infected adults, with the risk of side effects and related diseases (Mazzitelli et al., Citation2019; Morillo-Verdugo et al., Citation2018; Smit et al., Citation2015). Cardiovascular disease has emerged as an important cause of morbidity and mortality (Martin-Iguacel et al., Citation2015), while renal, neurocognitive, oncological, osteoporotic and mental diseases are also highly prevalent (Clifford & Ances, Citation2013; Gameiro et al., Citation2018; Ji & Lu, Citation2017; Negredo et al., Citation2018; Nosrat et al., Citation2017).
Management of comorbidities and polypharmacy in HIV-infected patients requires a coordinated action among different specialties to reduce individual risk, health system costs and improve overall clinical outcomes (Mazzitelli et al., Citation2019; Wing, Citation2016). The differential management according to gender is another important need to be assessed (Amin, Citation2015; Darlington & Hutson, Citation2017; Ghosn et al., Citation2018). In this regard, a marker of comedications in people living with HIV is the anticholinergic burden (Casajús-Navasal et al., Citation2018), although their use as surrogated marker of polypharmacy in HIV patients is still limited (Mazzitelli et al., Citation2019).
Another important tool is the use of patient-reported outcomes (PROs), which can capture relevant symptoms and health-related information, and can help to identify complications, including psychological alterations (Marrone et al., Citation2016). With growing constraints on time and resources, integration of PROs into decision-making and prioritization may provide a much-needed tool to ensure optimal HIV care (Kjær et al., Citation2018), identifying patients at risk of treatment failure or in need of additional support and assessment (Marrone et al., Citation2016). Despite their potential utility, the application of PROs in clinical practice is still limited (Engler et al., Citation2017).
In this context, the aim of this observational, cross-sectional study was to evaluate the clinical characteristics of the HIV-positive population in Menorca (Illes Balears, Spain), with a focus on their comorbidities, PROs and co-treatments and differences according to gender.
2. Methods
We conducted a unicenter, observational, cross-sectional study on HIV patients attending the pharmacy service from Hospital Mateu Orfila (Menorca, Illes Balears, Spain), between May 2019 and May 2020. Adult (≥18 years) HIV-positive patients on antiretroviral treatment were included.
Protocol, informed consent form and other patient information were reviewed and approved by the Clinical Research Ethics Committee (CREC)/Independent Ethics Committee (IEC) of Illes Balears (Palma de Mallorca, Spain). The study was performed following the principles of Declaration of Helsinki and its subsequent revisions. All patients received detailed information and provided written informed consent to participate prior to inclusion.
Data were collected in a single visit on anthropometric measurements [age, gender, body mass index (BMI)], addictions (tobacco consumption and drug abuse), clinical characteristics of HIV infection [date of diagnosis, transmission route, HCV and/or HBC co-infection, viral load, CD4 count (cells/mm3), viral load (detectable >50 copies/mL) and CDC staging] (CDC, Citation2014), antiretroviral treatment (drug, dose), comorbidities and cotreatments.
The Drug Burden Index (DBI) was obtained considering the dose of anticholinergic and sedative drugs (Hilmer, Citation2018; Kouladjian et al., Citation2016) using the Anticholinergic Burden Calculator (http://www.anticholinergicscales.es/) (Hilmer et al., Citation2007). The DBI tool was used to calculate cumulative exposure to medications with clinically significant anticholinergic and/or sedative effects dispensed from 1 May 2019 to 31 May 2020. Anticholinergic drug medications were identified using ATCC codes.
DBI scores for participants were calculated as continuous variables and then transformed into a categorical variable with three levels: 0 (no DBI exposure), 0–1 (low exposure), ≥1 (high exposure) (Byrne et al., Citation2019; O’Connell et al., Citation2018).
DDIs were assessed using BOT PLUS database from the Spanish General Council of the Pharmaceutical College (https://botplusweb.portalfarma.com/), which automatically detects DDIs based on the Summary of Product Characteristics (SmPC) and bibliographic references supporting the interaction (described or theoretical). DDIs were categorized into green (use as directed), yellow (moderate) and red (significant) categories.
Patients were required to complete the HIV Symptom Index (HIV-SI index), a self-reported 20-item symptom questionnaire (Justice et al., Citation2001). Respondents rated their experience during the past four weeks using a five-point Likert-type scale with values ranging from 0 (lack of symptom) to 4 (very bothersome) (total value: 0–80). A symptom was considered to be present if it has >2 points. The Spanish validated questionnaire was used (Ibarra-Barrueta et al., Citation2019).
Frequency tables were generated for categorical variables. Since continuous variables did not adjust to a normal distribution, they were expressed as median and interquartile range (IQR).
Differences found between subgroups were compared using nonparametric tests (Wilcoxon signed-rank). The chi-squared test or Fisher’s exact test were used for the analysis of association of qualitative variables.
A logistic regression model was performed to detect the factors independently associated with comorbidities and anticholinergic exposure. All models were adjusted using Wald statistic. The model was built including all variables with a p-value <.1 along the bivariate analysis.
In all analyses, the assumed alpha and beta errors were of 5% and 20%, respectively. All statistical analyses were carried out using R software, version 3.6.2.
3. Results
In total, 223 patients were included, 68.2% men, with a median age of 53.00 years (interquartile range: 44.50–58.00) and a median BMI of 24.07 (21.89–27.34). Almost half of the patients were smokers (47.73%) and 9.90% drug consumers ().
Table 1. Demographic characteristics of patients (n = 223).
The median age from diagnosis was 18.75 years (9.42-27.73), with a median CD4 count of 711.0 cell/mm3 (509.50–903.00), mainly undetectable (94.6%). The most frequent CDC stages were C3 (22.4%), A2 (19.3%), B3 (17.5%) and B2 (14.3%). By gender, the most advanced stages of the disease were more frequent in women: B3 (22.5% vs. 15.1%; p = .243), C3 (26.8% vs. 20.4%; p = .374).
Co-infection with HCV was present in 25.1%, while HBV coinfection and HCV and HBV coinfection occurred in 2.3% of patients ().
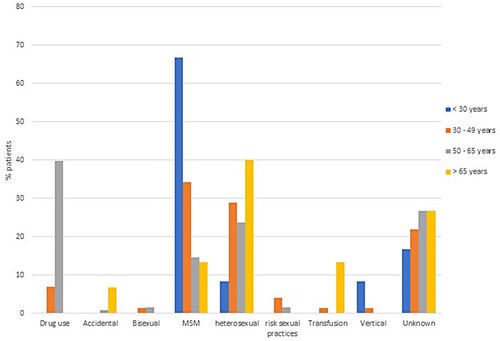
Sexual was the most frequent route of transmission (52.9%), with similar risk in heterosexual patients (25.6%) than in men who have sex with men (MSM) (23.8%) (2.2% risk practices and 1.3% bisexual), followed by parenteral transmission in injection drug users (25.1%), blood transfusions (1.3%) and vertical transmission (0.9%). The parenteral transmission (injection drug users) was prevalent in the age range of 50–65 years, the heterosexual transmission was more frequent in patients >60 years, while the MSM transmission was more frequent in younger patients (<30 years) ().
Figure 1. HIV transmission routes according to age ranges.
Regarding the antiretroviral treatment, 78.5% of patients were pre-treated. Most patients (86.1%) were receiving triple therapy, 7.2% bitherapy, 5.8% monotherapy and 0.9% quadruple therapy. The most frequent antiretroviral drugs were nucleoside reverse transcriptase inhibitors (NRTIs) (87.4%), followed by integrase inhibitors (INIs) (44.8%), non-nucleoside reverse transcriptase inhibitors (NNRTIs) (39.5%) and protease inhibitors (PI) (23.3%). The most frequent antiretroviral combinations were two NRTIs drugs plus one INIs (41.7%) and two NRTIs plus one NNRTIs (30.0%).
In the bivariate analysis, different conditions were associated with each group of antiretroviral drugs (). PIs were more frequently prescribed in women (33.8% vs. 18.4%; p = .011), while NRTIs were more frequently prescribed in men (92.1% vs. 77.5%; p = .002).
Table 2. Bivariate analysis identifying the factors associated with the use of antiretroviral drugs (INIs, NRTIs, NNRTIs and PI).
The main comorbidities were renal impairment (52.9%), osteoporosis (38.6%), cardiovascular diseases (25.6%), hypertension (20.6%), mental disorders (19.8%), malignancies (13.9%), cardiovascular event (6.3%) and diabetes mellitus (4.9%).
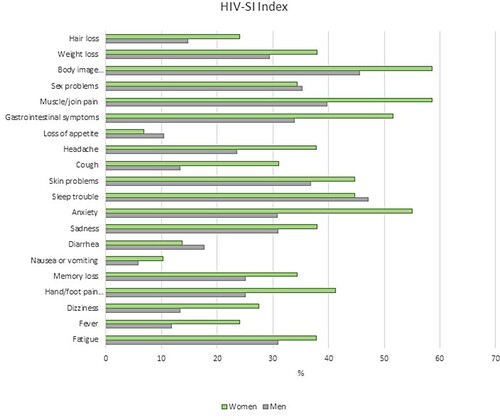
The most frequent symptoms, assessed using the HIV-SI index (>2 points), were changes in the body composition (fat deposits or weight increase) (49.5%), sleep troubles (46.4%) and muscle/joint pain (45.4%). Anxiety was present in 38.1% of patients and sadness and depression in 33.0%. The less frequent symptoms were loss of appetite (9.3%) and nausea and vomiting (7.2%).
The prevalence of symptoms was more frequent in women for most symptoms, with statistically significant differences between women and men in cough (31.0% vs. 13.3%; p = .033) and anxiety (55.0% vs. 30.8%; p = .048) (). Women taking INIs had statistically significant more hand/foot pain than men (41.3% vs. 19.6%; p = .024), while men treated with NRTIs had more hair loss than women (45.5% vs. 14.0%; p = .026). By age, patients aged <50 years suffered more headache than patients ≥50 years (41.9% vs. 21.2%; p = .039).
Figure 2. Prevalence of symptoms, assessed using the HIV-SI index, by gender.
Patients with sleep disturbances had statistically significant differences versus patients without this symptom: higher weight (p = .028) and BMI (p = .011), a lower time from diagnosis (p = .002), more frequency of naive patients (p = .021) and more use of INIs (p = .027). Patients with muscle pain had higher BMI (p = .004) and took more INIs (p = .020). Patients with body image changes had a lower age (p = .033), higher weight (p = .010) and BMI (p <.001).
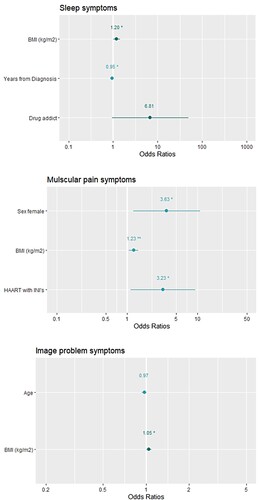
In the multivariate logistic regression, having sleep disturbances was associated with BMI [OR (95% CI): 1.199 (1.021–1.429); p = .032] and lower time from diagnosis [OR (95% CI): 0.948 (0.898–0.998); p = .046]. Muscle pain was associated with female gender [OR (95% CI): 3.633 (1.246–11.215); p = .0032], BMI [OR (95% CI): 1.230 (1.065–1.454); p < .001] and treatment with INIs [OR (95% CI): 3.230 (1.157–9.805); p = .029]. Body image changes were associated with higher BMI [OR (95% CI): 1.457 (1.227–1.794); p < .001] ().
Figure 3. Multivariate logistic regression. Factors associated with comorbidities. (A) Sleep symptoms. (B) Muscular pain symptoms. (C) Image problem symptoms.
For the treatment of the comorbidities, the most frequent drug groups (ATCC) were group A (alimentary tract and metabolism) (26.42%), particularly anti-ulcer, vitamins and mineral supplements; N (nervous system) (24.07%), particularly benzodiazepines and analgesic drugs; C (cardiovascular system), including antihypertensive and lipid-lowering drugs. Drug prescription increased with age, having polypharmacy among 27.5% of patients and 37.8% aged ≥50 years, and mean number of prescribed drugs increased from 0.82 drugs at <30 years, 1.89 at 30–50 years, 4.86 at 50–65 years and 8.87 at >65 years.
Polypharmacy was also higher in women than in men (35.3% vs. 24.0%; p = .036). A higher percentage of women than men were treated with 5–9 drugs (26.4% vs. 17.3%) and ≥10 drugs (8.9% vs. 6.7%).
In total, 303 DDIs were detected, 37 between antiretroviral drugs (16.6%), 136 between antiretroviral and non-antiretroviral drugs (61.0%) and 130 between non-antiretroviral drugs (58.3%). Most reported interactions had yellow category (75.6%), followed by green (17.5%) and red (6.9%). Among the antiretroviral drugs, red and yellow interactions were more frequent in PIs, particularly darunavir. Red interactions were more frequent in PIs (2.69%), NNRTIs (1.92%) and booster drugs (1.92%), while yellow interactions were mostly reported in PIs (51.1%) and booster drugs, particularly cobicistat (18.85%) ().
Table 3. Drug-to-drug interactions between antiretroviral drugs.
In non-antiretroviral drugs, yellow interactions were the most frequent, being the drugs more involved: nervous (32.45%) and cardiovascular system (22.16%). Red interactions were infrequent (nervous system) ().
DDIs were more frequent in women than in men (57.7% vs. 37.5%; p = 0.005) and increased with age (16.7% at <30 years, 28.8% at 30–50 years, 52.0% at 50–65 years and 73.3% at >65 years).
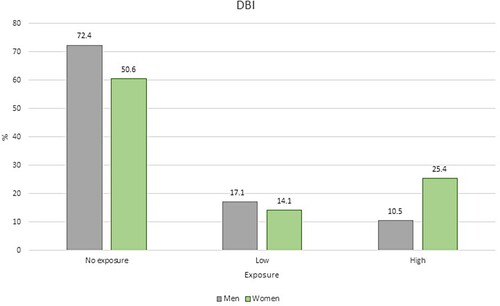
Regarding the anticholinergic burden, 31.3% of patients had low or high exposure (16.1% low and 15.2% high), while 68.6% of patients had no exposure.
Women had more exposure to anticholinergic drugs than men, with a mean DBI of 0.51 versus 0.27 (p = .113). Low exposure was more frequent in men (17.1% vs. 14.1%), while the high exposure was more prevalent in women (25.4% vs. 10.5%; p = .016) ().
Figure 4. Anticholinergic burden, according to DBI, by gender. Percentage of patients without exposure, low exposure and high exposure.
The main drugs accounting for the anticholinergic burden were benzodiazepines (40.87%), antidepressants (18.26%) and antiepileptics (15.65%). The occurrence of DDIs increased in patients with high anticholinergic exposure: 32.9% in patients without exposure, 52.8% in patients with low and 81.8% in patients with high exposure (p < .001).
The exposure to anticholinergic drugs (high and low) was associated with mental disorders [OR (95% CI): 13.189 (4.138–47.588); p < .001] and the number of prescribed drugs [OR (95% CI): 1.308 (1.113–1.570); p < .001].
4. Discussion
In Spain, there are more than 145,000 people living with HIV (Hemelaar, Citation2019), mainly occurring in men (approximately 85%), with a mean age of 36 years, and MSM (56.4%) (Unidad de Vigilancia de VIH, Citation2019).
In the Balearic Islands, the rates of HIV infection are usually above the rates of the whole country (Memòria VIH/SIDA, Citation2018), with more cases in Mallorca, and Eivissa and less cases in Menorca, where there are 223 HIV-positive subjects. Therefore, in our study, we assessed the complete sample of HIV individuals from this island, with an older age than the Spanish HIV population. Therefore, these results can be considered by clinicians and health service managers.
It is remarkable that, despite the higher prevalence reported in men, in our study, women had more advanced stages of the disease, significantly more comorbidities (cough and anxiety) than men. In consonance, we reported higher exposures to anticholinergic drugs and more frequency of DDIs, which increased with age. To our knowledge, it is the first report that shows worse results in most clinical characteristics in women from western countries. Sex differences in HIV can arise from a combination of different factors including sex hormones, genetic differences and sociobehavioral and environmental influences (Scully, Citation2018). However, few data exist assessing the prevalence and characteristics of women comorbidities and PROs and the role of sex differences in clinical interventions remains to be defined (Scully, Citation2018). Specific treatment response and adverse events also deserve further research. While current guidelines focus on preferred treatments in subgroups of patients (by age or special situations such as pregnancy, tuberculosis infection or malignancies), specific measures according to sex differences and PROs results are not addressed (Miralles et al., Citation2018; Mofenson et al., Citation2009; Ryom et al., Citation2018). Results obtained are supporting the need for specific management for HIV-infected women.
One interesting result of our study is the significantly higher prevalence of anxiety in women, thus pointing to a worse mental health, more stress and worse quality of life, associated with psychosocial determinants (such as poor social support, discrimination, gender-based violence) which are becoming increasingly apparent (Amin, Citation2015; Darlington & Hutson, Citation2017; Ghosn et al., 2018; Miralles et al., Citation2013). It is estimated that 60%–90% of women affected by gender-based violence develop anxiety disorders and approximately 50% develop mood disorders, such as depression (Rees et al., Citation2011; Zunner et al., Citation2015). Anxiety is more common among HIV-positive patients (ranging from 43.2% to 72.7% in the U.S.A.) (Ivanova et al., Citation2012) than in the rest of the population (Yousuf et al., Citation2020), where anxiety is the most common class of mental disorder (24.9%) (Bandelow & Michaelis, Citation2015) and also more frequent in women than in men (two to three times), a reflection of social gender differences and biological determinants (Parker & Brotchie, Citation2010). HIV-positive patients with depression or anxiety are more likely to acquire viral resistance and, as a consequence, to develop poor health outcomes (Ivanova et al., Citation2012; Yousuf et al., Citation2020). Then, management of mental disorders (anxiety and depression) among HIV-infected women should be a priority, particularly in pregnant women, with estimated rates of psychological distress up to 70% (Ivanova et al., Citation2012; Ngocho et al., Citation2019; Qin et al., Citation2019).
We also reported that DDIs were more frequent in women than in men and increased with age, in consonance with higher prevalence of comorbidities, polypharmacy and DBI values. Altogether, this highlights the need to implement specific measures for the management of HIV-infected women.
In our study, the prevalence of comorbidities was high, mainly renal impairment (52.9%), in accordance with previous studies (Greene et al., Citation2014; Moore et al., Citation2015). Polypharmacy was also frequent (27.5%), particularly in aged patients, representing a major risk for the occurrence of adverse events and DDIs (Wing, Citation2016). These results are in accordance with previous studies, in which polypharmacy and medication-related problems were still higher in patients aged ≥60 years (96% of patients taking five or more medications) (Greene et al., Citation2014) and ≥65 years (93%) (Bastida et al., Citation2017).
This highlights the need to review polypharmacy in HIV patients (Morillo-Verdugo et al., Citation2018), leading to pharmacological desprescription, a multidisciplinary process evaluating inadequate medications, benefit-risk ratio or patients’ preferences (Abrass et al., Citation2017; GeSIDA, Citation2018).
In our study, we described potential drug–drug interactions (6.9% red and 75.6% yellow) mostly associated with PIs and particularly with darunavir, followed by NNRTIs, in consonance with a previous study in Spanish HIV patients (65% with at least one potential interaction; 6.6% with a severe potential interaction), being the risk significantly associated with PIs use (Bastida et al., Citation2017).
Medication interactions between cART and other medications are a major consideration, particularly the cytochrome p450 inhibition that occurs with PIs (e.g., Darunavir) and NNRTI (e.g., Efavirenz) (Wing, Citation2016). These results support the need for regular review of all medications prescribed with regard to drug interactions in the management of HIV-infected patients (Wing, Citation2016).
In this regard, DBI has the potential as a clinical risk assessment tool to help clinicians recognize anticholinergic and sedative medicines that can impair function and prompt them to minimize patient’s exposure to these medicines. The use of electronic calculators allows to easily obtain patient’s DBI and its associated risks (Hilmer, Citation2018; Kouladjian et al., Citation2016).
We reported a high prevalence of patients with anticholinergic burden (up to 31.3%), in line with the results of previous studies (Casajús-Navasal et al., Citation2018; Mazzitelli et al., Citation2019), although different scales were used. For the first time, we detected that women had a statistically significant higher anticholinergic burden than men (39.4% vs. 27.6%).
In our study, we also evaluated PRO using the HIV-SI index. Altogether, polypharmacy and PROs are tools that allow to assess well-being, tolerability and safety of treatments and to stratify patients according to their complexity, and including other markers, such as pharmacogenetics (Hughes et al., Citation2008; Simpson et al., Citation2013; Sukasem et al., Citation2014).
In conclusion, in the HIV-positive population from Menorca, women, in comparison with men, had more advanced stages of the disease, significantly more symptoms (cough and anxiety) and higher exposures to anticholinergic drugs and more frequency of DDIs, which increased with age. These results support the need to implement specific measures for the management of HIV-infected women and tools to assess polypharmacy and the risk of DDIs.
Acknowledgement
Núria Piqué is a Serra Hunter fellow.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Abrass, C. K., Appelbaum, J. S., & Boyd, C. M. (2017). The HIV and aging consensus project: Recommended treatment strategies for clinicians managing older patients with HIV. The HIV and aging consensus project. American Academy of HIV Medicine, 1–76. https://aahivm.org/wp-content/uploads/2017/02/Aging-report-working-document-FINAL-12.1.pdf
- Akbari, M., Fararouei, M., Haghdoost, A. A., Gouya, M. M., & Kazerooni, P. A. (2019). Survival and associated factors among people living with HIV/AIDS: A 30-year national survey in Iran. Journal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences, 24, 5. https://doi.org/10.4103/jrms.JRMS_630_18
- Amin, A. (2015). Addressing gender inequalities to improve the sexual and reproductive health and wellbeing of women living with HIV. Journal of The international Aids Society, 18(Suppl 5), 20302. https://doi.org/10.7448/IAS.18.6.20302
- Bandelow, B., & Michaelis, S. (2015). Epidemiology of anxiety disorders in the 21st century. Dialogues in Clinical Neuroscience, 17(3), 327–335. https://doi.org/10.31887/DCNS.2015.17.3/bbandelow
- Bastida, C., Grau, A., Márquez, M., Tuset, M., De Lazzari, E., Martínez, E., & Gatell, J. M. (2017). Polifarmacia e interacciones farmacológicas potenciales en una población envejecida con infección por el VIH [Polypharmacy and potential drug-drug interactions in an HIV-infected elderly population]. Farmacia hospitalaria : organo oficial de expresion cientifica de la Sociedad Espanola de Farmacia Hospitalaria, 41(5), 618–624. https://doi.org/10.7399/fh.10778
- Byrne, C. J., Walsh, C., Cahir, C., & Bennett, K. (2019). Impact of drug burden index on adverse health outcomes in Irish community-dwelling older people: A cohort study. BMC Geriatrics, 19(1), 121. https://doi.org/10.1186/s12877-019-1138-7
- Casajús-Navasal, A., Marín-Gorricho, R., Gallardo-Anciano, J., Nebot-Villacampa, M. J., Zafra-Morales, R., & González-Pérez, Y. (2018). Prevalencia de prescripción de fármacos anticolinérgicos en pacientes mayores con VIH [Prevalence of the consumption of anticholinergic drugs in HIV patients]. Farmacia hospitalaria : organo oficial de expresion cientifica de la Sociedad Espanola de Farmacia Hospitalaria, 42(1), 1–4. https://doi.org/10.7399/fh.10842
- Centers for Disease Control and Prevention (CDC). (2014). Revised surveillance case definition for HIV infection-United States. MMWR Recommendations and Reports, 63, 1–10. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6303a1.htm
- Clifford, D. B., & Ances, B. M. (2013). HIV-associated neurocognitive disorder. The Lancet: Infectious Diseases, 13(11), 976–986. https://doi.org/10.1016/S1473-3099(13)70269-X
- Darlington, C. K., & Hutson, S. P. (2017). Understanding HIV-related stigma among women in the southern United States: A literature review. AIDS and Behavior, 21(1), 12–26. https://doi.org/10.1007/s10461-016-1504-9
- Engler, K., Lessard, D., & Lebouché, B. (2017). A review of HIV-specific patient-reported outcome measures. The Patient, 10(2), 187–202. https://doi.org/10.1007/s40271-016-0195-7
- Gameiro, J., Jorge, S., & Lopes, J. A. (2018). HIV and renal disease: A contemporary review. International Journal of STD & AIDS, 29(7), 714–719. https://doi.org/10.1177/0956462417750710
- GeSIDA (grupo de estudio del SIDA-SEIMC). Desprescripción farmacológica de la terapia no antiretroviral en pacientes con infección por VIH (update October 2018). Coord: JR Blanco, Ramón Morillo.
- Ghosn, J., Taiwo, B., Seedat, S., Autran, B., & Katlama, C. (2018). HIV. Lancet (London, England), 392(10148), 685–697. https://doi.org/10.1016/S0140-6736(18)31311-4
- Greene, M., Steinman, M. A., McNicholl, I. R., & Valcour, V. (2014). Polypharmacy, drug-drug interactions, and potentially inappropriate medications in older adults with human immunodeficiency virus infection. Journal of the American Geriatrics Society, 62(3), 447–453. https://doi.org/10.1111/jgs.12695
- Hemelaar, J. (2019). HIV in Europe: A long road still lies ahead. The Lancet Infectious Diseases, 19(2), 1. https://doi.org/10.1016/S1473-3099(18)30647-9
- Hilmer, S. N. (2018). Calculating and using the drug burden index score in research and practice. Expert Review of Clinical Pharmacology, 11(11), 1053–1055. https://doi.org/10.1080/17512433.2018.1528145
- Hilmer, S. N., Mager, D. E., Simonsick, E. M., Cao, Y., Ling, S. M., Windham, B. G., Harris, T. B., Hanlon, J. T., Rubin, S. M., Shorr, R. I., Bauer, D. C., & Abernethy, D. R. (2007). A drug burden index to define the functional burden of medications in older people. Archives of Internal Medicine, 167(8), 781–787. https://doi.org/10.1001/archinte.167.8.781
- Hughes, S., Hughes, A., Brothers, C., Spreen, W., Thorborn, D., & CNA106030 Study Team (2008). PREDICT-1 (CNA106030): The first powered, prospective trial of pharmacogenetic screening to reduce drug adverse events. Pharmaceutical Statistics, 7(2), 121–129. https://doi.org/10.1002/pst.286
- Ibarra-Barrueta, O., Mora-Atorrasagasti, O., Legarreta, M. J., Illaro-Uranga, A., & Morillo-Verdugo, R. (2019). Estudio piloto para desarrollar y validar un cuestionario basado en el índice de síntomas de VIH [Pilot study to develop and validate a questionnaire based on HIV symptoms index]. Farmacia hospitalaria: organo oficial de expresion cientifica de la Sociedad Espanola de Farmacia Hospitalaria, 43(3), 87–93. https://doi.org/10.7399/fh.11127
- Ivanova, E. L., Hart, T. A., Wagner, A. C., Aljassem, K., & Loutfy, M. R. (2012). Correlates of anxiety in women living with HIV of reproductive age. AIDS and Behavior, 16(8), 2181–2191. https://doi.org/10.1007/s10461-011-0133-6
- Ji, Y., & Lu, H. (2017). Malignancies in HIV-infected and AIDS patients. Advances in Experimental Medicine and Biology, 1018, 167–179. https://doi.org/10.1007/978-981-10-5765-6_10
- Justice, A. C., Holmes, W., Gifford, A. L., Rabeneck, L., Zackin, R., Sinclair, G., Weissman, S., Neidig, J., Marcus, C., Chesney, M., Cohn, S. E., Wu, A. W., & Adult AIDS Clinical Trials Unit Outcomes Committee. (2001). Development and validation of a self-completed HIV symptom index. Journal of Clinical Epidemiology, 54(Suppl 1), S77–S90. https://doi.org/10.1016/s0895-4356(01)00449-8
- Kjær, A., Rasmussen, T. A., Hjollund, N. H., Rodkjaer, L. O., & Storgaard, M. (2018). Patient-reported outcomes in daily clinical practise in HIV outpatient care. International Journal of Infectious Diseases: IJID: Official Publication of the International Society for Infectious Diseases, 69, 108–114. https://doi.org/10.1016/j.ijid.2018.02.015
- Kouladjian, L., Gnjidic, D., Chen, T. F., & Hilmer, S. N. (2016). Development, validation and evaluation of an electronic pharmacological tool: The Drug Burden Index Calculator©. Research in Social & Administrative Pharmacy: RSAP, 12(6), 865–875. https://doi.org/10.1016/j.sapharm.2015.11.002
- Lucas, S., & Nelson, A. M. (2015). HIV and the spectrum of human disease. The Journal of Pathology, 235(2), 229–241. https://doi.org/10.1002/path.4449
- Marrone, G., Mellgren, Å, Eriksson, L. E., & Svedhem, V. (2016). High concordance between self-reported adherence, treatment outcome and satisfaction with care using a nine-item health questionnaire in InfCareHIV. PLoS One, 11(6), Article 0156916. https://doi.org/10.1371/journal.pone.0156916
- Martin-Iguacel, R., Llibre, J. M., & Friis-Moller, N. (2015). Risk of cardiovascular disease in an aging HIV population: Where are we now? Current HIV/AIDS Reports, 12(4), 375–387. https://doi.org/10.1007/s11904-015-0284-6
- Mazzitelli, M., Milinkovic, A., Pereira, B., Palmer, J., Tong, T., Asboe, D., & Boffito, M. (2019). Polypharmacy and evaluation of anticholinergic risk in a cohort of elderly people living with HIV. AIDS (London, England), 33(15), 2439–2441. https://doi.org/10.1097/QAD.0000000000002403
- Memòria VIH/SIDA de les Illes Balears. (2018). Consellera de Salut i Consum. Direcció General de Salut Pública i Participació. Govern de les Illes Balears.
- Miralles, C., Mardarescu, M., & Sherr, L. (2013). What do we know about the situation of women living with HIV in Europe? Antiviral Therapy, 18(Suppl 2), 11–17. https://doi.org/10.3851/IMP2646
- Miralles, P., Navarro, J. T., Berenguer, J., Gómez Codina, J., Kwon, M., Serrano, D., Díez-Martín, J. L., Villà, S., Rubio, R., Menárguez, J., & Ribera Santasusana, J. M. (2018). Recomendaciones de GESIDA/PETHEMA sobre el diagnóstico y tratamiento de los linfomas en pacientes infectados por el virus de la inmunodeficiencia humana [GESIDA/PETHEMA recommendations on the diagnosis and treatment of lymphomas in patients infected by the human immunodeficiency virus]. Medicina Clinica, 151(1), 39.e1–39.e17. https://doi.org/10.1016/j.medcli.2017.11.037
- Mofenson, L. M., Brady, M. T., Danner, S. P., Dominguez, K. L., Hazra, R., Handelsman, E., Havens, P., Nesheim, S., Read, J. S., Serchuck, L., Van Dyke, R., & Centers for Disease Control and Prevention, National Institutes of Health, HIV Medicine Association of the Infectious Diseases Society of America, Pediatric Infectious Diseases Society, & American Academy of Pediatrics. (2009). Guidelines for the prevention and treatment of opportunistic infections among HIV-exposed and HIV-infected children: Recommendations from CDC, the National Institutes of Health, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. MMWR. Recommendations and Reports: Morbidity and Mortality Weekly Report. Recommendations and Reports, 58(RR-11), 1–166.
- Moore, H. N., Mao, L., & Oramasionwu, C. U. (2015). Factors associated with polypharmacy and the prescription of multiple medications among persons living with HIV (PLWH) compared to non-PLWH. AIDS Care, 27(12), 1443–1448. https://doi.org/10.1080/09540121.2015.1109583
- Morillo-Verdugo, R., Blanco Ramos, J. R., Abdel-Kader Martín, L., & Álvarez de Sotomayor, M. (2018). The challenge of aging and pharmacotherapeutic complexity in the HIV+ patient. Farmacia Hospitalaria, 42(3), 120–127. https://doi.org/10.7399/fh.10931
- Negredo, E., Domingo, P., Gutiérrez, F., Galindo, M. J., Knobel, H., Lozano, F., Martínez, E., Masiá, M., Polo, R., & Estrada, V. (2018). Executive summary of the consensus document on osteoporosis in HIV-infected individuals. Enfermedades infecciosas y microbiologia clinica, 36(5), 312–314. https://doi.org/10.1016/j.eimc.2017.03.010
- Ngocho, J. S., Watt, M. H., Minja, L., Knettel, B. A., Mmbaga, B. T., Williams, P. P., & Sorsdahl, K. (2019). Depression and anxiety among pregnant women living with HIV in Kilimanjaro region, Tanzania. PLoS One, 14(10), Article 0224515. https://doi.org/10.1371/journal.pone.0224515
- Nosrat, S., Whitworth, J. W., & Ciccolo, J. T. (2017). Exercise and mental health of people living with HIV: A systematic review. Chronic Illness, 13(4), 299–319. https://doi.org/10.1177/1742395317694224
- O’Connell, J., Burke, É, Mulryan, N., O'Dwyer, C., Donegan, C., McCallion, P., McCarron, M., Henman, M. C., & O’Dwyer, M. (2018). Drug burden index to define the burden of medicines in older adults with intellectual disabilities: An observational cross-sectional study. British Journal of Clinical Pharmacology, 84(3), 553–567. https://doi.org/10.1111/bcp.13479
- Obel, N., Omland, L. H., Kronborg, G., Larsen, C. S., Pedersen, C., Pedersen, G., Sørensen, H. T., & Gerstoft, J. (2011). Impact of non-HIV and HIV risk factors on survival in HIV-infected patients on HAART: A population-based nationwide cohort study. PLoS One, 6(7), Article 22698. https://doi.org/10.1371/journal.pone.0022698
- Parker, G., & Brotchie, H. (2010). Gender differences in depression. International Review of Psychiatry (Abingdon, England), 22(5), 429–436. https://doi.org/10.3109/09540261.2010.492391
- Qin, S., Tan, Y., Lu, B., Cheng, Y., & Nong, Y. (2019). Survey and analysis for impact factors of psychological distress in HIV-infected pregnant women who continue pregnancy. The Journal of Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 32(19), 3160–3167. https://doi.org/10.1080/14767058.2018.1459550
- Rees, S., Silove, D., Chey, T., Ivancic, L., Steel, Z., Creamer, M., Teesson, M., Bryant, R., McFarlane, A. C., Mills, K. L., Slade, T., Carragher, N., O'Donnell, M., & Forbes, D. (2011). Lifetime prevalence of gender-based violence in women and the relationship with mental disorders and psychosocial function. JAMA, 306(5), 513–521. https://doi.org/10.1001/jama.2011.1098
- Ryom, L., Boesecke, C., Bracchi, M., Ambrosioni, J., Pozniak, A., Arribas, J., Behrens, G., Mallon, P., Puoti, M., Rauch, A., Miro, J. M., Kirk, O., Marzolini, C., Lundgren, J. D., Battegay, M., & Governing Board, E. A. C. S. (2018). Highlights of the 2017 European AIDS clinical Society (EACS) Guidelines for the treatment of adult HIV-positive persons version 9.0. HIV Medicine, 19(5), 309–315. https://doi.org/10.1111/hiv.12600
- Scully, E. P. (2018). Sex differences in HIV infection. Current HIV/AIDS Reports, 15(2), 136–146. https://doi.org/10.1007/s11904-018-0383-2
- Simpson, K. N., Hanson, K. A., Harding, G., Haider, S., Tawadrous, M., Khachatryan, A., Pashos, C. L., & Wu, A. W. (2013). Patient reported outcome instruments used in clinical trials of HIV-infected adults on NNRTI-based therapy: A 10-year review. Health and Quality of Life Outcomes, 11(1), 164. https://doi.org/10.1186/1477-7525-11-164
- Smit, M., Brinkman, K., Geerlings, S., Smit, C., Thyagarajan, K., Sighem, A. v., de Wolf, F., & Hallett, T. B., & ATHENA Observational Cohort. (2015). Future challenges for clinical care of an ageing population infected with HIV: A modelling study. The Lancet. Infectious Diseases, 15(7), 810–818. https://doi.org/10.1016/S1473-3099(15)00056-0
- Sukasem, C., Chamnanphon, M., Koomdee, N., Santon, S., Jantararoungtong, T., Prommas, S., Puangpetch, A., & Manosuthi, W. (2014). Pharmacogenetics and clinical biomarkers for subtherapeutic plasma efavirenz concentration in HIV-1 infected Thai adults. Drug Metabolism and Pharmacokinetics, 29(4), 289–295. https://doi.org/10.2133/dmpk.dmpk-13-rg-077
- Sullivan, P. S., Jones, J. S., & Baral, S. D. (2014). The global north: HIV epidemiology in high-income countries. Current Opinion in HIV and AIDS, 9(2), 199–205. https://doi.org/10.1097/COH.0000000000000039
- Unidad de Vigilancia de VIH y Comportamientos de Riesgo. Vigilancia Epidemiológica del VIH y sida en España. (2018). Sistema de Información sobre Nuevos Diagnósticos de VIH y Registro Nacional de Casos de Sida. Plan Nacional sobre el Sida – D.G. de Salud Pública, Calidad e Innovación/Centro Nacional de Epidemiología – ISCIII. Madrid, Spain. 2019. https://www.mscbs.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/vigilancia/doc/Informe_VIH_SIDA_2019_21112019.pdf
- Wing, E. J. (2016). HIV and aging. International Journal of Infectious Diseases: IJID: Official Publication of the International Society for Infectious Diseases, 53, 61–68. https://doi.org/10.1016/j.ijid.2016.10.004
- Yousuf, A., Musa, R., Isa, M., & Arifin, S. (2020). Anxiety and depression among women living with HIV: Prevalence and correlations. Clinical Practice and Epidemiology in Mental Health: CP & EMH, 16(1), 59–66. https://doi.org/10.2174/1745017902016010059
- Zunner, B., Dworkin, S. L., Neylan, T. C., Bukusi, E. A., Oyaro, P., Cohen, C. R., Abwok, M., & Meffert, S. M. (2015). HIV, violence and women: Unmet mental health care needs. Journal of Affective Disorders, 174, 619–626. https://doi.org/10.1016/j.jad.2014.12.017
