
ABSTRACT
Background
Subacromial pain syndrome is a common musculoskeletal shoulder problem. The accuracy of clinical tests is low and techniques such as ultrasound and magnetic resonance imaging have been added to set up a diagnosis. Previous researchers have usually only examined the symptomatic shoulder. However, there might be similar findings in the asymptomatic shoulder.
Objective
The aim of the present study was to investigate the prevalence of structural abnormalities of both shoulders in patients with clinically diagnosed unilateral subacromial pain syndrome using diagnostic ultrasound.
Methods
Bilateral ultrasound examinations were performed in 115 consecutive patients, 54 men and 61 women. The patients were recruited from primary care centers in the area of Stockholm, Sweden.
Results
Abnormal ultrasound findings were found in both shoulders and increased with age (p = .0004). Bursitis was the most common ultrasound finding and significantly more prevalent in the symptomatic shoulder compared to the asymptomatic shoulder (90%:74%; p = .0021), though 73% of the bursitis were bilateral. Supraspinatus is the most vulnerable tendon of the rotator cuff in both shoulders. In terms of partial-thickness tears and tendinosis, the tendon was affected more commonly in the symptomatic shoulder compared to the asymptomatic shoulder (30%:14%: 14%; p = .0026) and (24%:10%; p = .0054), respectively, but for calcification no significant difference between the shoulders was found (18%:12%; 0.1988).
Conclusion
Ultrasound detected shoulder abnormalities were present in both symptomatic and asymptomatic shoulders. Bursitis and partial-thickness tears were more common in the affected shoulder when compared to the unaffected shoulder. Ultrasound as well as clinical examination findings and patient´s history should be taken into consideration when diagnosing patients with subacromial pain syndrome.
INTRODUCTION
There is still no consensus about the most appropriate terminology when describing disorders of the rotator cuff (Schellingerhout, Verhagen, Thomas, and Koes, Citation2008). In the present article, we use the term subacromial pain syndrome (SAPS), which is a combination of symptoms and findings, although the pathogenesis still is unknown. SAPS is one of the most common musculoskeletal conditions in patients seeking primary care (Urwin et al., Citation1998). The etiology is known to be multi-factorial (Seitz et al., Citation2011) and it includes several rotator cuff pathologies such as increased tendon thickness (e.g. tendinopathies), bursitis, and partial (PTTs´), or full-thickness tears (FTTs´), affecting the rotator cuff or the long head of the biceps tendon (Mitchell, Adebajo, Hay, and Carr, Citation2005). The pathogenesis of SAPS is still unknown. However, increased age, overload, genetic vulnerability and metabolic disorders such as diabetes mellitus (Abate, Schiavone, Salini, and Andia, Citation2013) and smoking (Carbone et al., Citation2012) have been suggested to be risk factors. Also, dysfunction of the scapula or the rotator cuff (Kibler et al., Citation2013), capsular tightness (Tyler, Nicholas, Roy, and Gleim, Citation2000) and a poor posture (Lewis, Wright, and Green, Citation2005) may play a role.
SAPS is a clinical diagnosis and a combination of different tests for physical examination have been suggested (Michener, Walsworth, Doukas, and Murphy, Citation2009). Due to low accuracy of the clinical tests (May et al., Citation2010), diagnostic ultrasound (US) has become a popular tool to identify structural changes of the shoulder joint. Diagnostic US has been shown to be equally useful for magnetic resonance imaging (MRI) regarding rotator cuff pathology (Chauhan, Ahluwalia, Sharma, and Thakur, Citation2016; Vlychou et al., Citation2009). An increasing number of medical care clinics and sports injury clinics therefore evaluate their patients with US examinations instead of MRI. The US is cost-effective, allows comparisons between both shoulders, can be dynamically executed and is often appreciated by the patients because of its convenience (Naredo et al., Citation2002).
Detailed descriptions of abnormalities from both shoulders in patients clinically diagnosed with unilateral SAPS are rare. When bilateral comparison with US has been made, the focus has often been on one or two variables, such as PTTs´ or FTTs´ or bursitis, without giving a more detailed presentation of other possible anomalies (Tsai et al., Citation2007; Yamaguchi et al., Citation2006). The samples are often found through mass-screening (Yamamoto et al., Citation2010), or participants with a defined occupation or sport (Guzowski et al., Citation2019) or after rotator cuff repair (Ro et al., Citation2015). This study investigates patients with unilateral pain. In a recent MRI study, a high prevalence of abnormalities in both shoulders was shown in patients with self-reported unilateral shoulder pain (Barreto et al., Citation2019). In a pilot study, detailed US findings of both shoulders in 20 clinically diagnosed SAPS patients was presented (Lewis et al., Citation2009). However, to our knowledge, a larger detailed US investigation of both shoulders on clinically diagnosed patients with unilateral SAPS is still lacking. Therefore, the aim of the present study was to use US in order to evaluate the prevalence of shoulder abnormalities of both shoulders in patients with unilateral SAPS. The hypothesis was to find similar abnormalities in both the unaffected shoulder and the affected shoulder, in primary care patients with clinically diagnosed SAPS.
METHODS
Study Design and Patients
This descriptive investigation was approved by the Regional Ethics Committee in Stockholm in 2009 (2009/1197-31/2) and performed according to the Declaration of Helsinki. Patients were consecutively recruited from seven primary care centers in Stockholm between 2012 and 2016. All patients received written information about the study and signed an informed consent to confirm their participation.
One hundredfifteen patients, 54 men and 61 women diagnosed with unilateral SAPS were included in the study. The patients were 20–59 years of age (mean 45, 0 ± 10, 4) with a pain duration of mean 22 ± 14.5 weeks. The right arm was dominant in 108 patients (94%), and the shoulder of the dominant arm was affected in 72 patients (63%). The dominant arm was defined as the arm that the patient chooses naturally when writing. The mean Constant-Murley assessment score (C-M score) of the present cohort was 38 ± 10 points. The recommended combination of clinical tests for evaluating SAPS was used (Michener, Walsworth, Doukas, and Murphy, Citation2009). All patients underwent bilateral diagnostic US within 5 weeks from the clinical examination. Here, SAPS imply a ruled out presence of restricted passive range of motion (PROM) of the shoulder joint and/or referred pain from the cervical or thoracic spine (Mitchell, Adebajo, Hay, and Carr, Citation2005). Also, clinical signs of total tears and full thickness tears (FTT´s) were excluded (Hertel, Ballmer, Lombert, and Gerber, Citation1996).
Inclusion and Exclusion Criteria
The inclusion criterion was patients aged 20–59 years that had suffered from SAPS between 4 weeks and 1 year. We used the recommended combination of clinical tests for evaluating the patients (Michener, Walsworth, Doukas, and Murphy, Citation2009). For inclusion at least two of these tests had to be positive together with a positive painful arc (Kessel and Watson, Citation1977).
Exclusion criteria were bilateral shoulder pain, earlier treatment with cortisone injection, diabetes mellitus (Abate, Schiavone, Salini, and Andia, Citation2013), history of trauma, fractures and dislocations of the shoulder joint, rheumatoid arthritis, severe arthroses, frozen shoulder (loss of passive and active range of motion) (Chiu et al., Citation2020), a positive drop-arm test (Calis et al., Citation2000) and other clinical signs of total tears or FTT´s. Fibromyalgia and thoracic or cervical spine syndromes.
Clinical Examination
The examiner followed a study protocol and all the tests followed the same order for each patient. To clinically exclude total tears and FTT´s of the rotator cuff, patients were tested for severe weakness (e.g. total “give-away”) with the following tests: 1) Jobe´s test/empty can test: sensitivity 0.60–0.75, specificity 0.13–0.33 (Jobe and Jobe, Citation1983; Kelly, Brittle, and Allen, Citation2010); 2) Drop arm test (lag sign, m. supraspinatus in particular): sensitivity 0.21, specificity 0.92 (Alqunaee, Galvin, and Fahey, Citation2012; Calis et al., Citation2000); and 3) Lag signs: sensitivity 0.45–0.56, specificity 0.56–0.98 (Bak et al., Citation2010; Hertel, Ballmer, Lombert, and Gerber, Citation1996).
Neurologic testing of the upper extremities was always performed. If a patient presented with significant upper extremity weakness and active ROM deficits, revealed reduced or altered sensation or reduced tendon reflexes, they were excluded from the trial. A traumatic history, together with the positive tests above, led to the subjective conclusion that the patient had a total rupture or FTT (larger injury), which led to exclusion. Tests to further identify pain or weakness during resisted flexion, abduction, external and internal rotations were performed (Park et al., Citation2005) as well as the lift off test (Gerber and Krushell, Citation1991), the Palm-up test (Hegedus et al., Citation2008). The Cross- body adduction test (Park et al., Citation2005) and the Hawkin-Kennedy test were used to identify possible impingement of the shoulder (Hawkins and Kennedy, Citation1980). We also measured ROM and evaluated joint-play in order to detect loss of active and passive range of motion (i.e., frozen shoulder, severe cases of arthritis, arthroses) was conducted. The clinical examination was carried out by the same physical therapist, with more than 20 years of clinical experience.
Diagnostic Ultrasound
For diagnostic purposes, the reliability and quality of US findings is highly dependent on the experience and skill of the investigator (Teefey et al., Citation2004). Therefore, a biomedical technician with a PhD in musculoskeletal US and 20 years of experience of US, performed all US examinations. Two different US machines were used (ACUSON AntaresTM and ACUSON S1000TM; Siemens Medical Solutions, USA), both equipped with high resolution Multi-D matrix transducers – WFX 13–5 (5–13 MHz) or 14L5 (5–14 MHz). The sonographic evaluation of the rotator cuff was performed in all patients according to a standardized protocol, the same that was thoroughly described by Vlychou et al. (Citation2009). A total tear was defined as a complete release of the tendon, a FTT as a tear that extends from the bursal to the articular surface and a partial-thickness tear (PTT) as a defect within the tendon, in either the longitudinal or the transverse plane.
During the US examinations the patients were seated on a swivel chair with a low backboard, and the examiner was standing behind the patient. The tendons of supraspinatus, subscapularis, infraspinatus and the long head of biceps were visualized in both a longitudinal and transversal plane. Both the tendons of subscapularis and infraspinatus were evaluated dynamically during internal and external rotation with the forearm in supination and the elbow in 90° of flexion. The acromioclavicular joint was evaluated in terms of possible sprains and osteoarthritis. The supraspinatus tendon and the subdeltoid/subacromial bursae were evaluated dynamically during abduction with the arm slightly internally rotated. The supraspinatus tendon was examined with the patient’s palm placed on the posterior region of the iliac wing with the elbow flexed and directed posteriorly. The US examiner was blinded to arm dominance, the patient´s symptom as well as to the purpose of the study.
Statistical Analysis
Statistical analyses were conducted using TIBCO Statistica® 13.4.0 and Excel 2016. All variables were summarized using standard descriptive statistics such as frequency, percent, mean and standard deviation. Chi2 (with Yates corrected Chi2 when appropriate) or Fisher's exact test, was used comparing the symptomatic and asymptomatic shoulder. The total number of US findings and bilateral findings in the age intervals; 20–29 years, 30–39 years, 40–49 years and 50–59 years, were presented and compared using Kruskal Wallis ANOVA. If differences were found, Mann Whitney U-test and Chi2 or Fisher's exact test was used to find out where the differences were. The significance level was set at p ≤ 0.05 (two-tailed).
RESULTS
Structural Abnormalities
US findings of structural abnormalities were present in both shoulders in patients with unilateral SAPS (). Bursitis was the most common US finding in all age groups, 90% in the symptomatic shoulder and 74% in the asymptomatic shoulder (p = .0021) (). Partial-thickness tears of the rotator cuff was found in 40% of the symptomatic shoulder and 17% of the asymptomatic shoulder (p = .0001) (). Twelve percent of the patients had ruptures in more than one tendon of the symptomatic shoulder when compared to 3.5% of the asymptomatic shoulder (p = .0247) (). Partial-thickness tears of the supraspinatus tendon was twice as common in the symptomatic shoulder when compared to the asymptomatic shoulder, 30% and 14%, respectively (p = .0026) (). Tendinosis of the rotator cuff was present in 29% of the symptomatic shoulder and 12% of the asymptomatic shoulder (p = .0019) (). Supraspinatus was found to be the most common muscle in terms of tendinosis, 24% of the symptomatic shoulder and 10% of the asymptomatic shoulder (p = .0054) (). Synovitis of the symptomatic shoulder (long head of biceps) was more common than of the asymptomatic shoulder, 16.5%, and 6%, respectively (p = .0220) (). There were fewer total structural abnormalities in the age group 20–29 years (A), compared to the other age groups (B, C, and D) (p = . 0004) ().
Table 1. Ultrasound findings of structural abnormalities in 115 patients with unilateral subacromial pain syndrome.
Table 2. Ultrasound findings by age group.
Table 3.. Detailed ultrasound findings of structural abnormalities in 115 patients with unilateral subacromial pain syndrome..
Bilateral Ultrasound Findings
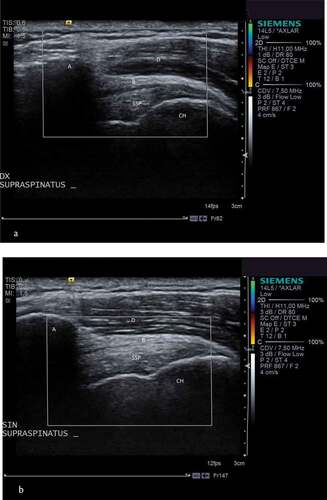
Out of the 115 patients, 84 patients (73%) had bilateral bursitis and 18 patients (15, 6%) presented with bilateral partial-thickness tears of the rotator cuff, 12 patients (10.4%) with bilateral calcification and 10 patients (8, 7%) with bilateral tendinosis (). In patients 30 years and older 73% of the bursitis, 39% of the partial-thickness tears, 10.4% of the calcifications, and 8.7% of the tendinosis were bilateral (). Three patients (2.6%) did not have any abnormalities in any of their shoulders. Bilateral abnormal US findings in five “typical” patients with unilateral SAPS are shown in -.
Table 4. Bilateral ultrasound findings of structural abnormalities in 115 patients with unilateral subacromial pain syndrome, presented in age intervals.
Figure 1. A and b. Ultrasound of both shoulders in a 43 year old female patient with unilateral subacromial pain syndrome.
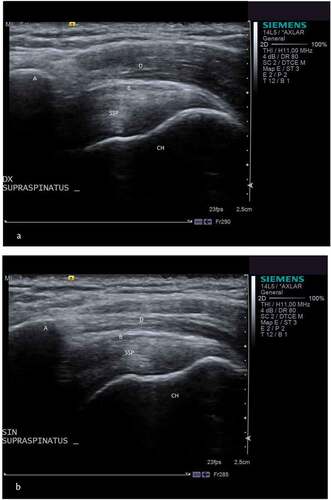
Figure 2. A and b. Ultrasound of both shoulders in a 48 year old female patient with unilateral subacromial pain syndrome.

Figure 3. A and b. Ultrasound of both shoulders in a 33 year old male patient with unilateral subacromial pain syndrome.

Figure 4. A and b. Ultrasound of both shoulders in a 42 year old male patient with unilateral subacromial pain syndrome.
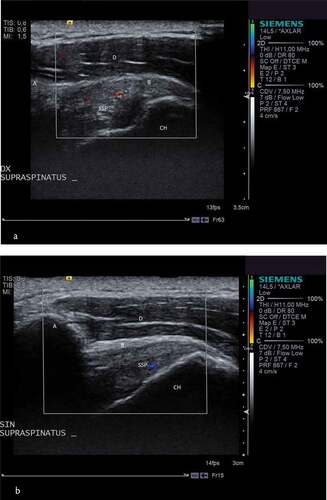
Figure 5. A and b. Ultrasound of both shoulders in a 53 year old male patient with unilateral subacromial pain syndrome.
DISCUSSION
The most important finding of the present study was the amount of bilateral findings in patients diagnosed with unilateral subacromial pain syndrome (SAPS). The findings were more prevalent in the symptomatic shoulder compared to the asymptomatic shoulder and this was particularly evident regarding bursitis and partial thickness tears. More than half of the patients in the present study (age group 30–59 years) presented with PTTs´ in their symptomatic shoulder. From a clinical perspective, this is important knowledge, especially knowing that patients seeking primary care frequently are offered corticosteroid injections as a treatment option. A tear of the rotator cuff is considered to be a contraindication for corticosteroid injections (Dean et al., Citation2014; Puzzitiello et al., Citation2020), and thus, when a corticosteroid injection is the planned treatment, a diagnostic US is a valuable recommendation.
Despite the fact that bursitis and PTTs were more evident in the affected shoulder, abnormalities were found in almost 90% of the patients´ asymptomatic shoulder. This high rate is in concert with a detailed description of US findings in asymptomatic shoulders in males (Girish et al., Citation2011). They reported abnormalities in 96% of their patients with the most common finding being bursal thickening. This is similar to the present study, where bursitis was shown in 90% of the symptomatic shoulder and 74% of the asymptomatic shoulder. The subacromial bursa has been suggested to play a key role when it comes to generate pain in patients with SAPS (Chillemi et al., Citation2016; Rahme, Nordgren, Hamberg, and Westerberg, Citation1993). Although, yet not proven, presence of neovascularity has been mentioned as another theory of pain (Lewis et al., Citation2009).
In the present study, 51.3% of the patients aged 30–59 years presented with partial-thickness tears of their symptomatic shoulder and 25.2% of their asymptomatic shoulder. This is in line with two recent publications reporting a rotator cuff tear in one shoulder to be a risk factor for the presence of a rotator cuff tear in the contralateral shoulder (Ranebo, Bjornsson Hallgren, and Adolfsson, Citation2018; Ro et al., Citation2015).
Hallgren et al. (Citation2014) reported the percentage of patients with partial-thickness tears and full-thickness tears of the rotator cuff to be 22% and 9%, respectively in the symptomatic shoulder. In the present study, almost twice as many patients (40%) presented with partial-thickness tears of the rotator cuff when compared to solely 1.7% with full-thickness tears and total ruptures (). The low prevalence of full-thickness tears and total ruptures in the present study might be due to the fact that patients with lag signs were excluded from the study. Furthermore, the patient´s in the present study also had a lower mean age and were not on a waiting list for surgery. Non-traumatic partial-thickness tears have been suggested to be a natural part of aging (Milgrom, Schaffler, Gilbert, and van Holsbeeck, Citation1995; Moosmayer, Smith, Tariq, and Larmo, Citation2009).
The supraspinatus muscle was the most vulnerable tendon of the rotator cuff in the symptomatic shoulder in terms of partial-thickness tears, tendinosis, as well as calcification. This was also the case when it comes to the asymptomatic shoulder although not of the same magnitude. The vulnerability of the supraspinatus muscle in patients with SAPS, found in the present study has been known for long and also recently reported in other US publications (Jobe and Moynes, Citation1982; Rodríguez-Piñero Durán, Vidal Vargas, and Castro Agudo, Citation2019).
Today, US has become increasingly common within physical therapy clinics (Kooijman et al., Citation2020) in diagnosing shoulder pain. However, several authors are questioning the patho-anatomical diagnostic approach when diagnosing SAPS (Cook, Rio, Purdam, and Docking, Citation2016; Lewis, Citation2009). Other authors still suggest that an US examination of patients with shoulder pain might be a useful tool to distinguish between the pathologic patterns in order to choose the optimal treatment (Tran et al., Citation2017). There are poor associations between symptoms in patients with SAPS and pathological US or MRI findings (Guzowski et al., Citation2019; Lewis, Citation2009). This might be due to the fact that imaginary findings are somewhat hard to interpret clinically and many individuals in the general population also present with abnormal findings of their asymptomatic shoulder, increasing with age (Barreto et al., Citation2019; Milgrom, Schaffler, Gilbert, and van Holsbeeck, Citation1995; Tempelhof, Rupp, and Seil, Citation1999). Approximately two-thirds of patients with rotator cuff tears do not complain of any symptoms (Yamamoto et al., Citation2011). Due to the fact that several findings are bilateral, it might be a good idea to include exercises bilaterally; however, this is yet to be studied in a clinical trial.
Considering the current knowledge, it is of utmost importance to explain to our patients that patho-anatomical changes does not always lead to symptoms, and that structural changes, including tears may be part of expected degeneration. Today, if a rupture of any sort is revealed, it is not uncommon for practitioners and patients to warrant a referral to an orthopedic clinic, instead of starting graded exercise, which is consensus for the physiotherapy treatment (Klintberg et al., Citation2015). For this group of patients surgical intervention is unnecessary and also correlated to significantly greater costs for the society than physiotherapy (Ketola et al., Citation2013). In concert with previous studies, the present study showed that US findings in terms of diagnosing patients with non-traumatic shoulder pain should not be used as the only diagnostic tool (Guzowski et al., Citation2019; Moosmayer, Smith, Tariq, and Larmo, Citation2009).
Study Limitations and Strengths
A limitation of the present investigation was lack of grading the pathology, which would have been valuable in order to compare the symptomatic and asymptomatic shoulder. The strength of the present study was the large sample size. Another strength was the thorough clinical examination performed before the US examination in order to rule out total rotator cuff tears and other symptoms not compatible with SAPS. A further strength was the blinded diagnostic US examination, following a standardized protocol, and performed by one expert within the field of musculoskeletal US. This minimizes the risk of misinterpretation of the diagnostic US.
CONCLUSION
Patients with unilateral SAPS presented with a number of abnormal US findings in both their symptomatic and asymptomatic shoulder. Most abnormalities were present in the symptomatic shoulder, which might explain the pain reported by the patients in solely their symptomatic shoulder. It is important to design treatment not only based on the imaginary findings, but also to take into account the patient´s history, complaints, and the results of a clinical examination. However, before the decision to treat the patient with a corticosteroid injection, a diagnostic US could be valuable in order to rule out partially thick tears.
Acknowledgments
The authors are grateful for the participating primary care centres and their SAPS patients, without whom this study could not have been conducted.
Disclosure Statement
No competing interest.
References
- Abate M, Schiavone C, Salini V, Andia I 2013 Management of limited joint mobility in diabetic patients. Diabetes Metabolic Syndrome and Obesity 6: 197–207. 10.2147/DMSO.S33943
- Alqunaee M, Galvin R, Fahey T 2012 Diagnostic accuracy of clinical tests for subacromial impingement syndrome: A systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation 93: 229–236. 2 10.1016/j.apmr.2011.08.035
- Bak K, Sørensen AK, Jørgensen U, Nygaard M, Krarup AL, Thune C, Sloth C, Pedersen ST 2010 The value of clinical tests in acute full-thickness tears of the supraspinatus tendon: Does a subacromial lidocaine injection help in the clinical diagnosis? A prospective study. Arthroscopy 26: 734–742. 6 10.1016/j.arthro.2009.11.005
- Barreto RP, Braman JP, Ludewig PM, Ribeiro LP, Camargo PR 2019 Bilateral magnetic resonance imaging findings in individuals with unilateral shoulder pain. Journal of Shoulder and Elbow Surgery 28: 1699–1706. 9 10.1016/j.jse.2019.04.001
- Calis M, Akgun K, Birtane M, Karacan I, Calis H, Tuzun F 2000 Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Annals of the Rheumatic Diseases 59: 44–47. 1 10.1136/ard.59.1.44
- Carbone S, Gumina S, Arceri V, Campagna V, Fagnani C, Postacchini F 2012 The impact of preoperative smoking habit on rotator cuff tear: Cigarette smoking influences rotator cuff tear sizes. Journal of Shoulder and Elbow Surgery 21: 56–60. 1 10.1016/j.jse.2011.01.039
- Chauhan NS, Ahluwalia A, Sharma YP, Thakur L 2016 A prospective comparative study of high resolution ultrasound and MRI in the diagnosis of rotator cuff tears in a tertiary hospital of north India. Polish Journal of Radiology 81: 491–497. 10.12659/PJR.897830
- Chillemi C, Petrozza V, Franceschini V, Garro L, Pacchiarotti A, Porta N, Cirenza M, Salate Santone F, Castagna A 2016 The role of tendon and subacromial bursa in rotator cuff tear pain: A clinical and histopathological study. Knee Surgery, Sports Traumatology, Arthroscopy 24: 3779–3786. 12 10.1007/s00167-015-3650-4
- Chiu YH, Chang KV, Chen IJ, Wu WT, Özçakar L 2020 Utility of sonoelastography for the evaluation of rotator cuff tendon and pertinent disorders: A systematic review and meta-analysis. European Radiology 30: 6663–6672. 12 10.1007/s00330-020-07059-2
- Cook JL, Rio E, Purdam CR, Docking SI 2016 Revisiting the continuum model of tendon pathology: What is its merit in clinical practice and research? British Journal of Sports Medicine 50: 1187–1191. 19 10.1136/bjsports-2015-095422
- Dean BJ, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ 2014 The risks and benefits of glucocorticoid treatment for tendinopathy: A systematic review of the effects of local glucocorticoid on tendon. Seminars in Arthritis and Rheumatism 43: 570–576.
- Gerber C, Krushell RJ 1991 Isolated rupture of the tendon of the subscapularis muscle. Clinical features in 16 cases. Journal of Bone and Joint Surgery (Br) 73: 389–394. doi:10.2106/00004623-199607000-00005; PMID:8698718
- Girish G, Lobo L, Jacobson J, Morag Y, Miller B, Jamadar D 2011 Ultrasound of the shoulder: Asymptomatic findings in men. American Journal of Roentgenology 197: W713–W719. 4 10.2214/AJR.11.6971
- Guzowski K, Stolarczyk A, Czyrny Z, Debek A, Kranc B 2019 Assessment of ultrasonography as a diagnostic tool in shoulder pain and alterations in glenohumeral range of motion in tennis players. Videosurgery and Other Miniinvasive Techniques 14: 114–125. 1 10.5114/wiitm.2018.81183
- Hallgren HC, Holmgren T, Oberg B, Johansson K, Adolfsson LE 2014 A specific exercise strategy reduced the need for surgery in subacromial pain patients. British Journal of Sports Medicine 48: 1431–1436. 19 10.1136/bjsports-2013-093233
- Hawkins RJ, Kennedy JC 1980 Impingement syndrome in athletes. American Journal of Sports Medicine 8: 151–158. 3 10.1177/036354658000800302
- Hegedus EJ, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman CT, Cook C 2008 Physical examination tests of the shoulder: A systematic review with meta-analysis of individual tests. British Journal of Sports Medicine 42: 80–92. 2 10.1136/bjsm.2007.038406
- Hertel R, Ballmer FT, Lombert SM, Gerber C 1996 Lag signs in the diagnosis of rotator cuff rupture. Journal of Shoulder and Elbow Surgery 5: 307–313. 4 10.1016/S1058-2746(96)80058-9
- Jobe FW, Jobe CM 1983 Painful athletic injuries of the shoulder. Clinical Orthopaedics and Related Research: 117–124. doi:10.1177/036354658201000602
- Jobe FW, Moynes DR 1982 Delineation of diagnostic criteria and a rehabilitation program for rotator cuff injuries. American Journal of Sports Medicine 10: 336–339. 6 10.1177/036354658201000602
- Kelly SM, Brittle N, Allen GM 2010 The value of physical tests for subacromial impingement syndrome: A study of diagnostic accuracy. Clinical Rehabilitation 24: 149–158. 2 10.1177/0269215509346103
- Kessel L, Watson M 1977 The painful arc syndrome. Clinical classification as a guide to manage-ment. Journal of Bone and Joint Surgery (Br) 59: 166–172. 2 10.1302/0301-620X.59B2.873977
- Ketola S, Lehtinen J, Rousi T, Nissinen M, Huhtala H, Konttinen Y, Arnala I 2013 No evidence of long-term benefits of arthroscopicacromioplasty in the treatment of shoulder impingement syndrome: Five-year results of a randomised controlled trial. Bone & Joint Research 2: 132–139. 7 10.1302/2046-3758.27.2000163
- Kibler WB, Ludewig PM, McClure PW, Michener LA, Bak K, Sciascia AD 2013 Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘Scapular Summit.’ British Journal of Sports Medicine 47: 877–885. 14 10.1136/bjsports-2013-092425
- Klintberg IH, Cools AM, Holmgren TM, Holzhausen AC, Johansson K, Maenhout AG, Moser JS, Spunton V, Ginn K 2015 Consensus for physiotherapy for shoulder pain. International Orthopaedics 39: 715–720. 4 10.1007/s00264-014-2639-9
- Kooijman MK, Swinkels IC, Koes BW, de Bakker D, Veenhof C 2020 One in six physiotherapy practices in primary care offer musculoskeletal ultrasound - an explorative survey. BMC Health Services Research 20: 246. 1 10.1186/s12913-020-05119-3
- Lewis JS 2009 Rotator cuff tendinopathy/subacromial impingement syndrome: Is it time for a new method of assessment? British Journal of Sports Medicine 43: 259–264. 4 10.1136/bjsm.2008.052183
- Lewis JS, Raza SA, Pilcher J, Heron C, Poloniecki JD 2009 The prevalence of neovascularity in patients clinically diagnosed with rotator cuff tendinopathy. BMC Musculoskeletal Disorders 10: 163. 1 10.1186/1471-2474-10-163
- Lewis JS, Wright C, Green A 2005 Subacromial impingement syndrome: The effect of changing posture on shoulder range of movement. Journal of Orthopaedic and Sports Physical Therapy 35: 72–87. 2 10.2519/jospt.2005.35.2.72
- May S, Chance-Larsen K, Littlewood C, Lomas D, Saad M 2010 Reliability of physical examination tests used in the assessment of patients with shoulder problems: A systematic review. Physiotherapy 96: 179–190. 3 10.1016/j.physio.2009.12.002
- Michener LA, Walsworth MK, Doukas WC, Murphy KP 2009 Reliability and diagnostic accuracy of 5 physical examination tests and combination of tests for subacromial impingement. Archives of Physical Medicine and Rehabilitation 90: 1898–1903. 11 10.1016/j.apmr.2009.05.015
- Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M 1995 Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. Journal of Bone and Joint Surgery (Br) 77: 296–298.
- Mitchell C, Adebajo A, Hay E, Carr A 2005 Shoulder pain: Diagnosis and management in primary care. British Medical Journal 331: 1124–1128. 7525 10.1136/bmj.331.7525.1124
- Moosmayer S, Smith HJ, Tariq R, Larmo A 2009 Prevalence and characteristics of asymptomatic tears of the rotator cuff: An ultrasonographic and clinical study. Journal of Bone and Joint Surgery (Br) 91: 196–200. 2 10.1302/0301-620X.91B2.21069
- Naredo E, Aguado P, De Miguel E, Uson J, Mayordomo L, Gijon-Baños J, Martin-Mola E 2002 Painful shoulder: Comparison of physical examination and ultrasonographic findings. Annals of the Rheumatic Diseases 61: 132–136. 2 10.1136/ard.61.2.132
- Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG 2005 Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. Journal of Bone and Joint Surgery (Am) 87: 1446–1455.
- Puzzitiello RN, Patel BH, Nwachukwu BU, Allen AA, Forsythe B, Salzler MJ 2020 Adverse impact of corticosteroid injection on rotator cuff tendon health and repair: A systematic review. Arthroscopy: The Journal of Arthroscopic & Related Surgery 36: 1468–1475. 5 10.1016/j.arthro.2019.12.006
- Rahme H, Nordgren H, Hamberg H, Westerberg C 1993 The subacromial bursa and the impingement syndrome. A clinical and histological study of 30 cases. Acta Orthopaedica Scandinavia 64: 485–488.
- Ranebo M, Bjornsson Hallgren H, Adolfsson L 2018 Patients with a long-standing cuff tear in one shoulder have high rates of contralateral cuff tears: A study of patients with arthro-scopically verified cuff tears 22 years ago. Journal of Shoulder and Elbow Surgery 27: e68–e74. 3 10.1016/j.jse.2017.10.007
- Ro KH, Park J, Lee S, Song D, Jeong H, Jeong W 2015 Status of the contralateral rotator cuff in patients undergoing rotator cuff repair. American Journal of Sports Medicine 43: 1091–1098. 5 10.1177/0363546515571554
- Rodríguez-Piñero Durán M, Vidal Vargas V, Castro Agudo M 2019 Ultrasound findings in chronic subacromial pain syndrome. Rehabilitacion 53: 240–246. 4 10.1016/j.rh.2019.06.002
- Schellingerhout JM, Verhagen AP, Thomas S, Koes BW 2008 Lack of uniformity in diagnostic labeling of shoulder pain: Time for a different approach. Manual Therapy 13: 478–483. 6 10.1016/j.math.2008.04.005
- Seitz AL, McClure PW, Finucane S, Boardman ND, Michener LA 2011 Mechanisms of rotator cuff tendinopathy: Intrinsic, extrinsic, Or Both? Clinical Biomechanics 26: 1–12. 1 10.1016/j.clinbiomech.2010.08.001
- Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, Yamaguchi K 2004 Detection and quantification of rotator cuff tears. Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. Journal of Bone and Joint Surgery (Am) 86: 708–716. 4 10.2106/00004623-200404000-00007
- Tempelhof S, Rupp S, Seil R 1999 Age-related prevalence of rotator cuff tears in asymptomatic shoulders. Journal of Shoulder and Elbow Surgery 8: 296–299. 4 10.1016/S1058-2746(99)90148-9
- Tran G, Hensor EM, Ray A, Kingsbury SR, O’Connor P, Conaghan PG 2017 Ultrasound-detected pathologies cluster into groups with different clinical outcomes: Data from 3000 community referrals for shoulder pain. Arthritis Research & Therapy 19: 30. 1 10.1186/s13075-017-1235-y
- Tsai YH, Huang TJ, Hsu WH, Huang KC, Li YY, Peng KT, Hsu RW 2007 Detection of subacromial bursa thickening by sonography in shoulder impingement syndrome. Chang Gung Medical Journal 30: 135–141.
- Tyler TF, Nicholas SJ, Roy T, Gleim GW 2000 Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. American Journal of Sports Medicine 28: 668–673. 5 10.1177/03635465000280050801
- Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, Simmons A, Williams G 1998 Estimating the burden of musculoskeletal disorders in the community: The comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Annals of Rheumatic Diseases 57: 649–655. 11 10.1136/ard.57.11.649
- Vlychou M, Dailiana Z, Fotiadou A, Papanagiotou M, Fezoulidis IV, Malizos K 2009 Symptomatic partial rotator cuff tears: Diagnostic performance of ultrasound and magnetic resonance imaging with surgical correlation. Acta Radiologica 50: 101–105.
- Yamaguchi K, Ditsios K, Middleton WD, Hildebolt CF, Galatz LM, Teefey SA 2006 The demographic and morphological features of rotator cuff disease. A comparison of asymptomatic and symptomatic shoulders. Journal of Bone and Joint Surgery (Am) 88: 1699–1704. 8 10.2106/00004623-200608000-00002
- Yamamoto A, Takagishi K, Kobayashi T, Shitara H, Osawa T 2011 Factors involved in the presence of symptoms associated with rotator cuff tears: A comparison of asymptomatic and symptomatic rotator cuff tears in the general population. Journal of Shoulder and Elbow Surgery 20: 1133–1137. 7 10.1016/j.jse.2011.01.011
- Yamamoto A, Takagishi K, Osawa T, Yanagawa T, Nakajima D, Shitara H, Kobayashi T 2010 Prevalence and risk factors of a rotator cuff tear in the general population. Journal of Shoulder and Elbow Surgery 19: 116–120. 1 10.1016/j.jse.2009.04.006