
Abstract
The allostatic load index (ALI) assesses the physiological adaption to chronic stress by cumulative changes in the circulation, respiration, inflammation, metabolic and anthropometric systems. The ALI thus can function as a risk marker for secondary prevention in occupational medicine. The aim of this study was to investigate the feasibility of creating a predictive marker by using data from an executive checkup program of an international company and to examine its relationship to work-related surrogate health parameters.
Datasets from 307 examinations of 151 executives (19 males and 132 females) were available. Each participant attended at least one checkup examination between 2003 and 2015. The mean age was 43.6 (SD ±6.6, 31–64y). We developed four different ALIs with different biomarkers of the cardio-vascular, immune, metabolic and anthropometric systems. As a primary mediator, the thyroid-stimulating hormone was used as a proxy. For each ALI, the associations with the work ability index (WAI) and categories of sick leave days (SLD) were examined. Zero inflation was considered for SLD.
One ALI showed a significant negative association with the WAI (B = −0.680, SE =0.266, p = .049). The results of a second ALI had a similar trend (B= −0.355, SE =0.201, p = .081). After adjustment for zero inflation two other ALIs showed a positive association with SLD.
This study provides the first hints that biomarkers form a secondary prevention program are useful in calculating a meaningful ALI. Thus, the concept of allostatic load could be used in workplace health-promotion.
Lay Summary
This study provides the first hints that biomarkers from a secondary prevention program are useful for calculating a meaningful ALI. To the best of our knowledge, this study is the first which examines ALI in relation to its predictive value and preventive potential. The results revealed, that the concept of allostatic load could be beneficial in workplace health-promotion.
Introduction
In many countries and several industry sectors different occupational health checkup (OHC) examinations are prescribed by law (Regulation for occupational provision, Citation2013; European Agency for Safety and Health at Work, Citation2017) and commonly used as tools to determine workers state of health in relation to their job task. Secondary preventive activities are based on markers, which were created from the obtained data. The medical nature and extent of the OHC differ according to the respective job task of the employees. However, several routine data like blood pressure, heart rate, and body mass index (BMI) are collected at every checkup during medical examination. Even a blood sample for medical laboratory analysis is often part of the OHC. In cases when the measured parameters are outside of the normal range, the occupational physician takes action and advises the employee to seek special medical consultation. The clinically irrelevant data is not considered further.
In the literature, there is growing evidence that stress and stress-related diseases have a significant impact on productivity (Goetzel et al., Citation2009; Schwatka et al., Citation2017) and general absence from work due to sickness (Mauss, Jarczok, & Fischer, Citation2016; Melchior et al., Citation2005; Michie & Williams, Citation2003; Zalli et al., Citation2014). However, psychological measures of stress like the perceived stress scale (Cohen, Kamarck, & Mermelstein Citation1983) or the Trier Inventory for the Assessment of Chronic Stress (TICS; Schulz, Schlotz, & Becker, Citation2004) and stress-related early warning indicators like the irritation scale (Mohr, Rigotti, & Muller, Citation2005), are usually not part of an OHC. Similarly, biological assessments of stress indicators like the allostatic load concept are rarely considered in an OHC.
The concepts of allostasis (Sterling & Eyer, Citation1988) and allostatic load (AL) (McEwen, Citation1998; McEwen and Norton Lasley, Citation2001; McEwen and Stellar, Citation1993) provide a framework for preventively assessing the effects of chronic or repetitive stress on worker health and make use of all assessed screening data.
By considering changes in biomarkers that are still within normal ranges, an early detection indicator, leading to preventive action needs, can be realized.
AL is the hypothalamic-pituitary-adrenal (HPA) axis mediated response of the body to chronic stress and the inability to bring down the level of stress back to a pre-stressor level (McEwen and Norton Lasley, Citation2001). The AL index (ALI) (Seeman, McEwen, Rowe, & Singer, 2001) originally contained primary mediators and secondary outcomes. Primary mediators are for example cortisol, dehydroepiandrosterone-sulfate (DHEA-S), epinephrine, and norepinephrine, which are directly influenced by the constantly upregulated HPA axis.
A secondary outcomes is, for example, elevated diastolic blood pressure at rest, which represents the wear and tear of the body due to the elevated primary mediators, which require a bodily adaptation to confront the stressors. Therefore, including the concept of allostatic load in an OHC may be an effective indicator for the early prevention of stress-related diseases, since according to McEwen (Citation1998), the assessment of multiple biomarkers even in the subclinical domain may be an indicator for the risk of the onset of later tertiary outcomes (i.e. diabetes, coronary heart disease, etc.).
Corresponding research has shown that work-related stress is associated with an increased allostatic load in various areas of work, such as public administration in Denmark (Carlsson, Hansen, Nielsen, Blond, & Netterstrom, Citation2017), health care in Egypt (Ali, Badawy, Rizk, Gomaa, & Saleh, Citation2016) and Sweden (Hasson, Von Thiele Schwarz, & Lindfors, Citation2009), teaching (female teachers) in Germany and Luxembourg (Bellingrath, Weigl, & Kudielka, Citation2009) or the IT sector in Sweden (Hasson et al., Citation2009). Coronado, Chandola, and Steptoe (Citation2018) showed a correlation for AL and effort-reward imbalance in a longitudinal study of workers over 50 y.
In another study, Juster et al. (Citation2011) found that workers exhibit a positive link between AL and chronic stress or burnout, but not with depression. All these results show that AL is a good and tailored tool for measuring stress outcomes at work. The next step in the application of AL would be to test, whether its use as a predictive screening instrument is possible and meaningful.
The present study is intended to investigate this and test the hypothesis in an occupational health context. Since the stress response requires a broad bodily adaptation, past research has included biomarkers from different response areas of the ALI: Neuroendocrine, Immune, Anthropometric, Cardiovascular, Respiratory, and Metabolic (Juster, McEwen, & Lupien, Citation2010). One challenge in applying AL in an OHC is in obtaining the primary mediators of AL for the HPA axis like cortisol, epinephrine, norepinephrine, dopamine or DHEA-S within routine data. Juster et al. (2010) have shown many examples in their review, of how to build an ALI without primary mediators, and to still come to conclusive results. Mauss, Li, Schmidt, Angerer, and Jarczok (Citation2015) decided for their literature review that the inclusion of at least one primary mediator should be a quality criterion, but even studies not reaching that goal showed evidence of the relation between occupational stress and ALI (Li, Zhang, Sun, Ke, Dong, & Wang, Citation2007; Li et al., Citation2007 Naswall, Lindfors, & Sverke, Citation2012).
In order to reach a compromise between a comprehensive allostatic load assessment and an applied setting, including parameters of thyroid function, which are more likely to be assessed in health checkups, can be considered. In fact, there is evidence that acute stress exposure has a direct influence on the secretion of thyroid stimulating hormone (TSH; MacLean et al., Citation1994). Similar to the control loop for cortisol, the output of the control loop for TSH is located in the hypothalamus. The respective releasing hormones cause on the one hand the release of the adrenocorticotropic hormone (ACTH) in the pituitary gland, which then controls the production of cortisol in the adrenal cortex and on the other hand the release of TSH in the pituitary gland, which then influences the thyroid metabolism. A connection between cortisol and TSH has already been described by Iranmanesh, Lizarralde, Johnson, and Veldhuis (1990). In a recent study in young healthy adults, Walter et al. (Citation2012) confirmed the positive association of TSH and cortisol, even in subclinical hypothyroidism. The authors identify hypothyroidism as being responsible for elevated cortisol levels, due to a decreased clearance and a reduced negative feedback of cortisol on the HPA. Thus, for the purpose of the present study the inclusion of TSH as a proxy for a primary stress mediator seems promising.
The aim of this study was to examine the feasibility of creating a summative preventive marker employing the concept of ALI by using routinely collected data from an OHC program for executives of an international corporate group. Within the group of executives, we want to examine the relationship between their ALIs and health-related outcomes (i.e. sick leave days) and self-reported work ability.
Materials and methods
Participants and procedure
The program started in 2003 and is still ongoing. The target audience of the program are executive managers of a global operating company. The available dataset included 307 examinations of 151 participants (19 female, 132 male) who attended at least one OHC by 2015. The total number of executives in the company was 4300, out of which 10% were women. Thus, a participation rate of 12.6% female executives in our study corresponds to the overall gender distribution in the company. The age of participants at their first examination was between 31 and 64 y (mean: 43.6; SD ±6.6) and 7.9% of the executives were smokers. Seven datasets were excluded from further analysis due to missing values in the relevant parameters. Two other datasets were excluded since the timespan between two examinations was too small (i.e. less than one year). Sixty nine of the executives only participated in the program one time, 82 participated repeatedly. For further details see .
Table 1. Descriptive data of cohort, work ability index, and categories of sick leave days.
Executives were invited to attend the OHC by the company’s medical office and the OHC examinations were conducted by the companies occupational physicians. Written informed consent was obtained from each participant before taking part in the OHC and they were informed in regards to the scientific investigation and publication of the data. The health check consisted of an extensive medical history and physical examinations, including the assessment of anthropometric parameters such as BMI and body fat analyses, as well as an interview to assess the criterion variables with validated scales regarding health and work ability of the executives.
Survey measure/outcome parameters
To assess work ability, the work ability index (WAI) questionnaire was used (Tuomi et al., Citation1994). It consists of 10 questions and a diagnostic list, which are summarized in seven dimensions. In detail, these are:
Current ability to work compared to the lifetime best.
Ability to work in relation to the requirements of the activity.
Number of diseases currently diagnosed by a physician.
Estimated impairment of work performance due to these diseases.
Number of sick leave days in the last 12 months.
Mental resources.
An evaluation scheme and a classification of the resulting index value are freely available on the website of the Federal Institute for Occupational Safety and Health (Citation2018). At the beginning of the questionnaire, it is recorded whether the participant’s work is predominantly mental, physical, or both to the same extent. The current work ability in comparison to the best ever achieved is evaluated with an interval scale. The ability to work in relation to the requirements is recorded with one question in relation to the physical and one to the psychological requirements. The respective scores were then weighted according to the predominant type of activity. The area of diagnosed diseases is subdivided into accident injuries, musculoskeletal disorders, cardiovascular diseases, respiratory diseases, mental disorders, neurological and sensory disorders, digestive system disorders, sexually transmissible diseases and urinary tract disorders, skin diseases, tumors, hormonal and metabolic disorders, blood diseases, birth defects and other diseases. The participants could indicate whether the diagnosis was made by a physician or by themselves.
The dimension of psychological performance reserves was measured by the questions of whether the participants have recently completed their daily tasks with joy, whether they have been active and lively in recent times and whether they are currently looking to the future with confidence.
The assessment of one's own ability to work in the next two years could be judged as unlikely, not sure or fairly certain.
Finally, as one part of the WAI assessment “sick leave days” in the last 12 months could be reported in the categories none, 1–9 days, 10–24 days, 25–99 days and 100–365 days.
The WAI is calculated as the total sum of the individual points from the seven different work ability dimensions described above. A score between seven and 21 points is considered critical and it is recommended to take steps to restore the ability to work. If the index is between 28 and 36 points, it is recommended to introduce actions for improvement. Between 37 and 43 points, the ability to work is rated as "good" and it is recommended to offer support activities. In the range of 44–49 points the ability to work is very good and it is recommended to focus on its preservation.
Health examinations
To assess a respiratory parameter for the ALI we assessed the forced expiratory volume in 1 s (FEV1) with a spirometry and a spiro-ergometry, which was also part of the OHC. The device used was a CARDIOVIT AT-104 PC (Schiller, Switzerland).
In the context of spiro-ergometry, heart rate, blood pressure, and the relative physiological working capacity at 150 watts (PWCrel150) were also recorded to assess the cardiovascular parameters.
Laboratory examinations
For the assessment of a primary mediator, immune, and metabolic parameters, non-fasting blood samples were taken for the following laboratory parameters: TSH as a proxy for a primary mediator. C-reactive protein, leukocytes were detected as immune parameters, triglycerides, cholesterol, high and low density lipoproteins, homocysteine, creatinine and glycosylated hemoglobin (HbA1c) as metabolic parameters. All laboratory analyses were conducted by a commercial laboratory provider (Laboratory Schottdorf, Citation2018).
Development of the ALI
All described ALI parameters were z-standardized by using the respective function integrated in SPSS (IBM-Corporation, Citation2015,Version 25): The values of the individual variables where transformed in a way that the resulting variable had the expectancy value of zero and the variance one. The standard deviation (SD) is the root of the variance and was therefore equal to one, too. After transformation, the variance of all measured values was determined and stored.
In the next step, it was then determined for each variable whether an upward or downward change or both would be relevant as a secondary outcome parameter. After transformation, the variance of all measured values was determined and stored. The variables HbA1c, heart rate, systolic, and diastolic blood pressure were each scored with one ALI point at more than one SD above the mean. The same applied to the laboratory parameters C-reactive protein (CRP), leukocytes, homocysteine, creatinine, triglycerides, high-density lipoproteins (HDL) and total cholesterol. The FEV1 and PWCrel150 were rated with one at more than one SD below the mean. BMI, TSH, and body fat were rated one at more than one SD above and below the mean.
Based on the review of Juster et al. (Citation2010), we decided to use at least one secondary outcome parameter from the cardiovascular, respiratory, immune, metabolic, and anthropometric system to form an index for the calculation of different ALI. Overall, we created four different ALIs. The detailed compositions of the ALIs are shown in .
Table 2. ALI composition.
Overall, three cardiovascular and three metabolic parameters were used, so that the number of variables with 10 was equal to that of the original ALI (Seeman et al., Citation2001). The sum of all variables led to the particular ALI score.
As can be seen from the , the available N-size differs considerably between each ALI for practical reasons. The analysis of HbA1c was not integrated in the OHC before 2013. Thus, for HbA1c, longitudinal data was missing. The main difference between ALI 1 and 2 and ALI 3 to 4 is the use of HbA1c in ALI 3 and 4 in the metabolic cluster.
In addition, results of CRP were not available for all participants, hence leucocytes for the immune cluster in most of the ALIs was referred to. In the anthropometric cluster, BMI or body fat percentage were selected as anthropometric values. As cardiovascular parameters, diastolic blood pressure and heart rate were used for all ALIs, as well as the cholesterol/HDL quotient in the metabolic cluster. In addition, systolic blood pressure and PWCrel150 were used for cardiovascular applications, while homocysteine, creatinine, and triglycerides were used for metabolism.
Statistical analysis
First, a descriptive analysis of the available data was conducted. Secondly, mixed models were built to examine a possible association between the different ALIs and the dependent variables. Additionally, the first two ALI models included a slope term to handle the effects of repeated measurements. The examinations of ALI 3 and 4 were cross-sectional analyses due to the missing repetition of HbA1c measurement. All models included the individual as a random factor. Each model was adjusted for age, sex, and smoking (yes/no).
For the regression on the WAI, a linear model was used. When the category of sick leave days was the criterion, a zero-inflation poisson-regression model was used, because an unproportioned number of executives reported no sick-leave days at all. A longitudinal mixed model analysis failed due to the very heterogeneous participation frequency and the wide range of time lags between the follow ups (1–9 y). All analyses were conducted by using the programs SPSS (Version 25);) and R 3.3.3 (R Development Core Team, Citation2016).
Results
shows the number of available measures for each biomarker and the results of the unstandardized biomarkers. The maximum values showed that pathological values were obtained (e.g. for diastolic blood pressure or CRP) but mean and SD indicated, that only a few of the results of each biomarker were above or below the reference values. The number of parameters which were valued with one to build the particular ALI is shown in . The highest ALI was shown for ALI 2 and 3 with a score of six out of 10. The mean scores and SDs of the ALI were 0.95 (1.04) for ALI 1, 1.15 (1.19) for ALI 2, 1.31 (1.16) for ALI 3, and 1.16 (1.12) for ALI 4 1. Descriptive data for the ALIs are shown in . The reported results from the WAI ranged from a minimum score of 13 up to a maximum score of 49. The mean score was 44.5 with a SD of 3.9.
Table 3. Measures of biomarkers.
Table 4. Number of items of ALI more than one SD above or below Z.
The results of the SLD are shown in . It is important to note that 36.9% of the participants reported sick leave days at category 3 (10–24 days last year) but only 2.4% at category 1 (1–3 days).
The cross-sectional analysis using the mixed model showed a significant negative association between ALI 1 and the WAI (B = − 0.697; p = .03) and a trend for ALI 2 and WAI (B = − 0.356; p = .08).
For ALI 3 and 4 the zero-inflation poisson-regression models showed significant results for both ALI and the categories of sick leave days with respect to the zero-inflation effects (ALI 3 B = 0.698; p = .008 and ALI 4 B = 0.597; p = .019). This means, that there was no detectable linear association between the ALI and the increasing categories, but there was a detectable significant difference in the ALI between the group of participants with no sick leave days and those with some sick leave days (see and ). Outliers were present, as can be seen in Figure1, but they would rather attenuate the found effect if they affect it at all. Therefore, a separate handling of the outliers was not carried out.
Figure 1. Mean of allostatic load index (ALI) three in the categories of sick leave days (SLD) without category 0 (no SLD) with respect to the zero inflation. Categories of SLD: 1 = 1–9 days; 2 = 10–24 days; 5 = 25–99 days; 6 = 100+ days. ° = outliers; box = interquartile range (IQR 25–75%), whiskers = 95% confidence interval (CI95) and missing whiskers = >IQR = CI 95.
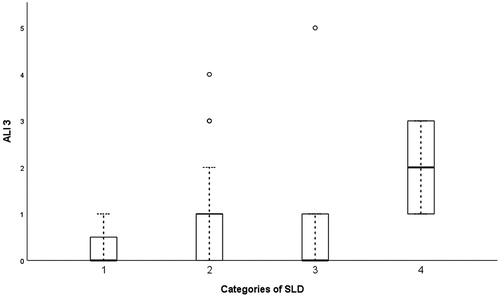
Table 5. Generalized mixed model analysis.
Discussion
The results of the present study have shown that it is possible to generate an allostatic load index with data collected in the course of an occupational health examination. It was found, that an ALI may have a predictive value in terms of perceived work ability and self-reported absenteeism (Marcatto et al., Citation2016; Stephan, Sutin, Luchetti, & Terracciano, Citation2016). Both are often the result of work-related stress and lead to a loss of productivity on the one hand and physical and mental health impairments on the other hand.
The integration of the recording of an ALI as part of occupational health examinations can be used by the occupational physician to take preventive action and to introduce procedures to reduce work-related stress before it leads to a reduction of the ability to work or to diseases.
The relation between ALI 1 and WAI and the significant zero inflation results for ALI 3 and 4 on SLD indicate that the selected mediators and outcomes for the different cluster of the ALI are important. ALI 1 is the only ALI containing CRP (due to the large number of missing CRP-values) and ALI 3 and 4 contain the HbA1c in contrast to ALI 1 and 2. CRP-levels in the upper normal range are well known as a promotor for the development of cardiovascular diseases (Kaptoge et al., Citation2012) or stroke (Rost et al., Citation2001). HbA1c seems to play a similar role in the development of dementia (Ramirez et al., Citation2015), chronic kidney,cardiovascular diseases (Hernandez et al., Citation2013) and type 2 Diabetes mellitus. Thus, for further studies, which rely on routine data of OHCs, choosing CRP as the representative of the inflammation cluster should be taken into consideration,
One notable aspect of the present study was the distinct composition of the ALI compared to the original ALI by McEwen (Citation1998), especially regarding the selection of the primary mediator parameter. The use of TSH as the primary mediator was due to the fact, that primary neurophysiological mediators like cortisol or norepinephrine are not routine values in secondary prevention. However, with our approach, we obtained significant associations with the outcome variables. The use of an endocrine parameter such as TSH, which is also linked to the HPA axis (Iranmanesh et al., Citation1990; Walter et al., Citation2012), seems to be a possible alternative.
Effect parameters of other studies (Karlamangla et al., Citation2002; Seplaki, Goldman, Glei, & Weinstein, Citation2005) are therefore comparable to the results of this study.
Nevertheless, DHEA-S could be monitored in blood analysis since it is not affected in the same way by a circadian rhythm as cortisol (Zhao et al., Citation2003). Other neurophysiological primary mediators like epinephrine, norepinephrine, aldosterone, or prolactin are comparably expensive, but more difficult to access. Twenty four hour urine collection or standardized conditions at exactly the same time of day are not easy to implement in OHC settings. So the inclusion of DHEAS in future studies should be considered, as well.
According to Juster et al. (Citation2010), other studies used peak expiratory flow (PEF) instead of FEV1 to represent the cluster of respiration in calculating an ALI. Unfortunately, the more frequently used PEF parameter was available only for 171 and FEV1 for 297 of 307 data sets, respectively. PEF measures the maximum expiratory gas flow while FEV1 measures the maximum expiratory volume in one second. The amount of gas exhaled in one second (FEV 1) is directly dependent on the maximum gas flow (PEF) so that both measures are closely related. Relying on FEV1 as a respiratory outcome for the present study lead to significant results.
Within the cardiovascular and metabolic system, we relied on different parameters to replicate the original 10-parameter ALI. Taking economic efficiency into account, subsequent studies on larger cohorts should also examine whether a composition of an ALI, e.g. one parameter per cluster, can still lead to valid results. The aim would be to detect which parameter contains the most predictive health value.
When interpreting the results of the present study one has to keep in mind that this was a highly selective study group, which would be expected to be well adapted to dealing with stress. All participants were managers of an international company. It is well known, that health and health-related behavior is affected by socio-economic status (Smith, Citation1999) and by the kind of employment (Karasek et al., Citation1988). As the data showed, 52.8% of the participants had no SLD in the past year before the examination. Thus, an additional healthy “manager” effect could be assumed, because only people with well-functioning strategies in handling job-related stress typically reach such a career level.
On the other hand, the high number of participants without any sick leave days could be an indicator of presentism during sickness (Roelen & Groothoff, Citation2010). To foster the preventive nature of the assessment, future studies should add more preventive outcome measures like presentism as a relevant measure for the organization, since presentism, just as absenteeism, could be associated with economic loss (Wada et al., Citation2013).
The relatively low number of female study participants is also due to the chosen occupational group. In national and international companies, women in leadership positions are clearly in the minority. In the present case, the proportion of female executives in the basic population is 10% (430 out of 4300). All 4300 executives were offered the opportunity to participate in the OHC. The proportion of women in the study population of 12.6% is therefore considered to be representative for the basic population. Nevertheless, the prevalence for specific tertiary outcomes like coronary heart diseases are different for men and women (Maas & Appelman, Citation2010). Further studies, which might be conducted in the general workforce, should consider potential gender differences for specific secondary and tertiary outcomes and evaluate the applicability of the selected ALI mediators also for women.
As a study limitation the assessment of the second outcome criterion of SLD needs to be discussed. SLD were present as a categorical variable and not, as with the WAI, as a continuous variable. First of all, the ranges within each category were rather large. This made a more determined analysis of this variable in the aftermath impossible and also potentially underestimates its true effect. In combination with repeated measurements, the choice of available statistical procedures for mixed effects models, which could handle this combination was very limited.
For ALI 3 and 4 (without repeated measurement due to HbA1c) a zero-inflation model was used and a poisson-distribution was assumed. The data for ALI 1 and 2 additionally contained repeated measures. This led us to a statistical procedure, which provides a zero inflated poisson regression and provides the opportunity to include a random and a slope term. But unfortunately, the procedure displays only the estimate for the general zero inflation of the model. For this reason, a significant zero inflation effect as for ALI 3 and 4 could not be provided.
Another shortcoming due to the applied setting was that the time span between two follow-ups of a participant varied between 1–9 y. The mean time lag was three years (SD = 1.6). In combination with the available outcome criteria, which referred to a timeslot of one year, a longitudinal effect over time could not be obtained. For further investigations, the outcome variable should be selected due to the possibility of longitudinal analyses and to the usability of parametric statistical procedures.
Conclusions
This feasibility study provided the first hints, that it could be possible to derive a valuable ALI from OHC routine data. In this study, an ALI with the items TSH, diastolic blood pressure, heart rate, relative physiological work capacity at 150 watts, FEV 1, CRP, cholesterol-HDL quotient, homocysteine, creatinine and BMI found the best predictive value for self-reported work-ability. A second index with the items TSH, diastolic blood pressure, heart rate, systolic blood pressure, FEV 1, leukocytes, cholesterol-HDL quotient, HbA1c, triglycerides and BMI showed a certain predictive value in relation to the category of sick leave days. The study has shown that more and prospectively planned research is recommended. If the above discussed issues will be considered it might be possible that an ALI derived from routine data could become a standard tool in occupational health prevention.
Ethical aspects
The present manuscript is based on a post-hoc analysis of data from a routine occupational health checkup program. The data was completely anonymized before it was given to the researchers. Due to these facts, no ethics committee was involved. All procedures of the study were in accordance with the Helsinki Declaration as revised in 2008. Written consent was obtained from each participant before joining the OHC and they were informed regarding the scientific investigation and publication of the data.
Disclosure statement
The authors declare that there is no conflict of interest. This study was not third party funded.
References
- Ali, O.S., Badawy, N., Rizk, S., Gomaa, H., & Saleh, M.S. (2016). Allostatic load assessment for early detection of stress in the workplace in Egypt. Open Access Macedonian Journal of Medical Sciences, 4, 493–498. doi:10.3889/oamjms.2016.066
- Federal Institute for Occupational Safety and Health. (2018). Initiative neue Qualität der Arbeit [New quality of work initiative]. Berlin, Germany: Federal Institute for Occupational Safety and Health, BAUA.
- Bellingrath, S., Weigl, T., & Kudielka, B.M. (2009). Chronic work stress and exhaustion is associated with higher allostastic load in female school teachers. Stress (Amsterdam, Netherlands), 12, 37–48. doi:10.1080/10253890802042041
- Carlsson, R.H., Hansen, A.M., Nielsen, M.L., Blond, M., & Netterstrom, B. (2017). Changes in allostatic load during workplace reorganization. Journal of Psychosomatic Research, 103, 34–41. doi:10.1016/j.jpsychores.2017.09.015
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. doi:10.2307/2136404
- Coronado, J.I.C., Chandola, T., & Steptoe, A. (2018). Allostatic load and effort-reward imbalance: Associations over the working-career. International Journal of Environmental Research and Public Health, 15, 191. doi:10.3390/ijerph15020191
- European Agency for Safety and Health at Work. (2017). Legislation - EU directives, standards guidelines and national legislation 2017. Retrieved from https://osha.europa.eu/en/safety-and-health-legislation/national-legislation-safety-and-health-work
- Regulation for occupational provision. (2013). Bundesgesundheitsblatt I p. 2768. Federal ministry for labor and social issues of Germany. Bonn; last amended by article 1 of the regulation of 23 October 2013. Bundesgesundheitsblatt I. p. 3882. Retrieved from https://www.juris.de/purl/gesetze/_ges/ArbMedVV
- Goetzel, R.Z., Carls, G.S., Wang, S., Kelly, E., Mauceri, E., Columbus, D., & Cavuoti, A. (2009). The relationship between modifiable health risk factors and medical expenditures, absenteeism, short-term disability, and presenteeism among employees at novartis. Journal of Occupational and Environmental Medicine/American College of Occupational and Environmental Medicine, 51, 487–499. doi:10.1097/JOM.0b013e31819eb902
- Hasson, D., Von Thiele Schwarz, U., & Lindfors, P. (2009). Self-rated health and allostatic load in women working in two occupational sectors. Journal of Health Psychology, 14, 568–577. doi:10.1177/1359105309103576
- Hernandez, D., Espejo-Gil, A., Bernal-Lopez, M.R., Mancera-Romero, J., Baca-Osorio, A.J., Tinahones, F.J., … Gomez-Huelgas, R. (2013). Association of HbA1c and cardiovascular and renal disease in an adult Mediterranean population. BMC Nephrology, 14, 151. doi:10.1186/1471-2369-14-151
- IBM-Corporation. (2015). IBM SPSS V23 Statistics for Windows (Version 4.0) [Computer software]. Armonk, NY.
- Iranmanesh, A., Lizarralde, G., Johnson, M.L., & Veldhuis, J.D. (1990). Dynamics of 24-hour endogenous cortisol secretion and clearance in primary hypothyroidism assessed before and after partial thyroid hormone replacement. The Journal of Clinical Endocrinology and Metabolism, 70, 155–161. doi:10.1210/jcem-70-1-155
- Juster, R.P., McEwen, B.S., & Lupien, S.J. (2010). Allostatic load biomarkers of chronic stress and impact on health and cognition. Neuroscience and Biobehavioral Reviews, 35, 2–16. doi:10.1016/j.neubiorev.2009.10.002
- Juster, R.P., Sindi, S., Marin, M.F., Perna, A., Hashemi, A., Pruessner, J.C., & Lupien, S.J. (2011). A clinical allostatic load index is associated with burnout symptoms and hypocortisolemic profiles in healthy workers. Psychoneuroendocrinology, 36, 797–805. doi:10.1016/j.psyneuen.2010.11.001
- Kaptoge, S., Di Angelantonio, E., Pennells, L., Wood, A.M., White, I.R., Gao, P., … Danesh, J. (2012). C-reactive protein, fibrinogen, and cardiovascular disease prediction. The New England Journal of Medicine, 367, 1310–1320. doi:10.1056/NEJMoa1107477
- Karasek, R.A., Theorell, T., Schwartz, J.E., Schnall, P.L., Pieper, C.F., & Michela, J.L. (1988). Job characteristics in relation to the prevalence of myocardial infarction in the US Health Examination Survey (HES) and the Health and Nutrition Examination Survey (HANES). American Journal of Public Health, 78, 910–918. doi:10.2105/AJPH.78.8.910
- Karlamangla, A.S., Singer, B.H., McEwen, B.S., Rowe, J.W., & Seeman, T.E. (2002). Allostatic load as a predictor of functional decline. MacArthur studies of successful aging. Journal of Clinical Epidemiology, 55, 696–710. doi:10.1016/S0895-4356(02)00399-2
- Laboratory Schottdorf MVZ GmbH. (2018). Analysis meethods. Augsburg, Germany. Retrieved from http://www.schottdorf.de/leistungen/pdf_lv/untersuchungen_alphabetisch.pdflin
- Li, W., Zhang, J.-Q., Sun, J., Ke, J.-H., Dong, Z.-Y., & Wang, S. (2007). Job stress related to glyco-lipid allostatic load, adiponectin and visfatin. Stress and Health, 23, 257. doi:10.1002/smi.1145
- Li, W., Zhang, J.-Q., Wang, S, et al (2007). Relationship between job stress and allostatic load. China Occupational Medicine, 3, 4.
- Maas, A., & Appelman, Y.E.A. (2010). Gender differences in coronary heart disease. Netherlands Heart Journal: Monthly Journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation, 18, 598–602. doi:10.1007/s12471-010-0841-y
- MacLean, C.R., Walton, K.G., Wenneberg, S.R., Levitsky, D.K., Mandarino, J.V., Waziri, R., & Schneider, R.H. (1994). Altered responses of cortisol, GH, TSH and testosterone to acute stress after four months' practice of transcendental meditation (TM). Annals of the New York Academy of Sciences, 746, 381–384. doi:10.1111/j.1749-6632.1994.tb39261.x
- Marcatto, F., Colautti, L., Larese Filon, F., Luis, O., Di Blas, L., Cavallero, C., & Ferrante, D. (2016). Work-related stress risk factors and health outcomes in public sector employees. Safety Science, 89, 274–278. doi:10.1016/j.ssci.2016.07.003
- Mauss, D., Jarczok, M.N., & Fischer, J.E. (2016). The streamlined allostatic load index: A replication of study results. Stress, 20, 553–558. doi:10.1080/10253890.2016.1219718
- Mauss, D., Li, J., Schmidt, B., Angerer, P., & Jarczok, M.N. (2015). Measuring allostatic load in the workforce: A systematic review. Industrial Health, 53, 5–20. doi:10.2486/indhealth.2014-0122
- McEwen, B., & Norton Lasley, E. (2001). The end of stress as we know it. Washington D.C: Joseph Henry Press.
- McEwen, B.S. (1998). Protective and damaging effects of stress mediators. The New England Journal of Medicine, 338, 171–179. doi:10.1056/NEJM199801153380307
- McEwen, B.S., & Stellar, E. (1993). Stress and the individual. Mechanisms leading to disease. Archives of Internal Medicine, 153, 2093–2101. doi:10.1001/archinte.1993.00410180039004
- Melchior, M., Krieger, N., Kawachi, I., Berkman, L.F., Niedhammer, I., & Goldberg, M. (2005). Work factors and occupational class disparities in sickness absence: Findings from the GAZEL cohort study. American Journal of Public Health, 95, 1206–1212. doi:10.2105/AJPH.2004.048835
- Michie, S., & Williams, S. (2003). Reducing work related psychological ill health and sickness absence: a systematic literature review. Occupational and Environmental Medicine, 60, 3–9. doi:10.1136/oem.60.1.3
- Mohr, G., Rigotti, T., & Muller, A. (2005). Irritation - An instrument assessing mental strain in working contexts. Scale and item parameters from 15 studies. Zeitschrift für Arbeits- und Organisationspsychologie, 49, 44–48. doi:10.1026/0932-4089.49.1.44
- Naswall, K., Lindfors, P., & Sverke, M. (2012). Job insecurity as a predictor of physiological indicators of health in healthy working women: An extension of previous research. Stress and Health, 28, 255–263. doi:10.1002/smi.1430
- R Development Core Team. (2016). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing.
- Ramirez, A., Wolfsgruber, S., Lange, C., Kaduszkiewicz, H., Weyerer, S., Werle, J., … Scherer, M. (2015). Elevated HbA1c is associated with increased risk of incident dementia in primary care patients. Journal of Alzheimer's Disease, 44, 1203–1212. doi:10.3233/JAD-141521
- Roelen, C.A., & Groothoff, J.W. (2010). Rigorous management of sickness absence provokes sickness presenteeism. Occupational Medicine (Oxford, England), 60, 244–246. doi:10.1093/occmed/kqq010
- Rost, N.S., Wolf, P.A., Kase, C.S., Kelly-Hayes, M., Silbershatz, H., Massaro, J.M., … Wilson, P.W. (2001). Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: the Framingham study. Stroke, 32, 2575–2579. doi:10.1161/hs1101.098151
- Schulz, P., Schlotz, W., & Becker, P. 2004. Trierer Inventar zum chronischen Stress. Göttingen Bern Toronto Seattle: Hogrefe Verlag.
- Schwatka, N.V., Atherly, A., Dally, M.J., Fang, H., V, S.B.C., Tenney, L., … Newman, L.S. (2017). Health risk factors as predictors of workers' compensation claim occurrence and cost. Occupational and Environmental Medicine.74, 14–23. doi:10.1136/oemed-2015-103334
- Seeman, T.E., McEwen, B.S., Rowe, J.W., & Singer, B.H. (2001). Allostatic load as a marker of cumulative biological risk: MacArthur studies of successful aging. Proceedings of the National Academy of Sciences of the United States of America, 98, 4770–4775. doi:10.1073/pnas.081072698
- Seplaki, C.L., Goldman, N., Glei, D., & Weinstein, M. (2005). A comparative analysis of measurement approaches for physiological dysregulation in an older population. Experimental Gerontology, 40, 438–449. doi: 10.1016/j.exger.2005.03.002
- Smith, J.P. (1999). Healthy bodies and thick wallets: The dual relation between health and economic status. Journal of Economic Perspectives, 13, 145–166. doi: 10.1257/jep.13.2.145
- Stephan, Y., Sutin, A.R., Luchetti, M., & Terracciano, A. (2016). Allostatic load and personality: A 4-year longitudinal study. Psychosomatic Medicine, 78, 302–310. doi:10.1097/PSY.0000000000000281
- Sterling, P., & Eyer, J. 1988. Allostasis: A new paradigm to explain arousal pathology. In: S. Fisher & J. Reason (Eds.), Handbook of life stress, cognition and health (pp. 629–649). New York: John Wiley & Sons.
- Tuomi, K., Ilmarinen, J., Jahkola, A., Katajarinne, L., & Tulkki, A. (1994). Work ability index. Helsinki: Institute of Occupational Health.
- Wada, K., Arakida, M., Watanabe, R., Negishi, M., Sato, J., & Tsutsumi, A. (2013). The economic impact of loss of performance due to absenteeism and presenteeism caused by depressive symptoms and comorbid health conditions among Japanese workers. Industrial Health, 51, 482–489. doi:10.2486/indhealth.2013-0016
- Walter, K.N., Corwin, E.J., Ulbrecht, J., Demers, L.M., Bennett, J.M., Whetzel, C.A., & Klein, L.C. (2012). Elevated thyroid stimulating hormone is associated with elevated cortisol in healthy young men and women. Thyroid Research, 5, 13. doi:10.1186/1756-6614-5-13
- Zalli, A., Carvalho, L.A., Lin, J., Hamer, M., Erusalimsky, J.D., Blackburn, E.H., & Steptoe, A. (2014). Shorter telomeres with high telomerase activity are associated with raised allostatic load and impoverished psychosocial resources. Proceedings of the National Academy of Sciences of the United States of America, 111, 4519–4524. doi:10.1073/pnas.1322145111
- Zhao, Z.Y., Xie, Y., Fu, Y.R., Li, Y.Y., Bogdan, A., & Touitou, Y. (2003). Circadian rhythm characteristics of serum cortisol and dehydroepiandrosterone sulfate in healthy Chinese men aged 30 to 60 years. A cross-sectional study. Steroids, 68, 133–138. doi:10.1016/S0039-128X(02)00167-8