
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
This study assessed effects and drivers of mother–child pair participation in agriculture-nutrition-health linkage projects. Data were collected from 2,271 households in Kenya. Three categories of participation regime were defined: none, partial and full participation. Bivariate analyses and multinomial-logit regression were used to assess the effects and drivers of participation, respectively. Results found higher diet quality and consumption of vitamin A foods, and more frequent visits to ante-natal clinics, among full participants. Regression results showed that partial and full participation decreased with the caregivers’ age, de-incentivisation of community health workers and health facility linkage, but increased with dependency ratio and wealth.
1. Introduction
Considerable progress has been made over the past two decades in reducing the prevalence of chronic malnutrition or stunting among young children in the world. Children stunted before two years of age are at higher risk of poor cognitive development and illness than non-stunted children (FAO et al. Citation2017). Globally, the prevalence of stunting has declined from 32.7% in 2000– to 22.9% in 2016 (UNICEF/WHO/World Bank Group Citation2017). However, stunting has declined twice as fast in Latin America and Asia as in sub-Saharan Africa (SSA). Currently, an estimated 54 million children under five years of age in SSA are stunted, with prevalence rates ranging from 33.2% in Southern Africa to 45.6% in Eastern Africa (UNICEF/WHO/World Bank Group Citation2017).
Despite progress, micronutrient-deficiency related malnutrition still remains a major concern in SSA. Among these, vitamin A deficiency (VAD) can lead to eye damage and xeropthalmia (leading to night blindness), weakened immunity, and general increase in the incidence and severity of infectious diseases and mortality (Schmitz et al. Citation2012; Low et al. Citation2017; Shikuku et al. Citation2019). VAD has also been linked to birth-related deaths among pregnant women. Furthermore, Villamor and Fawzi (Citation2005), Mayo-Wilson et al. (Citation2011) and Jones and de Brauw (Citation2015) argue that VAD is linked to increased incidence of measles and diarrhoea, both of which are associated with high child mortality.
It is estimated that 190 million pre-school age children suffer from VAD (2005 estimates), with 56.4 million in Africa (WHO Citation2009). A recent effort determining dietary micronutrient supplies found that SSA, as of 2011, had the highest estimated prevalence of inadequate intake of vitamin A and the second highest for iron, calcium, vitamin C, vitamin B12, zinc and niacin among the regions of the world (Beal et al. Citation2017). Moreover, SSA was the only region where dietary micronutrient density declined between 1961 and 2011.
Most governments address the problem of VAD by the distribution of high dose vitamin A capsules to young children at specific periods when they are most vulnerable to VAD (Bhutta and Baker Citation2015). However, this strategy has often proved ineffective due to access constraints, with reversal of gains in some cases (Ramakrishnan et al. Citation1999; Benn et al. Citation2015; Mason et al. Citation2015). In many developing countries, interventions to address micronutrient malnutrition have included kitchen/home gardening (Wijaya et al. Citation2010; Mohsin et al. Citation2017), promotion of fruit and vegetable consumption as sources of micronutrients (Dhandevi and Jeewon Citation2015), and biofortification (Low et al. Citation2017). Repjin et al. (ibid), for instance, report that home gardening increased the supply of vitamin A to households in Bangladesh by 189%. Mohsin et al. (Citation2017) found similar benefits from kitchen gardening in Pakistan. Dhandevi and Jewoo argue that increased vegetable consumption has the additional benefits of supplying other dietary ingredients including antioxidants, and recommend the use of multiple complementary interventions to address malnutrition. In Sub-Sahara Africa (SSA), complementary strategies for tackling the high prevalence of VAD have focused on industrial fortification of foods and, more recently, the biofortification of food staples (Low et al. Citation2017; Pambo, Otieno, and Okello Citation2017). The former involves addition of essential micronutrients into commonly consumed foods such as maize flour, sugar, cooking coils, butter/margarine and infant foods (Bromage et al. Citation2018; Cardoso et al. Citation2019). Biofortification, on the other hand, is a food-based approach that entails increasing the micronutrients in widely consumed food staples through conventional breeding processes (Nestel et al. Citation2006; Jones and de Brauw Citation2015). Since pro-vitamin A rich orange-fleshed sweetpotato (OFSP) contains energy as well as good levels of vitamin C and several B vitamins (Low et al. Citation2017), it is particularly important for SSA where many countries are still far below having their food supplies meet per capita energy requirements (Beal et al. Citation2017).
Past studies show that consumption of some of the vitamin A-rich biofortified staples can reduce the incidence of VAD, as well as illnesses associated with it (Hotz et al. Citation2012; Christinck and Weltzien Citation2013; Jones and de Brauw Citation2015; Laurie et al. Citation2015; Low et al. Citation2017). Specifically, Low et al. (Citation2017) and Hotz et al. (Citation2012) found evidence that consumption of vitamin A-rich sweetpotato combined with community level education reduced levels of VAD among target populations in Mozambique and Uganda, respectively. Jones and de Brauw (Citation2015) further found that the integrated biofortified sweetpotato-nutrition education approach reduced the incidence of childhood diseases, including diarrhoea, among children under two and five years of age in Mozambique. Laurie et al. (Citation2015) discuss similar benefits of biofortification in South Africa. Among the biofortified crops, the orange-fleshed sweetpotato (OFSP) has shown the greatest potential in combating VAD. Consumption of about 125 g of boiled orange-fleshed sweetpotato (OFSP) roots can supply the vitamin A requirement of a young child (Low et al. Citation2017).
Evidence of the potential to combat VAD using food-based agricultural interventions has led to increased investment in community-based projects that promote the production and consumption of OFSP by vulnerable households. However, the effects of such projects on nutritional, and hence health, outcomes greatly depends on the intensity with which targeted households participate in them (Jones and de Brauw Citation2015), though what factors drive participation in such community-based projects remain unclear. Jones and de Brauw (ibid) specifically find that the degree of participation in agriculture-nutrition interventions affects the outcomes of such interventions. Yet, past studies often treated participation in such community projects as though it was uniform; thus, in some cases, finding no effect of such interventions (Kass and Kolasa Citation1978; Brun, Reynaud, and Chevassus-Agnes Citation1989). This paper uses data collected from the endline survey of villages that participated in Mama SASHA project, a large agriculture-nutrition-health community intervention in western Kenya designed to address this issue. We first investigate the impact of degree of participation on nutritional outcomes and then proceed to investigate the drivers of participation in the different regimes of intervention. The latter captured the intensity of intervention in terms of services the participating household decided to receive from the project.
1.1. Study context
Mama SASHA was a four-year (2010–2013) quasi-experimental proof-of-concept project in Bungoma and Busia counties of western Kenya that linked delivery of planting material of OFSP with antenatal and postnatal care and enhanced nutrition education and counselling (Cole et al. Citation2016). There were four intervention health facilities where nurses were trained and provided with nutrition education flipcharts and vouchers for OFSP, and four control health facilities. At the intervention facilities, participants of the project were pregnant women and their subsequent offspring. Pregnant women receiving nutrition counselling at ante-natal care facilities and women having given birth recently attending post-natal clinics, received vouchers for OFSP vines that they could redeem at trained vine multipliers near health facilities. These pregnant and lactating women were also encouraged to attend community-level monthly mother-to-mother club meetings where trained community health workers (CHWs) provided further nutrition education and conducted cooking demonstrations of enhanced porridges for young children using OFSP and other locally available ingredients.
Participating households were urged to plant OFSP and consume it in the family and feed it, preferably as part of an enriched porridge, to young children. They, however, had a free-hand to decide the extent to which they would participate in different project activities designed to enhance provision of nutrition knowledge and hence influence feeding practices and diet quality.
2. Study methods
2.1. Empirical framework
This study uses descriptive statistics from the endline household survey to assess the outcome of participation in the project and the discrete choice model (DCM) to assess the choice of the level/intensity of participation. The descriptive statistics used include the means, standard errors and the p-value of the test of differences in mean outcomes between treatment/participant groups and the control groups.
DCM has been used widely in assessing the factors that affect the choice of an activity or event by an individual among a set of available options (Lapar et al. Citation2009). For instance, they have been used to assess the drivers of choice of the preferred retail outlet by consumer (Moore Citation1989; Okello et al. Citation2012) and choice of marketing arrangement/outlet by producers (Ondieki-Mwaura et al. Citation2013). In this paper, we use the multinomial logit (MNL) regression, a DCM, to assess the drivers of choice of the level of participation in a project with various gradations of participation levels. The underlying principle of DCM is that an individual or household acts to maximise utility within a range of constraints. In the context of this study, an individual’s or household’s choice of the extent of participation is therefore assumed to be the result of a subjective selection of the most preferred alternative from a restricted set of objectives. In this study, the choice is made among types of project participation.
In choosing the extent of participation in a project, the individual/household must internalise, among others, the location, personal and household-specific factors as well as the transaction costs involved. The first set of factors, the choice of type of participation in the Mama SASHA project, is likely to be affected by: household composition, period of birth of the child targeted by the project, incentives/rewards to project service providers such as the CHWs and other partners, and the crop/OSFP production aspects. Transaction costs of participation include the distance to the linked health facility and time spent in project activities such as attending the mother-to-mother club meetings.
The MNL model estimated in this study allows for the estimation of the probability that the jth participation type is chosen by the ith individual as the most preferred alternative, relative to not participating at all. We therefore estimated models of the form:
(1)
(1) where β represents the vector of coefficients to be estimated, X is the vector of covariates and ϵ is the stochastic term.
The dependent variable P is a discrete choice corresponding to the most preferred participation type. The participation types are: no participation (i.e. none), partial participation and full participation. Full participation occurred when the targeted individual/household chose participation in the whole suite of project-planned activities including visits to ante-natal clinics (ANC), attending mother-to-mother club meetings, and growing and consuming OFSP. Partial participation, on the other hand, occurred when the individual/household participated in only some of the activities, i.e. either attending the ANC, growing and consuming OFSP; or just participating in the pregnant women’s club. The no-participation group comprised households in villages targeted by the project which did not use any of the services provided by the project. The explanatory variables, i.e. the vector X, included location, personal and household-specific factors as well as transaction cost variables. The former included education, age, wealth index, access to land in the lowlands and dummies for the linked facility variables, while transaction costs were proxied in this study by the distance to the linked health facility. The choice of the variables was based on the literature and a priori expectations.
Two MNL regression models were estimated to assess the factors influencing the intensity of participation in the Mama SASHA project. The first model contained all the variables hypothesised to influence the participation regime chosen, based on the literature and a priori expectation, and hence is called a full (unrestricted) model. The second, however, had some of the variables that were insignificant dropped after a Wald test of joint exclusion indicated that they did not jointly explain the variability in the dependent variable. This second model thus yielded the partial (restricted) model.
2.2. Data
This study is based on village-level cross-sectional data collected as part of the Mama SASHA endline survey between March and May 2014. The households interviewed in this study were sampled using a two-stage cluster sampling technique. The sampling proceeded as follows: first, the linked health facilities were purposively selected and stratified by the treatment type as intervention and control, depending on whether the facility was in the area targeted by the project (intervention) or not (control). The former (Ndalu, Naitiri, Sinoko and Mihuu) were the facilities where households/caregivers in associated villages had been advised to visit for pre- and ante-natal care and from which they received nutrition education. The latter (Tongaren, Makhonge, Budalangi and Mukhobola), on the other hand, were the facilities that fell in the control areas, where usual care and services were provided to the surrounding villages. Note that all women had alternative choices for health care within the catchment areas of the study facilities. Indeed, data showed that 73% of the non-participant women in the intervention areas attended health facilities other than the four selected intervention facilities and their associated outreach dispensaries. These women simply did not have access to the antenatal care counsellling at the clinic and voucher opportunity.
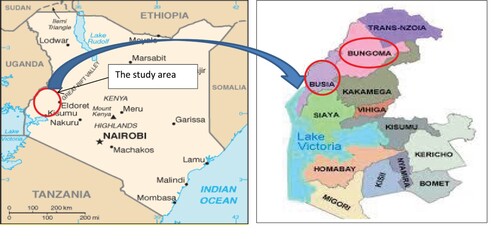
Next, a two-stage cluster sampling design was used to select villages and households. In the first stage sample points (“clusters”) were selected using a probability proportionate-to-sizeFootnote1 cluster sampling technique with villages as clusters. The villages comprised those covered by the selected health facilities. The second stage involved the selection of, on average, approximately sixty-eight households within each selected cluster (village), using systematic random sampling from the list obtained by enumeration. The survey was administered to households with children 6–23 months of age, with all eligible mother–child pairs and approximately one in three pregnant women being systematically included in the sample. This process resulted in 1,108 and 1,163 households being interviewed in the control and intervention areas, respectively, across 129 villages. Among the 1,163 households from the intervention areas, 536 did not participate in the project all, 390 participated partially, while the remaining 237 participated fully. The study locations are shown in .
Figure 1. Map of Kenya and western region showing the area where the study was conducted.
Data on dietary diversity were collected based on 24-hour recall of foods consumed by the reference child (i.e. a child under 5 years) and the caregiver. We used the standard 24-hour recall protocol adopted from Swindale and Bilinsky (Citation2006) and FAO and FHI 360 (Citation2016). The foods were grouped into: starchy staples, legumes and nuts, milk and dairy products, vegetables, fruits, meat (including organ, flesh and fish meat), eggs, and oil. Each group was captured as a binary variable equal to one if the child or caregiver consumed the food seven days preceding the survey and zero otherwise. The scores are therefore summations across the food consumed. The Child DDS was constructed using nine foods groups as recommended by Swindale and Bilinksy (2006) and FAO and FHI 360 (Citation2016). These were: Starchy staples; Legumes, Nuts, Seeds; Dark green leafy vegetables; Milk and milk products; Eggs; Flesh meat/fish; Organ meat; Vitamin A rich vegetables and fruits; Other fruits and vegetables. Caregiver DDS was, on the other hand, computed based on 10 food groups, namely Grains, white roots and tubers, and plantains; Pulses/Legumes (beans, peas and lentils); Nuts and seeds; Dairy products; Meat, poultry and fish; Eggs; Dark green leafy vegetables; Other vitamin A-rich vegetable; Other vegetables; and, Other fruits. Given the interest in vitamin A foods, we also collected data on consumption of various vitamin A rich foods, including orange-fleshed sweetpotato roots and leaves, using the Helen Keller International (HKI) Food Frequency protocol. The HKI protocol is a qualitative seven-day recall of the number of times that a child–mother pair consumed selected vitamin A rich foods (Sloan and Rosen Citation1997; Ramakrishnan et al. Citation1999).
In addition to the foods consumed by the mother–child pairs, data was also collected on household demographics (including mother/caregiver and child), locational variables, land access, and asset/wealth endowments. Data were entered using CSPro version 4.0 data entry software and analysed using STATA Version 14. A full list and description of the variables used to estimate the regression models in Equation (1) are given in below.
Table 1. Definition and descriptive statistics of the explanatory variables used in the MNL regression model.
3. Results
3.1. Characterising study households
The summary statistics in show that the majority (84%) of the households planted sweetpotato at least some time during the three years prior to the endline survey, had very small land holdings, averaging only about 1.5 acres, and did not have access to lowland areas (i.e. wetlands that can support a second season of OFSP production during the dry season in the uplands). Caregivers/mothers of the targeted children (i.e. children under two years of age) had a mean age of 29 years. About 30% of the children in the survey households were born after the incentives to CHWs (i.e. monetary stipend given to CHWs for their role in promoting project activities) had been dropped by 50% (from 1000 Ksh ($11.6 USD at 2014 exchange rates) per month to 500 Ksh ($5.8)), at the direction of the Ministry of Health.
3.2. Outcomes of participation in the Mama SASHA project
summarises the results of analysis of the quality of diets (measured in form of dietary diversity scores – DDS) of households in targeted villages versus non-targeted ones (i.e. control). It further disaggregates the outcomes by the regime of participation. The results show that households in targeted (intervention) villages fared much better than their counterparts in control villages. Indeed, the mean of both the mean Child DDS and Caregiver/woman DDS are significantly higher among the intervention households. The last three columns provide the DDS by the regime of project participation. Notably, the DDS for both the child and the woman increased with the number of services received (i.e. the regime of participation). Thus, the Child DDS for full participants was higher for full participants (4.05, p-value = 0.000) and partial participants (3.52, p-value = 0.000) than for non-participants (3.35, p-value = 0.018). A similar trend is observed for Caregivers’ DDS. These findings therefore suggest that the extent of participation in the project had a significant effect on quality of diets consumed by the targeted children and mothers.
Table 2. Mean child and caregiverTable Footnotea diet diversity scores (DDS) based on 24-hour recall of foods consumed.
The consumption of various vitamin-A rich foods by 6–23-month old children in the control and participant households is based on the seven-day recall period. captures the percentage of children consuming the item at least one day during the past week. As in the case of DDS, the results show that the effect of participation in the project is more pronounced among households that participated fully (used most of project services). Most importantly the results indicate that in many cases, simply comparing the control group and the intervention group could mask the effect of project participation. For instance, consumption of pumpkin and amaranth leaves, ripened papaya, was significantly higher among full participants (p-value: 0.008, 0.022 and 0.001, respectively) than the control group, but not significantly different for partial participants (p-value: 0.938, 0.857 and 0.931, respectively). Moreover, for some foods such as green leafy vegetables and carrots, consumption increased with the type of participation. For carrots, for instance, there was higher consumption among full participants (16%, p-value = 0.04) than partial (9%, p-value = 0.014) and non-participants (7%, p-value = 0.011). Similarly, compared to the control group, there was higher consumption of ripened mango among full participants (61%, p-value = 0.032) than partial participants (48%, p-value = 0.025). Furthermore, as in the case of DDS, the results indicate that the effect of participation in the project becomes stronger and more statistically significant as the extent of participation increases. Overall, these results show that: (1) the degree to which beneficiary households participated in the project influenced the magnitude of the benefits obtained; (2) there was greater consumption of vitamin A-rich foods even among households which do not participate in the project at all but are in the intervention areas, likely due to village-level spillover effects; and (3) comparison of intervention with the control groups without paying attention to the different degrees of participation would mask the effect of project.
Table 3. Proportion of children 6–23 months of age consuming other vitamin A-rich foods during the seven-day period.
The degree of participation in the community-based nutrition-sensitive agricultural project also affected caregivers’ health-seeking behaviours (). Pregnant women who participated in the project partially and fully, on average, made more frequent visits to ANC (4.51, p-value = 0.002 and 4.61, p-value = 0.001, respectively, compared to the control) than non-participants (3.87, p-value = 0.005). Moreover, full participants began attending ANC earlier in their pregnancy (3.37 months; p-value = 0.001) than non-participants (3.37 months, p-value = 1.07). The association of participation and the distance travelled to the ANC was however mixed, with results being insignificant for both non-participants and full participants compared to control participants. However, partial participants walked longer distances (44 min, p-value = 0.005) to reach the linked health facility than the control group (39 min).
Table 4. Effect of participation on health-seeking behaviours of pregnant women.
In line with Jones and de Brauw (Citation2015), the findings of this study have demonstrated that the extent of using project services affects the nutrition and health outcomes. Indeed, the discussion above has shown that the degree of participation in the agriculture-nutrition-health linkage projects affects diet quality, the consumption of vitamin A-rich foods and health-seeking behaviours. They show that the project intervention yielded better nutrition and health condition of the community. This is in line with the findings of Wijaya et al. (Citation2020) and Mariyono (Citation2018) which showed that programme changes implemented by the government increased livelihood quality in terms of nutrition and human capital.Footnote2 The question then is what motivates households in intervention (treatment) villages to participate fully, partially or not participate at all. In the next section, we turn to this question by investigating the factors that explain the extent of participation in the Mama SASHA project.
3.3. Drivers of participation in Mama SASHA project
The results of the unrestricted and restricted MNL models are presented in . The models were estimated using robust standard errors to correct for any form of heteroskesdasticity. The model statistics, shown by the very low p-values (0.000), indicate that the estimated models are highly significant at any conventional level significance. Specifically, they indicate that the models have good fit for the data.
Table 5. Results of the MNL regression models showing factors affecting the choice of level of participation in Mama SASHA project.
The results of the unrestricted and restricted models are quite similar indicating that the estimated model is quite stable and robust. Specifically, the number of variables that are significant, the direction of effect, and the pseudo-likelihood ratios are largely the same in both models. Consequently, we here discuss only the restricted model because it captures the significant factors driving participation compared to households who did not participate at all.
3.3.1. Factors affecting the likelihood of partial participation in the project
Focusing on the restricted model, results show that the likelihood of participating partially rather than not at all is affected by some household and individual-specific characteristics, wealth endowment, access to the linked facility, and reduction in the incentives to CHWs. Specifically, the older the caregiver and having the head of household not being the father or mother of the child significantly reduced the likelihood of partial participation in the project rather than non-participation. Prior experience in the production of sweetpotato, however, increased the likelihood that the respondent participated partially in Mama SASHA project. also shows that respondents who had their children born after the incentives to CHWs had been reduced were less likely to have participated in the project, even partially. CHWs were recruited from the intervention communities and were also engaged in encouraging pregnant women to attend ante-natal care services. Thus, this finding indicates that participation in a community-based nutrition-focused project is sensitive to the promotional and health education role played by community nutrition facilitators. It further demonstrates the importance of involving community members in community-based projects and also providing them with adequate incentives to carry out project activities, and therefore corroborates the findings of Smitasiri et al. (Citation1999).
As expected, distance to the linked health facility had a negative effect on the likelihood of partial participation versus non-participation. Thus, respondents who were further away from the linked health facility were less likely to participate in the project at all. The finding that distance is also a factor affecting the project participation is in line with the findings of Mariyono (Citation2019) who also found a negative effect of distance on project participation. Overall, these findings suggest that the high transaction costs of accessing community-based agriculture-nutrition-focused projects benefits can reduce the utilisation of the benefits from such projects.
The probability of partial participation in the Mama SASHA project was also driven by the kind of linked health facility the individual/household was advised to attend. As shown, respondents in the Sinoko and Mihuu health centre catchment areas were less likely to participate in the project partially. This finding may be related to the kind of services and the way services were offered at these linked health facilities or that residents were using alternative options in the catchment areas.
3.2.2. Factors influencing the likelihood of full to participation in the intervention
The last two columns of present the results of the restricted model estimated to assess conditioners of the likelihood of full participation in the project. Interestingly, unlike the partial participation model, results show that dependency ratio (that is the ratio of number of dependent members to the active members of the household expressed as percentage) affects the likelihood of full project participation, compared to not participating at all. The higher the dependency ratio, the more likely the respondent were to participate fully in the Mama SASHA project, other factors held constant. In addition, unlike the partial model, wealth has a moderately strong effect on the likelihood of full participation, which was not the case for the partial participation results. Results show that wealthier respondentsFootnote3 were more likely to fully participate in the Mama SASHA project as opposed to not participating at all. It is possible that the individuals/households that were better endowed with land and other resources were more able to spend the time and effort required for full participation. Such resources may include the labour to grow and maintain sweetpotato or perform household chores, access to transportation to visit the health facilities, and pay fees for some services at the health facility.
Results also show that the other individual/household-specific factors (i.e. age of caregiver and child being raised by another relative) had the same effect as in the partial participation model. Households with older caregivers and other relatives as heads were less likely to participate in the project fully. This finding probably reflects the fact that older caregivers might have considered themselves more experienced in personal and child care, thus did not see the need to participate in an intervention aimed at helping them raise healthy children or to eat well during pregnancy. The rest of the factors that affected the likelihood of participating fully in the project as opposed to not at all are similar to those of the partial participation model discussed above. They indicate that there was less likelihood that the respondents participated fully than partially in the project when the child was born after the CHW support had been reduced, when the health facility was far away, and when the catchment areas was for the Naitiri or Sinoko health facilities. Nonetheless, facility linkage had a joint significant effect on participation level chosen. Indeed, A Wald test of joint significance of facility linkage yields a Chi-Square Statistic of 41.21 and p-value of 0.0000.
4. Summary, conclusion and implications
Most past studies have mainly focused on demonstrating the effectiveness of an agriculture-nutrition education intervention using OFSP as a key entry in increasing vitamin A intakes and combating vitamin A deficiency (VAD) (Low et al. Citation2017; Hotz et al. Citation2012). In this paper, we examined the outcome of varying degrees of participation in a community-based project targeting improved young child feeding practices, improved ante-natal nutrition services for pregnant women, and reduction of VAD among young children and the factors that affect the extent to which an individual/household participates in such interventions. We used bivariate analyses and a multinomial logit regression technique to assess the effects of participation, and factors that influence the likelihood, by targeted households, to participate fully, partially or not participate all, in an agriculture-health/nutrition-based project implemented in western Kenya from 2010 to 2013.
The results of analysis of the outcomes of participation in the project support the argument that the benefits of community-based agriculture-nutrition interventions are moderated by the degree of participation in such projects. The degree of participation affected quality of diets, consumption of vitamin A-rich foods and caregivers’ health-seeking behaviours. In addition, there was greater consumption of vitamin A-rich foods even among households which do not participate in the project at all but were in the intervention areas, probably due to spillover effects. Furthermore, the findings demonstrate that failure to look at different types of participation in assessing the impact of agriculture-nutrition-health linkage projects can mask project effects. The findings also demonstrate that the likelihood of full or partial participation in a project is affected by individual/personal and household level characteristics, household wealth endowment, health service incentive system offered to community nutrition promoters, and the transaction costs associated with nature of the linked health facilities. It specifically finds that some of these factors (e.g. wealth and dependency ratio) explain fuller participation in the project.
This paper concludes that participation in the Mama SASHA project positively affected the diets (i.e. nutrition outcomes) and health-seeking behaviours of participants, and that magnitude of effect depended on the degree/intensity of participation. It also concludes that the intensity of participation in such agriculture-nutrition-health projects is affected by both personal and household-specific factors as well as non-household-specific factors, and that wealth and the nature of the linked facility are important in encouraging the choice of the type of participation in agriculture-nutrition-marketing interventions aimed at promoting the production and consumption of OFSP by vulnerable households. Findings imply the need to consider both household and non-household (e.g. distance to health facility) factors and the systems of incentives for motivating the delivery of project services in the design of agriculture-nutrition-health projects. They also imply that failure to disaggregate participation into various categories during analyses can mask the effect of the project.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 See Lemeshow and Robinson (Citation1985) for a discussion on the use of this technique in surveys.
2 We thank anonymous reviewer for recommending this additional insight.
3 Note that wealth here is relative. None of the households in this community would be considered rich. Some, however, were better off than others.
References
- Beal, T., E. Massiot, J. E. Arsenault, M. R. Smith, and R. J. Hijmans. 2017. “Global Trends in Dietary Micronutrient Supplies and Estimated Prevalence of Inadequate Intakes.” PLoS One 12 (4): e0175554. doi:10.1371/journal.pone.0175554.
- Benn, C. S., P. Aaby, R. J. Arts, K. J. Jensen, M. G. Netea and A. B. Fisker. 2015. “An Enigma: why Vitamin A Supplementation Does not Always Reduce Mortality Even Though Vitamin A Deficiency is Associated with Increased Mortality.” International Journal of Epidemiology 44 (3).
- Bhutta, Z. A., and S. L. Baker. 2015. “Premature Abandonment of Global Vitamin A Supplementation Programmes is not Prudent!” International Journal of Epidemiology 44 (1): 297–299.
- Bromage, S., D. Ganmaa, J. W. Rich-Edwards, B. Rosner, J. Bater, and W. W. Fawzi. 2018. “Projected Effectiveness of Mandatory Industrial Fortification of Wheat Flour, Milk, and Edible oil with Multiple Micronutrients among Mongolian Adults.” PloS One 13 (8): e0201230.
- Brun, T., J. Reynaud, and S. Chevassus-Agnes. 1989. "Food and Nutritional Impact of One Home Garden Project in Senegal." Ecology of Food and Nutrition 23 (2): 91–108.
- Cardoso, R. V., Â Fernandes, A. M. Gonzaléz-Paramás, L. Barros, and I. C. Ferreira. 2019. “Flour Fortification for Nutritional and Health Improvement: A Review.” Food Research International 125: 108576.
- Christinck, A., and E. Weltzien. 2013. “Plant Breeding for Nutrition-Sensitive Agriculture: an Appraisal of Developments in Plant Breeding.” Food Security 5 (5): 693–707.
- Cole, D. C., C. Levin, C. Loechl, G. Thiele, F. Grant, A. W. Girard, K. Sindi, and J. Low. 2016. “Planning an Integrated Agriculture and Health Program and Designing its Evaluation: Experience From Western Kenya.” Evaluation and Program Planning 56: 11–22.
- Dhandevi, P. E. M., and R. Jeewon. 2015. “Fruit and Vegetable Intake: Benefits and Progress of Nutrition Education Interventions-Narrative Review Article.” Iranian Journal of Public Health 44 (10): 1309.
- FAO and FHI 360. 2016. Minimum Dietary Diversity for Women: A Guide for Measurement. Rome: FAO.
- FAO, IFAD, UNICEF, WFP and WHO. 2017. The State of Food Security and Nutrition in the World 2017. Building Resilience for Peace and Food Security. Rome: FAO. http://www.fao.org/3/a-I7695e.pdf.
- Hotz, C., C. Loechl, A. de Brauw, P. Eozenou, D. Gilligan, M. Moursi, B. Munhaua, P. van Jaarsveld, A. Carriquiry, and J. V. Meenakshi. 2012. "A Large-Scale Intervention to Introduce Orange Sweet Potato in Rural Mozambique Increases Vitamin A Intakes among Children and Women." British Journal of Nutrition 108 (1): 163–176.
- Jones, K. M., and A. de Brauw. 2015. “Using Agriculture to Improve Child Health: Promoting Orange Sweet Potatoes Reduces Diarrhea.” World Development 74: 15–24.
- Kass, E., and K. Kolasa. 1978. "Supplemental Commodity Food Use by Participants in the Project Focus: Hope in Detroit, Michigan." Ecology of Food and Nutrition 7 (1): 57–61.
- Lapar, L. A., N. N. Toan, N. N. Que, M. Mohammed, C. Tisdell, and S. Staal. 2009. “Market Outlet Choices in the Context of Changing Demand for Meat: Implications for Smallholder Inclusion in the Pork Supply Chain in Vietnam.” Selected paper presented at the IAAE, Beijing, China, August 16–22.
- Laurie, S., M. Faber, P. Adebola, and A. Belete. 2015. “Biofortification of Sweet Potato for Food and Nutrition Security in South Africa.” Food Research International 76: 962–970.
- Lemeshow, S., and D. Robinson. 1985. "Surveys to Measure Programme Coverage and Impact: A Review of the Methodology Used by the Expanded Programme on Immunization." World Health Stat Q 38 (1): 65–75.
- Low, J. W., R. O. Mwanga, M. Andrade, E. Carey, and A. M. Ball. 2017. “Tackling Vitamin A Deficiency with Biofortified Sweetpotato in sub-Saharan Africa.” Global Food Security 14: 23–30. https://doi.org/10.1016/j.gfs.2017.01.004.
- Mariyono, J. 2018. “Empowering Rural Livelihoods Through Farmers’ Field School on Vegetable Production in Aceh Province-Indonesia.” Journal of Rural Development 37 (1): 129–145.
- Mariyono, J. 2019. “Stepping up to Market Participation of Smallholder Agriculture in Rural Areas of Indonesia.” Agricultural Finance Review 79 (2): 255–270.
- Mason, J., T. Greiner, R. Shrimpton, D. Sanders, and J. Yukich. 2015. “Vitamin A Policies Need Rethinking.” International Journal of Epidemiology 44 (1): 283–292.
- Mayo-Wilson, E., A. Imdad, K. Herzer, M. Y. Yakoob, and Z. A. Bhutta. 2011. “Vitamin A Supplements for Preventing Mortality, Illness, and Blindness in Children Aged Under 5: Systematic Review and Meta-Analysis.” The British Medical Journal 343: 1–19. https://doi.org/10.1136/bmj.d5094.
- Mohsin, M., M. M. Anwar, F. Jamal, F. Ajmal, and J. Breuste. 2017. “Assessing the Role and Effectiveness of Kitchen Gardening Toward Food Security in Punjab, Pakistan: a Case of District Bahawalpur.” International Journal of Urban Sustainable Development 9 (1): 64–78.
- Moore, L. 1989. “Modelling Store Choice: A Segmented Approach Using Stated Preference Analysis.” Transactions of the Institute of British Geographers, New Series 14 (4): 461–477.
- Nestel, P., H. E. Bouis, J. V. Meenakshi, and W. Pfeiffer. 2006. “Biofortification of Staple Food Crops.” The Journal of Nutrition 136 (4): 1064–1067.
- Okello, J. J., C. J. Lagerkvist, S. Hess, M. Ngigi, and N. Karanja. 2012. “Choice of Fresh Vegetable Retail Outlets by Developing-Country Urban Consumers: the Case of Kale Consumers in Nairobi, Kenya.” The European Journal of Development Research 24 (3): 434–449.
- Ondieki-Mwaura, F. N., L. M. Njoroge, J. J. Okello, and J. M. Bahemuka. 2013. “Determinants of Participation in Identified Institutional Arrangements in Kenya’s Export French Bean Sector.” A paper presented at the 4th International Conference of the African association of agricultural Economists, Hammamet, Tunisia.
- Pambo, K. O., D. J. Otieno, and J. J. Okello. 2017. “Analysis of Consumer Preference for Vitamin A-Fortified Sugar in Kenya.” The European Journal of Development Research 29 (4): 745–768.
- Ramakrishnan, U., R. Martorell, M. C. Latham, and R. Abel. 1999. "Dietary Vitamin A Intakes of Preschool-Age Children in South India." The Journal of Nutrition 129 (11): 2021–2027.
- Rutstein, S. O., and K. Johnson. 2004. The DHS Wealth Index. DHS Comparative Reports no. 6. Calverton: ORC Macro.
- Schmitz, J., K. P. West Jr., S. K. Khatry, L. Wu, S. C. Le Clerq, S. L. Karna, and J. Pillion. 2012. “Vitamin A Supplementation in Preschool Children and Risk of Hearing Loss as Adolescents and Young Adults in Rural Nepal: Randomised Trial Cohort Follow-up Study.” British Medical Journal 344: d7962.
- Shikuku, K. M., J. J. Okello, S. Wambugu, K. Sindi, J. W. Low, and M. McEwan. 2019. “Nutrition and Food Security Impacts of Quality Seeds of Biofortified Orange-Fleshed Sweetpotato: Quasi-Experimental Evidence From Tanzania.” World Development 124: 104646.
- Sloan, N. L., D. Rosen, T. de la Paz, M. Arita, C. Temalilwa, and N. W. Solomons. 1997. "Identifying Areas with Vitamin A Deficiency: The Validity of a Semiquantitative Food Frequency Method." American Journal of Public Health 87 (2): 186–191.
- Smitasiri, S., K. Sangobwarchar, P. Kongpunya, C. Subsuwan, O. Banjong, C. Chitchumroonechokchai, W. Rusami-Sopaporn, S. Veeravong, and S. Dhanamitta. 1999. "Sustaining Behavioural Change to Enhance Micronutrient Status through Community-and Women-Based Interventions in North-East Thailand: Vitamin A." Food and Nutrition Bulletin 20 (2): 243–251.
- Swindale, A., and P. Bilinsky. 2006. “Development of a Universally Applicable Household Food Insecurity Measurement Tool: Process, Current Status, and Outstanding Issues.” The Journal of Nutrition 136 (5): 1449S–1452S.
- United Nations Children’s Fund (UNICEF), WHO, World Bank Group. 2017. Levels and Trends in Child Malnutrition: Joint Child Malnutrition Estimates. Key findings of the 2017 edition.
- Villamor, E., and W. W. Fawzi. 2005. “Effects of Vitamin A Supplementation on Immune Responses and Correlation with Clinical Outcomes.” Clinical Microbiology Reviews 18 (3): 446–464.
- Wijaya, A. F., A. Kuntariningsih, S. Sarwono, and A. Suryono. 2010. “Malnutrition Mitigation and Community Empowerment Through the Sustainable Food Reserve Programme in Indonesia.” Development in Practices (in press). https://doi.org/10.1080/09614524.2020.1782845.
- World Health Organization (WHO). 2009. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005. WHO Global Database on Vitamin A Deficiency. Geneva: World Health Organization.