
Abstract
Purpose
Congenital visual impairment and additional disabilities (VIAD) may hamper the development of a child’s communication skills and the quality of overall emotional availability between a child and his/her parents. This study investigated the effects of bodily-tactile intervention on a Finnish 26-year-old mother’s use of the bodily-tactile modality, the gestural and vocal expressions of her one-year-old child with VIAD, and emotional availability between the dyad.
Materials and methods
Mixed methods were used in the video analysis. The child’s and his mother’s bodily-tactile and gestural expressions were analyzed using a coding procedure. Applied conversation analysis was used to further analyse the child’s emerging gestural expressions in their sequential interactive context. Emotional availability scales were used to analyze the emotional quality of the interaction.
Results
The results showed that the mother increased her use of the bodily-tactile modality during the intervention, especially in play and tactile signing. The child imitated new signs and developed new gestural expressions based on his bodily-tactile experiences during the intervention sessions. His vocalizations did not change. Emotional availability remained stable.
Conclusions
The case study approach allowed the in-depth investigation of the components contributing to the emergence of gestural expressions in children with VIAD.
Bodily-tactile modality may compensate for the absence of a child’s vision in child–parent interactions.
Bodily-tactile early intervention may be effective in guiding caregivers to use bodily-tactile modality in interacting with their child with VIAD.
Caregivers’ use of bodily-tactile modality in interactions may contribute to the development of gestural expressions in a child with VIAD.
The use of bodily-tactile modality in interactions may improve the emotional connection between children with VIAD and their caregivers.
Implications for rehabilitation
Introduction
Visual impairment (VI) hampers early interaction between children and their parents. Additional disabilities (AD) further complicate the situation. It can be difficult for children to access their parents’ emotional responses, which are accompanied by facial and body gestures [Citation1,Citation2]. Similarly, children can express their attention and intentional expressions through subtle body movements or hand gestures, which the parents may not detect or respond to [Citation3,Citation4]. Parents may also not be aware of their children’s need for tactile experiences to develop communicative abilities [Citation5,Citation6]. As a result, children with visual impairment and additional disabilities (VIAD) may experience fewer opportunities to use their potential in communication. Moreover, the quality of overall emotional availability (EA), which means a good emotional connection between children and their parents, can become compromised [Citation7].
Most children (65%) who have VI also have complex health conditions and AD, such as cognitive, motor, or hearing impairment [Citation8]. AD can be caused by rare genetic syndromes, such as L1 syndrome, which primarily affects males and is estimated to affect 1/30,000 (X-linked hydrocephalus with stenosis of the aqueduct of Sylvius (HSAS), [Citation9]). L1 syndrome is associated with hydrocephalus, adducted thumbs, spasticity of the legs, intellectual disability [Citation9], and delayed language development with first words emerging at four years [Citation10], and no spontaneous speech shown by 5- and 8-year-old children [Citation11].
The literature on the communication development of children with VIAD is scarce, and meta-analyses are lacking. A systematic overview is available only on the communication and language profiles of the subgroup of children with congenital deafblindness (CDB), which shows heterogeneity in the group [Citation12]. The difficulty in developing verbal skills has been reported in the literature among children with VIAD [Citation13–15]. The findings suggest that most preschool and school-aged children with VIAD express themselves through preverbal communication behaviors, including vocalizations, body movements, and gestures [Citation13,Citation14]. Learning about their children’s diagnosis often comes as a shock to parents. Children with VIAD typically receive intensive pediatric care during their first months of life. Appointments with speech pathologists are often related to children’s feeding problems. Families receive guidance on interaction during appointments, but there may be no existing systematic pediatric pathways for more intensive communication interventions.
In the absence of vision, touch can be used in communication in a compensatory sense. Studies on cross-sensory perception have shown that infants can connect information from different sensory modalities to the same phenomenon [Citation16,Citation17]. Cross-sensory perception makes it possible for persons with dual sensory loss to receive speech and visual sign language in the tactile modality [Citation18,Citation19]. In the bodily-tactile modality, body postures, body movements, manual gestures, and touch patterns can have various communicative meanings [Citation1,Citation6]. Some bodily-tactile actions can compensate for the functions of vision. For example, eye contact can be expressed as tactile contact [Citation20]. The bodily-tactile modality can also be used for functions such as imitation [Citation21] or anticipating activities related to a child’s body [Citation22]. However, without professional support, parents may not be aware that the bodily-tactile modality can enhance their interaction with their child with VIAD [Citation3].
EA was determined as an outcome variable of this study due to the risk of developing compromised EA between children with VIAD and their mothers. EA is a relational construct; thus, the caregiver cannot be evaluated as highly sensitive without the child’s emotional responsiveness [Citation7]. There is evidence that typical parent–child dyads with higher EA show greater attachment security, emotion regulation, empathy, and social and language development in children [Citation23]. In the assessment, EA is operationalized as four dimensions evaluated in the adult: sensitivity, structuring, nonintrusiveness, and nonhostility. The two dimensions evaluated in the child are responsiveness and involvement [Citation7]. To our knowledge, only two studies have examined EA in mothers and their typically developing children with VI [Citation24,Citation25]. The results indicated that the mothers had some challenges in their sensitivity and abilities to structure play with their children. The children’s EA scores showed considerable individual variability.
This study aims to test an intervention suitable for children with VIAD that enables parent–child dyads to have more accessible social interactions. Increased accessibility can emerge both in children’s ability to access their parents’ bodily-tactile expressions and the parents’ ability to access their children’s atypical gestures [Citation26]. Moreover, when children with VIAD create embodied gestures, parents have more to respond to, which, in turn, enhances the transactional nature of the interaction in the dyad. The transactional model views children’s developmental outcomes depending on the individual child and his/her experiences in interaction [Citation27,Citation28]. Thus, parents’ sensitive reactions to their children’s signals and their ability to provide them with bodily-tactile interactional experiences that stimulate the children to create gestures may have positive transactional effects not only on the interaction in the moment but also over time. Furthermore, the strengthened reciprocal access of parents and their children to each other’s communicative expressions is also likely to contribute to their emotional well-being.
VI does not hinder harmonious interaction between parents and their children if the bodily-tactile modality is used as a compensatory strategy [e.g., Citation29–33]. Although the studies differed in their perspectives, they all found the bodily-tactile modality as an alternative modality for shared meaning construction in interaction (e.g., tactile contact in the absence of eye contact). Accordingly, children with VI have been described as enjoying bodily-tactile interaction games (e.g., pat-a-cake), which offer more opportunities for reciprocity through body and hand movements [Citation4,Citation34]. Moreover, bodily-tactile interaction games create the basis for more complex forms of bodily-tactile communication to develop. For example, children with VIAD may present referential mimetic gestures, which are embodied imitations of some of the interlocutor’s actions in a particular interaction episode, as perceived by the child [Citation5,Citation35]. Moreover, as not all children are able to develop skills in oral language, they may benefit from tactile signing as a form of augmentative or alternative communication [Citation36].
To date, despite the clinical practices and existing intervention guidelines related to the alternative use of the bodily-tactile modality in interactions with children with VIAD [Citation26,Citation36–38], there has been little scientific interest in studying the bodily-tactile forms of communication or the effects of early interventions on children under two years of age with VIAD. The recent findings on the bodily-tactile forms of communication are mainly from studies that included children with CDB and their communication partners [Citation5,Citation29,Citation33] but not normally hearing children with VIAD. Moreover, Ely et al. [Citation39] found that providers of early intervention services for 0–3-year-old children with VI and their families felt inadequately educated for their work, which indicates the need for further research and development of clinical practices to ensure sufficient systematicity and specificity in early intervention. To our knowledge, only five intervention studies have addressed interaction and included participants aged 0–2 years with VIAD [Citation22,Citation34,Citation40–42]. These intervention studies are listed in .
Table 1. Summary of the studies exploring the effects of interventions for 0–2-year-olds with VIAD.
Existing intervention studies differ in their emphasis. While Rogow [Citation34] and Metell [Citation41] used music and nursery rhymes as a means to enhance the elements of early interaction and children’s participation, Chen et al. [Citation22] used promoting learning through active interaction curriculum to foster parent–child interactions in the families’ daily routines. Platje et al. [Citation42] adapted a video-feedback intervention for parents of children with VIAD to foster parental sensitivity. Dyzel et al. [Citation40] tested the effects of an interactive technology-based playmat on caregivers’ sensitive and responsive behaviors. However, none of the interventions used bodily-tactile modality as the main element.
This study aimed to bridge the gap between intervention guidelines, clinical practices, and research-based knowledge by implementing a bodily-tactile intervention for a mother and her child with VIAD. By empowering the mother to use the bodily-tactile modality in interaction the aim was to prevent asymmetries in participation and to support the transactional nature of a dyadic interaction [Citation27,Citation28,Citation43,Citation44]. Four research questions emerged: First, how does the mother use the bodily-tactile modality in the interaction before, during, and after the intervention? Second, what are the characteristics of the child’s gestural and vocal expressions before, during, and after the intervention? Third, does the child develop new gestures during the intervention, and if so, how do the gestures that emerge relate sequentially to his bodily-tactile experiences in the interaction? Lastly, what is the quality of the emotional relationship between the mother and her child before, during, and after the intervention?
Methods
Participants
The participants were a mother and her son (pseudonym Robin) recruited as a convenience sample by a staff member of the pediatric neurology department at a university hospital in Southern Finland. The family was recruited because Robin was aged <24 months, had severe VI, and was at a preverbal stage of language development (maximum 10 words or signs used). After reading a study information letter, the mother contacted the first author to express interest and provide written consent prior to participation. The study was approved by the ethics committee of the Helsinki and Uusimaa Hospital District. The family received a 20 euro toy gift card for participation.
Information related to Robin’s development and functioning of the senses was gathered from medical records and a parental interview. Robin was one year and five months old at the outset of the study. He had an L1CAM gene mutation causing L1 syndrome, with agenesis of the corpus callosum, obstructive hydrocephalus (with a shunt), adducted thumbs, epilepsy, and a mixed specific developmental disorder. Aside from L1 syndrome, Robin had a congenital VI that caused a 50% degree of visual disability. Moreover, he had strabismus and nystagmus. Robin was able to detect a toy when it was brought near him, but he could not see far or pictures in books. Robin used eyeglasses for half of the day. His hearing was normal. Robin was hypotonic and could not sit without support. During the time of the study, Robin’s family had five counselling sessions with a speech pathologist because of Robin’s eating difficulties. At the outset of the study, Robin had not had any support for communication. Robin’s 26-year-old mother is a healthcare professional.
According to Robin’s mother, Robin liked to sit on his parents’ laps and was interested in exploring his parents’ faces using his hands. He expressed himself through vocalizing and body movements. His communicative initiatives were infrequent. He would sometimes bring his hands together at the beginning of the popular Finnish nursery rhyme “Hämä-hämä-häkki” (Itsy Bitsy Spider) and imitate his mother vocally if she used a sound belonging to his sound repertoire in initiating the dialogue. Robin seemed to understand his own name and speech connected to everyday routines. His mother found it easy to read Robin’s emotions. However, she wished Robin was able to express his thoughts and desires better.
Design and procedure
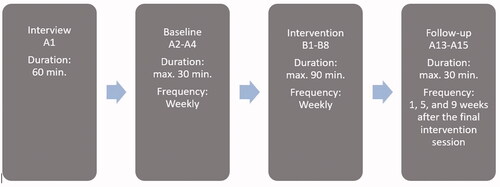
The therapist met the family 15 times at home. The sessions were video recorded using two video cameras, and all recordings were made at the same time in the morning when Robin was well rested. During the recordings, Robin wore his eyeglasses and was most often positioned on his mother’s lap, sometimes in the supine position. In the third baseline session, he sat in a supportive seat opposite his mother. An ABA design was used to study the differences between the conditions [Citation45] (). “A” refers to a session without intervention and “B” to a session with intervention. The mother was interviewed during the first meeting before the baseline recordings. The therapist who carried out the intervention had an MA in speech-language pathology and an MSc in educational sciences, with a specialization in communication and CDB. The intervention was designed for this study based on the expertise of the first author.
Figure 1. Progress of data collection.
Note: The recordings were made weekly during a weekday that was convenient for the family.
Baseline
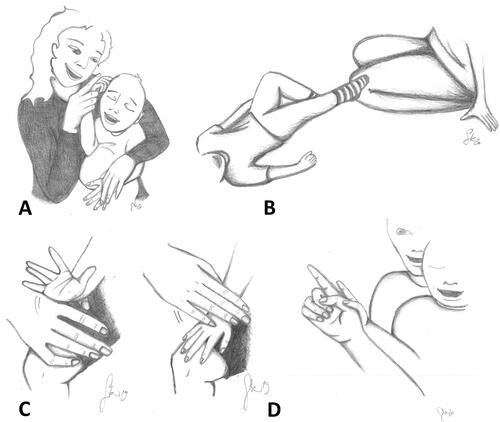
The recordings A2–A4 were made weekly and lasted about 30 min each. During the recordings, the mother was asked to play with Robin, as she normally would. Their play with and without toys was recorded separately. The mother was not told about the content of the intervention until the end of the last baseline recording to keep the interaction as natural as possible. The information from the baseline recordings was used to plan the content of the intervention. For example, Robin had learnt three signs from “Itsy Bitsy Spider,” which the mother sang with coactive signing [Citation36] (). In coactive signing, the mother used the physical guidance of Robin’s hands to facilitate the production of standard manual signs. However, Robin’s mother was unaware of his independent use of these signs.
Figure 2. Illustrative Examples of Bodily-Tactile Communication: Coactive Signing, Tactile Contact, Imitation in the Bodily-Tactile Modality, and Tactile Pointing Gesture. Drawings by Saara Koivula.
Bodily-tactile intervention
After the last baseline recording, the mother was informed about Robin’s way of making tactile contact with his leg, which she had not been aware of (). The aim was to help the mother notice Robin’s communicative abilities that otherwise might have gone unnoticed. Moreover, Robin’s mother was given information about using the bodily-tactile modality in imitation () and anticipating activities.
The intervention sessions were conducted weekly at home. The sessions lasted a maximum of 90 min, which included preparation time (10 min maximum), discussion and video feedback with the mother (15–30 min), triadic play session (10–30 min), and free play recordings (20 min maximum). The intervention aimed to empower the mother by co-operating with her and sharing ideas on how to support Robin’s communication development and modify interactions in a way that would enable Robin to be an active participant in them. The therapist modeled the use of the bodily-tactile modality in interactions by building on and expanding the types of songs and games that the mother was already singing and playing with Robin [see Citation34,Citation41]. Thus, the emphasis was on expanding their shareable bodily-tactile experiences. Most of the new nursery rhymes were played in the body-with-body alignment [Citation1] and some in the face-to-face position. Moreover, the therapist aimed to help the mother detect and respond to Robin’s gestures. The content of the intervention was based on the literature on the transactional model of development [Citation27,Citation28, see also Citation44], tactile strategies [e.g., Citation36,Citation38], interventions for blind children with or without AD [e.g., Citation3,Citation34], intervention guidelines for deafblind children [Citation26], and the mentalization-based, short-term parent–child intervention model “Nurture and Play” [Citation46].
The structure of each intervention session consisted of the following elements: (a) information sharing, discussion, and video feedback; (b) triadic play session; and (c) free play. During the information sharing, discussion, and video feedback section, the mother was shown video clips of her interaction with Robin and some other videos related to communication with children with VIAD. The video analysis aimed to help the mother detect Robin’s gestures. Moreover, the therapist used modeling to demonstrate the use of the bodily-tactile modality in interactions. The mother received a folder containing brief texts on the themes of the sessions and pictures of 23 signs. The purpose of the folder was to help her remember the information shared during the meetings and to facilitate sign learning. At the end of the intervention, the mother was given information about the literature and websites on supporting communication with children with VIAD.
In the triadic play session, different bodily-tactile forms of communication were applied in songs and games. During sessions B1 and B2, the mother was introduced to tactile imitation as a strategy to create imitative dialogues. She was also shown how touch could be used to anticipate sensations on Robin’s skin during play and daily routines (e.g., touching his stomach before spreading cream on it). The mother was also guided to use touch to inform Robin that she had noticed his gestures or movements. In the bodily-tactile games, the mother could touch Robin’s hands or legs after he moved them and interpret the movements as intentional contributions to the game, fostering Robin’s role in the interaction. Moreover, hand-under-hand guidance was introduced as a less intrusive strategy for physical assistance than hand-over-hand guidance [Citation36]. During sessions B3 and B4, the focus was on detecting Robin’s subtle signs. During sessions B5 and B6, the mother was introduced to a tactile pointing gesture (). As Robin had some vision, this aimed to give Robin’s mother a way to facilitate her attempts to guide his attention. The mother was also encouraged to take pauses in the interaction so that Robin would have a longer time to take his turn [Citation47]. During sessions B7 and B8, the themes of the previous sessions were rehearsed. Some tactile signs were modeled to Robin and his mother in all the sessions, except the last two. After the triadic play session, free play between Robin and his mother, with and without toys, was recorded. After the recordings, the mother was given some ideas about the use of tactile modality in interactions and play for the following week.
Follow-up
The follow-up sessions were carried out one, five, and nine weeks after the final intervention session. During the follow-up recordings, the mother was asked to play with Robin with and without toys, as she liked. In the follow-up A14 and A15 recordings, Robin had nasogastric intubation due to his eating problems and vomiting.
Data analysis
Free play without toys between Robin and his mother was analyzed from three baseline, three intervention, and three follow-up sessions. The length of free play in the sessions varied from 10–13 min. To obtain a comprehensive view of the characteristics and possible changes in the interactions, the data were analyzed with mixed observational methods. First, Robin’s and the mother’s expressions were analyzed using a systematic coding procedure developed for this study. A new coding procedure was developed because the existing communication protocols did not capture the bodily-tactile characteristics of the data. During the analysis, it was found that an even more detailed approach would be needed to study the sequential connectedness between the mother’s bodily-tactile input and Robin’s emerging new gestural expressions. For this purpose, some of Robin’s expressions were further analyzed in their interaction context using applied conversation analysis (CA) [Citation48]. Second, to obtain an overall perspective of the emotional quality of the interaction, EA Scales were used in the analysis [Citation7].
The analysis using EA Scales was based on the full recordings. To analyze the mother’s use of bodily-tactile modality in interactions and Robin’s expressions, the length of each video clip was edited and rounded off to the nearest full minute (10:00, 11:00, 12:00, or 13:00). This was done to compare the frequencies of the studied phenomenon per minute. ELAN version 6.0 (2020) was used to code the videos. Each expression was coded in its context. For example, when defining the categories for the mother’s use of bodily-tactile modality, Robin’s previous expression was identified to examine the relatedness of the expressions (e.g., imitations). Mutually exclusive categories were used. If there were two simultaneous gestures or movements belonging to different categories (e.g., simultaneous sign and bouncing), both expressions were coded.
Coding procedures for the mother’s use of bodily-tactile modality in interactions and Robin’s expressions
A coding procedure was developed to capture the frequency and duration of different bodily-tactile forms of communication [Citation5,Citation22,Citation36,Citation38]. First, the categories were created by identifying the different forms of bodily-tactile communication appearing in the data. Only bodily-tactile behaviors related to social interaction were coded. For example, the mother’s touches connected to changing Robin’s position were not analyzed. Some of the bodily-tactile forms of communication were related to the themes of intervention, while others were spontaneously developed by the mother. Her spontaneously created bodily-tactile forms of communication were also analyzed but separated from the intervention-based bodily-tactile forms of communication. Two consecutive similar touches or movements were coded as one expression if they appeared within 2 s in the following categories: signs, touches related to anticipating and noticing, touches or movements connected to play, hand-over-hand guidance, and other tactile attention-directing gestures. Without the timeframe, it would have been difficult to decide whether a repetitive gesture or movement should be coded as one expression or two separate expressions. The categories of the coding procedures for the mother’s use of bodily-tactile modality in interactions and Robin’s expressions are presented in .
Table 2. The categories of the coding procedures for the mother’s use of bodily-tactile modality in interactions and Robin’s expressions.
Conversational analysis of the connectedness between Robin’s gestural expressions and his bodily-tactile experiences in play
To obtain more detailed information on the interactive processes in which Robin’s new gestural expressions emerged, the principles of applied CA were used in the analyses [Citation50]. Applied CA is an analytic framework for analyzing interactions in detail in its context [Citation51]. Applied CA was used to study the emergence of new gestural expressions because it looks at turn taking and sequential organization in interactions [Citation51,Citation52]. Thus, through applied CA, it was possible to analyze gestures connected to the previous action that they emerged from. Applied CA has also been used in studying atypical interactions [Citation48] and bodily-tactile expressions [Citation53].
The data showed that many of Robin’s intervention-based new gestural expressions appeared in the context of the nursery rhyme “Magpie Makes Porridge.” Consequently, all episodes of interaction including the rhyme were searched in the data, and six episodes were found. The rhyme is similar to the English nursery rhyme “Round and Round the Garden,” as it contains a simultaneous verbal and bodily-tactile narrative and a climax at the end. The rhyme is described below, with an English translation and a tactile description.
1. Harakka huttua keittää, hännällänsä hämmentää.
Magpie makes porridge, stirring it with her tail.
THE MOTHER MAKES A CIRCULAR MOVEMENT ON THE CHILD’S PALM WITH HER INDEX FINGER.
2. Antaa tuolle pojalle, antaa tuolle pojalle, tuolle pojalle, tuolle pojalle, mutta yksi poika jäi ilman.
She gives (it) to that chick, gives (it) to that chick, that chick, that chick, but one chick is left without.
THE MOTHER TOUCHES THE CHILD’S FINGERS ONE BY ONE, STARTING FROM THE THUMB.
3. Se hyppäsi kivelle,
She jumps on a stone,
THE MOTHER TOUCHES THE CHILD’S WRIST.
4. kannolle
on a tree stump
THE MOTHER TOUCHES THE CHILD’S ELBOW.
5. ja lähti vettä hakemaan, ja lähti vettä hakemaan.
and goes to look for some water and goes to look for some water.
THE MOTHER TICKLES THE CHILD’S ARMPIT.
Subsequently, the interactive sequences within the episodes were transcribed using applied CA to capture the shape and temporality of the sensorial and multimodal embodied conduct [Citation54,Citation55]. The transcriptions were simplified for the readability and purpose of the study. In the transcript, information related to Robin’s and his mother’s expressions is written in sequential order, one below the other. The transcript includes information related to expressions of vocal, gestural, and bodily means. Utterances in Finnish are written in small and bold letters and loosely translated into English. Information related to non-verbal and bodily expressions is written on the lowest line in capital letters. The signs are written in capital letters and in italics. If there is no speech, information connected to bodily expressions is described on its own line. The notation symbols are described in the Appendix. An example of the transcription is given below. 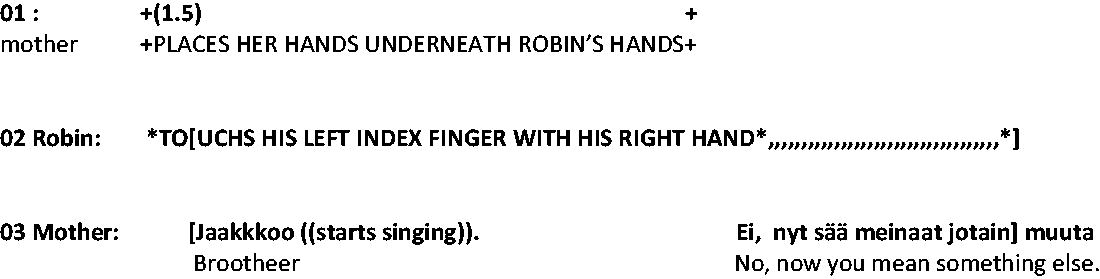
In the analysis, Robin’s gestures were identified from the data and analyzed sequentially in their context with respect to the bodily-tactile experiences given by his mother during the rhyme. Moreover, the timing of Robin’s and his mother’s expressions in relation to each other was examined.
Emotional availability
EA Scales (4th ed.) were used for analyzing the emotional connection and quality of interaction between Robin and his mother [Citation7]. The adult subscales are sensitivity (caregiver’s ability to be warm and emotionally connected with the child), structuring (caregiver’s ability to structure a play in an appropriate way), nonhostility (caregiver’s ability to be free of negativity), and nonintrusiveness (caregiver’s ability to interact with the child without intervening in their autonomy). The child subscales are responsiveness (child’s emotional responsiveness toward the caregiver) and involvement (child’s initiative in the interaction with the caregiver). All subscales can have numeric values from 1 to 7 (1 = non-optimal, 2.5/3 = somewhat (insensitive), 4 = inconsistent, 5.5/6 = moderate, 7 = optimal). The coder and the second coder for the EA reliability test completed reliability training in the use of the EA Scales and coding frame. The coders were informed of the level of sensory functioning and development of the observed child and blinded to the phase of intervention prior to coding. Before the analysis, the coder was shown an example video from the non-analyzed data to familiarize her with Robin’s special features of interaction. The guidelines of the EA Scales for children with disabilities were followed in coding [Citation7,Citation56].
Reliability
All data (100%), including the mother’s bodily-tactile and Robin’s gestural expressions, were re-coded by a second coder who had considerable experience in working with children with multiple disabilities and who was a fluent Finnish Sign Language user. All the data were re-coded because the coding procedure was new and had been developed for this study, and verifying the reliability of the coding procedure was important. The second coder was blinded to the phase of intervention prior to coding. Before coding, she was trained to use the coding procedure and was given information on the sign repertoire of the data. She was also given information about Robin’s sensory functioning and development. The reliability of each coding category was calculated as the number of agreements divided by the number of agreements plus disagreements multiplied by 100.
In terms of the mother’s behavior, interobserver agreement was 93% for the total amount of tactility in interaction, 97% for tactile signs, 88% for touches and movements connected to play, 94% for tactile imitation, 95% for anticipation and noticing, 95% for tactile pointing, 89% for non-intervention-based bodily-tactile forms of communication, and 95% for non-tactile signs, non-tactile conventional gestures, and non-tactile pointing. For Robin’s expressions, the interobserver agreement was 65% for signs, 69% for sign imitations, 70% for reaching and requesting, and 80% for motor imitation. As the interobserver agreement for signs, sign imitations, and reaching and requesting did not reach an acceptable level of reliability, only the expressions found by both coders were included in the results. Among the signs found by both coders, 3% were categorized with different labels (e.g., MAGPIE vs. SPIDER). The quality of Robin’s vocalizations was re-analyzed for 33% of the data. One video from the baseline, intervention, and follow-up recordings was randomly chosen for the reliability test. Interobserver agreement was 100%.
The reliability of the EA coding was ensured by using another second coder. Altogether, 33% of the data was re-coded; one video from baseline, intervention, and follow-up recordings was randomly chosen. The percent agreement was 94% when counting the maximum 0.5-point differences between the coders on each scale.
Results
The mother’s intervention-based bodily-tactile forms of communication
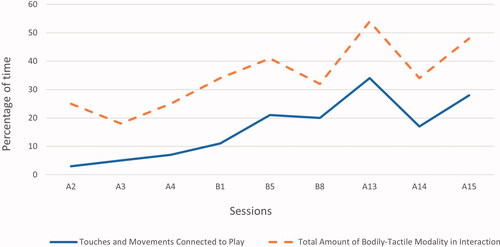
The results on the amount of time the mother used the bodily-tactile modality in interactions are illustrated in . During the intervention, the mother increased her use of the bodily-tactile modality in interactions with Robin. The results remained the same in the follow-up recordings.
Figure 3. The mother’s use of bodily-tactile modality in interactions and touches and movements connected to play as a percentage of time per session.
Note: The total amount of bodily-tactile modality in interactions includes the use of all intervention-based and non-intervention based bodily-tactile forms of communication.
Tactile signs
The frequency and contexts of the mother’s signs are presented in . The overall frequency of tactile signs did not change notably from baseline to intervention. In the baseline recordings, the mother used tactile signs only in “Itsy Bitsy Spider,” which she sang several times with Robin during the sessions. However, in the intervention and follow-up sessions, the mother started using tactile signs to support her spoken messages and in new songs. Thus, the contexts for using tactile signs were expanded. The mother made most of the tactile signs by coactive signing ().
Table 3. Frequencies of the mother’s signs and Robin’s gestural expressions.
The results for the mother’s sign vocabulary are presented in . In the baseline sessions, her tactile sign vocabulary consisted of signs that belonged to the “Itsy Bitsy Spider” nursery rhyme. In the intervention and follow-up sessions, the mother’s sign vocabulary doubled. She began to use tactile signs in new nursery rhymes and in daily routines at home.
Table 4. Robin’s and his mother’s sign vocabulary.
Other intervention-based bodily-tactile forms of communication
Touches and movements connected to play
The results on the amount of time Robin’s mother used touches and movements connected to play are presented in . In the baseline sessions, the mother used movements such as bouncing or swinging, along with singing, but she did not do this systematically. During the intervention and follow-up sessions, the duration of the touches and movements connected to play clearly increased, and the mother started using new nursery rhymes with bodily-tactile patterns (e.g., coactive hand and body movements in songs and games, including air flow and other tactile sensations).
Tactile attention-directing gestures
The mother did not use hand-under-hand guidance in any of the sessions. In the baseline sessions, she used only non-tactile pointing gestures. Due to his VI, Robin did not direct his attention toward the object pointed at on any of the pointing occasions (n = 3). Tactile pointing occurred in sessions B5 (n = 13) and B8 (n = 2). It appeared to be a helpful strategy, as about half of the occasions led Robin to direct his attention to the object (e.g., a lamp) tactically pointed at.
Touches related to anticipating and noticing
The mother’s touches related to anticipating and noticing were not detected in the baseline sessions, but they occurred in sessions B1 (n = 18), A13 (n = 13), A14 (n = 15), and A15 (n = 5). Robin’s mother used tactile anticipation cues connected to a specific game and before lifting him up. She used touch related to noticing in moments when she wanted to express to Robin that she had noticed his movement or non-readable gesture.
Bodily-tactile imitation
Robin’s mother tactilely imitated Robin’s finger movements in one of the baseline sessions (A3). Bodily-tactile imitation games became more frequent during the intervention, as they appeared in all the recordings, but this was not the case in the follow-up recordings.
The mother’s non-intervention-based bodily-tactile forms of communication
The mother used sporadic, non-intervention-based bodily-tactile forms of communication. Hand-over-hand guidance was used in all sessions except one (B1).
Robin’s expressions
Tactile contact
Characteristically, Robin was not able to make any eye contact with his mother during the interaction. At times, when he was either seated in a supportive chair facing his mother or lying on the floor, he made tactile contact with his mother using his foot (). When he sat in his mother’s lap, he was in tactile contact with his mother through body-with-body alignment.
Gestural and vocal expressions
The results of Robin’s gestural expressions are presented in . His sign vocabulary is listed in . In the baseline recordings, Robin used three signs, which were all connected to “Itsy Bitsy Spider.” Robin’s mother was unaware of his signs. During the intervention, Robin’s mother began detecting more of Robin’s signs. Moreover, during the intervention, Robin developed a new mimetic gesture referring to the rhyme “Magpie Makes Porridge,” which later became a mutually recognized sign for “MAGPIE” for the rhyme. He used “MAGPIE” several times during intervention sessions B5 and B8 and in all follow-up recordings. He also started using the sign DOG imitatively and spontaneously. Moreover, after the A13 recordings, the mother said that Robin had started imitating the sign “EAT,” sometimes also making it spontaneously. Robin’s vocalization was non-canonical throughout the sessions and consisted of an /s/-sound, phonation, vowel sounds, lip vibration sounds, smacking sounds, sighs, and laughter.
Contextual emergence of new gestures
The results of Robin’s gestural expressions in “Magpie Makes Porridge” are presented in . The nursery rhyme “Magpie Makes Porridge” was introduced to Robin and his mother in the fourth intervention session. To demonstrate the mother’s use of the bodily-tactile modality and Robin’s gestural contribution to the rhyme, we present the following two extracts from the fifth intervention session. Still pictures are included in the transcriptions. The first extract shows how the mother uses the bodily-tactile modality in the rhyme (Extract 1(Figures 1 and 3)). Robin uses a mimetic gesture to anticipate his mother’s subsequent touches on his fingers (Extract 1(Figure 2)).
Extract 1. Robin’s mimetic anticipatory gesture
Robin’s gestures and movements are denoted by an asterisk (*).
The mother’s gestures and movements are denoted by a plus symbol (+).
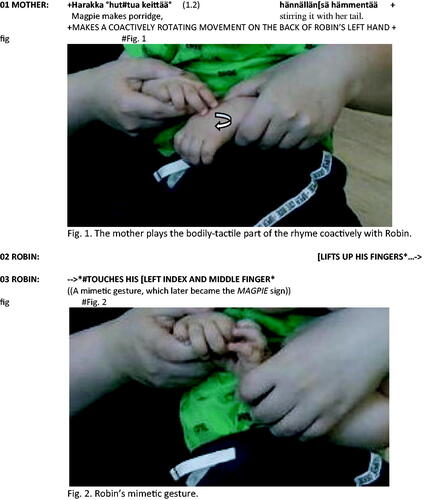

Robin’s mother makes the rotating movements of the rhyme coactively with Robin’s right hand, while Robin’s left hand is used as the scene in the story (Extract 1(Figure 1)). During the rhyme, Robin is very attentive in perceiving the rhyme in both auditive and bodily-tactile ways. His body language signals attentiveness through expectant stillness. The form and timing of his gesture indicate his detailed knowledge of the rhyme. Robin’s gesture begins while his mother is still speaking (lines 1–2), and his mimetic gesture anticipates his mother’s subsequent touches on his fingers (Extract 1(Figure 2)). The mother notices Robin’s gesture and comments on it (line 4). The mother’s verbal noticing explicitly confirms Robin’s sense of tactile gesture, thus reinforcing its shared meaning.
Extract 2 illustrates the part of the rhyme in which the bodily-tactile narrative storyline continues from the fingers to the wrist. Robin anticipates his mother’s subsequent touch through another type of anticipatory gesture that reflects his embodied memory of how his mother’s touch feels on his arm.
Extract 2. Robin’s gesture anticipating his mother’s next point of touch
Robin’s gestures and movements are denoted by an asterisk (*). The mother’s gestures and movements are denoted by a plus symbol (+).
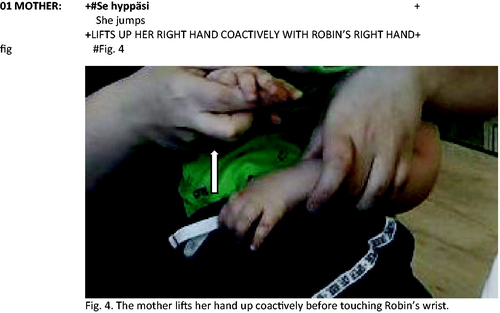
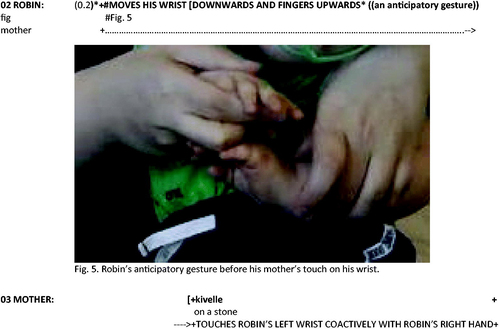
The mother lifts her hand up coactively with Robin’s right hand (Extract 2(Figure 4)). As Robin’s hand follows his mother’s movement coactively, he receives detailed bodily-tactile information on the timing of the movements. Subsequently, Robin makes an anticipatory gesture by moving his fingers upward and wrist downward as his mother is about to touch his wrist (Extract 2(Figure 5)).
The results of the multimodal and sensorial analysis showed that sequentiality is also a fundamental principle of social interaction in the bodily-tactile nursery rhymes in which the adult is typically the primary speaker and the child is the recipient [cf. Citation54,Citation55]. Although the rhymes did not include adjacency pairs (e.g., a question and an answer), adjacent actions emerged in that Robin anticipated his mother’s subsequent action with his gestures. He learned the bodily-tactile structure of the rhyme, which enabled him to participate in the storytelling through gestures. Robin initiated his gestures and vocalizations during short pauses and so that they overlapped with his mother’s expressions. The mother’s verbal and embodied actions emerged in synchrony with each other but followed different temporalities [see Citation55]. Her verbal and embodied actions overlapped with half of Robin’s gestural expressions but only one of his vocalizations.
Robin made two types of gestures. The first type was a mimetic gesture, which was an imitation of how he felt his mother’s touches on his fingers, as illustrated in Extract 1(Figure 2) [cf. Citation35]. Robin made the gesture by touching his index or middle finger or thumb. As Robin often made this gesture before his mother’s touch on his fingers, it was also an anticipatory gesture. Moreover, he used the gesture in other contexts, in which it seemed like a request or sometimes an answer to his mother. The mimetic gesture can be understood as a referential gesture representing the rhyme outside of its original context [Citation57].
The second type of Robin’s gestures (Extract 2(Figure 5)) always appeared in a specific part of the rhyme, anticipating the subsequent touch on his arm. Besides being an anticipatory gesture, it could be interpreted as an early pointing gesture, which Robin used to direct his own attention to the event [see Citation57,Citation58]. Moreover, Robin used a similar gesture by moving his fingers upward in specific contexts to anticipate his mother’s subsequent touches. For example, he moved his fingers upward after his mother’s suggestion to play “Maggie Makes Porridge.” He also lifted his fingers up at the beginning of the rhyme before his mother touched his fingers. In sum, all of Robin’s emerging gestures reflected his bodily-tactile experiences of the rhyme. Similarly, Ask Larsen [Citation53] found that the gestural expressions of a child with CDB referred to the tactile nursery rhyme “Round and Round the Garden.”
Emotional availability between Robin and his mother
The results of Robin’s and his mother’s EA are presented in . During the baseline sessions, the mother scored high in sensitivity, structuring, and nonhostility, and the scores remained high throughout the intervention and follow-up sessions. Her scores in non-intrusiveness corresponded with benign intrusiveness in two baseline recordings. During the intervention, her scores corresponded with general nonintrusiveness but returned to the level of benign intrusiveness in the last two follow-up recordings. Similarly, there was a slight improvement in Robin’s scores in responsiveness from baseline to intervention, but the scores returned to the baseline level in the last two follow-up recordings. Robin’s involvement remained similar throughout the sessions, except the last two follow-up recordings, when his scores decreased below the baseline.
Table 5. Emotional availability between Robin and his mother.
Feedback from the mother
After the intervention, Robin’s mother was asked to give feedback on the intervention through a feedback form and a video-recorded interview. She rated the intervention as very useful (5) on a scale ranging from not useful at all (1) to very useful (5) and found the content of the intervention to be excellent for them. The mother explained that all the introduced forms of bodily-tactile communication were new to them. She especially valued the new bodily-tactile games because they added to their repertoire and made playing easier. Moreover, the mother reported that she and Robin understood each other more. She also felt that she was more competent in detecting Robin’s gestures and responding to him. Lastly, she appreciated the fact that she was free to apply the shared ideas without demand. In her opinion, the best time for early intervention would be when a child with VIAD is around 6–18 months old.
Discussion
The results of this study showed that the mother’s use of the bodily-tactile modality in interactions increased from baseline to intervention in its entirety and remained high during the follow-up sessions. Similarly, Lindström [Citation33] found in her follow-up study that care workers were able to accommodate visual information in the bodily-tactile modality in interactions with a young man with CDB. By increasing the use of the bodily-tactile modality in interactions, Robin’s mother was able to increase Robin’s ability to perceive her expressions and his chances of participating in the interaction. The most notable changes in the mother’s use of the bodily-tactile modality in interactions were found in tactile signing and using touches and movements connected to play. The change in the mother’s tactile signing had already had an impact on Robin’s expressions after a short time, as he started imitating two signs (DOG and EAT) during the intervention and follow-up sessions. Learning new signs is likely to take much more time than the timeframe of this study; thus, the results of Robin’s manual sign acquisition may only be evident over time.
Moreover, the results showed that the bodily-tactile structure of the rhyme “Magpie Makes Porridge” helped Robin to perceive segments of action, anticipate them, and take an initiative role in the rhyme by using his self-created gestural expressions. Similar findings have been reported by Ask Larsen [Citation53] and Rogow [Citation34]. The results also confirmed earlier findings that the gestures of persons with VI are often based on bodily-tactile explorations and experiences [Citation5,Citation59]. Moreover, the results are in accordance with earlier findings underlining the important role of routinized nursery rhymes in contributing to children’s language development [Citation34,Citation60,Citation61].
In this study, Robin reached a level of communicative development in which the symbolic use of gestures emerged in signing but not vocally. His signs were based on his experiences with tactile signing and bodily-tactile nursery rhymes. Thus, it is crucial to understand the importance of both a child’s spontaneously emerging expressions and a communication partner’s contribution in providing tactile linguistic input when considering the basis for developing communication skills in children with VIAD [Citation33]. If the bodily-tactile modality is not used systematically in interacting with children, then they may not be able to use their full competence in communication. Moreover, parents’ use of the bodily-tactile modality in interactions may work as a strategy to prevent asymmetries in communication and the emotional and behavioral problems often found in children with VIAD [Citation62].
As the intervention aimed to support Robin’s participation in interaction and the development of his communication skills by empowering his mother in communication, it was necessary to determine whether the intervention had any transactional effects. Sameroff and MacKenzie [Citation28] suggested that transactions are documented when the activity of one person changes the usual activity of another person either qualitatively or quantitatively. Based on this, the bodily-tactile intervention provides evidence for positive transactional processes, as the new bodily-tactile play and tactile signs used by the mother increased Robin’s sign and gestural repertoire. Similarly, Rogow [Citation34] found that new gestural and bodily behaviors emerged during an intervention that used nursery rhymes to foster communication with children with VIAD.
The mother’s raw EA scores showed little difference from baseline to intervention. This may be due to her high scores at baseline or the inability of the EA Scales to detect micro-level changes in interaction. When a parent already has high EA at baseline, there is no need for change. However, the high parental EA in typical terms may not be sufficient to support communication and language development in children with VIAD because it does not fulfill the developmental needs of the children. Just as the parents of a blind child need to adapt their linguistic input [Citation25], the parents of a child with VIAD may need to adapt their linguistic and bodily-tactile input in their interactions with their child.
Although Robin’s responsiveness scores were slightly better in the intervention and follow-up sessions than in the baseline sessions, the change was not notable. His good responsiveness and involvement could be associated with his mother’s sensitivity and his ability to express himself with signs [see Citation63]. Robin’s involvement was stable and rather good until the last two follow-up sessions, when his involvement decreased. This decrease was most likely due to the nasogastric intubation that he had in the last two follow-up recordings.
Three analytical approaches were used in the analysis to capture the effects of the intervention comprehensively. We acknowledge that qualitative analysis includes reflexivity. The new coding procedure developed for this study was able to capture the changes in the mother’s use of the bodily-tactile modality in interactions and in Robin’s expressions. However, only with applied CA was it possible to capture multimodality in interactions in form and timing and to see how the mother’s bodily-tactile interaction was related to Robin’s emerging gestures. Although the EA Scales were unable to capture the changes in Robin’s or his mother’s expressions, it was an important measure to use, as the emotional aspect is a crucial part of the quality of interaction between parents and their child with VIAD. The results of this study support the use of mixed methods in examining atypical interaction in children with VIAD.
This study is theoretically in accordance with current intervention approaches [Citation26,Citation32,Citation37] but differs from others in emphasis and design. First, the focus was narrowed to nursery rhymes as a context of interaction and empowering the mother to use the bodily-tactile modality in interactions with her child with VIAD. Although Metell [Citation41] and Rogow [Citation34] also used musical interaction and nursery rhymes as a strategy to foster interaction between children with VIAD and their caregivers, they did not systematically guide caregivers to use different forms of bodily-tactile communication with children with VIAD. Second, the findings indicate that the bodily-tactile knowledge from the field of CDB could be applied to a broader population of children with VIAD and their caretakers. Third, this study controlled the quality of emotional relationships in the mother–child dyad, unlike the other intervention studies aiming to foster interaction between caregivers and their 0–2-year-old children with VIAD. EA is suggested to be an important dimension to control in future intervention studies, as challenges in early interaction between parents and their children may lead to emotional unavailability.
Limitations and future directions
The results of this study suggest that Robin’s new gestures and signs are related to the bodily-tactile experiences provided by his mother. Thus, by empowering Robin’s mother with new ideas and abilities to compensate for the lack of visual information in interaction, it was possible to enhance reciprocity in interaction and reveal Robin’s potential in communication. It is pivotal that even a brief intervention was able to enhance the interaction between Robin and his mother. However, as the results of this study are based on one mother–child dyad, they cannot be generalized. Further studies are needed to confirm the positive outcomes of this study. Moreover, a longer follow-up period is needed to monitor the lasting effects of the results. Note that a brief early intervention is only the start and that parents should be offered the possibility of further guidance in tactile communication, if needed. Future studies could explore longer interventions at later stages of tactile communication development. The benefits of bodily-tactile early intervention could also be tested in other populations, such as children with multiple disabilities who have functioning vision and hearing. It is hypothesized that parents’ systematic use of the bodily-tactile forms of communication with their children with multiple disabilities would foster the children’s gestural development and enhance interaction with their parents.
Other areas also require further investigation. First, the process of the analysis and the reliability test exhibited challenges in detecting Robin’s early signs and gestures. Indeed, it may be a challenge to reach acceptable reliability in coding the expressions of children with VIAD due to their low readability. Future studies should focus on determining the best practices for professionals and parents to detect a child’s emerging bodily and gestural expressions. This process is likely to be continuous as the child develops communicative competence [Citation26]. If applied CA is used in video analysis, it may only be successful with detailed ethnographic background information from the parents [see 50]. Developing the best ways to assess the communication skills of a child with VIAD is needed both in research and clinical work [Citation14]. Besides determining the child’s stage in communication development, developing assessment strategies, which reveal the potential for communication instead of deficiencies, is needed. Second, different forms of bodily-tactile communication should be studied in more depth because there is little research-based evidence of their benefits. Third, studies using EA Scales are needed to gain knowledge about EA in children with VIAD and their parents, as the children’s VIAD may compromise EA between their parents. Moreover, there is a need to gain more information on the usability of EA Scales in assessing children with VIAD. Lastly, as this study focused only on the signs Robin produced in the nursery rhyme “Magpie Makes Porridge,” all of Robin’s signs should be studied using multimodal CA to obtain a full picture of their contexts and connectedness to bodily-tactile experiences in interaction.
Finally, the mother’s feedback gives reason to conclude that she was empowered by the intervention. This may be due to her elevated self-efficacy and control over her broadened possibilities in communicating and playing with her son and seeing Robin’s potential in communication [see Citation64]. Ideally, empowerment is the process and the result of early intervention in parents and their children with VIAD [Citation64]. In this process, professionals should adopt an interactive pattern of partnership through which they can equip parents with new skills and ideas to support their child’s communication development [see 65]. Accordingly, professionals may need to evaluate their own work during the intervention, as there is easily a danger of over-reliance on professional input [Citation65,Citation66].
Conclusion
The findings of this study suggest that the mother increased her use of the bodily-tactile modality in interactions during and after the intervention, especially in tactile signing and using touches and movements connected to play. Moreover, the results show that Robin started imitating new signs and developed new gestures related to his bodily-tactile experiences in play. Robin used gestures for symbolic communication, which he was not able to do vocally. The effect of the intervention on EA was minor. In sum, the results of the study indicate the importance of the caregivers’ use of the bodily-tactile modality in interactions in contributing to the development of communication skills and well-being of a child with VIAD.
Acknowledgments
The authors acknowledge Tuire Lähdesmäki and Heljä Salminen for their help in contacting the family; Tuire Lähdesmäki for being the doctor responsible for the study; Jani Pöyhönen, Peter Dahl, and IT Services at the University of Turku for their help in technical issues; Hetti Hakanen for the EA analysis; Saara Koivula for the drawings; and Anu Kajamies for her assistance in the analysis.
Disclosure statement
We have no known conflicts of interest to disclose.
Data availability statement
The data cannot be shared due to ethical restrictions.
Additional information
Funding
References
- Gregersen A. Body with body: interacting with children with congenital deafblindness in the human niche. J Deafblind Studies Commun. 2018;4(1):67–83.
- Lang M, Hintermair M, Sarimski K. Social-emotional competences in very young visually impaired children. Br J Vis Impair. 2017;35(1):29–43.
- Fraiberg S. Intervention in infancy: a program for blind infants. J Am Acad Child Psychiatry. 1971;10(3):381–405.
- Preisler GM. Early patterns of interaction between blind infants and their sighted mothers. Child Care Health Dev. 1991;17(2):65–90.
- Forsgren GAGC, Daelman M, Hart P. Sign construction based on heightened tactile perception by persons with congenital deafblindness. J Deafblind Studies Commun. 2018;4(1):4–23.
- Nicholas J. From active touch to tactile communication - what’s tactile cognition got to do with it? Aalborg: the Danish Resource Centre on Congenital Deafblindness; 2010. Available from: https://socialstyrelsen.dk/udgivelser/from-active-touch-to-tactile-communication
- Biringen Z. Emotional availability (EA) scales. Infancy/early childhood version. 4th ed. Boulder (CO): www.emotionalavailability.com; 2008.
- Hatton DD, Ivy SE, Boyer C. Severe visual impairments in infants and toddlers in the United States. J Vis Impair Blind. 2013;107(5):325–336.
- Stumpel C, Vos YJ. L1 syndrome. In: Adam MP, Ardinger HH, Pagon RA editors. GeneReviews. Seattle (WA): University of Washington; 1993–2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1484/
- Schrander-Stumpel C, Legius E, Fryns JP, et al. MASA syndrome: new clinical features and linkage analysis using DNA probes. J Med Genet. 1990;27(11):688–692.
- Bianchine JW, Lewis Jr RC. The MASA syndrome: a new heritable mental retardation syndrome. Clin Genet. 1974;5(4):298–306.
- Dammeyer J, Ask Larsen F. Communication and language profiles of children with congenital deafblindness. Br J Vis Impair. 2016;34(3):214–224.
- Argyropoulos V, Kanari C, Hathazi A, et al. Children with vision impairment and multiple disabilities: issues of communication skills and professionals’ challenges. Paper presented at: International Conference on Education and New Developments (END 2020); 2020 June 27–29; Zagreb, Croatia.
- Ayyıldız E, Akçin N, Güven Y. Development of preverbal communication skills scale for children with multiple disabilities and visual impairment. J Hum Sci. 2016;13(2):2668–2681.
- Mallineni S, Nutheti R, Thangadurai S, et al. Non-verbal communication in children with visual impairment. Br J Vis Impair. 2006;24(1):30–33.
- Guellaï B, Callin A, Bevilacqua F, et al. Sensus communis: some perspectives on the origins of non-synchronous cross-sensory associations. Front Psychol. 2019;10:523.
- Stern DN. The interpersonal world of infant: a view from psychoanalysis & developmental psychology. New York (NY): Basic Books; 1985.
- Norton SJ, Schultz MC, Reed CM, et al. Analytic study of the Tadoma method: background and preliminary results. J Speech Hear Res. 1977;20(3):574–595.
- Obretenova S, Halko MA, Plow EB, et al. Neuroplasticity associated with tactile language communication in deaf-blind subject. Front Hum Neurosci. 2010;3:60.
- Rattray J, Zeedyk MS. Early communication in dyads with visual impairment. Infant Child Dev. 2005;14(3):287–309.
- Peltokorpi S, Daelman M, Salo S, et al. Effects of tactile imitation guidance on imitation and emotional availability. A case report of a mother and her child with congenital deafblindness. Front Psychol. 2020;11:540355.
- Chen D, Klein MD, Haney M. Promoting interactions with infants who have complex multiple disabilities: development and field-testing of the PLAI curriculum. Infants Young Child. 2007;20(2):149–162.
- Biringen Z, Derscheid D, Vliegen N, et al. Emotional availability (EA): theoretical background, empirical research using the EA scales, and clinical applications. Dev Rev. 2014;34(2):114–167.
- Campbell J. Understanding the emotional needs of children who are blind [research report]. J Vis Impair Blind. 2007;101(6):351–355.
- Campbell J, Johnston C. Emotional availability in parent–child dyads where children are blind. Parent Sci Pract. 2009;9(3-4):216–227.
- Nafstad AV, Rødbroe IB. Communicative relations: interventions that create communication with persons with congenital deafblindness. Aalborg: Materialecentret; 2015. Available from: https://www.statped.no/globalassets/laringsressurs/dokumenter/02-bokhefte/communicative-relations-uk.pdf
- Sameroff AJ, Chandler MJ. Reproductive risk and the continuum of caretaking casualty. In: Horowitz FD, Hetherington EM, Scarr-Salapatek S editors. Review of child development research. Vol. 4. Chicago (IL): The University of Chicago Press; 1975. p. 187–244.
- Sameroff AJ, Mackenzie MJ. Research strategies for capturing transactional models of development: the limits of the possible. Dev Psychopathol. 2003;15(3):613–640.
- Brede KS, Souriau J. Let me join your tactile attention: a sign language perspective on the communicative togetherness with a child who is congenitally deafblind. J Deafblind Studies Commun. 2016;2(1):4–21.
- Chiesa S, Galati D, Schmidt S. Communicative interactions between visually impaired mothers and their sighted children: analysis of gaze, facial expressions, voice and physical contacts. Child Care Health Dev. 2015;41(6):1040–1046.
- Hart P. Moving beyond the common touchpoint – discovering language with a congenitally deafblind people [dissertation]. Dundee: University of Dundee; 2010. Available from: https://discovery.dundee.ac.uk/en/studentTheses/moving-beyond-the-common-touchpoint-discovering-language-with-con
- Janssen MJ, Riksen-Walraven JM, van Dijk JPM, et al. Interaction coaching with mothers of children with congenital deaf-blindness at home: applying the diagnostic intervention model. J Vis Impair Blind. 2010;104(1):15–29.
- Lindström C. Contributing to a tactile language: partners communicative accommodation to a bodily/tactile modality. J Deafblind Studies Commun. 2019;5(1):50–72.
- Rogow SM. Rhythms and rhymes: developing communication in very young blind and multihandicapped children. Child Care Health Dev. 1982;8(5):249–260.
- Buelund Selling H. Apple trees and horse bus - conversation through bodily and mimetic utterances. In: Creutz M, Melin E, Lindström C editors. If you can see it, you can support it. Stockholm: Nordic Welfare Centre; 2019. p. 137–145. Available from: https://nordicwelfare.org/wp-content/uploads/2019/06/If-you-can-see-it-you-can-support-it-a-book-on-tactile-language.pdf
- Chen D, Downing JE. Tactile strategies for children who have visual impairments and multiple disabilities: promoting communication and learning skills. New York (NY): AFB Press; 2006.
- Chen D, editor. Essential elements in early intervention: visual impairment and multiple disabilities. 2nd ed. New York (NY): AFB Press; 2014.
- Miles B. Talking the language of the hands to the hands. New York (NY): The National Information Clearinghouse on Children Who Are Deaf-Blind; 2003. Available from: https://nationaldb.org/library/page/1930
- Ely MS, Ostrosky MM, Burke MM. Self-efficacy of providers of early intervention services to young children with visual impairments and their families. J Vis Impair Blind. 2020;114(2):114–126.
- Dyzel V, Dekkers-Verbon P, Toeters M, et al. For happy children with a visual or visual-and-intellectual disability: efficacy research to promote sensitive caregiving with the Barti-mat. Br J Vis Impair. 2021.
- Metell M. "A great moment … because of the music”: an exploratory study of music therapy and early interaction with children with visual impairment and their sighted caregivers. Br J Vis Impair. 2015;33(2):111–125.
- Platje E, Sterkenburg P, Overbeek M, et al. The efficacy of VIPP-V parenting training for parents of young children with a visual or visual-and-intellectual disability: a randomized controlled trial. Attach Hum Dev. 2018;20(5):455–472.
- Bateson MC. 'The epigenesis of conversational interaction’: a personal account of research development. In: Bullowa M, editor. Before speech: the beginning of interpersonal communication. Cambridge (UK): Cambridge University Press; 1979. p. 63–77.
- Bronfenbrenner U, Ceci SJ. Nature-nurture reconceptualized in developmental perspective: a bioecological model. Psychol Rev. 1994;101(4):568–586.
- Kratochwill TR, Hitchcock J, Horner RH, et al. Single-case design technical documentation. Washington (DC): What Works Clearinghouse; 2010. Available from: https://ies.ed.gov/ncee/wwc/Document/229
- Salo SJ, Flykt M, Mäkelä J, et al. The effectiveness of Nurture and Play: a mentalisation-based parenting group intervention for prenatally depressed mothers. Prim Health Care Res Dev. 2019;20:e157.
- Johnson N, Parker AT. Effects of wait time when communicating with children who have sensory and additional disabilities. J Vis Impair Blind. 2013;107(5):363–374.
- Antaki C, Wilkinson R. Conversation analysis and the study of atypical populations. In: Sidnell J, Stivers T, editors. The handbook of conversation analysis. Chichester: Wiley-Blackwell; 2013. p. 533–550.
- Bigelow AE. The development of joint attention in blind infants. Dev Psychopathol. 2003;15(2):259–275.
- Antaki C. Six kinds of applied conversation analysis. In: Antaki C, editor. Applied conversation analysis: intervention and change in institutional talk. London: Palgrave Macmillan; 2011. p. 1–14.
- Goodwin C, Heritage J. Conversation analysis. Annu Rev Anthropol. 1990;19:283–307.
- Schegloff EA. Sequence organization in interaction: a primer in conversation analysis. Vol. 1. Cambridge (UK): Cambridge University Press; 2007.
- Ask Larsen F. The washing-smooth hole-fish - and other findings of potential and negotiation strategies in conversation with congenitally deafblind children [master’s thesis]. Aarhus: University of Aarhus; 2003. Available from: https://nordicwelfare.org/en/publikationer/the-washing-smooth-hole-fish/
- Mondada L. Challenges of multimodality: language and the body in social interaction. J Socioling. 2016;20(3):336–366.
- Mondada L. Multiple temporalities of language and body in interaction: challenges for transcribing multimodality. Res Lang Soc Interact. 2018;51(1):85–106.
- Biringen Z, Fidler DJ, Barrett KC, et al. Applying the emotional availability scales to children with disabilities. Infant Ment Health J. 2005;26(4):369–391.
- Iverson JM, Thal DJ. Communicative transitions: there’s more to the hand than meets the eye. In: Wetherby AM, Warren SF, Reichle J, editors. Transitions in prelinguistic communication: communication and language intervention series. vol. 7. Baltimore (MD): Paul Brookes Publishing Co; 1998. p. 59–86.
- Bates E, Benigni L, Bretherton I, et al. Cognition and communication from nine months to thirteen months: correlational findings. In: Bates E, editor. The emergence of symbols: cognition and communication in infancy. New York (NY): Academic Press; 1979. p. 69–140.
- Iverson JM, Goldin-Meadow S. What’s communication got to do with it? Gesture in children blind from birth. Dev Psychol. 1997;33(3):453–467.
- Bråten S, Trevarthen C. From infant intersubjectivity and participant movements to simulation and conversation in cultural common sense. In: Bråten S, editor. On being moved: from mirror neurons to empathy. Amsterdam: John Benjamins Publishing Co; 2007. p. 21–34.
- Ratner N, Bruner J. Games, social exchange and the acquisition of language. J Child Lang. 1978;5(3):391–401.
- Alimovic S. Emotional and behavioural problems in children with visual impairment and multiple disabilities. J Intellect Disabil Res. 2013;57(2):153–160.
- Gul H, Erol N, Akin DP, et al. Emotional availability in early mother-child interactions for children with autism spectrum disorders, other psychiatric disorders, and developmental delay. Infant Ment Health J. 2016;37(2):151–159.
- Nachshen JS. Empowerment and families: building bridges between parents and professionals, theory and research. J Dev Disabil. 2004;11(1):67–75.
- Dunst CJ, Trivette CM. Helping, helplessness, and harm. In: Witt JC, Elliott SN, Gresham FM, editors. Handbook of behavior therapy in education. New York (NY): Plenum Press; 1988. p. 343–376.
- Carpenter B. Empowering parents: the use of a parent as research paradigm in early intervention. J Child Fam Stud. 1997;6(4):391–398.