
Abstract
This study was carried out at Qassim Region, Central of Saudi Arabia, to study dermatophytosis in a private farm of dromedary camels. The prevalence of dermatophytosis in camels was 11.5% and significantly differed among different age groups (p ≤ .0001 and odds ratio = 14.61), with higher prevalence among camels younger than three years (22.10%). Clinical signs of ringworm recorded in this study were non-pruriginous dry circumscribed discrete, crusty hairless lesion distributed over the head, neck, shoulder, limbs and flanks. Mycological examination revealed Trichophyton verrucosum from the clinically diseased camels (n = 23). Significant improvement in the terms of rapid recovery was recorded in camels receiving topical application of 10% iodine ointment for three weeks in addition to intramuscular injection of vitamin A (400,000 IU/animal) on alternate days for three times and mineral mixture supplementation as dietary additives for three weeks compared to the group that was treated using iodine ointment for three weeks alone.
1. Introduction
Dermatophytosis (syn. ringworm) is a zoonotic skin infection of keratinized tissues caused by a specialized group of fungi named dermatophytes (Shams-Ghahfarokhi et al. Citation2009). The disease can affect all domestic animals (Connole Citation1990), including camels (Mancianti et al. Citation1988; Fadlelmula et al. Citation1994).
Some dermatophytes have great zoonotic importance, where many of them occurring primarily in animals and can be transmitted from infected animals to man (Nakamura et al. Citation1999).
Dermatophytes are filamentous fungi which invade keratinized tissues of humans and animals, causing mild to severe, localized and/or diffuse infections. Zoophilic and Geophilic dermatophytes infect both animals and humans, whereas anthropophilic ones are mainly found on humans (Cafarchia, Iatta, et al. Citation2013).
Taxonomically, dermatophytes comprise three closely related genera: Epidermophyton, Microsporum and Trichophyton. Microsporum and Trichophyton are represented by multiple species (Weitzman and Summerbell Citation1995).
The transmission of dermatophytosis is usually by direct contact with infected host (animals or humans) or asymptomatic carriers and/or indirect contact with infected exfoliated skin or hairs in premises and equipments (Smith Citation2002; Cafarchia, Figueredo, et al. Citation2013). Diagnosis of dermatophytosis is mainly based on clinical signs, whereas direct microscopic examination and culture of skin scraping and hairs from the periphery of lesions are necessary to confirm the clinical diagnosis (Markus et al. Citation2001). This investigation was delineated to study an outbreak of dermatophytosis in dromedary camels with emphasis on clinical, cultural and treatment.
2. Materials and methods
2.1. Animals and samples collection
Herd screening was done in 200 female camels of different age groups belonging to private farm at Qassim Region, Central of Saudi Arabia.
Skin scrapings and wool clippings were collected (before treatment and after recovery) according to Kelly (Citation1984) for mycological examination.
2.2. Epidemiological and clinical investigation
All camels under study were subjected to clinical examination. Epidemiological data were estimated according to Martin et al. (Citation1987) and clinical findings were recorded (Rosenberger Citation1979).
2.3. Mycological examination
2.3.1. Direct microscopic examination
It was done by using 20% potassium hydroxide solution for the presence of arthrospores and hyphae under a light microscope using low and high powers.
2.3.2. Mycological culture
Culture was done on Sabouraud Dextrose Agar (SDA) media with chloramphenicol and cyclohexidine. The media kept at 27°C for four weeks. The dermatophyte identification was made based on the colony characteristics and microscopic features of the fungal isolates according to the methods described by Rippon (Citation1988) and Larone (Citation1995). The culture plates were then incubated at ambient temperature (~27°C) for up to four weeks before discarding to ensure about the appearance of slow growing dermatophytes (Robert and Pihet Citation2008).
2.4. Therapeutic trials
Diseased camels were divided into two groups. Group 1 (12 camels) was treated after removal of skin crusts using topical application of 10% iodine ointment daily for three weeks, while group 2 (11 camels) was treated by the same method, but intramuscular injection of vitamin A (400,000 IU/animal) on alternate days for three times was administered along with mineral mixture supplementation as dietary additives for three weeks. Disinfection of animal housing and equipments was done in adjunct with animal treatment using 10% hypochlorite solution (Rycroft and McLay Citation1991).
2.5. Statistical analysis
Data were analysed statistically according to Snedecor and Cochran (Citation1980).
3. Results and discussion
Over the last two decades, the number of fungal and fungal-like diseases of plant and animals in both natural and controlled systems has increased, most likely as a consequence of environmental changes (Fisher et al. Citation2012).
In the present study, 200 female camels were examined clinically and mycologically for dermatophytosis, and 23 were infected representing a prevalence rate of 11.5%. Wernery and Kaaden (Citation2002) reported dermatophytosis to be a common disease of camels worldwide. Similar result was reported previously by Kuttin et al. (Citation1986). On the contrary, higher prevalence of 48% (Mahmoud Citation1993) and 43.5% (Fadlelmula et al. Citation1994) were reported in camels, whereas Gitao et al. (Citation1998) reported lower prevalence of 8.58% in camels suffering from dermatophytosis.
The disease prevalence was significantly different among different age groups (p ≤ .0001 and odds ratio = 14.61), whereas the prevalence was significantly higher (22.10%) among camels younger than three years than those (1.9%) older than three years. Similar results on age were reported by Agab (Citation1993) and Khamiev (Citation1981). The variation in the disease prevalence among different studies may be attributed to the hygienic measures applied in each farm and the immunity of the camels under study (Kuttin et al. Citation1986; Mahmoud Citation1993).
The cutaneous lesions, macroscopic and microscopic cultural findings are shown in . Infected camels showed multifocal to generalized skin lesions in the form of circumscribed discrete, crusty hairless areas distributed over the neck, shoulder, limbs and flanks. The lesions are non-pruriginous dry, with powdery scales.
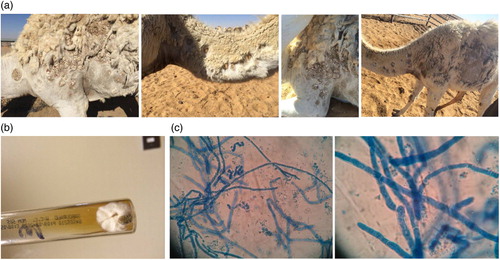
In this study, Trichophyton verrucosum was isolated and identified from all clinically diseased camels (n = 23). On SDA media, colonies were small, button or disk shaped, heaped and folded white to cream-coloured colony with no reverse pigment, with a velvety surface, raised centre and flat periphery. Microscopically, slide cultures prepared from the fungal colonies showed broad, irregular hyphae with many terminal and intercalary chlamydospores. Chlamydospores were numerous, symmetrical typically present in chains that are considered as a predominant microscopic feature of T. verrucosum and do have diagnostic value for the fungus. In the present study, T. verrucosum was isolated from both young and old camels.
T. verrucosum is the most common dermatophyte that affects camels (Abdalla and Salim Citation2010). The finding was in accordance with the finding of FadlelMula et al. (Citation1994), although Kuttin et al. (Citation1986) and Mahmoud (Citation1993) had isolated T. verrucosum from young camels and Trichophyton mentagrophytes only from old ones.
The treatment trials of dermatophytosis revealed that group 2 showed higher and rapid cure rate (cured before three weeks) compared to group 1. Similar result was recorded previously by Manefield and Tinson (Citation1997) who found that Trichophyton infection in camels was effectively treated by chlorinated or iodine-based topical treatments. Also, Radostits et al. (Citation2000) reported that supplementation of the diet with vitamin A to young housed animals should be encouraged as a preventive measure for ringworm infection.
In this study, 10% hypochlorite solution was used in the disinfection procedure (Rycroft and McLay Citation1991) since most of dermatophytes can remain viable in infected soil and premises for many years (Haggag et al. Citation1999; Nashwa Citation2001; Efuntoye and Fashanu Citation2002).
4. Conclusion
It can be concluded that ringworm is a common disease affecting young dromedary camels below three years of age and T. verrucosum is a common cause. Vitamin A and mineral supplementation besides topical application with iodine ointment enhance the recovery rate.
References
- Abdalla WG, Salim MO. 2010. Isolation and identification of Dermatophytes from infected Camels. Sudan J Vet Res. 25:94–53.
- Agab H. 1993. Epidemiology of camel diseases in eastern Sudan with emphasis on brucellosis [M.V.Sc thesis]. Khartoum (Sudan): University of Khartoum.
- Cafarchia C, Figueredo LA, Otranto D. 2013. Fungal diseases of horses. Vet Microbiol. 167:215–234. 10.1016/j.vetmic.2013.01.015
- Cafarchia C, Iatta R, Latrofa MS, Graser Y, Otranto D. 2013. Molecular epidemiology, phylogeny and evolution of dermatophytes. Inf Genet Evol. 20:336–351. 10.1016/j.meegid.2013.09.005
- Connole MD. 1990. Review of animal mycoses in Australia. Mycopathologia. 111:133–164. 10.1007/BF02282798
- Efuntoye MO, Fashanu SO. 2002. Fungi isolated from skins and pens of healthy animals in Nigeria. Mycopathologia. 153:21–23. 10.1023/A:1015207831240
- Fadlelmula A, Agab H, Le Horgne JM, Abbas B, Abdalla AE. 1994. First isolation of Trichophyton verrucosum as the aetiology of ringworm in the Sudanese camels (Camelus dromedarius). Revue d,Elevage Et De Medicine Veterinaire Des Pays Tropicaux. 47:184–187.
- Fisher MC, Henk DA, Briggs CJ, Brownstein JS, Madoff LC, McCraw SL, Gurr SJ. 2012. Emerging fungal threats to animal, plant and ecosystem health. Nature. 484:186–194. 10.1038/nature10947
- Gitao CG, Agab H, Khalifalla AG. 1998. An outbreak of a mixed infection of Dermatophilus congolensis and Microsporum gypseum in camels (Camelus dromedaríus) in Saudi Arabia Revue Scientifique Et Technique De L`Office International Des Epizooties. 17:749–755.
- Haggag Y, Draz A, Samaha H. 1999. Soil as a reservoir of certain dermatophytes and other fungi to man and animals. Alexandria J Vet Sci. 15:1–9.
- Kelly WR. 1984. Veterinary clinical diagnosis. 3rd ed. London: Bailliera Tindal.
- Khamiev S Kh. 1981. Vet Bull Vol 52 Abst 1126.
- Kuttin ES, Alhanaty E, Feldman M, Chaimovits M, Müller J. 1986. Dermatophytosis of camels. J Med Vet Mycol. 24:341–344. 10.1080/02681218680000501
- Larone DH. 1995. Medically important fungi: a guide to identification. 3rd ed. Washington (DC): ASM Press.
- Mahmoud AL. 1993. Dermatophytes and other associated fungi isolated from ringworm lesions of camels. Folia Microbiol (Praha). 38:505–508. 10.1007/BF02814404
- Mancianti F, Papini R, Cavicchio P. 1988. Dermatofizia da Microsporum gypseum in un camello (Camelus dromedarius). Ann Fac Med Vet Univ Pisa. 4:233–237.
- Manefield GW, Tinson AH. 1997. Camels: a compendium Sydney post graduate foundation vade mecum series C no. 22. Sydney : Post Graduate Foundation, Sydney University.
- Markus R, Huzaira M, Anderson RR, Gonzaliz S. 2001. A better potassium hydroxide preparation: in vivo diagnosis of tinea with confocal microscopy. Arch Dermatol. 137:1076–1078.
- Martin SW, Meek AH, Willeberg P. 1987. Veterinary epidemiology. Principles and methods. Ames (IA): Iowa State University Press.
- Nakamura Y, Watanabe S, Hasegawa A. 1999. Dermatomycosis in human and animals. Nippon Ishinkin Gakkai Zasshi. 40:9–14. 10.3314/jjmm.40.9
- Nashwa KO. 2001. Zoonotic aspect of Trichophyton mentagrophytes in rabbit farms. Beni-Suef. Vet Med J. 11:49–56.
- Radostits OM, Blood DC, Gay CC. 2000. Veterinary medicine. 9th ed. London (UK): Bailliere.
- Rippon JW. 1988. Medical mycology, the pathogenic fungi and the pathogenic actinomycetes. 3rd ed. Philadelphia: W.B.Saunders.
- Robert R, Pihet M. 2008. Conventional methods for the diagnosis of dermatophytosis. Mycopathologia. 166:295–306. 10.1007/s11046-008-9106-3
- Rosenberger G. 1979. Clinical examination of cattle. A Text Book. 3rd ed. Berlin: Pray.
- Rycroft AN, McLay C. 1991. Disinfection in the control of small animal ringworm due to Microsporum canis. Vet Rec. 129:239–241.
- Shams-Ghahfarokhi M, Mosleh-Tehrani F, Ranjbar-Bahadori S, Razzaghi-Abyaneh M. 2009. An epidemiological survey on cattle ringworm in major dairy farms of Mashhad city, Eastern Iran. Iran J Microbiol. 1:31–36.
- Smith BP. 2002. Large animal internal medicine. Diseases of horse, cattle, sheep and goats. 4th ed. St. Louis (MO): Mosby-Elsevier.
- Snedecor GW, Cochran WG. 1980. Statistical methods. 8th ed. Ames (IA): The Iowa State, University Press.
- Weitzman I, Summerbell RC. 1995. The dermatophytes. Clin Microbiol Review. 8:240–259.
- Wernery U, Kaaden OR. 2002. Infectious diseases of camelids. Berlin: Blackwell Science.