
ABSTRACT
Livestock productivity for pastoralist households, who depend upon their livestock as a source of livelihood, is constrained by infectious diseases among other factors. Pastoralists in the arid and semi-arid lands (ASALs) of the Horn of Africa lack access to livestock health inputs and services. To assess the profitability of private animal health service delivery, mobile veterinary clinics were piloted in three ASAL counties in Kenya. Our findings reveal the positive impact of the clinics on animal health provision as well as policy and regulatory factors that affect its viability.
Introduction
Pastoralism, defined as the use of extensive grazing on rangelands for livestock production (FAO Citation2001) is widely practiced globally. It is estimated that 38% of the earth’s surface is devoted to agriculture and livestock production takes up 75% of agricultural land (Breu et al. Citation2015). Pastoralism is widespread in Africa, Central, and South Asia, producing 35% of world’s cattle, 55% of sheep and goats and most of the dromedary (Kaufmann, Hulsebusch, and Kratli Citation2018). It dominates the economies of dryland areas of the Horn of Africa, and has proven to be a remarkably robust and adaptable form of livestock production (Catley, Lind, and Scoones Citation2016). African pastoralism is characterised by a high reliance on livestock as a source of economic and social well-being, and various types of strategic mobility to access water and grazing resources in areas of high rainfall variability (African Union Citation2013).
The livestock sector has a key role in how to achieve the balance between food production, livelihoods, and environmental objectives (Herrero and Thornton Citation2013). Besides significant contribution to gross domestic product and indirect contribution through production of organic fertiliser, draught power, and foreign exchange earnings (de Haan et al. Citation2016), livestock contributes to food supply by converting low-value materials, inedible or unpalatable for people, into nutrition-dense animal-source foods (milk, meat and eggs) (Smith et al. Citation2013). This is especially true for African pastoralism, which is characterised by the limited use of cultivated fodder and occurs in areas unsuitable for cropping, with minimal competition with food crops (Krätli et al. Citation2013). While some authors had predicted the disappearance of pastoralism, rangelands continue to provide livelihoods to some 120 million people and cover 45% of the world’s surface area (Scoones et al. Citation2020). While these areas remain poor and often forgotten by decision and policymakers, others recognise the resilience of pastoralism in the face of numerous weather, political, and market shocks.
Regional demand for meat and milk is expected to double by 2030 (de Haan et al. Citation2016), hence the concern of sustainably increasing livestock productivity in sub-Saharan Africa (SSA). However, one limitation on livestock productivity for pastoral households is infectious diseases, coupled with limited access to livestock health inputs (AU-IBAR Citation2010; Marsh et al. Citation2016). Animal diseases are responsible for annual losses amounting to a quarter of the total value of livestock production in SSA (AU-IBAR Citation2010). Providing adequate animal health services to pastoralists in SSA has remained a challenge in spite of previous recent reforms (Ilukor, Birner, and Nielsen Citation2015). In Tanzania, for example, lack of access to animal health inputs and services has been cited as a major challenge by pastoralists (Gustafson et al. Citation2015) despite many stakeholders being aware of the need for reforms (Rutabanzibwa Citation2002). In Kenya, the service evolved from colonial-era private veterinary practice to free services for all immediately post-independence in the 1970s, then to structural adjustment between 1980–1992 (this involved disinvestment by the government from provision of clinical services) and training of community animal health workers (CAHWs) particularly in arid and semi-arid lands (ASALs) to supplement the few veterinary professionals (Higham et al. Citation2016; Young et al. Citation2003). Over the years, the delivery of animal health services in pastoral livestock production areas has struggled with low resources (few veterinarians and budget allocation by government) and low incentives for setting up private practices (Ilukor Citation2017).
Animal health services and products are currently provided in Kenya by veterinary surgeons, animal health assistants (paraprofessionals), shops and market vendors, ethnoveterinary practitioners, natural healers (Heffernan and Misturelli Citation2002; Young et al. Citation2003), and self-diagnosis and medication (Lamuka et al. Citation2017). The shops, mainly agrovet shops but also ordinary shops, are retailers of mixed agricultural supplies, the majority of which are privately owned (Higham et al. Citation2016). CAHWs and animal health assistants (AHAs) were able to provide private services for many years (Rubyogo et al. Citation2005), until 2012 when CAHWs were disbanded in spite of empirical evidence in the late 1990s (Okwiri, Kajume, and Odondi Citation2001) that privatised networks of AHAs linked to CAHWs were the most economically feasible approach to provide sustainable primary level clinical services in Kenya. This was because of concerns by government statutory bodies that CAHWs did not fit within the existing technical, legal and policy framework (Mugunieri, Irungu, and Omiti Citation2004).
Livestock diseases still rank as the main production constraint in pastoral areas in Kenya (Onono et al. Citation2018) and privatisation of animal health services created a gap that is yet to be filled. Few trained veterinarians are willing to work in pastoral livestock production systems which have high livestock populations, given their remoteness (Lamuka et al. Citation2017). Moreover, challenges, including the transhumant/nomadic nature of pastoralists (leading to spatial and temporal variation in demand), economic non-viability of private sector provision of animal health goods and services due to the high travel costs of serving pastoral livestock keepers, and poor infrastructure that leads to high delivery costs (Ilukor Citation2014; Lamuka et al. Citation2017) crowd-out private investment in the provision of animal health inputs and services among pastoralists. Self-diagnosis and medication have therefore become a rampant practice which can lead to, among other things, inappropriate drug use (Lamuka et al. Citation2017) and consequently antimicrobial resistance problems in some cases (i.e. high levels of antimicrobials use, low levels of professional consultation, and absence of withdrawal, potentially affects the dissemination of resistance) (Caudell et al. Citation2017).
Since improved use of animal health services by pastoralists increases economic wealth for these households (Marsh et al. Citation2016), new models are needed to improve access to, and use of, animal health services among pastoralists. With the aim of testing whether profitable private animal health service delivery can be established in ASALs and identifying the conditions (policies or regulations) that would enhance its viability, mobile veterinary clinics were piloted in three ASAL counties in Kenya. The clinics involved partnering with private sector agrovets to create regular and scheduled clinical veterinary visits, through high livestock concentration points such as markets, watering points, and grazing areas (considering migration of livestock), by veterinarians providing animal health products and services. We present the results from a participatory impact evaluation of this innovative model of delivering animal health services and inputs in pastoral production systems in Kenya. Lessons from this approach are also relevant to pastoral areas in other countries in East Africa and other regions of the world.
Methods
Study area
The mobile clinic delivery system was tested in Isiolo, Marsabit, and Garissa counties in Kenya (). The three counties are ASALs where pastoralism is the mainstay of the populations. ASALs in Kenya account for 50% of Kenya’s total livestock population, some 1.6 million tropical animal unitsFootnote1 which provide 90% of the regions’ employment and 50% of their household incomes (Nyanjom Citation2014). The three counties have a total population of 1,057,460 (291,166 in Marsabit, 623,060 in Garissa, and 143,234 in Isiolo) according to the 2009 Kenya Population and Housing census.
Figure 1. The study sites.
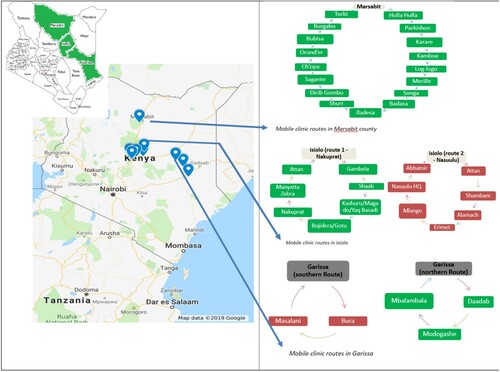
Marsabit is the second largest county in Kenya, with 75% of its land classified as rangeland and used for livestock grazing. It is largely arid/semi-arid and inhabited mostly by semi-nomadic livestock herders (Haro, Doyo, and McPeak Citation2005). The inhabitants of Garissa county are pastoralists and agro-pastoralists keeping camels, cattle, sheep, goats, and donkeys and doing some crop farming along the river Tana. The county is the immediate catchment for the Garissa livestock market, which is the largest in East Africa and supplies livestock for both the local market and export (Mwanyumba et al. Citation2015). Likewise, Isiolo county is characterised by very arid, arid, and semi-arid agro-ecological zones. The vegetation is comprised of shrubs and acacia trees, which supports rearing of camels, goats, sheep, and cattle (Affognon et al. Citation2017). Located in remote and arid regions with very little transport infrastructure and other means of communication, a dispersed population, scattered over a large area in relatively small settlements (GoK Citation2012), renders the ASALs prone to poor service delivery, including animal health services. To date, the areas lack technical personnel, infrastructure and other basic facilities.
The mobile veterinary clinic concept
Pastoralists face many challenges in relation to livestock diseases (presence of several endemic and epidemic diseases), external parasites (ticks, mites, tsetse flies), irregular animal health services, high cost of drugs, high prevalence of counterfeit drugs, fluctuating and poor prices for their livestock (income source), and long distances to urban centres where animal health inputs and services can be found. Given these challenges, the mobile veterinary clinic concept was built on a weekly circuit in which service providers deliver animal health products and services through designated service points along a chosen route. This was carried out by two private service providers (Sidai Africa Limited in Marsabit and Isiolo counties, and FACTS Agrovet in Garissa county). Overseen by government veterinarians, it entailed travelling to watering points, markets and villages where pastoralists often gather large numbers of animals. Sidai is a large social venture company operating in many counties with significant support from donors, while FACTS is a small agrovet company owned by young professionals operating in Garissa.
The veterinarians from Sidai and FACTS, accompanied by county veterinary officers, offered the full range of animal health services allowed by law, including tick control, hoof trimming, dehorning, castration, pregnancy diagnosis, treatments, sale of veterinary inputs, and dissemination of advice from extension services. In Isiolo and Garissa, there were two routes, a northern and southern route. Each route was covered by a weekly circuit of scheduled visits for products and service provision from one point to another along the route with a break before the other route was served. In Marsabit, there was one continuous route through all the scheduled points. illustrates the routes where the delivery system was tested.
Assessment methods, sites, and timing
Following research approval granted by ILRI’s institutional research ethics committee, a baseline survey was conducted at the beginning of the study, interviewing service providers in all the routes in the three study counties. Written informed consent was obtained from respondents before commencing interviews. Owing to very few actors in the area, all animal health products and service providers (excluding government veterinary officers) were surveyed. shows the categories and numbers of service providers in the study areas.
Table 1. Number of animal health service actors (excluding government veterinarians) in the sites at the baseline.
Sidai and FACTs then initiated the mobile clinics with an embedded monitoring survey for four months before a final impact evaluation study was conducted. The final impact evaluation applied a participatory impact assessment (PIA) approach. PIA aims at involving communities in describing and analysing changes in an area during, or shortly after the implementation of a project (Admassu et al. Citation2005). Using participatory ranking and scoring methods, in focus group discussions (FGDs) and key informant interviews (KIIs), PIA enables qualitative indicators to be presented numerically and to assess project attribution, by comparing both the project and non-project factors that contributed to any assessed change (Catley et al. Citation2008). PIA was used to assess the impact of the tested delivery approach that was piloted between December 2017 and April 2018. The PIA was conducted four months after the end of the pilot to observe the impact and sustainability of the clinics by assessing different aspects of the delivery system before, during, and after the pilot.
The study aim was to assess changes in the delivery of animal health inputs and services over time and whether the changes, if any, can be attributed to the tested delivery system, and to elicit feedback and perceptions of pastoralists regarding the impact of the mobile clinics on the delivery of animal health products and services. A mix FGDs and KIIs was used. In total 11 FGDs (each composed of a group of informants), one in each of the points listed in , and five KIIs with the service providers, county veterinary officers, and community leaders (leaders from two livestock conservancies in Isiolo where the delivery system was implemented) were conducted.
Table 2. Study sites and participants’ profile.
The study applied a scoring method using proportional piling techniques in FGDs to elicit data used to assess impacts of the mobile clinics on knowledge, availability, quality, and affordability of different animal health products and services (), observed by groups of informants. A scoring method was developed that required informants to score the attributes of animal health products and services (quality, availability, and affordability), and knowledge imparted on pastoralists from advisory services that may have accompanied the purchase of the products/services, before, during, and after the testing of mobile clinics. Taking each product/service category in turn, informants were asked to distribute 10 marbles to show the level of each attribute before, during and after. To elicit attribution, informants were then asked to explain the reasoning behind the scores and to discuss the mobile clinic’s inputs and activities relative to other non-mobile clinic factors that may have contributed to the observed changes.
Table 3. Assessment objects.
Further, a participatory actor’s scoring matrix was developed. Informants were asked to score (proportional piling using 10–20 marbles, depending on the number of actors – animal health service providers available in the area), different attributes () of these actors before and after the tested delivery system. Informants then discussed the relative merits of the different animal health service providers. Information from the scores was complemented with information on the communities’ perceptions of the attributes. Consequently, a pairwise comparison matrix was developed to assess the communities’ trade-offs between the actors’ attributes and eventually rank the attributes from the most important to the least important.
Finally, the livestock keepers’ willingness to pay (WTP) for products and services brought closer through mobile clinics was elicited using an open-ended contingent valuation approach. Informants were asked to rank the common products and services sought after. In each FGD, the most commonly sought-after product/service was identified. The product’s average price in nearby town formed a reference price from which the informants’ WTP, if the product was to be sold through mobile clinics (making the product accessible to the producers), was assessed. The modal WTP price (quoted by most informants) was then evaluated in terms of the percentage increase from the reference price.
Following Admassu et al. (Citation2005), the methods were repeated for each of the 11 FGDs, one group per study site. The groups consisted of an average of 18 people per site in the 11 sites (210 people in total), of which 72% were male, and 51% had attended the mobile clinics (). A median test was used to assess whether scores obtained on perceived levels of services before and after the intervention changed significantly. Kendal coefficient of concordance (W) was used to assess whether there was agreement between the 11 groups in terms of the observed impacts of the mobile clinic. Kendall’s W, a normalisation of the statistic of the Friedman test, is a non-parametric statistic which ranges from 0 (no agreement) to 1 (complete agreement among raters).
Results and discussion
The impact on animal health products and services’ attributes
The pre-implementation status of the study site with regard to the provision of animal health services was characterised by a thin presence of animal health input and service provision (). In addition, as described by an informant from Isiolo, people are sparsely distributed across the county, the government gives irregular free services, especially vaccinations, and due to the absence of services, people became accustomed to treating their own animals. The results of the scoring exercise, individual scores (out of 10 from the proportional piling exercise) of each attribute (knowledge, availability, quality, and affordability) are presented in , , and further illustrated in .
Figure 2. Changes in scores for different animal health service delivery attributes before, during, and after the mobile clinics.
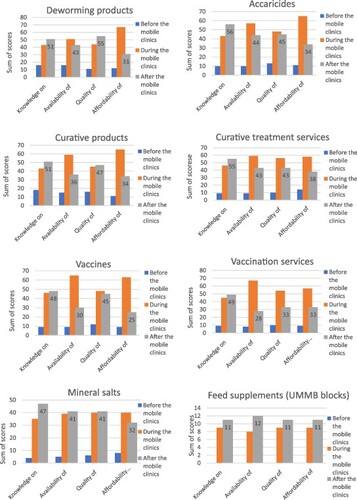
Table 4. Median test for difference in animal health products and services’ attributes before and after.
Table 5. Kendal’s W estimation for different animal health products/services attributes.
reveals that the scores of all the attributes increased during the time when the tested delivery system was implemented. While the score for some of the products/services’ delivery attributes fell after the tested delivery system, the scores remained higher than the before scores. The median test results () reveal that except for affordability of vaccines, the observed changes on all the animal health products and services’ attributes are statistically significant. The estimated Kendall’s W results imply that there was no agreement among informants across the study on the status of the attributes before the mobile clinics. This is expected since the sites varied in status of animal health products/service delivery, some sites being more remote than others, and some having had access to some form of animal health services (this was observed during baseline). However, there was strong significant agreement (concordance) among informants across the study sites on the status of the animal health service delivery attributes during (except for mineral salts) and after the tested delivery system (). The agreement was much stronger for some attributes such as curative products and vaccines. The level of agreement after the mobile runs, though strong, was lower than during the runs, reflecting that absence of the mobile clinic had a destabilising effect but did not return to pre-implementation status. These results therefore give a strong indication that the tested delivery system not only had a positive impact on knowledge on, availability of, quality of, and affordability of the animal health services and products, but that the impact went beyond the tested delivery system’s life – an indication of sustainability.
Proximity to the major towns was observed as a major factor that influenced the sustainability of the observed impacts, particularly in Isiolo county. In sites near major towns, scores for attributes continued to increase (in most cases) after the intervention, as opposed to sites furthest from major towns where the scores fell drastically after intervention. For instance, a positive change was observed after the intervention in sites near Isiolo town (in Shambani and Erimet) and drastic negative change for most of the attributes in sites furthest from Isiolo town (in Daaba and Kachuru).
The indicative impact on sustainability was surprising and unexpected. The tested delivery system, by design did not envision this kind of impact. Once the support ended, it was expected that either the implementers (Sidai and FACTs), would continue with the intervention, in case they realise its viability, or they would stop, letting people go back to the “before” scenario. However, despite the observed sustained change after the tested delivery system, the implementers did not continue with the mobile clinics, noting the huge logistical costs involved. The sustained impact from the intervention could have been due to the nature of the pastoral production and approaches after the mobile clinics stopped.
Pastoralists live in communal societies where people share knowledge and have a strongly developed socio-capital system. Those who gained knowledge from the mobile clinics shared it with other community members and helped them manage the animal health challenges they face. Moreover, after the tested delivery system, some communities living in remote areas would pool resources and send one person to buy the products on market days, as opposed to many individuals travelling to town, hence reducing the cost of transport. Informants from Daaba explained that such an arrangement would save them approximately US$23 per trip if ten people pool resources.
Moreover, the service providers devised ways of continuing with some aspects of the mobile clinic elements, albeit with a change of approach. FACTS in Garissa resorted to using CDRs (community disease reporters – initially trained as CAHWS before the practice was outlawed) because they can deliver specified non-veterinary products and services. FACTs would send some products (allowable by law) to the CDRs, who are paid a commission, by public transport, making the products and related services accessible to people in remote areas where the CDRs live:
The use of public transport and CDRs reduces transport and other logistics costs. By October 2018, FACTs had done this twice with very positive results, saving approximately US$50–70 per day and also being able to access non-motorable remote areas. However, use of public transport is limited by the need for cold chain transport for vaccines which cannot be done via public transport. (Study informant from Garissa)
In some areas, particularly in sites near Isiolo town and Garissa, traders and local shopkeepers who also stocked some animal health products established supply links with the two agrovets, Sidai Africa and FACTS, respectively. They have used these linkages to source animal health products, particularly from Sidai Agrovets. Sidai moved to strengthen these linkages by striving to provide sought-after products in ways that would support their profitable sale without necessarily increasing the prices paid by the final buyers. For instance, Sidai gets orders from these traders and sends them the products in bulk via public transport.
Attribution: factors that explain observed changes
Context analysis of the discussions with informants produced four themes as the drivers behind the changes in practices observed during and after the mobile clinics: (i) advisory services (bundled with the purchase of products); (ii) accessibility and affordability; (iii) linkages; and (iv) extending service provision (use of CDRs and franchisees).
The mobile clinic teams not only provided products and services for purchase but also advised community members on drugs, treatment, vaccines, mineral salts and application and storage of acaricides. They also gave advice on dosage and how to check the quality of the drugs. Moreover, Sidai used local radio stations to pass on the information about animal health problems and products.
Sasa ukidunga hii dawa ya sasa ya Sidai, ng’ombe inapona na kunona kabisa [when you inject the drugs from Sidai, the cattle get completely healed and fattened]. (Informants from Shambani)
Hata tunajua majina zao [we now know their names]. (Informant from Balambala)
By coordinating with the county government to provide vaccines (available for free in Marsabit county), bringing products and services to village level, at affordable prices, and bundling products with services (e.g. curative treatment service provided free upon purchase of drugs), the mobile clinics made it possible for the pastoralists to access quality and affordable products and services. The teams also provided good contacts and networks for curative treatment service during the runs:
Tuko na number zao za simu, tunaweza pigia hao wakatupa ushauri au tuwaite wakuje [we have their phone numbers, we can call them to request for advice or request them to come]. (Informants from Shambani)
Hawako mbali, tunawapa kwa simu [They are not far, we reach them by phone call]. (Informants from Balambala in Garissa)
Moreover, to extend service provision Sidai trained animal health assistants to provide vaccination services. In some points in Isiolo, Sidai established new franchisees who have motorbikes to deliver drugs, but not to all areas covered by the clinics. FACTS in Garissa used CDRs to take products closer to the pastoralists.
It is interesting to note that all four themes could be attributed to the mobile veterinary clinic intervention activities. As such, it can be confidently inferred that the intervention contributed to the observed impacts on animal health products/service attributes.
The impact on animal health service providers’ attributes
The results in reveal that stores combining both human medicine and agro-veterinary business formed the major block (43%) of actors supplying animal health products and services in the study area. There were also retail shops trading in household consumer goods alongside some basic animal health products. Very few (4%) private animal health service providers (veterinarians and trained animal health assistants) were found in the area. With the implementation of the mobile clinics, it was expected that the clinics would have some impact on the delivery of animal health services, particularly in terms of the interaction between different actors and the community, quality of products, quality of services, affordability, and accessibility.
Using the participatory actor scoring matrix scoring conducted during the study’s final evaluation, presents the estimation of Kendall’s W to assess the perceptions of informants regarding the impact of the mobile clinics on animal health goods/service providers. The estimations, further illustrated in , reveal a decline in the communities’ rating of government veterinary officials and a rise in the rating for agrovets and chemists, for all the service provider’s attributes (i.e. trust between the service provider and the community, the range of products and services offered by the provider, quality of advice offered by the provider, quality of service offered by the provider, accessibility of the products and services offered by the provider, and affordability of the products and services offered by the provider) after the mobile clinics. The median test results () reveal strong significant difference in trust, range of products and services, quality of advice, and quality of service for agrovets and chemists before and after the clinics. It also reveals significant difference in quality of advice, quality of service, accessibility, and affordability of government veterinary officials before and after the mobile clinics. Further, the Kendall’s W results reveal strong significant agreement (concordance) among informants across the study sites on the perceived attributes of the animal health providers and after the tested delivery system. Consequently, the results of the matrix indicate that the mobile clinics had a positive impact on the trust between the community and standard agrovets/chemists, range and quality of products and services offered, quality of advice and quality of services offered by standard agrovets/chemists.
Figure 3. Informant’s opinion on different animal health providers’ characteristics before and after the mobile clinics.
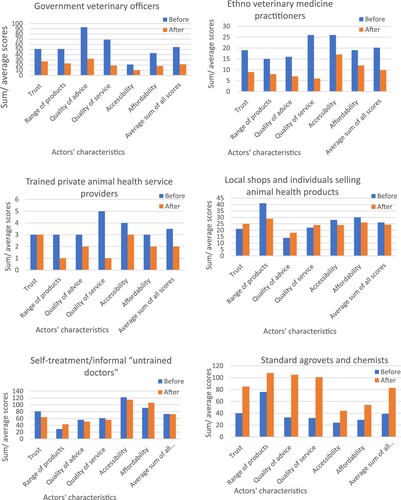
Table 6. Kendall’s W estimation for different animal health providers (actors) attributes, before and after mobile clinics.
Table 7. Median test for difference in animal health providers’ attributes before and after the mobile clinics.
From the discussions with the informants, it was observed that government veterinary officials were rare and their services very infrequent; sometimes it took them more than a year to receive any service from government officials. For ethnoveterinary medicine, the major challenges noted were that the success rates were low and the cost high. For instance, in Attan and Shambani (Isiolo county), informants observed that the practitioners are paid in kind (live goats) instead of cash, making it very expensive for minor treatment.
Before the mobile clinics, informants indicated a high score for self-treatment/informal “untrained doctors”, followed by government veterinary officers and standard agrovets. After the clinics, standard agrovets and chemists were scored very highly, above the others. After scoring each actor that is accessible in the study site, informants discussed the merits of these. A pairwise comparison matrix was used to evaluate the trade-offs that pastoralists make with regard to these characteristics. The results () show that quality of service was the top-ranked characteristic in Daaba, Attan, Bojidera, Kashuru, Nasuulu Headquarters (HQ) in Isiolo, Karare in Marsabit, and Balambala and Modogashe in Garissa. Quality of advice was ranked the second and third-most sought for characteristic in most sites except in Shambani and Attan, both sites in Isiolo. Informants in Nasuulu HQ stated that “we prioritise getting quality advice before looking at the range of products on offer”. Range of products offered by the animal health actors ranked the least sought for characteristic in most sites.
Table 8. Pairwise ranking of animal health actors’ attributes.
Willingness to pay
The willingness to pay (WTP) for animal health products and services brought closer to the pastoralists was found to range between 0 to 25% of the commonly bought products or services (). Only in three out of 11 sites did pastoralists indicate a WTP premium of more than 10% of the cost of a commonly bought product. Discussion with informants revealed four factors driving WTP: affordability, liquidity constraints, proximity to the nearest town, and the nature of the travel to towns. Affordability, implying the financial ability to purchase the inputs and services, was pointed out by majority of the FGDs (8 out of 11). Liquidity constraints were mentioned in one focus group, that some people did not having ready cash for purchasing yet they have livestock, and was also expressed by FACTS and Sidai. For instance, an informant in Garissa observed that:
Some pastoralists gave FACTS livestock in exchange for the products, this being a desperate situation where the pastoralists really needed the products but could not access cash to purchase them. Others asked for credit.
Table 9. Willingness to pay for animal health products through mobile clinics.
Profitability, cost and its implication on sustainability
An analysis of the service providers’ sales and revenues revealed that Sidai Africa had higher sales revenues and profits from Isiolo, compared to Marsabit. In Isiolo the highest profit margins were from the sale of minerals and vitamins, and vaccines. In Marsabit, vaccines provided the highest gross profit margin. In Garissa, vaccines and acaricides had the highest profit margins.
Further analysis of the service providers’ profitability was conducted by looking at the service providers’ entire gross margin during the period when the mobile clinics were conducted and comparing it to a similar period the previous year. reveals that the mobile clinic had a positive effect on the gross profits of the service providers. However, considering other direct costs, mainly logistics and additional personnel costs, the net profits for implementing the mobile veterinary clinic was negative, a loss of US$18,627 in Marsabit and Isiolo, and US$4,837 in Garissa. This implies that the logistical costs associated with organising and running the mobile clinics are prohibitive to private service providers. The loss is a disincentive for private sector players investing, without external support, in such an animal health delivery system.
Figure 4. Profit analysis: Service providers’ profits during the mobile run period against a similar period (months) the previous year in Isiolo (Sidai) and Garissa (FACTS). Notes: *(1 November 2017–2030 April 2018) **i.e. previous year (1 November 2016–2030 April 2017).
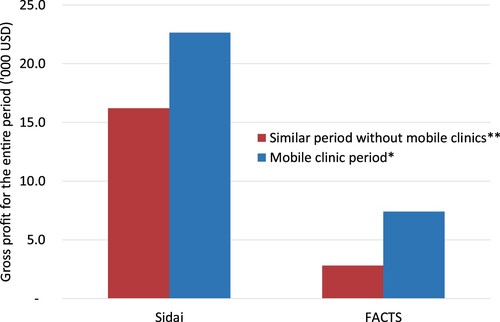
An informant from Garissa indicated that transportation cost was the prohibiting factor due to very long distances to reach out to pastoralists. Sidai also expressed concern over transport and logistical costs. An informant from Isiolo stated that “the best way to reach pastoralists with animal health products and services is to reduce transport costs by having local stockists selling products near farmers”. These sentiments concur with the results from the profit analysis, which revealed that huge losses would have been incurred by both service providers if costs of transport and other logistics are taken into consideration. It is worth noting that in testing the delivery system, the cost of transport and other logistics, including an extra human resource (an intern), which both service providers indicated was pivotal to the implementation of the mobile clinics, was borne by donor funding. It is also important to note that a local drug stockists option (at the village level, not a franchise system as proposed by Sidai) has been tested by development agents. Bett, Jost, and Mariner (Citation2008) found that local drug stockists were patchily distributed and rarely stocked sufficient quantities (and range) of veterinary drugs to satisfy local demand. Lessons from such interventions can be used to inform the recommendation by Sidai regarding expanding their local franchise network.
Implication and conclusions
The mobile clinics brought animal health service and inputs closer to the pastoralists and had a significant effect on the pastoralists’ knowledge on animal health, the availability, affordability and quality of animal heath inputs and services that pastoralists receive. It had positive effect on the attributes of private sector providers in the study area, on the trust between the pastoralists and the providers, the range of products and services, quality of advice, accessibility, and affordability of their products and services. This study’s observations reveal that pastoralists experienced good-quality products and services, leading to increased demand and modest willingness to pay for these services (a pull factor), albeit constrained by liquidity (lack of cash to purchase). While authors like Gustafson et al. (Citation2015) had previously highlighted the need to enhance communication and trust between pastoralists and animal health service providers in Tanzania, this paper shows that mobile clinics are part of the solution. However, the viability of private service providers (a push factor) stood in balance since without logistical support, private providers would make losses and hence find it unattractive to bring animal health inputs and services closer to the pastoralists. Nonetheless, given that this pilot was supported by donor funding, some of the costs were higher than would normally be paid by the providers. There is therefore scope for reduced logistical costs and improved profitability.
The delivery of vaccines by the private sector is highly restricted in Kenya, consequently, vaccines were not a central focus of the mobile clinics and were only delivered under the supervision of government veterinarians. However, vaccines had the greatest profit margin in all the counties. This indicates that vaccines, if given a stronger focus, have the scope to drive profitability higher. Routine vaccination practiced to the required level of coverage through the private sector by the pastoralists across the region, given the large livestock population and number of diseases to be controlled, would generate substantial revenues, making private mobile service delivery a more viable option. Besides, vaccination is a more appropriate disease control approach under pastoral conditions given the difficulties of providing clinical services. Widespread use of vaccines would also potentially reduce the need for antimicrobials and probably the risk of antimicrobial resistance. Therefore, the evidence from this study implies that the restriction on the delivery of vaccines is undermining the viability of the private sector in the provision of animal health services in ASALs. The viability of private sector delivery of vaccine also requires increased public awareness of the importance of routine vaccination through concerted efforts from the government, development partners, and the private sector to demystify pastoralists misconceptions and limited knowledge on vaccines:
Importantly, pastoralists placed a premium of quality advisory messages, consequently, greater effort should focus on how to provide extension services to pastoralists. This is an emerging area of possible partnership between the public and private sectors. As evident from this study, it is not economically viable for private sector to solely provide mobile animal health services in these ASAL areas without support. A possible public–private sector partnership would be for the public sector to subsidise the private sector’s logistic costs so that the private sector could deliver extension services alongside products and other animal health services to pastoralists. Such approach is worth considering in other pastoral areas of East Africa and beyond. The research has also shown areas for future research, including the level and type of subsidies required for the private sector to continue providing the services, pastoralists’ views about the value of the extension services provided and whether these will influence their willingness to pay.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Immaculate Omondi
Immaculate Omondi holds PhD in Agricultural Economics and Development Economics and works at the International Livestock Research Institute.
Isabelle Baltenweck
Isabelle Baltenweck holds PhD in Agricultural Economics and Development Economics and works at the International Livestock Research Institute.
Emmanuel Kinuthia
Emmanuel Kinuthia holds MSc. degrees in Agricultural and Applied Economics and work at the International Livestock Research Institute.
Leonard Kirui
Leonard Kirui holds MSc. degrees in Agricultural and Applied Economics and works at the International Livestock Research Institute.
George Njoroge-Wamwere
George Njoroge-Wamwere holds an MSc in Veterinary Epidemiology and Economics and works at the International Livestock Research Institute.
Bernard Bett
Bernard Bett holds PhD in Veterinary Epidemiology and Economics and works at the International Livestock Research Institute.
Ambrose Munene
Ambrose Munene, of Technoserve (Kenya), holds a BSc in agricultural economics.
Siyat Onle
Siyat Onle, of Farmers’ Agrisystems Capacity and Technical Solutions (FACTS), holds a BSc in agribusiness management and a diploma in animal health and production.
Diba Dida
Diba Dida, of Sidai Africa, holds an MSc in transboundary animal disease management.
Henry Kiara
Henry Kiara holds PhD in Veterinary Epidemiology and Economics and works at the International Livestock Research Institute.
Notes
1 Tropical livestock unit (TLU) is an aggregate measure of livestock holding where livestock numbers converted to a common unit using TLU equivalents. See Njuki et al. (Citation2011) for details of TLU calculations.
References
- Admassu, B., S. Nega, T. Haile, B. Abera, A. Hussein, and A. Catley. 2005. “Impact Assessment of a Community-Based Animal Health Project in Dollo Ado and Dollo Bay Districts, Southern Ethiopia.” Tropical Animal Health and Production 37 (1): 33–48.
- Affognon, H., P. Mburu, O. A. Hassan, S. Kingori, C. Ahlm, and R. Sang. 2017. “Ethnic Groups’ Knowledge, Attitude and Practices and Rift Valley Fever Exposure in Isiolo County of Kenya.” PLOS Neglected Tropical Diseases 11 (3): 1–12.
- African Union. 2013. “Policy Framework for Pastoralism in Africa: Securing, Protecting and Improving the Lives, Livelihoods and Rights of Pastoralist Communities.” Accessed 15 July 2020. https://cgspace.cgiar.org/bitstream/handle/10568/81080/1735_PDF.pdf?sequence=1&isAllowed=y.
- AU-IBAR (African Union – Interafrican Bureau for Animal Resources). 2010. “Framework for Mainstreaming Livestock in the CAADP Pillars.” Accessed 15 July 2020. www.igadhost.com/igaddata/docs/ibarCAADP_en.pdf.
- Bett, B., C. Jost, and J. C. Mariner. 2008. “Participatory Investigation of Important Animal Health Problems Among the Turkana Pastoralists: Relative Incidence, Impact on Livelihoods and Suggested Interventions.” Discussion Paper No. 15. International Livestock Research Institute.
- Breu, T., F. U. Höggel, A. Lannen, and H. Rueff. 2015. “Sustainable Livestock Production? Industrial Agriculture versus Pastoralism.” CDE Policy Brief No. 7. Centre for Development and Environment.
- Catley, A., J. Burns, D. Abebe, and O. Suji. 2008. “Participatory Impact Assessment: A Guide for Practitioners.” Accessed 15 July 2020. www.livestock-emergency.net/wp-content/uploads/2017/10/PIA-Guideline.pdf.
- Catley, A., J. Lind, and I. Scoones. 2016. “The Futures of Pastoralism in the Horn of Africa: Pathways of Growth and Change.” Revue scientifique et technique (International Office of Epizootics) 35 (2): 389–403.
- Caudell, M. A., M. B. Quinlan, M. Subbiah, D. R. Call, C. J. Roulette, J. W. Roulette, A. Roth, L. Matthews, and R. J. Quinlan. 2017. “Antimicrobial Use and Veterinary Care among Agro-Pastoralists in Northern Tanzania.” PLoS ONE 12 (1): 1–18.
- de Haan, C., T. Robinson, G. Conchedda, P. Ericksen, M. Said, L. Robinson, F. Flintan, et al. 2016. “Livestock Production Systems: Seizing the Opportunities for Pastoralists and Agro-Pastoralists.” In Confronting Drought in Africa’s Drylands: Opportunities for Enhancing Resilience, edited by R. Cervigni, and M. L. Morris, 47. Washington, DC: World Bank-AFD.
- FAO. 2001. “Pastoralism in the New Millennium.” Animal Production and Health Paper No. 150. Accessed 15 July 2020. www.fao.org/DOCREP/005/y2647e/y2647e00.htm.
- GoK (Government of Kenya). 2012. “Vision 2030: Development Strategy for Northern Kenya and Other Arid Lands.” Nairobi: Government of Kenya.
- Gustafson, C. R., E. VanWormer, R. Kazwala, A. Makweta, G. Paul, W. Smith, and J. A. K. Mazet. 2015. “Educating Pastoralists and Extension Officers on Diverse Livestock Diseases in a Changing Environment in Tanzania.” Pastoralism 5 (1): 1–12.
- Haro, G. O., G. J. Doyo, and J. G. McPeak. 2005. “Linkages Between Community, Environmental, and Conflict Management: Experiences from Northern Kenya.” World Development 33 (2): 285–299.
- Heffernan, C., and F. Misturelli. 2002. “The Delivery of Veterinary Services to the Poor: Preliminary findings from Kenya.” Accessed 15 July 2020. https://assets.publishing.service.gov.uk/media/57a08d2aed915d3cfd001868/R7359a.pdf.
- Herrero, M., and P. K. Thornton. 2013. “Livestock and Global Change: Emerging Issues for Sustainable Food Systems.” PNAS 110 (52): 20878–20881.
- Higham, L. E., W. Ongeri, K. Asena, and M. V. Thrusfield. 2016. “Characterising and Comparing Animal-Health Services in the Rift Valley, Kenya: An Exploratory Analysis (Part I).” Tropical Animal Health and Production 48 (8): 1621–1632.
- Ilukor, J. 2014. “An Analysis of Institutional Arrangements for Providing Animal Health Services: A Theoretical Framework and Empirical Evidence from Kenya and Uganda.” PhD diss., University of Hohenheim. Accessed 15 July 2020. http://opus.uni-hohenheim.de/volltexte/2016/1139/pdf/John_Ilukor_Dissertation_2015_Final.pdf.
- Ilukor, J. 2017. “Improving the Delivery of Veterinary Services in Africa: Insights from the Empirical Application of Transaction Costs Theory in Uganda and Kenya.” Revue scientifique et technique (International Office of Epizootics) 36 (1): 279–289.
- Ilukor, J., R. Birner, and T. Nielsen. 2015. “Addressing Governance Challenges in the Provision of Animal Health Services: A Review of the Literature and Empirical Application Transaction Cost Theory.” Preventive Veterinary Medicine 122 (1–2): 1–13.
- Kaufmann, B., C. G. Hulsebusch, and S. Kratli. 2018. “Pastoral Livestock Production Systems.” In Encyclopedia of Food Security and Sustainability (Vol. 1), edited by P. Ferranti, E. M. Berry, and J. R. Anderson, 178–186. Oxford: Elsevier.
- Krätli, S., C. Huelsebusch, S. Brooks, and B. Kaufmann. 2013. “Pastoralism: A Critical Asset for Food Security Under Global Climate Change.” Animal Frontiers 3 (1): 42–50.
- Lamuka, P. O., F. M. Njeruh, G. C. Gitau, and K. A. Abey. 2017. “Camel Health Management and Pastoralists’ Knowledge and Information on Zoonoses and Food Safety Risks in Isiolo County, Kenya.” Pastoralism 7 (20): 1–10.
- Marsh, T. L., J. Yoder, T. Deboch, T. F. McElwain, and G. H. Palmer. 2016. “Livestock Vaccinations Translate Into Increased Human Capital and School Attendance by Girls.” Science Advances 2 (12): 1–16.
- Mugunieri, G. L., P. Irungu, and J. Omiti. 2004. “Performance of Community-Based Animal Health Workers in the Delivery of Livestock Health Services.” Tropical Animal Health and Production 36 (6): 523–535.
- Mwanyumba, P. M., R. W. Wahome, L. MacOpiyo, and P. Kanyari. 2015. “Livestock Herd Structures and Dynamics in Garissa County, Kenya.” Pastoralism 5 (26): 1–16.
- Njuki, J. M., J. Poole, N. Johnson, I. Baltenweck, P. Pali, Z. Lokman, and S. Mburu. 2011. “Gender, Livestock and Livelihood Indicators.” Accessed 15 July 2020. https://cgspace.cgiar.org/bitstream/handle/10568/3036/Gender%20Livestock%20and%20Livelihood%20Indicators.pdf?sequence=4&isAllowed=y.
- Nyanjom, O. 2014. “Remarginalising Kenyan Pastoralists: The Hidden Curse of National Growth and Development.” African Study Monographs 50: 43–72.
- Okwiri, F. O., J. Kajume, and R. K. Odondi. 2001. “An Assessment of the Economic Viability of Private Animal Health Service Delivery in Pastoral Areas in Kenya.” African Union/Interafrican Bureau for Animal Resources.
- Onono, J. O., P. Alarcon, M. Karani, P. Muinde, J. M. Akoko, C. Maud, E. M. Fevre, B. Haesler, and J. Rushton. 2018. “Identification of Production Challenges and Benefits Using Value Chain Mapping of Egg Food Systems in Nairobi, Kenya.” Agricultural Systems 159: 1–8.
- Rubyogo, J. C., P. M. Murithii, G. J. O. Agumbah, and G. Obhai. 2005. “Sustainability of a Privatized Community-Based Animal Health Worker System in Mwingi District, Kenya.” Tropical Animal Health and Production 37: 253–266.
- Rutabanzibwa, A. P. 2002. “Veterinary Legal Reform in Tanzania.” Primary Animal Health Care in the 21st Century: Shaping the Rules, Policies and Institutions, 15–18 October, Mombasa, Kenya.
- Scoones, I., J. Lind, N. Maru, M. Nori, L. Pappagallo, T. Shariff, G. Simula, J. Swift, M. Taye, and P. Tsering. 2020. “Pastoralism and Development: Fifty Years of Dynamic Change.” IDS Bulletin 51 (1A): 1–20.
- Smith, J., K. Sones, D. Grace, S. MacMillan, S. Tarawali, and M. Herrero. 2013. “Beyond Milk, Meat and Eggs: Role of Livestock in Food and Nutrition Security.” Animal Frontiers 3 (1): 6–13.
- Young, J., J. Kajume, and J. Wanyama. 2003. “Animal Health Care in Kenya: The Road to Community-based Animal Health Service Delivery.” Working Paper No. 214. Overseas Development Institute. Accessed 15 July 2020. www.odi.org/sites/odi.org.uk/files/odi-assets/publications-opinion-files/178.pdf.