ABSTRACT
Background and Introduction
Rapid Response Teams (RRTs) are multidisciplinary, ‘hospital at home’ services which have developed over the last 10 years, aiming to improve recovery from illness more efficiently, prevent unnecessary hospital admission, and prevent early admission to residential care. However, little is known about the experience of professionals working in these roles.
Purpose
The aim of this study was to explore how working in an RRT is experienced and perceived by physiotherapists.
Methods
This study used phenomenographically inspired methodology. Six participants who were working in RRTs were recruited to this study and all were working in the South of England. Data were collected via semi-structured interviews, and phenomenographic analysis was undertaken.
Results
Participants working in RRTs described a range of varied, concrete lived-through experiences in addition to a more rhetorical discussion of how they conceptualized their work. Six main categories of description were generated from the analysis; each was assigned a metaphor. These included ‘the detective,’ ‘the guru,’ ‘the lone ranger,’ ‘the team player,’ ‘the bricoleur,’ and ‘an emotional rollercoaster’; all categories were present with varied meanings. ‘An emotional rollercoaster’ was present within and throughout participants’ descriptions of all other categories.
Conclusion
This study provides valuable insights into physiotherapists’ experience and conceptualization of working within this discipline, which may have implications for physiotherapy practice, workforce development, new and current RR physiotherapy services, RRT health professionals, and physiotherapy education.
Introduction
In the last decade, the National Health Service (NHS) has struggled to meet the health demands of the population (Addicott, Maguire, Honeyman, and Jabbal, Citation2015; Gilburt, Citation2016). For instance, emergency departments (EDs) have seen a dramatic increase in attendance and admissions, with admissions increasing faster than the population, identifying that there were 69 emergency admissions per 1000 of the population in 2011/2012 (Blunt, Bardsley, and Dixon, Citation2010) and 77.1 per 1000 in 2016/2017 (Baker, Citation2017). EDs in the United Kingdom (UK) are required to meet a target, whereby 95% of patients need to be assessed, treated, and discharged within a four-hour target (Department of Health, Citation2015; Evans, Citation2017); however, only 85.1% of EDs are achieving this (NHS England, Citation2013). In 2017, 2.5 million waited longer than 4 hours (Murray et al., Citation2017). This increase in demand on NHS acute services is impacted by more individuals living with chronic and complex illness (Addicott, Maguire, Honeyman, and Jabbal, Citation2015) and an aging population (Centre for Workforce Intelligence, Citation2011; Department of Health, Citation2015). There are 12 million people over the age of 65 in the UK, and four million are living with long-term conditions (Age, Citation2019) requiring health intervention in acute and community settings (Office for National Statistics, Citation2013). Evidence has confirmed that unnecessary admission can cause significant health detriment such as deconditioning; increased risk of hospital acquired infection; institutionalization; and disorientation (Mendes, Rodrigues, Preto, and Novo, Citation2016; Mudge et al., Citation2017; Oliver, Foot, and Humphries, Citation2014) potentially leading to longer hospital stays, further deterioration in health, and increased costs to the healthcare system. The upshot is an unprecedented extra strain on clinical resources (Addicott, Maguire, Honeyman, and Jabbal, Citation2015) costing the NHS an estimated additional £13.5 billion a year (Department of Health, Citation2015).
In response to this crisis, health and social care have required substantial reconfiguration (Gilburt, Citation2016) and the NHS workforce has adjusted to provide innovative solutions. One strategy has been to move care away from hospitals, and closer to home (King’s Fund, Citation2015; NHS England, Citation2014; Nuffield Trust, Citation2017) by developing services that integrate health and social care (e.g., community integrated rapid response team (RRT)). The RRT is a multi-professional approach to ‘hospital at home’ and is a relatively new service within the NHS in the UK which may include physiotherapists, occupational therapists, nurses, GPs, social workers, rehabilitation assistants, and pharmacists. RRTs provide an immediate response, at home, to individuals with acute complex health care needs aiming to improve recovery, prevent unnecessary hospital admission, and delay admission to residential care (Clift, Citation2015; NHS Benchmarking Network, Citation2013; Stevenson and Spencer, Citation2002). The ‘Long Term Plan’ (NHS England, Citation2019) has confirmed further support to develop additional RRTs to continue to keep patients out of hospital, promising £4.5 billion in funding to primary care. For many health professionals such as physiotherapists, this commitment to move more care to the community has meant new roles, ways of working, and clinical environments.
This study focuses on the physiotherapy profession specifically, and the perception and experience of physiotherapists working within community RRTs. To date, the literature investigating avoidable admission teams like the RRT is predominantly quantitative, and the main focus of research has been to evaluate the impact of the whole team rather than consider individual roles, for example, whether RRTs are cost effective, safe, can reduce avoidable adult admissions, and provide patient satisfaction. Literature undertaken in the UK, Australia, Italy, and New Zealand that has reviewed avoidable admission teams such RRTs and hospital at home teams, has shown that they can improve patient satisfaction, reduce readmission and mortality rates (Caplan et al., Citation2012; Facultad and Lee, Citation2019; Lee, Pickstone, Facultad, and Titchener, Citation2017; Lee and Titchener, Citation2017; Montalto, Citation2010; Montalto, Lui, Mullins, and Woodmason, Citation2010; Shepperd et al., Citation2009; Varney, Weiland, and Jelinek, Citation2014; Wilson et al., Citation1999). Although physiotherapists have been working in avoidable admission and hospital at home services such as the RRT for over a decade, little is known about their experience of working within this discipline. The qualitative evidence exploring the RRT and the experiences of clinicians working in this field, as well as patients receiving care from these teams, is scarce. These insights will add a rich understanding of working in these teams, which may inform successful implementation of RRTs in practice. Thus, to address this gap in the literature, this study aims to explore how working in an RRT is experienced and perceived by physiotherapists.
Method
Methodology and study design
This interpretive qualitative study used a phenomenographic approach (Giorgi, Citation1999; Marton, Dahlgren, Svensson, and Säljö, Citation1977; Marton and Svensson, Citation1979; Säljö, Citation1979). Phenomenography seeks to discover variances in the way individuals experience and understand phenomena in the world they live in (Barnard, McCosker, and Gerber, Citation1999; Larsson and Holmström, Citation2007). It is concerned with describing how things appear to, and are experienced by, individuals (Pang, Citation2003). Phenomenography sits within an interpretivist paradigm (Cibangu and Hepworth, Citation2016) recognizing that there are many ways of interpreting reality. Ontologically phenomenography is based on a nondualist world view, in which there is just one world, and it is that world which is experienced (Åkerlind, Citation2012; Marton, Citation1981; Sin, Citation2010). In this non-dualist view, ‘the internal’ (i.e. thinking) and the ‘external’ (i.e. the world or activity) are not seen as isolated entities’ (Svensson, Citation1997). Epistemologically phenomenography employs a ‘second order’ perspective which focuses on individual’s experiences of a phenomenon. Specifically, analysis focuses on ‘what’ is the focus of attention and ‘how’ it is experienced or perceived by an individual (Yates, Partridge, and Bruce, Citation2012). Thus, phenomenography offers great value as an approach for researching healthcare (Holmström, Halford, and Rosenqvist, Citation2003). Recognizing how healthcare phenomena are understood and experienced by clinicians, patients, and providers, is vital to help improve, shape, and develop efficient and effective future healthcare practice (Barnard, McCosker, and Gerber, Citation1999; Larsson and Holmström, Citation2007). For this reason, a phenomenographically inspired approach was appropriate for this specific study, which aimed to explore a new healthcare phenomenon; physiotherapists’ experiences and perceptions of working in an RRT as conceptualized by the therapists themselves.
Sampling and participant recruitment
Purposive sampling was used to recruit 6 participants, who had at least 12 months’ experience of working in an RRT in the UK. Purposive sampling was chosen to provide the best chance of revealing the various experiences and perspectives of the phenomenon (Braun and Clarke, Citation2013; Creswell and Poth, Citation2009) and is commonly used in phenomenography (Yates, Partridge, and Bruce, Citation2012). There is no prescriptive number of participants suggested for phenomenographic studies (Yates, Partridge, and Bruce, Citation2012) but in common with other qualitative research includes a small number of participants, seeking to elicit rich (thick) descriptions, and aiming for a deeper analysis of the data (Braun and Clarke, Citation2013). Participant volunteers were recruited via the Chartered Society of Physiotherapy (CSP) using their website by posting a research invitation on relevant Interactive CSP (iCSP) web pages. All participants were provided with an information sheet and asked to complete a consent form before participating. Ethical approval was granted by the Health and Social Science, Science and Engineering Research Ethics and Governance Committee at the University of Brighton in November 2015.
Details of the six participants can be found in . Due to the small number of physiotherapists in RRT roles, further information on participants is not included due to a risk of compromising their anonymity.
Table 1. Participant characteristics.
Data collection
Data was collected through semi-structured interviews via Skype or face-to-face (depending on participant choice) and lasted between 40 and 80 minutes. All interviews were audio recorded and transcribed, and participants were anonymized by number. Face-to-face interviews occurred in a location convenient to the participant in a private room. The participants were asked to discuss their experience of working in an RRT in as much detail as possible, and encouraged to speak freely about their experiences. The interview was initiated by asking the question: ‘Can you tell me in as much detail as possible about your experience of working in a rapid response team?’. Although the researcher allowed the participant to lead the direction of the interview and the content discussed, prompts were used to encourage participants to engage and aid elaboration of any meaningful situations. For example, prompts included ‘Can you tell me a little bit more about that experience?‘ and ’can you give me an example of what that was like?’
Data analysis
This study has followed an idiographic phenomenographic analysis process guided by Larsson and Holmström (Citation2007) (). Each transcript was initially read twice to get a sense of the whole (step 1) and then divided into meaning units (step 2). Phenomenographic analysis is an iterative process whereby the researcher engages in dialog with the text, trying not to predict any outcomes (Åkerlind, Citation2005). To aid this process, the main researcher kept a reflexive diary. Notes were made during this process, specifically on the participants’ focus of attention, what this was on, and how they described their way of working, and therefore the phenomenon (step 3). Initial descriptions of participants’ understandings were made, and these were grouped into categories constructed on similarities and differences. Connected or related statements were grouped into dimensions of variation. Quotes were arranged into piles, uncertain cases were reviewed, and eventually the criterion characteristics for each group were made explicit (Åkerlind, Citation2005) (step 4). Next, these were developed into descriptive categories of meaning and were assigned metaphors (step 5). The descriptive categories were then arranged into an outcome space (step 6). The relationships and any hierarchies between categories were considered, as well as non-dominant ways of understanding (step 7). The steps of the analysis are further illustrated in the Appendix.
Table 2. Steps of the phenomenographic analysis (Larsson and Holmström, Citation2007).
The first author, an advanced practitioner physiotherapist with postgraduate training in research undertook the analysis, and the second author, an experienced researcher, musculoskeletal physiotherapist, and academic acted as co-reader, providing dialogic discussion and alternative interpretations of meaning, findings, the descriptive categories, and final outcome space.
Findings
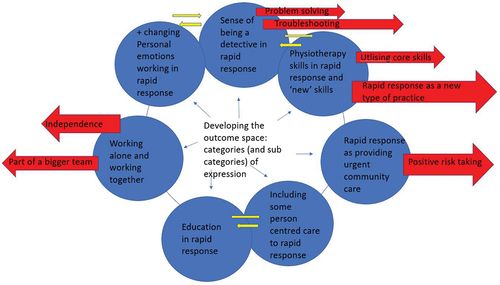
Six categories of description were generated from the analysis of the participants’ accounts of their experiences, and these categories were present with varied meaning. Each category was assigned a metaphor to illustrate understanding and meaning relating to working in an RRT. These were as follows: 1) ‘the Detective’; 2) ‘the Guru’; 3) ‘the Lone Ranger’; 4) ‘the Team Player’; 5) ‘the Bricoleur’; and 6) ‘an emotional roller coaster’ (). The category ‘an emotional rollercoaster’ intertwines with the five other categories of description, which were derived from various, but equally important, conceptions. As the ‘emotional roller coaster’ category was present throughout participants’ descriptions of all categories, this will be discussed throughout and not separately as is illustrated in the outcome space ().
Figure 1. The outcome space.

Table 3. Descriptive categories.
The detective
The metaphor ‘the Detective’ illustrates that participants conceptualized working in an RRT as investigative work. This category was characterized by descriptions of clinical assessment, utilizing knowledge, reasoning, and problem solving. To be ‘a detective,’ participants described the act of reviewing a wide spectrum of clinical information gained through history taking (including an attention to current symptoms), physical assessment, and specific test results.
… in this rapid response setting, oh yeah there’s quite a broad range of answers, and having a broad spectrum of advanced knowledge helps us to … decide on our next steps (P1)
They perceived this information facilitated problem solving and clinical decision-making to aid diagnosis/and or formulation of a treatment plan. Within their descriptions was a perception that in the RR setting, these detective skills need to be broader and more advanced than those required in other settings requiring additional training and yet recognition that the investigative tools at their disposal were not always adequate.
… we took the observations … her blood pressure was very high, and temperature … and we did check the urine … all the ketones and nitrates and we did not notice an underlying infection … presenting with symptoms like confusion and drowsiness … we had to send her into the hospital for further investigations to see what exactly the underlying illness turned out to be … (P2)
Participants conveyed the importance of taking a holistic perspective, with their role as a detective involving consideration of broader aspects of health and wellbeing. For some participants, this meant considering the psychosocial factors and for others this also included a broadening of their detective work into domains traditionally considered the work of other health professionals.
… you see the patient from a holistic approach, so not only just for the physio, but you see and assess them for all aspects of health, the nursing, and OT wise and all the social problems … and problem solve and bring a solution for them … (P4)
Participants acknowledged that this detective role is an ‘emotional roller coaster.’ Each participant described a wide and varied range of emotions in relation to their experience. The highs and lows in their accounts of working in an RRT were meaningfully related to the speed needed in their detective work, having to make decisions with uncertain and incomplete information and the potential consequences and responsibility associated with their decision-making.
… very rewarding … because we problem solve, use our clinical knowledge and make these decisions and it made a difference in that man’s life … (P1)
Oh yes, this job does get your heart racing! The nurses say, ‘You always look so calm.’ I say, ‘Yes, I look calm but my heart is really going!’ I think if it’s a life and death situation, I do get a bit nervous, you know, apprehensive, I have to gather information and make decisions quickly, and I can get that butterfly feeling … (P5)
The guru
The term guru is used as it reflects participants’ perceptions of their educational role in an RRT. ‘Guru’ is based on the Sanskrit term (language from ancient India) meaning ‘teacher, guide or expert’ of a certain knowledge or field (Pertz, Citation2007). A guru in the context of RRT will share expert knowledge from their professional experience. This descriptive category was characterized by recognition of their clinical expertise and skills and descriptions of being a guide and educator.
I would say it is exciting, I feel proud of what I am doing, I think I am utilizing whatever knowledge, skill and experience I have gained, still using my physiotherapy expertise to guide others, you know, team members and patients … (P3)
Participants conceptualized a broad educational role with the RRT, involved teaching their colleagues from other disciplines on physiotherapy-specific knowledge and skill, but also educating and guiding their patients and the carers/relatives on their illness and/or management and treatment plan. Participants conveyed a sense of education in this setting as a guiding, facilitatory process moving toward self-management and health promotion.
… being a physiotherapist, we share our knowledge on this team, share with other professionals, teach others about our own clinical knowledge … (P2)
Similarly, another individual spoke to the significance of education as a guiding, facilitatory process.
… education happens quite a lot you know, to educate and guide the patient about their condition or teach them to help themselves and self-manage their condition … (P3)
The lone ranger
The sense of being alone was conveyed as significantly meaningful. Participants’ accounts were dominated by descriptions of experiences in their RRT roles where they visited patients and experienced clinical situations alone, thus they perceived themselves at times to be ‘lone rangers.’ Within this category, they conveyed the importance of clinical experience and knowledge in developing clinical competence and autonomous decision-making.
I have to make the decision on my own … is the patient to stay in the community or go back to the hospital … so here, in this team, I have to think about everything myself, each and every aspect of the patients err situation, their clinical care … . (P4)
Participants conveyed a sense of responsibility when making clinical decisions in ensuring their skills were up to date, the need to be honest about their knowledge, and to work within their scope of practice.
…if I’m in doubt and on my own, or I don’t know what needs to be done next steps, I know when to ask for help … sometimes you know you are presented with a very ill, acutely ill people and err, sometimes it goes a bit beyond the scope … (P3)
They also recognized the importance of developing competence in clinical skills that may normally be otherwise associated with different roles such as nurses or occupational therapists.
… you need to be competent, especially as you are often on your own … so you need to be competent enough to take blood pressure or competent enough to do blood glucose levels … and make decisions etc … (P2)
The ‘emotional roller coaster’ was expressed through varying emotions associated with being ‘a lone ranger.’ As illustrated in the quotes below, emotions ranged from anxiety, uncertainty and a sense of responsibility to confidence in their decision-making abilities.
It’s actually … it’s very challenging, especially as we often work alone … It is a challenge, but again at the same time, how do I put it? I am confident … (P6)
Similarly, another individual spoke to the challenges of working alone.
I feel quite good in myself …, I’m reasonably confident with err, what I do … … … … . It is a feeling of uncertainty as a clinician … we are left alone completely … so sometimes it feels a bit daunting to be taking such huge decisions, just being alone standing there, the patient looking at you, if they have family, everybody is looking at you … (P3)
In contrast to descriptions of lone working, participants’ descriptions revealed examples of team working.
The team player
Contrasting with the sense of being a lone ranger, participants also perceived themselves to be part of a larger team which involved working collaboratively and learning from others. For some participants, the ‘team player’ was about working closely together with colleagues to improve care, whereby it was perceived that by drawing on the skills of everyone in the team, care could be more person-centered.
Now when we sit down or work together as a multi-disciplinary team … The good thing is, when there is more than one of you, you can also have these different ideas … somebody can come up with, ‘What about this?’, and ultimately the care delivered is therefore improved (P6)
Participants perceived that working in a multidisciplinary team offered multiple perspectives, diverse thinking, and nuanced knowledge and skill, thereby affording learning opportunities and contributing to their own professional development.
Yes so more heads are better than one … you’re constantly learning from each other … that is the beauty of working in the multi-disciplinary team (P6)
While the diversity of perspectives offered by the team was considered by some participants ‘beautiful’ and ‘reassuring,’ for others, it was at times a source of frustration. Thus, being a ‘team player’ was described with varying emotions, and once again the ‘an emotional roller coaster’ category is embedded and woven into this category.
… we try to always work together but sometimes this is hard, when people have different thought processes and opinions … sometimes I find this frustrating (P3)
The emotional rollercoaster was also woven through the final category of description: The Bricoleur.
The bricoleur
Bricoleur is a French word that means a handyperson who uses all tools and types of knowledge that are available to complete a job (Kincheloe, Citation2005). The concept of the Bricoleur resonates with participants conceptualization of their role in an RRT. They described their role as an unconventional role that crossed professional boundaries and was not ‘traditional’ physiotherapy as the job went beyond ‘core’ physiotherapy.
I have to be flexible and move away from some of the traditional boundaries of the profession and there is some cross over with other disciplines like occupational therapy … (P1)
As such, they conveyed the importance of gaining and using additional skills and knowledge to facilitate complex clinical reasoning and decision-making. Participants perceived that exposure and experience in this setting is required to craft and master these additional skills and embed them into their practice.
… in rapid response … you are doing a different role, not just a physio role, a different role, in the sense that … you need so many other skills, new skills, liaising with different professionals, and getting trained into many skills … (P2)
The challenges and emotional labor associated with the role, alongside the satisfaction experienced in becoming a bricoleur are reflected in the ‘emotional roller coaster’ category.
… it’s very challenging wearing all of these different hats. It’s at the same time very rewarding. When you can see the change in that person and especially when you even hear it and they end up saying to you, ‘Thank you for whatever you have done,’ you feel oh wow, I’ve fulfilled my role (P6)
The outcome space
The six categories of description and their relations to each other are presented in an ‘outcome space’ (). illustrates the relationships and connections between the categories of description found in this study and provides a way of viewing the collective experience of working in an RRT despite the fact that this same phenomenon was perceived differently by different participants (Åkerlind, Citation2005; Larsson and Holmström, Citation2007). Working in an RRT for these participants, at this point in time, was represented by the first five categories of description which illuminate the complexity of the multiple roles or ‘hats’ that participants described as fundamental to working in an RRT. The final category ‘an emotional roller coaster’ intertwines throughout all other categories and is presented as the most dominant category. It illuminates the varied emotions associated with the complexity, uncertainty, and responsibility of working in an RRT experienced by these participants.
Discussion
Participants (physiotherapists) working in RRTs described a range of experiences and perceptions of how they conceptualized their work. Participants understood RR work to have various meanings including ‘detective’ problem solving; working as a ‘guru’ in guiding and educating colleagues and patients; working as both ‘lone rangers’ and ‘team players’; and working as a ‘bricoleur’ by using a pluralistic range of knowledge. To work in RR, participants openly perceived and expressed many emotions. These emotional meanings varied and formed ‘an emotional roller coaster.’
In this study, participants perceived that a broader range of knowledge, skills, and investigations were essential to undertake detective work in the RRT setting, and that by using their knowledge, they could then make informed clinical decisions, problem-solve, or determine the next decision. However, participants did not explicitly outline the details of how they embarked upon this process. Working like a detective has been found in other disciplines of healthcare practice. Studies exploring clinical reasoning in physiotherapy emphasize that there is a dialectical reasoning process, which involves combining multiple knowledge sources (Edwards et al., Citation2004) and this resonates with this study’s findings. However, little is known about how therapists in certain situations interpret this information to decide what the clinical issue or next steps may be (Ahlsen, Mengshoel, Bondevik, and Engebretsen, Citation2018). An exploratory study which reviewed physiotherapists working with patients suffering from chronic muscle pain identified that to develop clinical reasoning and problem-solving, physiotherapists consider clues, weigh up different stories, and question the information available (Ahlsen, Mengshoel, Bondevik, and Engebretsen, Citation2018). This detective work and clue construction which triggers questioning and drives reasoning was considered to be driven by ‘uncertainty’ (Ahlsen, Mengshoel, Bondevik, and Engebretsen, Citation2018). Doody and McAteer (Citation2002) also found that physiotherapists, like detectives, undertake a process of cue acquisition, hypothesis generation, and evaluation, which aids clinical reasoning and decision-making. Working like a ‘detective’ is not unique to the RRTs or to the physiotherapy profession, with both tele-nurses (Kaminsky, Rosenqvist, and Holmström, Citation2008) and a life history reflection by an occupational therapist describing ‘detective’ work (Yerxa, Citation2000). Future studies may want to consider how other health professionals undertake problem-solving and clinical reasoning within their practice, as advanced insight into this is likely to contribute toward improving care delivery.
Participants in this study perceived themselves to work as ‘gurus,’ educating and offering expertise. What was emphasized was that in the RRT setting, in addition to recognizing themselves as ‘educators’ for patients, they considered that they had an extended education role with carers and relatives, helping them to better support those needing care at home. Additionally, they conveyed their role in educating other team members which they conveyed as meaningfully related to their close working relationship with other professionals and the overlapping of professional boundaries in the RRT setting. Participants predominantly described didactic education methods; however, some participants referred to ‘guiding,’ and described encouraging their patients to ‘self-manage,’ indicating that they may be moving toward providing more person-centered educational methods. What was absent in the data was explicit descriptions of a more patient-centered model of healthcare (Wittink and Oosterhaven, Citation2018): For example, the data did not include concrete descriptions of participants asking whether education was wanted or needed, exploring patients’ and carers’ pre-understanding, or eliciting what information they considered might be helpful. Other research has also found that health professionals consider education as a key aspect of their work (Forbes, Mandrusiak, Russell, and Smith, Citation2017; Lundh, Rosenhall, and Törnkvist, Citation2006). It has also been suggested that experienced physiotherapists may be more likely to report using self-management education strategies that are patient-centered, and look for patients to obtain full understanding as a means of evaluating their teaching, compared to novices (Forbes, Mandrusiak, Russell, and Smith, Citation2017). A more person-centered educational approach was conceptualized in a phenomenographic study in tele-nurses; they perceived their role as encompassing a large educational aspect, and described themselves as coaches, perceiving validating persons complaints and creating a pleasant atmosphere for the caller as ‘coaching’ strategies, and emphasized the importance of listening and being a discussion partner (Kaminsky, Rosenqvist, and Holmström, Citation2008). These descriptions of educating in this way are less didactic in nature, and are related to encouraging patient empowerment over their situations (Gibson, Citation1991; Jotterand, Amodio, and Elger, Citation2016).
Participants in this study perceived that being an ‘expert’ was essential. They considered themselves as experts by providing an array of expert physiotherapy clinical skills and knowledge to their patients and their wider team. Other research has found that physiotherapists consider themselves ‘experts,’ but this appears to relate to a physiotherapy specialty, rather than being a generalist physiotherapy expert. For example, physiotherapists treating people with anterior cruciate ligament described themselves as rehabilitation experts within this discipline (von Aesch, Perry, and Sole, Citation2016) and physiotherapists working in EDs viewed themselves as musculoskeletal experts (Lefmann and Sheppard, Citation2014). Recognizing ‘expertise’ and specifically ‘generalist expertise’ among physiotherapists and other allied health professionals is important for future workforce planning, especially if services are required to adjust to meet the changing healthcare demands. If there are specific ‘expertise’ skills among professionals working in various disciplines, then they could be utilized more effectively.
Participants described their role as working both as a ‘lone ranger’ and a ‘team player,’ which might be considered contradictory. Traditionally in healthcare, doctors have described themselves as ‘lone rangers’ accountable for their patients’ care (Saha, Citation2016), but the findings of this study suggest that as physiotherapists take on more autonomous advanced practice roles, they also face the challenges of being ‘lone rangers.’ This resonates with physiotherapists working in EDs with amplified autonomy, who also described their work as ‘lone rangers’ with feelings of isolation from their peers (Kilner and Sheppard, Citation2010). Transitioning from one role to another, such as registered nurses to advanced nurse practitioners, has been described as a lonely experience due to increased autonomy, loss of professional identity, and having limited people to consult (Jangland, Uhlin, and Arakelian, Citation2016). Moving from one role to another can trigger loss of confidence and insecurity, and this may be intensified without support from a wider team (MacLellan, Levett-Jones, and Higgins, Citation2015). Conversely, despite increased autonomy, participants also perceived themselves as belonging to teams. In today’s healthcare system, teamwork is considered essential to providing effective patient-centered care to minimize adverse events (Babiker et al., Citation2014). Nursing research has also identified that clinicians who work alone also recognize the necessity of collaborative team working to solve challenging clinical situations (Jangland, Uhlin, and Arakelian, Citation2016) but those in new roles such as advanced nurse practitioners do not always feel welcome and supported (Jangland, Uhlin, and Arakelian, Citation2016). Physiotherapists in EDs have also expressed the challenge of trying to work autonomously and be accepted in a team, perceiving that it was a struggle to build strong relationships and gain approval (Lefmann and Sheppard, Citation2014).
Working in healthcare is frequently described as ‘uncertain’ (Ghosh, Citation2004) which is replicated in this study as some participants expressed that working alone can cause uncertainty. Facing uncertainty is a regular occurrence for health professionals, and especially for those training or working in new disciplines (Kim and Lee, Citation2018). However, in an age of increased transparency and low trust among the public, acknowledging and coping with uncertainty is critical (Kim and Lee, Citation2018). An intolerance to clinical uncertainty can cause emotional distress and burnout among health professionals and may cause patient harm. Being aware of uncertainty, acknowledging it, and engaging in appropriate coping strategies can aid clinicians in dealing with the emotional pressure and stress uncertainty triggers. One successful strategy used to support health-care staff undertaking new or challenging roles has been the development of the Schwartz Center Rounds (Maben et al., Citation2018). The aim of these forums is to improve staff well-being, and ultimately patient care (Maben et al., Citation2018). The fact that participants in this study expressed uncertainty and loneliness suggests that strategies such as Schwartz Rounds may be needed to support those undertaking pioneering or new roles. The ‘lone ranger’ experience and its accompanying uncertainty raise further questions about how emerging roles are being supported, and whether more support needs to be offered through education to ensure these professionals have an appropriate and effective support system to avoid feeling isolated and uncertain.
Participants in this study expressed that to work as an RR physiotherapist they worked as a ‘bricoleur’ by crossing professional boundaries and perceived their roles as ‘unconventional.’ In response to the challenges facing the UK’s healthcare system, traditional roles and responsibilities are converging (Crouch and Brown, Citation2018) and the ‘role extension’ of clinicians gaining additional skills improves patient outcomes when coupled with sufficient organizational support (Hourahane et al., Citation2012). Shaw and DeForge (Citation2012) believe physiotherapists working as bricoleurs will embrace many epistemologies and acquire new ways of clinical reasoning to offer an improved holistic approach to their practice. The ‘bricoleur’ is also seen in nursing, where practitioners develop their clinical practice by adding different skills for new responsibilities (Daly and Carnwell, Citation2003; Gobbi, Citation2005). Nurses working in complex disciplines such as falls’ prevention need knowledge of multiple skills, and an ability to undertake multiple tasks (Jangland, Uhlin, and Arakelian, Citation2016; Kirkpatrick, Boblin, Ireland, and Robertson, Citation2014). Physiotherapists working in EDs have expressed that their clinical role is different from that of a ‘traditional’ physiotherapist (Kilner and Sheppard, Citation2010) for various reasons including skills in differential diagnosis, more autonomy, longer shifts, the need to work under pressure, and taking on roles beyond their previous remit. The crossing of professional boundaries beyond ‘traditional’ roles may have implications for how pre- and post-registration healthcare education for clinicians is delivered to ensure patient safety and quality care is achieved. Furthermore, drawing on multiple types of knowledge could help professions such as physiotherapists move closer toward an improved holistic understanding of health and illness, improving person-centered care (Shaw and DeForge, Citation2012).
In this study, throughout every category of description, participants expressed their work as ‘an emotional rollercoaster,’ describing both positive and negative emotions. Other research focused on exploring emotional experience has found clinicians experience a range of emotions in their roles (Larner, Wagstaff, Thelwell, and Corbett, Citation2017; Röing, Hirsch, and Holmström, Citation2006). Oncology clinicians have described their role as ‘riding the rollercoaster’ (Phillips and Volker, Citation2019) and surgeons have expressed a wide range of emotions when undertaking their work including anxiety, fear, distress, guilt, and accountability (Orri, Revah-Lévy, Farges, and Harris, Citation2015). However, emotions have also been recognized in a positive sense, with research finding that clinician emotion may play a key role in clinical reasoning and decision-making, giving credibility to intuition and ‘gut feeling’ (Kozlowski et al., Citation2017; Langridge, Roberts, and Pope, Citation2016; Woolley and Kostopoulou, Citation2013). In this study, participants experienced a wide range of emotions across all categories including both positivity such as confidence and feelings of their roles being rewarding, and also negativity such as fear and frustration. It is unclear whether the perceived emotion in this study is linked purely to RR work, or whether participants were still adjusting to working within a pioneering area. Evidence considering role transitions among other health professionals has confirmed that stress is present in those undertaking novice or pioneering roles (Duchscher, Citation2008; Etheridge, Citation2007). Other research concludes that previous clinical experience combined with existing clinical skills and knowledge can facilitate confidence for role transitions (Melrose and Gordon, Citation2011). A potential future avenue of exploration would be to consider whether there is a link between emotion and clinical decision-making, and whether acknowledging emotion assists RR physiotherapists in recognizing and managing stress and/or burnout.
Methodological considerations
Credibility, dependability, and transferability need to be considered when determining whether the qualitative research undertaken is of appropriate quality (Rolfe, Citation2006). There was variation in most of the characteristics of the participants who were recruited () with a mix of ages, years of physiotherapy experience. However, five out of the six participants were male, and all participants included were from London or Greater London despite the recruitment process targeting all geographical areas of the UK, which could be a limitation. It is important to acknowledge that the work undertaken by RRT physiotherapists may differ depending on location and context. There is no national register of UK physiotherapists in RRTs, which limited the study’s ability to target the desired population. We acknowledge that these findings represent the perceptions of these physiotherapists at this point in time, and in line with our phenomenographic approach, do not seek to generalize findings. Instead, we provide in-depth insight into these individuals’ experiences while working in the context of an RRT and invite readers to consider whether these findings resonate with them and their context.
An appropriate sample size is important to ensure credibility. However, there is no accepted participant number required for qualitative studies as the sample size depends on the research purpose and richness of the data. A small data set is normal to allow for an in-depth understanding of the phenomenon. There is no set number of participants suggested for phenomenographic studies (Yates, Partridge, and Bruce, Citation2012) although some authors advocate more than 10 to maximize the likelihood of finding variation (Holmström, Halford, and Rosenqvist, Citation2003). Six participants were recruited to this study as it explores an emerging role, and only a small number of physiotherapists currently work in this area. Although this study highlights variation between participants, it does not claim to saturate the variations within experience (Braun and Clarke, Citation2021). To aid dependability, this study undertook a pilot interview to check that the question(s) asked generated information on the phenomenon being explored (Åkerlind, Citation2005). During the official interviews, the same key questions and prompts were used to ensure that the same subject material was covered. The findings of this study form a basis for future research by providing some insights into the variation in experiences and perceptions of those working in these roles, so that they and others may be better supported as these roles develop into more mainstream areas of practice. Interviews varied in length, taking between 40 and 80 minutes. All participants expressed various experiences of undertaking RR work, and in varying ways, providing multiple concrete examples, and rich (thick) descriptions.
The main researcher works in an RRT, which may have compromised objectivity and professionalism. However, the main researcher undertook a process of reflexivity throughout data collection and data analysis, considered any preconceptions, and did their best to ‘bridle’ their pre-conceptions (Dahlberg, Citation2006) by keeping a reflexive diary, before reaching final descriptive categories. They also closely liaised with the second researcher, an experienced qualitative researcher, during the data analysis and determination of the final categories to help reduce insider researcher bias. These processes promoted methodological rigor and strengthened the credibility of this study (Åkerlind, Citation2005). To illustrate how the descriptive categories and the final outcome space was formulated, the study has presented a comprehensive and varied selection of quotations from all participants. In line with Graneheim, Lindgren, and Lundman (Citation2017) this study has described the context, methodology, characteristics of participants, data collection, and analysis process as comprehensively as possible to enhance transferability. It is hoped that the findings discovered among RR physiotherapists will encourage further research to compare experiences and perceptions of those within similar settings.
Implications for clinical practice
Researching professionals’ experiences and perceptions of emerging roles is essential for transforming practice and providing the necessary evidence required to support the development of new care pathways. This study highlights the various ways physiotherapists perceive and experience their roles within RRTs, and provides insight into how they view their skills and knowledge. This could prove useful for future workforce planning, as physiotherapists with RRT expertise and experience could be utilized further by working in other health disciplines and new care models. This study highlights that RRT physiotherapists experience a range of rollercoaster of emotions, emphasizing the need to implement support strategies for persons working in these roles to ensure they maintain a healthy emotional wellbeing, enabling them to better care for others. Further research is needed to evaluate how physiotherapists can be better prepared for role transition.
Conclusions
The RR physiotherapy role and discipline is new and largely unexplored. This is the first qualitative study which has investigated how working in RRTs is experienced and perceived by physiotherapists. It adds a human perspective to the RR physiotherapy literature, acknowledging that experience and perception may offer valuable insight into RR physiotherapy and health professional practice. It also considers how current and new RR physiotherapy services could be delivered and developed, and offers food for thought for pre- and post-physiotherapy educational programs preparing future clinicians to work in the discipline. The numbers of RRTs continue to expand with associated physiotherapy posts being advertised and developed, indicating that clinical practice in this area is ahead of research. The findings of this study suggest a need for further qualitative research on physiotherapists and other health professionals working in RRTs. This will have important implications for delivering future effective, safe, and quality care within this area of practice.
Acknowledgments
We would like to warmly thank the physiotherapists who kindly agreed to take part in this study and shared the experiences of their practice. The research was funded by the National Institute of Health Research (NIHR) as part of a funded MRes completed at Brighton University.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Addicott R, Maguire D, Honeyman M, Jabbal J 2015 Workforce Planning in the NHS. The King’s Fund http://www.kingsfund.org.uk/publications/workforce-planning-nhs.
- Age UK 2019 Later Life in the United Kingdom. https://www.ageuk.org.uk/globalassets/age-uk/documents/reports-and-publications/later_life_uk_factsheet.pdf.
- Ahlsen B, Mengshoel A, Bondevik H, Engebretsen E 2018 Physiotherapists as detectives: Investigating clues and plots in the clinical encounter. Medical Humanities 44: 40–45. doi:10.1136/medhum-2017-011229.
- Åkerlind GS 2005 Variation and commonality in phenomenographic research methods. Higher Education Research and Development 24: 321–334. doi:10.1080/07294360500284672.
- Åkerlind GS 2012 Variation and commonality in phenomenographic research methods. Higher Education Research and Development 31: 115–127. doi:10.1080/07294360.2011.642845.
- Babiker A, El Husseini M, Al Nemri A, Al Frayh A, Al Juryyan N, Faki M, Assiri A, Al Saadi M, Shaikh F, Al Zamil F 2014 Health care professional development: Working as a team to improve patient care. Sudanese Journal of Paediatrics 14: 9–16.
- Baker C 2017 Accident and emergency statistics: Demand, performance and pressure. Briefing Paper Number 6964. House of Commons Library pp. 1–32. https://commonslibrary.parliament.uk/research-briefings/sn06964/.
- Barnard A, McCosker H, Gerber R 1999 Phenomenography: A qualitative research approach for exploring understanding in health care. Qualitative Health Research 9: 212–226. doi:10.1177/104973299129121794.
- Blunt I, Bardsley M, Dixon J 2010 Trends in emergency admissions in England 2004–2009: Is greater efficiency breeding inefficiency? Nuffield Trust. https://www.nuffieldtrust.org.uk/research/trends-in-emergency-admissions-in-england-2004-2009.
- Braun V, Clarke V 2013 Successful qualitative research. A practical guide for beginners pp. 45–56. London: SAGE.
- Braun V, Clarke V 2021 To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qualitative Research in Sport, Exercise and Health 13: 201–216. doi:10.1080/2159676X.2019.1704846.
- Caplan GA, Sulaiman NS, Mangin DA, Aimonino Ricauda N, Wilson AD, Barclay LA 2012 Meta-analysis of ”hospital in the home”. Medical Journal of Australia 197: 512–519. doi:10.5694/mja12.10480.
- Centre for Workforce Intelligence 2011 Workforce risks and opportunities: Adult social care. London: Centre for Workforce Intelligence. www.cfwi.org.uk/publications/workforce-risks-and-opportunities-adult-social-care.
- Cibangu S, Hepworth M 2016 The uses of phenomenology and phenomenography: A critical review. Library & Information Science Research 38: 148–160. doi:10.1016/j.lisr.2016.05.001.
- Clift E 2015 How a rapid response team is supporting people to remain at home. Nursing Older People 27: 16–21. doi:10.7748/nop.27.10.16.s19.
- Creswell JW, Poth NP 2009 Qualitative inquiry and research design. Choosing among five approaches (4th ed), pp. 100–159. London: SAGE.
- Crouch R, Brown R 2018 Advanced clinical practitioners in emergency care: Past, present and future. British Journal of Hospital Medicine 79: 511–515. doi:10.12968/hmed.2018.79.9.511.
- Dahlberg K 2006 The essence of essences: The search for meaning structures in phenomenological analysis of lifeworld phenomena. International Journal of Qualitative Studies on Health and Well-Being 1: 11–19. doi:10.1080/17482620500478405.
- Daly W, Carnwell R 2003 Nursing roles and levels of practice: A framework for differentiating between elementary, specialist and advancing nursing practice. Journal of Clinical Nursing 12: 158–167. doi:10.1046/j.1365-2702.2003.00690.x.
- Department of Health 2015 Transforming urgent and emergency care services in England https://www.england.nhs.uk/wp-content/uploads/2015/06/trans-uec.pdf.
- Doody C, McAteer M 2002 Clinical reasoning of expert and novice physiotherapists in an outpatient orthopaedic setting. Physiotherapy 88: 258–268. doi:10.1016/S0031-9406(05)61417-4.
- Duchscher JB 2008 A process of becoming: The stages of new nursing graduate professional role transition. Journal of Continuing Education in Nursing 39: 441–450. doi:10.3928/00220124-20081001-03.
- Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen GM 2004 Clinical reasoning strategies in physical therapy. Physical Therapy 84: 312–330. doi:10.1093/ptj/84.4.312.
- Etheridge SA 2007 Learning to think like a nurse: Stories from new nurse graduates. Journal of Continuing Education in Nursing 38: 24–30. doi:10.3928/00220124-20070101-05.
- Evans N 2017 Clock ticking again on four-hour target. Emergency Nurse 25: 8–10. doi:10.7748/en.25.1.8.s9.
- Facultad J, Lee G 2019 Patient satisfaction with a hospital-in-the-home service. British Journal of Community Nursing 24: 79–185. doi:10.12968/bjcn.2019.24.4.179.
- Forbes R, Mandrusiak A, Russell T, Smith M 2017 Evaluating physiotherapists’ practice and perceptions of patient education: A national survey in Australia. International Journal of Therapy and Rehabilitation 24: 122–130. doi:10.12968/ijtr.2017.24.3.122.
- Ghosh AK 2004 Understanding medical uncertainty: A primer for physicians. Journal of the Association of Physicians of India 52: 739–742.
- Gibson C 1991 A concept analysis of empowerment. Journal of Advanced Nursing 16: 354–361. doi:10.1111/j.1365-2648.1991.tb01660.x.
- Gilburt H 2016 Supporting integration through new roles and working across boundaries. London: King’s Fund. https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Supporting_integration_web.pdf.
- Giorgi A 1999 A phenomenographical perspective on some phenomenographic results on learning. Journal of Phenomenological Psychology 30: 68–93. doi:10.1163/156916299X00110.
- Gobbi M 2005 Nursing practice as bricoleur activity: A concept explored. Nursing Inquiry 12: 117–125. doi:10.1111/j.1440-1800.2005.00261.x.
- Graneheim U, Lindgren B, Lundman B 2017 Methodological challenges in qualitative content analysis: A discussion paper. Nurse Education Today 56: 29–34. doi:10.1016/j.nedt.2017.06.002.
- Holmström I, Halford C, Rosenqvist U 2003 Swedish health care professionals’ diverse understandings of diabetes care. Patient Education and Counselling 51: 53–58. doi:10.1016/S0738-3991(02)00212-4.
- Hourahane G, West N, Barnes R, Rees S, Bowyer A, Dundon J, Allen D 2012 Supporting trail-blazing: A systematic review of the factors that facilitate or inhibit the implementation of new nursing roles: The experiences of UK consultant nurses. Joanna Briggs Institute Library of Systematic Reviews 10: 3146–3294. doi:10.11124/jbisrir-2012-21.
- Jangland E, Uhlin PY, Arakelian E 2016 Between two roles - Experiences of newly trained nurse practitioners in surgical care in Sweden: A qualitative study using repeated interviews. Nurse Education in Practice 21: 93–99. doi:10.1016/j.nepr.2016.10.005.
- Jotterand F, Amodio A, Elger BS 2016 Patient education as empowerment and self-rebiasing. Medicine, Health Care, and Philosophy 19: 553–561. doi:10.1007/s11019-016-9702-9.
- Kaminsky E, Rosenqvist U, Holmström I 2008 Telenurses’ understanding of work: Detective or educator? Journal of Advanced Nursing 65: 382–390. doi:10.1111/j.1365-2648.2008.04877.x.
- Kilner E, Sheppard L 2010 The ‘lone ranger’: A descriptive study of physiotherapy practice in Australian emergency departments. Physiotherapy 96: 248–256. doi:10.1016/j.physio.2010.01.002.
- Kim K, Lee Y 2018 Understanding uncertainty in medicine: Concepts and implications in medical education. Korean Journal of Medical Education 30: 181–188. doi:10.3946/kjme.2018.92.
- Kincheloe J 2005 On to the next level: Continuing the conceptualization of the bricolage. Qualitative Inquiry 11: 323–350. doi:10.1177/1077800405275056.
- King’s Fund 2015 Ten Priorities for Commissioners. https://www.kingsfund.org.uk/publications/articles/transforming-our-health-care-system-ten-priorities-commissioners/summary
- Kirkpatrick H, Boblin S, Ireland S, Robertson K 2014 The nurse as bricoleur in falls prevention: Learning from a case study of the implementation of fall prevention best practices. Worldviews on Evidence-Based Nursing 11: 118–125. doi:10.1111/wvn.12026.
- Kozlowski D, Hutchinson M, Hurley J, Rowley J, Sutherland J 2017 The role of emotion in clinical decision making: An integrative literature review. BMC Medical Education 17: 255. doi:10.1186/s12909-017-1089-7.
- Langridge N, Roberts L, Pope C 2016 The role of clinician emotion in clinical reasoning: Balancing the analytical process. Manual Therapy 21: 277–281. doi:10.1016/j.math.2015.06.007.
- Larner R, Wagstaff C, Thelwell R, Corbett J 2017 A multi-study examination of organizational stressors, emotional labour, burnout, and turnover in sport organizations. Scandinavian Journal of Medicine & Science in Sports 27: 2103–2115. doi:10.1111/sms.12833.
- Larsson J, Holmström I 2007 Phenomenographic or phenomenological analysis: Does it matter? Examples from a study on anaesthesiologists’ work. International Journal of Qualitative Studies on Health and Well-Being 2: 55–64. doi:10.1080/17482620601068105.
- Lee G, Pickstone N, Facultad J, Titchener K 2017 The future of community nursing: Hospital in the home. British Journal of Community Nursing 22: 174–180. doi:10.12968/bjcn.2017.22.4.174.
- Lee G, Titchener K 2017 The Guy’s and St Thomas’s NHS Foundation Trust @home service: An overview of a new service. London Journal of Primary Care 9: 18–22. doi:10.1080/17571472.2016.1211592.
- Lefmann S, Sheppard L 2014 Perceptions of emergency department staff of the role of physiotherapists in the system: A qualitative investigation. Physiotherapy 100: 86–91. doi:10.1016/j.physio.2013.08.004.
- Lundh L, Rosenhall L, Törnkvist L 2006 Care of patients with chronic obstructive pulmonary disease in primary health care. Journal of Advanced Nursing 56: 237–246. doi:10.1111/j.1365-2648.2006.04027.x.
- Maben J, Taylor C, Dawson J, Leamy M, McCarthy I, Reynolds E, Ross S, Shuldham C, Bennett L, Foot C 2018 A realist informed mixed-methods evaluation of Schwartz Center Rounds® in England. Health Services and Delivery Research 6: 1–260.
- MacLellan L, Levett-Jones T, Higgins I 2015 Nurse practitioner role transition: A concept analysis. Journal of the American Association of Nurse Practitioners 27: 389–397. doi:10.1002/2327-6924.12165.
- Marton F 1981 Phenomenography - Describing conceptions of the world around us. Instructional Science 10: 177–200. doi:10.1007/BF00132516.
- Marton F, Dahlgren LO, Svensson L, Säljö R 1977 Learning and Conception of the World Around Us. Stockholm: Almquist and Wiksell.
- Marton F, Svensson L 1979 Conceptions of research in student learning. Higher Education 8: 471–486. doi:10.1007/BF01680537.
- Melrose A, Gordon K 2011 Overcoming barriers to role transition during online post LPN to BN program. Nurse Education in Practice 11: 31–35. doi:10.1016/j.nepr.2010.06.002.
- Mendes E, Rodrigues JP, Preto L, Novo A 2016 Functional and cognitive decline in hospitalized elderly. Journal of Ageing and Innovation 5: 11–21.
- Montalto M 2010 The 500‐bed hospital that isn’t there: The Victorian Department of Health review of the Hospital in the Home program. Medical Journal of Australia 193: 598–601. doi:10.5694/j.1326-5377.2010.tb04070.x.
- Montalto M, Lui B, Mullins A, Woodmason K 2010 Medically-managed Hospital in the Home: 7-year study of mortality and unplanned interruption. Australian Health Review 34: 269–275. doi:10.1071/AH09771.
- Mudge AM, Banks MD, Barnett AG, Blackberry I, Graves N, Green T, Harvey G, Hubbard RE, Inouye SK, Kurrle S, et al. 2017 CHERISH (collaboration for hospitalised elders reducing the impact of stays in hospital): Protocol for a multi-site improvement program to reduce geriatric syndromes in older inpatients BMC Geriatrics 17 11. doi:10.1186/s12877-016-0399-7.
- Murray R, Jabbal J, Thompson J, Baird B, Maguire D 2017 NHS areas planning to cancel or delay spending due to financial pressures: Quarterly monitoring report June. The Kings Fund.
- NHS Benchmarking Network 2013 National audit of intermediate care report www.nhsbenchmarking.nhs.uk/National-Audit-of-Intermediate-Care/year-two.php.
- NHS England 2013 “Transforming urgent and emergency care services in England,” Urgent and Emergency Care Review (end of Phase 1 report: Appendix 1) – Revised Evidence Base from the Urgent and Emergency Care Review. https://www.nhs.uk/nhsengland/keogh-review/documents/uecr.ph1report.appendix%201.evbase.fv.pdf.
- NHS England 2014 Five Year Forward View. https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf.
- NHS England 2019 The NHS long term plan. https://www.longtermplan.nhs.uk/.
- Nuffield Trust 2017 Shifting the balance of care. https://www.nuffieldtrust.org.uk/research/shifting-the-balance-of-care-great-expectations.
- Office for National Statistics 2013 General Lifestyle Survey 2011. London: Office for National Statistics.
- Oliver D, Foot C, Humphries R 2014 Making our health and care systems fit for an ageing population https://www.kingsfund.org.uk/publications/making-our-health-and-care-systems-fit-ageing-population.
- Orri M, Revah-Lévy A, Farges O, Harris F 2015 Surgeons’ emotional experience of their everyday practice - A qualitative study. PLoSOne 10: e0143763. doi:10.1371/journal.pone.0143763.
- Pang MF 2003 Two faces of variation. On continuity in the phenomenographic movement. Scandinavian Journal of Educational Research 47: 145–156. doi:10.1080/00313830308612.
- Pertz S 2007 The guru in Me - Critical perspectives on management pp. 2–3. Germany: GRIN Verlag.
- Phillips C, Volker D 2019 Riding the roller coaster. Cancer Nursing 43: E283–E290. doi:10.1097/NCC.0000000000000734.
- Röing M, Hirsch J, Holmström I 2006 Ways of understanding the encounter with head and neck cancer patients in the hospital dental team - A phenomenographic study. Supportive Care in Cancer 14: 1046–1054. doi:10.1007/s00520-006-0043-8.
- Rolfe G 2006 Validity, trustworthiness and rigour: Quality and the idea of qualitative research. Journal of Advanced Nursing 53: 304–310. doi:10.1111/j.1365-2648.2006.03727.x.
- Saha JB 2016 Leadership in Healthcare. Journal of Comprehensive Health 4: 4–5. doi:10.53553/JCH.v04i01.001.
- Säljö R 1979 Learning about learning. Higher Education 8: 443–451. doi:10.1007/BF01680533.
- Shaw J, DeForge R 2012 Physiotherapy as bricolage: Theorizing expert practice. Physiotherapy Theory and Practice 28: 420–427. doi:10.3109/09593985.2012.676941.
- Shepperd D, Doll H, Angus R, Clarke M, Iliffe S, Kalra L, Ricauda NA, Tibaldi V, Wilson AD 2009 Avoiding hospital admissions through provision of hospital care at home: A systematic review and meta-analysis. Canadian Medical Association Journal 180: 175–182. doi:10.1503/cmaj.081491.
- Sin S 2010 Considerations of quality in phenomenographic research. International Journal of Qualitative Methods 9: 305–319. doi:10.1177/160940691000900401.
- Stevenson J, Spencer L 2002 Developing intermediate care: A guide for health and social services professionals https://www.kingsfund.org.uk/sites/default/files/Developing-Intermediate-Care-guide-health-social-services-professionals-Jan-Stevenson-Linda-Spencer-The-Kings-Fund-July-2009.pdf
- Svensson L 1997 Theoretical foundations of phenomenography. Higher Education Research and Development 16: 159–171. doi:10.1080/0729436970160204.
- Varney J, Weiland T, Jelinek G 2014 Efficacy of hospital in the home services providing care for patients admitted from emergency departments. International Journal of Evidence-Based Healthcare 12: 128–141. doi:10.1097/XEB.0000000000000011.
- von Aesch A, Perry M, Sole G 2016 Physiotherapists’ experiences of the management of anterior cruciate ligament injuries. Physical Therapy in Sport 19: 14–22. doi:10.1016/j.ptsp.2015.08.004.
- Wilson A, Parker H, Wynn A, Jagger C, Spiers N, Jones J, Parker G 1999 Randomised controlled trial of effectiveness of Leicester hospital at home scheme compared with hospital care. British Medical Journal 319: 1542–1546. doi:10.1136/bmj.319.7224.1542.
- Wittink H, Oosterhaven J 2018 Patient education and health literacy. Musculoskeletal Science and Practice 38: 120–127. doi:10.1016/j.msksp.2018.06.004.
- Woolley A, Kostopoulou O 2013 Clinical intuition in family medicine: More than first impressions. Annals of Family Medicine 11: 60–66. doi:10.1370/afm.1433.
- Yates C, Partridge H, Bruce C 2012 Exploring information experiences through phenomenography. Library and Information Research 36: 96–119. doi:10.29173/lirg496.
- Yerxa EJ 2000 Confessions of an occupational therapist who became a detective. British Journal of Occupational Therapist 63: 192–199. doi:10.1177/030802260006300502.
Appendix
Table A1. Data analysis example from participant 2. Exploring what was the focus of their attention and how they described it (analysis steps 2 and 3).
Table A2. Initial descriptions of understanding from meaning units for participant 2 (analysis step 4).
Table A3. Data analysis compiling quotes across participants. Example of category of descriptions of the Lone Ranger (analysis step 4).
Figure A1. Early development the metaphors and outcome space.