
Abstract
This study explored how participation constitutes and is constituted by practices of power in group homes for people with intellectual disability. The study used disciplinary power as theoretical perspective and was based on 50 h of observation in two group homes with a total of 15 residents. The analysis identifies practices of power and their relationship to individual agency and participation. The results show that institutional structures construct practices of power that define codes of conduct for the group home residents and their possibility for participation. This study offers implications for the daily lives of residents in group homes for people with intellectual disability.
Introduction
A home is a fundamental aspect of constructions of identity, social relationships, independence and participation (Annison Citation2000; Sixsmith Citation1986; Tideman Citation2000). Research on group homes for people with intellectual disability labels has often focused on residents’ living conditions, on the content of the provided services and on support staffs’ management and promotion of residents’ autonomy and decision-making (see Kåhlin Citation2015; Talman Citation2018; Tideman Citation2000). Due to their intellectual disability labels, residents in group homes have been viewed as unable to make well-founded choices (Hellzen, Haugenes, and Östby Citation2018; Talman et al. Citation2019). Support in group homes are often based on the staff’s experiences and perceptions of what the residents need, which can negate and neglect residents’ voices in daily life decisions and limit their participation (Altermark Citation2017; Löfgren-Mårtensson Citation2013). Although group home staff aim to facilitate residents’ autonomy and participation, they may unintentionally exert their stronger power position to provide support and activities governed by social norms (Hellzen, Haugenes, and Östby Citation2018). In Sweden, group homes are founded on legislations that asserts individuals’ right to self-determination (SFS 1993:387 6 §); but, in practice, group home staff play a determining role in residents’ lives (Beadle-Brown et al. Citation2014; Löfgren-Mårtensson Citation2013). Although staff are present in residents’ homes to facilitate participation and independence, staffs’ support can take the form to ‘discipline’ residents and making them obedient (Hellzen, Haugenes, and Östby Citation2018) and self-governing, turning them into docile bodies by establishing repetitive rhythms and routines that foster desirable behavior (Foucault Citation1995).
Group homes establish a defined and structured environment with recurring daily routines – a context in which disciplinary power thrives (Axelsson and Qvarsebo Citation2017). The post-institutional era after the 1970s (c.f. Grunewald Citation2008) transformed institutional power practices in group homes, from sovereign- to disciplinary power, from reprimanding- and visible power to moralising- and invisible power (Foucualt Citation1995; Axelsson and Qvarsebo Citation2017). Altermark (Citation2017, 1317) discussed ‘the perceived break between the oppression of the past and the emancipatory ambitions of present’ and pointed out that power is ever-present and transformative. The power present in group homes today works by delineating what excluded groups should do to become included, thus linking power to knowledge and specifying what constitutes ‘truth’ in different contexts (Hall Citation2001).
The present study aims to understand how participation in group homes for people with intellectual disability constitutes and is constituted by practices of power, using the Foucauldian perspective of disciplinary power to analyses power practices in group home contexts. The following two questions guided the study (1) How are residents guided by codes of conduct? And (2) how do residents perceive and respond to practices of power?
Previous research
Group homes
The concept of a ‘home’ encompasses ideas of independence, privacy and freedom of choice: what individuals do in their home is their own business (Sjöström Citation2008; Smith Citation1994). A home is personal and is more than just a physical and architectural structure; it implies certain social relationships and interactions, security, happiness and belonging, and it is important for individuals’ identity formation (Clement and Bigby Citation2010).
In Sweden, people with intellectual disability labels are eligible for support from legislation concerning support and service for people with certain functional impairment (LSS), which aims to facilitate equal living conditions and participation in community, where housing is a specific support service (SFS 1993:387 9 §). Housing with special services (i.e. group homes) often consists of smaller apartments gathered around common areas with support staff available at all times (National Board of Health and Welfare Citation2018). Such apartments should be considered as the residents’ private homes. However, group homes are a unique residential environment; in addition to being an institutional living arrangement, they are also an ordinary residence and a workplace for support staff (Kåhlin, Kjellberg, and Hagberg Citation2016). Service providers thus play a critical role in the construction and reconstruction of residents’ conceptualisation of home (Clement and Bigby Citation2010).
The prefix ’group’ in ‘group homes’ defines them as being distinct from ‘normal’ homes. Residents in group homes share aspects of their home with other individuals whom they have not chosen for themselves (Löfgren-Mårtensson Citation2013; Tideman Citation2000), and must create relationships with both other residents and support staff (Clement and Bigby Citation2010). Residents can be firmly guided to participate in activities with other residents, and thereafter treated as a group rather than individuals. Goffman (Citation2007) describes this as a ‘block pattern’, in which group home staff aim to facilitate support through supervision. This can neglect the individual and emphasise ascribed labels, such as intellectual disability, by focusing on disabilities rather than abilities. Moreover, staff in group homes have conflicting duties towards residents: a duty of care, that is, provide support, and a duty to recognise and facilitate residents’ autonomy.
The group home is a context where staff often struggle to balance control, autonomy and guidance, while residents struggle with individuality, identity and intrusions into their private lives (Hellzen, Haugenes, and Östby Citation2018).
‘Normal’ participation
Participation has varying meanings for different people in different contexts. In sports and daily activity services, participation has been shown to relate to social interactions and performing, and plays an important role in identity formation and social positioning (Svanelöv et al. Citation2019; Svanelöv et al., Citationforthcoming). In group homes, participation can be described as different kinds of ‘doing’: doing with others, doing for others and being part of someone else’s doing. In addition, group home staff may perceive that residents’ participation and agency are limited by residents’ impairments, and that knowledge about residents’ own needs and desires may be insufficient (Bigby et al. Citation2015; Kåhlin Citation2015). Since support staff play a vital role in providing support and individual assistance to residents in group homes, it is not uncommon for services and support to be influenced by staffs’ personal values and attitudes. Support and services may also be influenced by the group home’s organisational culture (Löfgren-Mårtensson Citation2013; Power Citation2013; Talman et al. Citation2019).
The ‘normal’ is to be a full functional contributing citizen, but residents in group homes can be caught in a catch-22: they can accentuate their disability to increase their welfare support or they can emphasise their readiness for independence, whereby their welfare support will be reduced (Goodley Citation2014). Disability is thus perceived as a deviance from the normal and as a forced identity with involuntary alienation (Löfgren-Mårtensson Citation2013). People living in group homes are introduced to institutional support that also comprises much of their social network (Clement and Bigby Citation2010). Norms within such institutional structures mediate and reproduce power, and have the potential to both reinforce or undermine power (Foucault Citation1990). Established norms thus construct and legitimise differing aspects of participation and how apply to people viewed as deviant (see Löfgren-Mårtensson Citation2013).
The right for participation for people with intellectual disability is emphasised in policy documents worldwide (Hammel et al. Citation2008), and in Sweden through the LSS (SFS 1993:387), through the national action plan on disability policy ‘from patient to citizen’ (Government Bill 1999/2000:79) and through the national goal and direction of disability policies (Government Bill 2016/17:188). These policies stipulate rights to community, equality and moral citizenship, and they seek to prevent discrimination and facilitate participation for all individuals at all levels in society. In these policies, participation is defined as meaningful involvement in activities and decision-making processes, being able to express your voice, and the right to contest when participatory rights are denied. However, Shrewsbury (Citation2015) has argued that the voices of people with intellectual disability are often omitted or consist only of an ‘empty ritual of participation’. Participation entails civic activities and duties associated with citizenship, which people with intellectual disability often cannot live up to because of their stigmatised and deviant status and their consequently diminished opportunities (Altermark Citation2017). Power within the realm of disability services operates by constructing ideals of self-determination, independence and participation (Altermark, Citation2016), from which people with intellectual disability can be subjected to paternalism and reprimanded if their behavior does not live up to the ideals (Yates, Citation2005).
Institutional power in group homes
Institutions can be characterised as a means of observation and surveillance or of safety and knowledge; individualisation and totalisation, isolation and transparency. Institutions are embedded with and reproduce disciplinary power, and punishment and reward practices that can foster dependence or independence (Axelsson and Qvarsebo Citation2017; Foucault Citation1990; Citation1995). Group homes regulated by the LSS are not supposed to be institutional in character (National Board of Health and Welfare Citation2018) and are supposed to facilitate goals of individual independence and participation. Although group homes conditions are considerably better today than before their official deinstitutionalisation in the 1960s (c.f. Clement and Bigby Citation2010; Grunewald Citation2008), there are still institutional power mentalities in their organisation (Altermark Citation2017), notably by the use of ‘goodwill’ guidance to foster residents citizenship, independence and participation. That is, the institutional structures ‘teach capabilities that they perceive as necessary to enable people with intellectual disabilities to become integrated community members’ (Altermark Citation2017, 1324). Institutional power structures in group homes formulate what excluded groups should strive for in order to become included, and this power shapes the everyday lives of group home residents (Altermark Citation2017; Löfgren-Mårtensson Citation2013). Although group home services and supports are ostensibly intended to serve residents and facilitate their independence and self-determination, these services are often performed within structured constraints (Clement and Bigby Citation2010) that can limit residents’ way of life (Altermark Citation2017; Löfgren-Mårtensson Citation2013).
Theoretical framework
The present study’s theoretical framework was inspired by Foucault’s discussion of disciplinary power as a set of instruments, techniques and procedures that demonstrate the ‘right’ way (Foucault Citation1995). The study focuses on practices of power within group homes. Power surrounds everything and is ever-present; it is not about the degree of tolerance or oppression but about how and in what ways it is characterised (Foucault Citation1995). Disciplinary power ‘makes individuals; it is the specific technique of a power that regards individuals both as objects and as instruments of its exercise’ (170); it guides (and sometimes forces) ideas of what is good for the individual (Altermark Citation2017; Välikangas and Seeck Citation2011) and creates rules by which individuals must abide (Foucault Citation1990). This conforming power is present in institutional settings that focus on constructing moral and ethical community members (Axelsson and Qvarsebo Citation2017).
Disciplinary power create boundaries and practices for that which is culturally and socially acceptable to say and do (Edley Citation2001; Engström Citation2012; Foucault Citation1972). Different practices of power form ideological bases, which compare and differentiate individuals according to desired norms (c.f. Foucault Citation1995; Carabine Citation2001; Hörnqvist Citation2012). Power practices can be expressed in conformity or resistance to sanctioned ways of conduct – standards of conduct that individuals must relate to in order to be legitimised, accepted or denied or to negotiate their social position. Power practices can also impose a conduct of conduct, where conformity or resistance make individuals ‘discipline’ and position themselves from discourses’ boundaries and knowledge of what is acceptable (Hall Citation2001).
Method
This study was based on observations in two group homes. The data consist of field notes with descriptions of situations in which residents received support from staff and of everyday situations in the residents’ apartments or common areas.
Ethical considerations
This study was approved by the Ethical Board of Uppsala, Sweden (dnr: 2015/391/1), and the research followed the good research practice ethical guidelines and regulations of the Swedish Research Council (Citation2017). Group home residents were provided with both written and oral information about the study and they provided informed consent, either orally or via sign language, before- and continually during observations (consent was reobtained every time before entering their apartment and every time the residents received help and support from staff). Group home staff were given information about the study, and they also provided informed consent, since they are part of the residents’ daily lives providing support. In some cases, staff members were unwilling to participate. In the instances, observations were not conducted while they provided support to residents. The residents’ legal guardians or trustees were also informed about the study (Clement and Bigby Citation2013).
The use of observations in residents’ homes necessarily involved an intrusion into their private life, and this was discussed with staff, residents and their trustees or legal guardian. These discussions included information about the research’s purpose of serving the greater good and the eventual consequences for the residents. The residents’ confidentiality was assured to the greatest extent by assigning fictive names and by keeping field notes separated from contact information. Specific details in the field notes were altered and locked up (Bryman Citation2016).
Research participants and data collection
The research participants were residents in group homes for people with intellectual disability, assigned through LSS. Observations were conducted at two group homes, each of which had a shared common area/living room and kitchen. One group home consisted of ten individual apartments while the other had five. In total, 15 residents, between 27 and 83 years of age, were observed on 14 occasions in October and November 2018. Observations took place on all days of the week, at all hours of the day, except at night, and lasted around 3.5 to 4 h, with a total of 50 h of observation. Intimate situations, such as showering and undressing, were not observed.
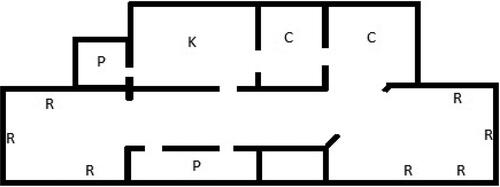
The smaller group home was a standalone building with five apartments. The larger one occupied two floors in a tower building and consisted of a total of ten apartments (seven were located on one floor, while three apartments were located on a different floor; other tenants in the building were not assigned by LSS). Both group homes were centred around staff accommodation rooms and a common room and/or kitchen, with adjoining corridors where the residents’ apartments were located (see and ). Both group homes were located close to grocery stores and bus stops in fairly populated areas. The group homes interior were neither newly renovated nor particularly worn. The walls were painted white, beige and light brown, with linoleum floors.
Figure 1. Group home 1. R = resident; K = kitchen; C = common area; P = staff accommodation room.
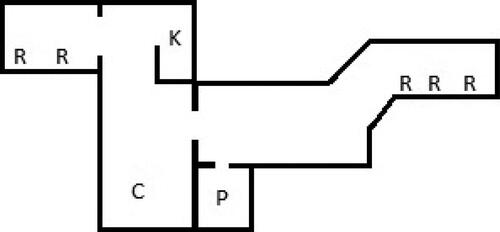
Figure 2. Group home 2. R = resident; K = kitchen; C = common area; P = staff accommodation room.
Observations were conducted through the role of the observer as participant method (Burgess Citation1984): the observer was present in the same room as the residents under observation, but the observer stayed in the background and did not interrupt the resident’s activities. Observations were conducted in the residents’ apartments, the group home common areas and in the staff accommodation rooms. During observations, the observer engaged residents in conversations about observed situations, following what Burgess (Citation1984) calls interviews as conversations.
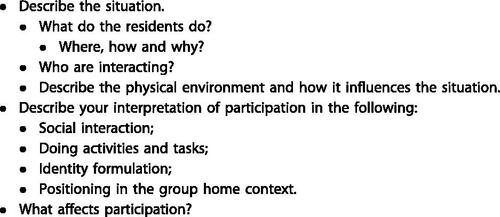
An observation schedule was used to identify different aspects of participation in observed situations (Wolcott Citation1990). The schedule was based on previous studies on participation and on policy documents (c.f. Svanelöv et al. Citation2019, Citationforthcoming; Kåhlin Citation2015; Government Bill 1999/2000:79, 2016/17:188) (see ).
Figure 3. Observation schedule.
Field notes of observations consisted of descriptions of situations, details of conversations and accounts of events. It was sometimes inappropriate to write down field notes, for example in emotional situations or when residents interacted directly with the observer; in these instances, notes were recorded later from memory, or key notes were written down during natural pauses in social situations. At the end of each observation session, comprehensive notes about all that transpired were written down (Bryman Citation2016; Burgess Citation1984). Filed notes also included the observer’s personal reflections and interpretations of observations and of the events that transpired during the observations (Burgess Citation1984).
Analysis
The study’s analysis focused on how residents related to practices of power in group homes, using the theoretical framework of disciplinary power. Different practices of power were identified and derived based on recurrent themes, inter-relationships, overlaps and absences in the field notes (Carabine Citation2001). The analysis focused on how residents interacted with their physical environment, with other residents and with staff, as well as interpreting what the interaction meant in regard to participation. The analysis process was iterative, and field notes were read and reread thoroughly several times to identify themes (Winther Jörgensen and Philips Citation2000). Theme analysis then identified discursive patterns of how power creates conditions for participation and how power positions residents in relation to ‘normal’ views of participation, how and in what ways power interacted with the residents and how and in what ways residents were subjected to power that hindered or facilitated participation (c.f. Foucault Citation1972, Citation1995).
Results
The results presents the themes identified by the analysis and describes ample situations in order to provide transparency. In Group home 1 lived Zoe, Darin, Lisa, Bert, Diana, Emma, Ruby, Eva, Carl and Jessica; in Group Home 2 lived Karin, Alberto, Anna, George and Jonathan.
A scheduled must
The scheduled agenda in the group homes structured residents’ daily living. The availability to do things whenever they wanted was limited, and residents’ expression of desires or demands, for example ‘I want to eat now’ or ‘can I have coffee now?’ were limited to times when support was scheduled.
I entered Diana’s apartment (with her approval) with a staff member (who had a scheduled support). The staff member asked if Diana wanted to have some dinner. Diana answered that she did not want to eat right now. The staff member responded that now is when they have time to help.
This extract shows how residents had to conform to schedules and institutional support structures for everyday activities like eating dinner. Eating and hunger were thus adapted to an institutional clock that dictated specific times at which support could be provided.
Diana sits in the kitchen, waiting for a staff member to prepare dinner. Diana has difficulty walking and uses a walker. The support staff member has prepared dinner and serves her a plate of food. Diana eats in the kitchen; meanwhile, the staff member does the dishes and tidies in the kitchen. When Diana has eaten, she asks if she can go to the toilet. The staff member helps her use the toilet and then leaves the apartment.
This extract illustrates the structured and scheduled context of group homes. Diana’s meal situation is a ‘support service’; she sits idle and waits for her dinner to be prepared and is not being active in its preparation. She eats alone, and while she eats, other scheduled chores and support services are accomplished by the staff member. Diana’s idleness could be interpreted as laziness or cunning, as she receives dinner without much personal effort. However, it can also be interpreted as exclusion from everyday decisions; a passive acceptance of institutional effectiveness. The group home has a limited amount of time to provide support, and in this context Diana’s dinner is constructed as a support service, not a meal time. The social networks established in group homes are formed on the basis of professional relationships, not friendship, and guide residents passively accept ‘normal’ ways.
In addition, Diana has difficulty walking and going to the toilet by herself; thus, she ask for permission to use the lavatory. Attentiveness to institutional structures means that everyday obstacles can be perceived as a liability. For example, the need to use the toilet, even in one’s own home can be perceived as a burden for the residents towards those helping. In addition, use of a question to request permission to use the toilet speak about something ’unspoken’, that Diana may have been previously denied such permission. Sanctioned codes of conduct must be heeded by residents as is further demonstrated in the following two extracts:
It is morning around 8:30 a.m. and Lisa leaves her apartment and walks up to the staff accommodation room and says that she wants breakfast. A staff member tells her to wait and to go back to her apartment. Breakfast is served at specific times, when staff are scheduled to provide support.
It is Tuesday morning. Zoe sits in her armchair waiting for breakfast. She wants to shower. A staff member tells her that she has to wait until evening. ‘Then it’s your time to shower’.
Here it becomes clear that residents have to conform to specific times for meals, washing etc., when staff support is scheduled, thereby embedding an authoritarian power structure. The scheduled support and activities can also be connected to normative views of doing things; for example, breakfast is eaten 9 a.m., neither earlier nor later.
Zoe and I sit in the kitchen (a common area). She wonder what is in my notebook. I say that I take notes of what is happening here and ask if she wants to look at it, but she declines. She wants me to draw. I draw animals, and she guesses at what I am drawing. I ask her if she likes to draw; she does but they do not do it so often. I ask why, and she says it is because there is no time. I ask the staff if they draw or do things in the common areas. They say that they do it sometimes, but only when it is on their schedule.
The residents do not have many activities outside scheduled support services. The group home context emphasises duties of care and professional work rather than friendship and social support; even if some staff would like to draw with the residents, there is no organisational support for activities outside the scheduled structure.
In the situation described in the extract above, Zoe did not want to draw. It could be simply that she did not want to; but based on her answers that ‘they do not do it so often’ and that ‘there is no time’, and that drawing is provided as a ‘support activity’, it is possible that Zoe may not want to draw because she feels that it conflicts with what is expected. Drawing is a controlled social activity and a planned support, and the desired behavior for residents is to not draw.
From the hallway, I hear Alberto screaming from his room. He does not want to shower and screams ‘Ouch! What are you doing!’, ‘no!’, ‘stop!’. Alberto is scheduled to have support to shower now.
The line between fostering, helping and supporting individuals in their everyday lives is a delicate balance. Alberto does not want to shower at this moment, but staff have time to help him now. The extract above show how participation is a scheduled must. Support services regulated by LSS and other disability policy documents, and aim to enhance and facilitate individuals’ independence and participation. It comes down to institutional ideals of fostering ‘good residents’ and ideas of what is good for the individual.
Negotiations of power
Bert sits on his couch and I sit on a chair next to him. In the kitchen (in Bert’s apartment) there is a staff member trying to prepare dinner, looking for things in the kitchen cabinets. After a while the staff member walks up to Bert and says that he has to moisturise his skin and gives him a lotion bottle, but Bert does not want to. The staff member say that he has to do it, and Bert says ‘ok, but it has to be on my conditions’. Bert says that he has pain in his shoulder, so he cannot take off his shirt or apply his lotion by himself; he tells the staff member to do it. The staff member agrees after a while, but implies that Bert is convenient. After the staff member has applied lotion for him, Bert put on his shirt by himself.
Bert is told that he has to moisturise his skin even though he does not want to. Regardless of whether Bert needs to apply moisturising lotion, ideals of ‘what is good for him’ are imposed on him. However, Bert does not simply conform to these ideas; he negotiates the terms of conduct by strengthen his role as a ‘disabled person’ in the care receiver-care provider relationship, thus maintaining some control over the situation. However, it is noteworthy in this extract that Bert did not express strong enough power to control the ultimate results of planned support activity (lotion was applied to him), or perhaps he was unable to; he only negotiated the established terms.
I sit on a chair in Bert’s living room; Bert sits next to me on his couch. We talk about support and participation. He is happy with the support and help he receives with domestic chores. He says that he also helps the staff do the dishes in the common kitchen. When I ask him if one can participate in one’s owns home, he says ‘If I’m participating in my home? Well yes, what else if not more!’
Bert thus implied that participation in his own home is a kind of meta-participation; it is something more than being part of something in his own home. I observed that when staff told Bert to do things, such as apply lotion, undress or put on socks, he indicated that he had pain, poor balance, was cold or had no energy, thereby using his perceived weaknesses as instruments with which to negotiate power. Bert tested the staffs’ boundaries and reinforced his status as a ‘disabled person’ in order to receive more help and support, while staff appeared to adopt an ‘it-goes-faster-if-I-do-it-myself’ attitude. Diana also tested the staffs’ willingness to do things for her and to alter the hierarchical power relationship between her and them:
Diana asked a staff member if they could go and buy cigarettes for her. She says that she cannot find the store well and that she does not have the energy to go shopping. The staff member says that they cannot help her with that now. I asked Diana if the staff usually help her with buying cigarettes, and she said ‘yes sometimes’. I also asked the staff if they help Diana buy cigarettes, and they said that she can and usually does it herself, but she often wants company. However, there is limited time.
By emphasising their difficulties and perceived weaknesses, residents thus resisted or negotiated enforced practices and tried to receive more than their routinely allocated support. Although staff could ignore the residents’ attempts to strengthen their normative roles as ‘disabled’, residents could usually alter the terms of their support. However, since the staff were in a stronger power position they construct what residents should abide by to in order to receive support.
In addition, social interaction with staff members formed a major part of residents’ social network and their attempts to receive more support also served to extend these social interactions. Social relationships between residents and staff were structured by the group home context and by staffs’ obligation to maintain professional distance from the residents. Interactions also had the potential to impact residents’ support services, creating ideological binaries between professional work and friendship, between dependence and independence.
Institutional structure
While I am wandering the hallway of the group home, Lisa comes out of her apartment and says that she wants coffee. There are no staff to hear her, so she raises her voice as she walks down the long narrow hallway. She stops outside the staffs’ accommodation room, whose door is open, and becomes quiet. She does not knock or say anything to get the staffs’ attention, but waits for the staff to notice her. When they do, she repeats her desire for coffee. The staff tells her that she cannot have coffee now; she has to wait. Lisa asks if she can wait in the kitchen (common area), but she is instructed to wait in her apartment. Lisa walks quietly to her apartment.
As illustrated by this extract, some doors need not be closed to signal ‘no entry’; but they express a restrictive power. The institutional structure of group homes creates a sovereign and disciplinary power that seeks to shape ideal behavior; there is a right time for drinking coffee; you cannot disturb those in higher position of power; and you have no access to certain areas in the group home, even though common areas should be available for all. In the extract above, Lisa’s apartment becomes an expression for ‘banishment’. The following two extracts further illustrate the role of the private apartments and doors within the group homes:
(Group Home 1) I am sitting in the hallway (outside some apartments), and all the residents’ doors are open, except for Jonathan’s; he closes his door and is firm that it should be closed. However, when there are many scheduled support services in residents’ apartments, even Jonathan’s door is open. Alberto’s apartment door is open, and I hear him call for help to get out of bed. It is morning and he wants to get up. Nobody hears him, so he remains in his bed.
(Group Home 2) Darin’s door is always open. I asked the staff why, and they said it is because he is old and has many scheduled support services. For example, Darin needs to be reminded to go the bathroom, and it easier for the staff if the door is open. In the same hallway, Zoe always has her door open, even if the staff want it to be shut. Zoe sits in her armchair in front of her TV, and is positioned so she can see out through her door and along the long hallway were the other residents’ apartments, the staff accommodation rooms and the common areas are located.
Doors are a symbolic expression of power, availability and access. It signals something when the door to one’s home is open, and the meaning differs when residents choose to open it themselves or if it is staff make that decision. Residents who receive extensive attention and hygienic support (e.g. going to toilet and undressing), such as Darin and Alberto, often have their doors open due to their extensive need for care. This openness into residents’ apartments can be seen as an intrusion into their private lives. I asked Anna’s opinion of the ‘open door policy’ and she said that she did not like it; she felt that she could not be herself or do what she wanted. For Alberto, who lay in his bed and called for help, the ‘open door policy’ did not work in attracting the attention of the staff. Along with several other residents, he also had an alarm to call staff. For the alarm to be triggered he needed to push a button on a remote or activate a motion sensor in the apartment. But when residents cannot get out of bed by themselves, they must wait for their scheduled support time to be seen or heard.
Lisa sits at the dining table in her apartment while a staff member, standing by the kitchen sink, asks what she wants to eat. The question is more of a reminder to Lisa as she has a weekly dinner schedule. I look in the kitchen cabinets while the staff member takes out a plate and glass, and see that they are quite empty. I look at the fridge and freezer and notice that they have locks. The staff member leaves the apartment. I ask Lisa what the locks on the fridge and freezer are there for, and she replies that she does not know. The staff member comes back with Lisa’s dinner and leaves the apartment. The staff member says that Lisa cannot have food in her apartment, because then she will eat it all.
This extract demonstrates that the lack of food in Lisa’s apartment (as well as in Anna’s apartment in group Home 2) was due to an institutional decision; she was considered unable to handle having food in her apartment. The locks on the fridge and freezer did not have a practical use. Since the fridge and freezer were empty; rather, the locks served as a powerful statement of appropriate behavior.
Another example of institutional ideas of what is good for the individual being imposed was a situation that occurred when Diana asked for coffee with her lunch and a staff member said no. Diana then asked if she could have coffee after lunch and the staff member said yes. This enforced the normative idea that coffee should be drunk after lunch, not during, and that the staff knows what was good for her.
I sit at the dining table in the common area (kitchen), at 6 p.m. A staff member is preparing Alberto’s dinner. They roll him (in his wheelchair) from his apartment to the common area (kitchen) and stops him next to (not in front of) the table. Alberto has an eating tray on his wheelchair. Alberto says that he does not want to eat, but he is being told that he must. He gets anxious and sad. For a while he sits and stares at the food, which is placed on his tray, and eventually he eats with low interest.
Institutional ideas of a ‘good resident’ or of the ‘correct’ way of behaviour are illustrated here. Alberto ‘needs’ to eat at this time. It is the same time as yesterday and the day before that; Alberto needs to eat now because of the staff have to follow the schedule in order to provide support to other residents.
I have spent many hours in the common areas and they are often empty. Residents usually use these areas when the staff have scheduled support, such as joint fika (drinking coffee and socialising) or mealtimes. On one Thursday evening, around 7 p.m., I sit in the television-room (a common area) with Alberto, Karin and George (Alberto and Karin use wheelchairs and need the staff’s help to move around) watching television. The staff are preparing the residents for bed sequentially, moving to and from the television-room. One by one, the residents are withdrawn from watching television and are prepared for bed. Are the common areas natural areas designed for residents, or have the staff established the rules for their use?
A television is central in many residents’ apartments as well as in the common areas and watching television occupies a substantial part of residents’ time. All residents have access and possibility to go outside, but during my observations, residents only went outside when the staff had a scheduled support or had scheduled time to accompany the them, for instance to go grocery shopping or take a walk. Some residents had daily activity services and went by taxi, only Zoe went outside by herself, to take out the garbage. Similarly, activities in the common area were rarely spontaneous: they were typically structured and planned support, alongside the staff. Television was a means for distraction while residents were waiting to go to bed; during this time, the staff had a tight schedule and high workload, meaning that support took the form of an assembly line.
Architectural boundaries
The Staffs’ accommodation rooms were centrally located within each group home, with corridors on each side, leading to residents’ apartments. The architectural structure of the group homes speaks of closeness to support and help as well as surveillance, control and prohibition. The common areas were also centrally located, next to the staffs’ accommodation rooms, creating an invisible, yet visible, surveillance and decisive power. The omnipresent power was that residents seemed to feel a need for ‘permission’ to use common areas. Their presence in the common areas – for example, drinking coffee together every day at 7 p.m., and watching television before bed – was deemed a support service, initiated by staff.
Discussion
Participation in the group home context is delimited and opened up by practices of power, which define what is considered acceptable and residents’ positions within the group homes. The following discussion identifies such practices of power.
Conformity, resistance and negotiation
Participation is constituted according to hierarchal power relations of disciplinary or fostering ideals; residents must either conform to, resist or negotiate with the institutional structures. The group home context creates institutionally defined time-frames that are constructed to ‘help’ or guide residents to a ‘good’ life – a life that is considered to conform to ‘normal’ routines. Conforming to the rules for support is vital to residents’ participation in the group homes. The group homes’ practices of power ‘make individuals’ (c.f. Foucault Citation1995) self-governing from that which is perceived as normal. The group home context labels residents as being abnormal; otherwise, they would not have special housing via LSS, ‘Normal’ for group home residents therefore deviates from ‘normal’ citizens’ routines.
The Support structures in the group homes help residents with some essential daily tasks, such as getting out of bed and preparing meals. Residents are at a crossroads of conformity and resistance; conformity, or acceptance to established structures can facilitate participation – but participation for whom? To draw on Foucault’s (Citation1995) ideas of disciplinary and sovereign power and Freire’s (Citation2017) ideas of oppression, if you are living and operating in an institutional context of surveillance, oppression and fostering, ideas of the ‘normal’ are shaped from this mould. Conforming to these practices of power within this context can lead residents to internalise institutional ideals of participation; but in order to notice and be aware of different power practices that ‘control’ admission to participation, you have to resist them and ‘break free. Only after challenging prevailing practices of power can participation be reconstructed and negotiated.
When Diana asked if’ she could go to the toilet or when Zoe asked if she could shower now, they speak of an obedience to the mandated schedules of the group home’s support services. The support schedule controls everyday life to the extent that basic needs, such as using the lavatory or washing up, manifest as inconveniences. Sjöström (Citation2008) argued that the concept of ‘home’ encompasses independence and freedom of choice; but group homes are modified to accommodate legislation, work procedures and financial constraints, which derives from ‘normal’ ways of living. Group homes thus enforce practices of power to which residents must conform, or else resist or negotiate with, in order to ‘have’ participation.
Contradictory beliefs
Power practices in group homes are based on two contradictory ideologies. On the one hand are ideas of caring for the individual, providing support and fostering the individual to be a ‘good resident’ and learn the ‘normal’ ways of living. On the other hand are ideas of facilitating individuals’ independence and participation in community. Engström (Citation2012) described this as conflicting ‘truths’, and Foucault (Citation1995) argued that ideological beliefs are controlled, selected, organised and shared by certain people to either limit or strengthen their power. How this power is limited or strengthened is shown through power practices.
Residents could use these conflicting beliefs to resist, challenge or negotiate practices of power by strengthening their normative roles; that is, by emphasising their stereotypical roles in the group home context and of ‘being disabled’. By emphasising their support needs and their dependence, residents could make staff provide more support – although still according to an inflexible schedule. Although staff did not provide substantially more support to residents, their attempts to facilitate residents’ independence could be hindered. At the same time, the residents’ attempts to strengthen their normative roles indicated their acceptance of society’s categorisation and labelling of disability. However, since societal rules dictate that support is only provided on the basis of disability, residents strengthened their independence by reinforcing their dependence.
Fostering ‘good’ residents
Power practices of ‘what is right for you’ were hard for residents to resist. These practices of power are imbedded in group homes’ institutional character and the historical view of disability; they are ever-present and transformative and dictate what residents should do to be ‘normal’. As noted by Altermark (Citation2017), the group home context today still has an institutional character, albeit with different practices of power than in the era prior to the deinstitutionalization.
As observed by Talman et al. (Citation2019), staffs’ professional attitudes towards residents were prominent in group homes. However, while Talman et al. discussed being professional as a way for staff to be aware of residents’ needs and abilities, in this study, being professional in your work was observed to be in contrast to friendship, and consisted primarily of performing support in a structured and ‘correct’ way. In addition, Power (Citation2013) and Löfgren-Mårtensson (Citation2013) noted that staff play an influential and controlling role in resident’s lives. Support can take the form of both caring and discipline, guiding residents to being ‘good’ residents. The rejection of Diana’s request to have coffee with her lunch and Zoe’s schedule of showering in the evening are both examples of this.
Participation was constituted by others’ better knowing; someone else determined the ground rules for participation, to which residents had to conform or negotiate. As noted by Axelsson and Qvarsebo (Citation2017), the quasi-institutional setting of a group home establishes conformity and disciplinary power, presumably with good intentions, but with an inevitable focus on constructing morally good and cooperative community members. Such attempts to foster ‘good’ behaviour can take the form of conduct of conduct, to which residents must subordinate to practices of power. For example, activities such as drawing were considered to be a support activity, and attempting to do so outside of the scheduled time created conflicts. By not initiating activities outside of the planned structure, individuals were acting in a desirable way, and were not threatening discursive boundaries.
The invisible line
Practices of power are often unspoken; they are perceived but not clearly articulated. In group homes, invisible lines position individuals within a hierarchy. In the study, invisible lines restricted residents’ access to certain areas, such as staff accommodation rooms. During my observations, only Lisa tried to contact staff who were in their accommodation room and she did so via a reserved silence; although the door to the staff room was open, it was still closed, her access was restricted. The invisible line represent sovereign power (c.f. Foucault, Citation1995), prohibition and restriction. Residents were not allowed through some doors, and the common areas were reconstructed as places for scheduled support activities.
Artefacts, such as doors, are excellent instruments with which to enact practices of power, especially when the choice of having the door to one’s home open or closed is not within the individuals’ control but is sanctioned through institutional agendas. Group homes, including the residents’ apartments, are both homes and a workplace, with conflicting interests. An open door thus both facilitates support and at the same time limits independence, privacy and freedom of choice, constructing power as invisible and visible at the same time. In relation to Bentham’s panopticon (Axelsson and Qvarsebo Citation2017; Foucault Citation1995), power practices construct invisible lines, where control, support, guidance and discipline becomes visible and invisible at the same time; residents cannot be sure whether they are alone or watched.
Methodological considerations
It is impossible to know whether and to what extent a research context has been influenced by an observer and how the observer is influenced by the research context. For example, in the present study, it is not known whether residents’ answers or reflections would have been the same in the absence of an observer. I attempted to reduce this uncertainty by becoming acquainted with the context cultural preferences and terminology used in the group home and by establishing relationships with the group home staff and residents, while disturbing the social situations as little as possible (Burgess Citation1984). However, as a researcher, I am also part of the discursive representation presented here. This article is both a constructor and a product of ways of talking about participation.
In qualitative research, it is often difficult to draw a line between the good of research and consequences for the research participants. In the present study, group homes are the residents’ homes, the staffs’ workplace and research site for researchers. This said: how long can the researcher go before intervening in sensitive or potentially harmful situations? When does the observer stop being a researcher and becomes a helping hand? Too much involvement in the residents and staffs’ daily routines would have biased the data. On the other hand, too little social involvement and a distant attitude could have created uncomfortable situations where the researcher participants do not act as they normally do.
Conclusion
This study does not suggest that group homes take the form of ‘the lyricism of the cold monster’ (Foucault Citation2007, 144); they are not totalitarian institutions that oppress and reign over residents. However, their structured and planned executions of power attempts to foster cooperate behaviour and conduct of conduct. Practices of power are inherent in group homes, and individuals must conform to, resist or negotiate these practices and position themselves within its hierarchy. Power practices constitutes and legitimise what is acceptable and desirable. Residents are in a subordinate power position and their participation is constructed by powerful guidelines based on normality.
This study offers implications for the daily lives of residents in group homes for people with intellectual disability. Increased understanding of how participation is constructed and how practices of power opens up or delimit participation. The study also elucidates institutional structures that can be used to facilitate participation in group homes.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Related Research Data
References
- Altermark, N. 2016. “After Inclusion: Intellectual Disability as Biopolitics.” PhD diss., Lund University.
- Altermark, N. 2017. “The Post-Institutional Era: Visions of History in Research on Intellectual Disability.” Disability & Society 32(9): 1315–1332. doi:10.1080/09687599.2017.1322497.
- Annison, J. E. 2000. “Towards a Clearer Understanding of the Meaning of ’Home.” Journal of Intellectual & Developmental Disability 25(4): 251–262. doi:10.1080/13668250020019566-1.
- Axelsson, T., and J. Qvarsebo. 2017. Maktens skepnader och effekter: Maktanalys i Foucaults anda. Lund: Studentlitteratur.
- Beadle-Brown, J., J. Mansell, B. Ashman, J. Ockenden, R. Iles, and B. Whelton. 2014. “Practice Leadership and Active Support in Residential Services for People with Intellectual Disabilities: An Exploratory Study.” Journal of Intellectual Disability Research 58(9): 838–850. doi:10.1111/jir.12099.
- Bigby, C., M. Knox, J. Beadle-Brown, and T. Clement. 2015. “We Just Call Them People’: Positive Regard as a Dimension of Culture in Group Homes for People with Severe Intellectual Disability.” Journal of Applied Research in Intellectual Disabilities 28(4): 283–295. doi:10.1111/jar.12128.
- Bryman, A. 2016. Social Research Methods. Oxford: Oxford University Press.
- Burgess, R. G. 1984. In The Field: An Introduction to Field Research. London: Unwin Hyman.
- Carabine, J. 2001. ” “Unmarried Motherhood 1830–1990: A Genealogical Analysis.” In Discourse as Data: A Guide for Analysis. M. Wetherell, S. Taylor, and S. J. Yates, eds., 267–310. Los Angeles: Sage.
- Clement, T., and C. Bigby. 2010. Group Homes for People with Intellectual Disabilities: encouraging Inclusion and Participation. London: Jessica Kingsley Publishers.
- Clement, T., and C. Bigby. 2013. “Ethical Challenges in Researching in Group Homes for People with Severe Learning Difficulties: Shifting the Balance of Power.” Disability & Society 28(4): 486–499. doi:10.1080/09687599.2012.711245.
- Edley, N. 2001. “Analysing Masculinity: Interpretative Repertoires, Ideological Dilemmas and Subject Positions.” In Discourse as Data: A Guide for Analysis. M. Wetherell, S. Taylor, and S. J. Yates, eds., 189–228. Los Angeles: Sage.
- Engström, A. 2012. “ Dimmornas bro: en berättelse om konstruktionen och iscensättandet av kliniska adjunkter.” PhD diss., Mälardalen University.
- Foucault, M. 1972. The Archaeology of Knowledge and the Discourse on Language. New York: Pantheon Books.
- Foucault, M. 1990. The History of Sexuality Vol. 1 the Will to Knowledge. Harmondsworth: Penguin.
- Foucault, M. 1995. Discipline & Punish: The Birth of the Prison. New York: Vintage Books.
- Foucault, M. 2007. Security, Territory, Population: Lectures at the Collège de France 1977–1978. New York: Palgrave Macmillan.
- Freire, P. 2017. Pedagogy of the Oppressed. London: Penguin Classics.
- Goffman, E. 2007. Asylums: Essays on the Social Situation of Mental Patients and Other Inmates. New Brunswick, NJ: Aldine Transaction.
- Goodley, D. 2014. Dis/Ability Studies: theorizing Disablism and Ableism. London: Routledge.
- Government Bill. 1999/2000:79. Från patient till medborgare – en nationell handplinsplan för handikappolitiken. Stockholm: Ministry of Health and Social Affairs.
- Government Bill. 2016/17:188. Nationellt mål och inriktning för funktionshinderspolitiken. Stockholm: Ministry of Health and Social Affairs.
- Grunewald, K. 2008. Från idiot till medborgare: de utvecklingsstördas historia. Stockholm: Gothia.
- Hall, S. 2001. “Foucault: Power, Knowledge and Discourse.” In Discourse Theory and Practice: A Reader. M. Wetherell, S. Taylor, and S. J. Yates, eds., 72–81. Los Angeles: Sage.
- Hammel, J., S. Magasi, A. Heinemann, G. Whiteneck, J. Bogner, and E. Rodriguez. 2008. “What Does Participation Mean? an Insider Perspective from People with Disabilities.” Disability and Rehabilitation 30(19): 1445–1460. doi:10.1080/09638280701625534.
- Hellzen, O., M. Haugenes, and M. Östby. 2018. “It’s My Home and Your Work’: The Views of a Filmed Vignette Describing a Challenging Everyday Situation from the Perspective of People with Intellectual Disabilities.” International Journal of Qualitative Studies on Health and Well-Being 13(1): 1468198–1468199. doi:10.1080/17482631.2018.1468198.
- Hörnqvist, M. 2012. En annan Foucault. Stockholm: Carlssons.
- Kåhlin, I. 2015. “Delaktig (även) på äldre dar: åldrande och delaktighet bland personer med intellektuell funktionsnedsättning som Bor i gruppbostad.” PhD diss., Linköping University.
- Kåhlin, I., A. Kjellberg, and J. E. Hagberg. 2016. “ Choice and Control for People Ageing with Intellectual Disability in Group Homes.” Scandinavian Journal of Occupational Therapy 23(2): 127–137. doi:10.3109/11038128.2015.1095235.
- Löfgren-Mårtensson, L. 2013. “Hip to Be Crip’ about Crip Theory, Sexuality and People with Intellectual Disabilities.” Sexuality and Disability 31(4): 413–424. doi:10.1007/s11195-013-9287-7.
- National Board of Health and Welfare. 2018. Bostad Med Särskild Service För Vuxna Enligt LSS. Stockholm: National Board of Health and Welfare.
- Power, A. 2013. “Understanding the Complex Negotiations in Fulfilling the Right to Independent Living for Disabled People.” Disability & Society 28(2): 204–217. doi:10.1080/09687599.2012.699280.
- SFS 1993:387. Lagen om stöd och service till visa funktionshindrade [Act concerning support and service for persons with certain functional impairment]. Stockholm: Ministry of Health and Social Affairs.
- Shrewsbury, D. 2015. “Disability and Participation in the Professions: Examples from Higher and Medical Education.” Disability & Society 30(1): 87–100. doi:10.1080/09687599.2014.982785.
- Sixsmith, J. 1986. “The Meaning of Home: An Exploratory Study of Environmental Experience.” Journal of Environmental Psychology 6(4): 281–298. doi:10.1016/S0272-4944(86)80002-0.
- Sjöström, S. 2008. “Omsorgshemmet och innebörden av begreppet hem.” In Boende och sociala sammanhang – för människor med funktionshinder. J. Paulsson, and B. Ringby Jansson, eds., 61–80. Lund: Studentlitteratur.
- Smith, S. G. 1994. “The Essential Qualities of a Home.” Journal of Environmental Psychology 14(1): 31–46. doi:10.1016/S0272-4944(05)80196-3.
- Svanelöv, E., E. Flygare Wallén, P. Enarsson, and J. Stier, Forthcoming. “‘Everybody with Disability Should be Included’: A Qualitative interview study of Athletes’ Experiences of Disability Sports Participation in Perspective of theory of able-mindedness”.
- Svanelöv, E., P. Enarsson, E. F. Wallén, and J. Stier. 2019. “Understandings of Participation in Daily Activity Services among People with Intellectual Disabilities: A Pedagogical Sociocultural Perspective.” Journal of Intellectual Disabilities 23(2): 203–215. doi:10.1177/1744629517743578.
- Talman, L. 2018. “Participation in Everyday Life for Adults with Profound Intellectual (and Multiple) Disabilities.” PhD diss., Mälardalen University.
- Talman, L., J. Wilder, J. Stier, and C. Gustafsson. 2019. “Staff Members and Managers’ Views of the Conditions for the Participation of Adults with Profound Intellectual and Multiple Disabilities.” Journal of Applied Research in Intellectual Disabilities 32(1): 143–151. doi:10.1111/jar.12516.
- The National Board of Health and Welfare. 2018. Bostad med särskild service för vuxna enligt LSS [Housing with special services for adults according to LSS]. Stockholm: The National Board of Health and Welfare.
- The Swedish Research Council. 2017. Good Research Practice. Stockholm: The Swedish Research Council.
- Tideman, M. 2000. Normalisering och kategorisering: om handikappideologi och välfärdspolitik I teori och praktik för personer med utvecklingsstörning. Lund: Studentlitteratur.
- Välikangas, A., and H. Seeck. 2011. “Exporing the Foucauldian Interpretation of Power and Subject in Organizations.” Journal of Management & Organization 17(6): 812–827. doi:10.1017/S183336720000119X.
- Winther Jörgensen, M., and L. Philips. 2000. Diskursanalys som teori och metod. Lund: Studentlitteratur.
- Wolcott, H. F. 1990. “Making a Study ‘More Ethnographic.” Journal of Contemporary Ethnography 19(1): 44–72. doi:10.1177/089124190019001003.
- Yates, S. 2005. “Truth, Power, and Ethics in Care Services for People with Learning Difficulties.” In Foucault and the Government of Disability. S. Tremain, ed., 65–77. Ann Arbor: University of Michigan Press.
