
Abstract
As a time-efficient training system, high intensity interval training (HIIT) is well known for several beneficial effects. However, the literature on the stress-generating effects of HIIT shows a research deficit. A standardized comparable stressor and different kinds of stress-parameters are needed for quantifying the results. The present study examined the hormonal, autonomic, and psychological stress outcomes of HIIT compared to a standardized psychosocial stressor and tested the cross-stressor-adaptation (CSA) hypothesis which implies a stress-buffering effect at a good fitness level. In a sample of 32 healthy young males (24.31 ± 3.35 years of age) stress was induced with a multiple Wingate (WG), as a HIIT all-out performance test, involving four 30 sec all-out exercise bouts. In addition, the Trier Social Stress Test (TSST), which consists of a mock job interview and mental arithmetic performance, was used for stress induction. Cortisol, heart rate variability (HRV), and stress-related questionnaires were assessed before, during, and after stress induction. Both the Wingate as well as the TSST led to a highly significant change in time and stressor for cortisol and HRV. Furthermore, a significantly higher delta during Wingate was identified. In part, the TSST had a significantly higher impact on the psychological measurements than the WG. In contrast to the literature, this study was not able to confirm the stress-buffering effect of the CSA hypothesis. These findings prove the stressful effect of HIIT. The prevention of negative health effects needs to be taken into consideration in sports training methods and programs as well as in stress-related research
By using a well-estimated psychosocial stressor for comparison and several stress parameters, this study is able to show the strong stress-generating effect of high intensity interval training (HIIT). Interestingly, subjective stress perception differed from objective stress response. This research is an important step towards understanding stress-related disorders in elite sport and making recommendations for reducing autonomic as well as hormonal stress in high intensity sport.
Lay summary
Introduction
As a time-efficient and effective physical training system, high intensity interval training (HIIT) is employed more and more in high performance sports as well as in popular sports (Gillen & Gibala, Citation2014; Wahl, Hägele, Zinner, Bloch, & Mester, Citation2010a, Citation2010b). Athletes switch repeatedly between sessions of very intense and relatively brief intermittent exercise which is often performed at maximum effort. Nevertheless, there are also critical effects of this training stimulus: HIIT is capable of increasing stress parameters, such as the glucocorticoid hormone cortisol, which is secreted by the hypothalamic-pituitary-adrenal (HPA) axis as a result of physical or psychosocial stress (Hill et al., Citation2008; McGuigan, Egan, & Foster, Citation2004; Wahl et al., Citation2013).
Wahl et al. (Citation2013) compared three different intensities of varying duration. The most intense protocol with the shortest duration, a HIIT stimulus, resulted in the highest and most significant increase in cortisol compared to the baseline. Thereby the researchers used a multiple Wingate (WG) for the most intensive protocol. A WG is an anaerobic and supramaximal physical test which requires pedaling for 30 seconds at maximal subjective power on an ergometer (Bar-Or, Citation1987). As a limiting factor, the influence of repeated vein punctures was not controlled for by this HIIT-protocol by Wahl et al. (Citation2013).
Next to Wahl et al. (Citation2013), Hill et al. (Citation2008) obtained only one blood cortisol sample directly after participant’s physical ergometer task, thus they did not evaluate the cortisol course. Furthermore, neither Hill et al. (Citation2008) nor Wahl et al. (Citation2013) used a comparative stressor to quantify the extent of stress nor did they use other stress parameters (objective or subjective) than cortisol to verify the measured stress-generating effect.
Besides cortisol, the heart rate variability (HRV) is another suitable, objective stress indicator. Affected by the parasympathetic and sympathetic cardiac nerves, its measurements can be used to assess the fluctuation of individual heart beats and as a marker for cardiac stress. While a high variability stands for a healthy autonomic system able to react adequately to environmental influences, a low HRV reflects an autonomic inflexibility (Petrowski et al., Citation2017).
Based on Selye (Citation1981) and his concept of stress, the cross-stressor-adaptation-(CSA) hypothesis was set up. It implies that physical activity might be seen as a stressor leading to appropriate adaptation processes. Accordingly, the stress reactivity of athletic individuals should also be less pronounced in nonphysical stressors (Kobasa, Maddi, & Puccetti, Citation1982; Sothmann et al., Citation1996). However, respective results proved to be inconsistent (Crews & Landers, Citation1987; Forcier et al., Citation2006; Jackson & Dishman, Citation2006). Meanwhile, Jackson and Dishman (Citation2006) showed empirical evidence for better physiological recovery after psychological stress despite a slightly increased stress response in comparison to unfit individuals. According to the authors, the range of the laboratory stressors and methods employed, the differences in the physiological response, the different types of individuals, and the dependent variables were responsible for the inconsistent results of their meta-regression analysis.
Both an intense physical (Wahl et al., Citation2013) and a psychosocial stressor (Kudielka, Hellhammer, & Kirschbaum, Citation2007) independently lead to an increase in stress-related parameters. Therefore, the aim of this study was to find out whether HIIT is to be understood as a stressor and whether the existing inconsistent results regarding the CSA hypothesis might be improved by using gold standard measuring tools – without the listed limitations of previous studies. It was hypothesized that both conditions would result in a comparable increase in the cortisol level and a decrease in the HRV, whereby fit individuals would show a lower stress response, in general.
Methods
Sample
The sample of male participants (N = 32; M = 24.31 years of age, SD = 3.35) was recruited through online announcements on the homepage of the German Sport University Cologne (DSHS). Only men were recruited to avoid cortisol differences based on the menstrual cycle phase (Kirschbaum, Wüst, & Hellhammer, Citation1992). Two members of this sample attested to smoking five cigarettes/day.
Based on Rimmele et al. (Citation2007, Citation2009) and Klaperski et al. (Citation2013), those participants who exercised less than 2 hours/week were classified as inactive (n = 8), those exercising 2–6 hours/week as moderately active (n = 10), and those exercising more than 6 hours/week as vigorously active (n = 14). Aside of this kind of classification, based on the information given by the participants, the group was also divided by median split in regard to their relative VO2max-values in order to obtain an objective activity classification system.
A power analysis showed that expecting a medium effect size of Cohen’s f = 0.20 and using an ANOVA for repeated measures as statistical test for proving in-between interactions with two tests, n = 10 repetitions, a significance level of p = .05, and a power of 95% (1-β = 0.95) showed that a total sample size of n = 32 subjects was needed. Detailed subject characteristics are shown in .
Table 1. Characteristics of individuals (N = 32).
Study protocol
All participants read and signed a written informed consent form in order to participate in the present study, which had been approved by the local Ethical Committee (ethnical commitment number: 129/2015). The present study was conducted in accordance with the Declaration of Helsinki. A short medical history check via telephone was used to identify exclusion criteria by asking for psychological disorders, (chronic) cardiac or orthopedic problems, recent vaccinations, stress research experience, or other mental or physical illnesses affecting the HPA axis. All the participants were awarded an expense allowance of 100 euros as compensation for participation and were asked to fill out several questionnaires in the context of preliminary investigations to assess further psychological and physical impairments as possible exclusion criteria.
All participants performed an ergometer test on the upright bike with additional spirometry to determine the individual VO2max as well as the maximum performance (watt). The step-test starts at 30 W and increases automatically by 40 W every three minutes until volitional exhaustion was reached (Hollman-Venrath protocol). Hereby, the participants cycled between 60 and 80 revolutions per minute (rpm).
After successful preliminary medical investigation, the participants were separated into two randomized groups to perform a cross-over design. While the first group started with the physical stressor (Wahl et al., Citation2013), the second group began with the psychological stressor. The TSST as well as the HIIT (Kirschbaum, Pirke, & Hellhammer, Citation1993; Wahl et al., Citation2013) are evidence-based and suitable methods for examining the stress reactivity and are replicable under laboratory conditions.
On arrival, the participants were outfitted with a pulse watch to ensure a wireless heartrate (HR) and heartrate-variability (HRV) transfer. For all participants, an intravenous catheter was used (at −60 min; meaning 60 min before stress induction) to obtain blood samples before and after the stressor: two samples before (−15 min; −1 min) and eight samples after each stressor (+1 min; +5 min; +10 min; +20 min; +30 min; +45 min; +60 min; +75 min; and ) during which eight mL of venous blood were collected using a Monovette-system. Furthermore, the HR and the HRV were measured at selected moments: two before, two during, and two after stress induction. To assure an identical baseline, standardized breathing at rest prior to stress induction was performed with each participant (3 sec/breath).
Figure 1. Wingate timesheet. The timeline information is related to the use of stress. Solid line = subject on ergometer; dashed line: subject in supine or seated position; arrow down: permanent venous catheter; marked columns: physical stress.
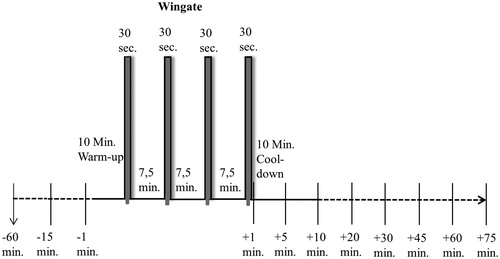
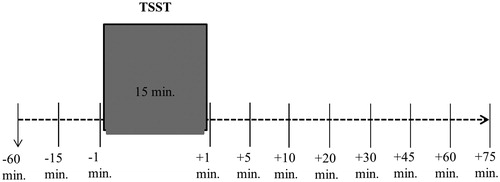
Figure 2. Trier Social Stress Test timesheet. Timeline information is related to the use of stress. Solid line: subject in stress task; dashed line: subject in supine or seated position; arrow down: permanent venous catheter; marked column: psychosocial stress.
In addition to the blood samples and the HR/HRV, several questionnaires were used during each setting to evaluate the two stressors via subjective, stress-related parameters. The state version of the State-Trait-Anxiety Inventory (STAI; Laux, Glanzmann, Schaffner, & Spielberger, Citation1981) was handed out right before and right after the stressors to measure anxiety dependent differences over time.
During stress the Primary Appraisal Secondary Appraisal (PASA) was used to assess cognitive appraisal processes regarding the current stressful situation. Post-stress: the Visual Analog Scale (VAS) as a straight line from 0 to 100 assessing the extent of the subjective perception of the stressfulness of the stressor was used (Petrowski, Wintermann, Schaarschmidt, Bornstein, & Kirschbaum, Citation2013).
Due to the susceptibility of cortisol to the circadian rhythm (Hellhammer, Kudielka, Schommer, & Hellhammer, Citation2004), the measurements were standardized between 1 pm and 5 pm. Furthermore, glucose intake is a potential way of influencing the cortisol level (Gonzalez-Bono, Rohleder, Hellhammer, Salvador, & Kirschbaum, Citation2002; Hellhammer et al., Citation2004). Respectively, caloric intake had to cease two hours prior to each examination. This way, both possible influences, time of day and caloric intake, could be reduced to a minimum. The room-temperature, as well as the humidity, were kept constant.
Interventions
Physical stressor – modified Wingate-test
Following a 10 min warm-up session of 70 rpm, the participants were asked to perform four 30 sec-tasks using their individual maximum strength at 120 rpm followed by a 7.5 min recovery phase at 70 rpm (). Thus, the multiple WG is a typical high intensity interval training. The bicycle ergometer was employed in the isokinetic mode, which enhances the actual load as soon as the participant tries to ride faster than 120 rpm, to reach the maximum physical exhaustion of all subjects. At all times, the participants were to remain in the seated position. In contrast to Wahl et al. (Citation2013), strong verbal motivation was not given to reduce possible sources of irritation, respectively additional stress, of a psychological origin.
Psychosocial stress – Trier Social Stress test
The TSST is the gold standard and most employed procedure for inducing high levels of psychosocial stress in laboratory settings (Kudielka et al., Citation2007). It was performed following the directions by Kirschbaum et al. (Citation1993). This protocol is capable of increasing the salivary cortisol response approx. two- to threefold in 70–80% of all tested individuals, reaching the peak level approx. 10-20 minutes after the end of the stress task (Kudielka et al., Citation2007). This stressor is a social-evaluative situation, which includes a 3-min preparation period, a 5-min mock job interview, and a subsequent 5-min arithmetic task in front of a two-person panel. The interview is sound- and video-recorded (Kirschbaum et al., Citation1993). All the subjects were told to convince the two-person panel that they were the perfect person for the job. Hereby, the panel-team was introduced as being trained in nonverbal behavior.
Instruments
Questionnaires
The preliminary evaluation of the participants included the following questionnaires:
(1) The Symptom-Check-List-90-R consists of 90 items with a five-point rating scale from 0-‘Not at all’ to 4-‘Extremly’ (SCL-90-R; Derogatis, Citation1977). Cronbach’s alpha = 0.920. (2) Beck Depression Inventory consisting of 21 symptoms rated for intensity from 0 to 3 with question-dependent answers (BDI; Beck and Beamesderfer, Citation1974). Cronbach’s alpha = 0.613. (3) Perceived Stress Scale consisting of 14 items rated on a 5-point Likert scale from 0-‘Never’ to 4-‘Very often’ (PSS; Cohen et al., Citation1983). Cronbach’s alpha = 0.368. (4) State-Trait Anxiety Inventory Form X2 consisting of 20 items with a 4-point rating scale from 0-‘Almost never’ to 3-‘Almost always’ (STAI-X2; Laux et al., Citation1981). Cronbach’s alpha = 0.617. (5) And the Freiburg Questionnaire on Physical Activity – short version, which consists of 12 questions that include different kinds of daily activities (FFKA; Frey et al., Citation1999). Cronbach’s alpha = 0.178.
The stress interventions included the following questionnaires:
(6) The state version of the STAI, which consists of 20-items, e.g. ‘I feel calm’ or ‘I feel strained’, for measuring the extent of anxiety induced by the acute stress protocol on a four-point Likert scale from 1-‘Not at all’ to 4-‘Very much so’. It was analyzed by calculating the total sum score. Low scores indicate mild anxiety, whereas high scores indicate a strong form of anxiety. Cronbach’s alpha = 0.673. (7) The PASA with 16 situation-specific items on a six-point Likert scale from ‘Strongly disagree’ to ‘Strongly agree’ gets formed by four primary (Threat, Challenge, Self-Concept and Control Expectancy) and two secondary scales: Primary Appraisal = (Challenge + Threat/2); Secondary Appraisal = (Self-Concept + Control Expectancy/2). A general stress index gets represented by the sum of primary and secondary appraisal. Example items are ‘I do not feel threatened by the situations’ or ‘This situation is not a challenge for me’ (Gaab, Rohleder, Nater, & Ehlert, Citation2005; Hammerfald et al., Citation2006) Cronbach’s alpha = 0.785. (8) The VAS consists of 8 items, each on a straight 100 mm scale. The subjects marked the line from 0 ‘Not at all’ to 100 ‘Very much’. Scores were determined by calculating from the left end to the mark with a ruler. An example item is ‘I found the situation challenging’ (Petrowski et al., Citation2013). Cronbach’s alpha = 0.449.
All these instruments were administered in German.
Blood analytics
After resting for 10 min at room temperature for the deactivation of coagulation factors, the blood samples were centrifuged for 10 min at 3400 rpm and 20 °C. Serum cortisol concentrations were determined using the Elecsys Cortisol II electrochemiluminescence immunoassay (ECLIA) on a Roche Cobas e602 analyzer. The lower and upper limits of the measurements were 0.054–63.4 µg/dL. Concentrations above the measuring range >63.4 µg/dL were measured in 10-fold dilution. Intra-assay co-efficient of variation (CV), 5.4% at 3.62 µg/dL, 2.4% at 37.6 µg/dL, 1.5% at 319 µg/dL and 1.7% at 551 µg/dL.
HRV-analytics
The HR and HRV variables were determined and analyzed by means of the HRV-watch system. The values were measured over 3 min during the first and 5 min during the following five intervals (standardized breathing - sb; rest; Wingate: warm-up/TSST: interview; Wingate: second break/TSST: arithmetic; Wingate: cool-down/TSST: recovery - rec; at rest 2). The watch recorded by a receptor belt with a sampling rate of 1.000 Hz gave a temporal solution of 1 ms per RR phase.
The HRV software corrected the artifacts using an error filter. To detect the heart rate variability, the following parameters were used: the root mean square of successive differences (RMSSD), high frequency power (HF; 0.15–0.40 Hz), low frequency power (LF; 0.04–0.15 Hz), and the LF/HF ratio.
Statistical procedure
Missing data (2.1%) were replaced by using multiple imputations (Spieß, Citation2010), and outliers were identified as values under and above 1.5 times the interquartile range (Walfish, Citation2006). To measure the global effect during the two stressors, the data were tested for normal distribution, and the baseline values of both stressors were tested by t-test.
As the HRV values were distorted, all indices were log10 transformed (Agelink et al., Citation2001). After the transformation, all the HRV values showed a normal distribution. Subsequently, an analysis of variance (ANOVA) for repeated measures with post-hoc testing (Bonferroni) was performed to analyze the time and test- dependent trend (for cortisol and HRV). An ANCOVA was performed to analyze the smoking status as a covariate.
To analyze the delta, the mean of all differences between peak and baseline was calculated. Negative delta was analyzed by the difference between the peak and the last value (+75 min). For this, a one-way ANOVA (in the three-activity-group classification) and a t-test (in the two-activity-group classification) were used. Statistical differences were considered to be significant for p < .05. Data analyses were carried out using SPSS v. 24 (SPSS Inc., Chicago, IL, USA).
Results
Cortisol
There were no significant differences in the baseline values (−1 min) between the two stressors (t(31) = −1.70, p = .100). Smoking as a covariate had no significant impact (F(1, 30) = 0.12, p = .891).
Both the TSST as well as the WG led to a highly significant increase over time (F(1.72, 53.18) = 61.66, p < .001, ηp2 = 0.67) and test (F(1, 31) = 14.27, p = .001, ηp2 = 0.32). Furthermore, a highly significant interaction effect of time and stressor was found (F(1.89, 58.49) = 17.11, p < .001, ηp2 = 0.36). Post-hoc analysis revealed a highly significant increase in both stress sittings (p < .001). The smoking status as a covariate did not affect the values (all p > .05) ()
Figure 3. Serum cortisol response (nmol/l) to physical (Wingate) and psychosocial stress (TSST) in 32 healthy subjects. Shown are the mean values with standard errors. Time information is related to the use of stress. Marked column: stress induction; white circles: Wingate; black squares: TSST.
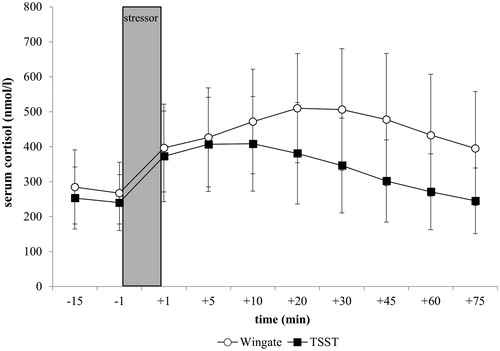
A significant difference in the delta between the WG (M = 9.97, SD = 5.13) and the TSST (M = 6.58, SD = 3.80) was identified (t(31) = −3.37, p < .01, Cohen’s d = 0.75).
Heart rate variability
No significant differences in the baseline values (rest1) (t(31) = −0.01, p = .987) between the two stressors could be detected.
Furthermore, both the TSST as well as the WG led to a highly significant decrease over time (F(1.64, 50.80) = 37.14, p < .001, ηp2 = 0.55) and test (F(1, 30) = 22.62, p < .001, ηp2 = 0.43). Additionally, a highly significant interaction effect of time and test was identified (F(3.22, 99.95) = 24.33, p < .01, ηp2 = 0.44). Post-hoc measurements revealed a highly significant decrease of heart rate variability induced through TSST and WG (p < .001).
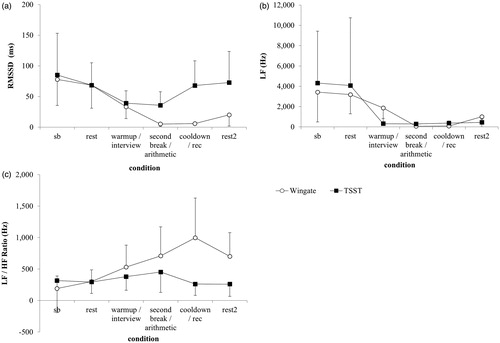
Progress of the root mean square of successive differences (RMSSD-TSST: (F(1.75, 54.29) = 15.59, p < .001, ηp2 = 0.34); RMSSD-WG: (F(1.74, 54.06) = 57.94, p < .001, ηp2 = 0.65)) and low frequency (LF-TSST: (F(2.16, 67.06) = 4.05, p = .019, ηp2 = 0.12); LF-WG: (F(2.47, 76.43) = 26.94, p < .001, ηp2 = 0.47)) showed a significant decrease in the WG as well as the TSST. For the low frequency/high frequency ratio (LF/HF ratio), a significant increase was detected in both conditions (LF/HF-TSST: (F(2.04, 63.18) = 3.17, p = .048, ηp2 = 0.09); LF/HF-WG: (F(2.94, 91.26) = 21.05, p < .001, ηp2 = 0.40)). The RMSSD, LF and the LF/HF ratio progress are shown in .
Figure 4. HRV response to physical (Wingate) and psychosocial stress (TSST) in 32 healthy subjects. (a) Root mean square successive differences (RMSSD), (b) Low frequency power (LF) and (c) Low frequency/high frequency ratio (LF/HF). Shown are the mean values with standard errors. sb : standardized breathing, rec : recovery. White circles: Wingate; black squares: TSST.
Detailed results concerning the different HRV parameters are displayed in .
Table 2. HRV statistics.
Subjective measurements
PASA: The threat dimension of the TSST (M = 3.05; SD = 0.99) was significantly higher than in the WG (M = 1.59; SD = 0.67; (t(31) = 7.32, p < .001, Cohen’s d = 1.73). In addition, the primary appraisal of the TSST was significantly higher (M = 3.57, SD = 0.72 vs. M = 2.78, SD = 0.53; (t(28) = 5.03, p < .01, Cohen’s d = 1.25). However, the other dimensions: Challenge, Self-Concept, Control Expectancy and also the secondary appraisal in general showed no significant difference (p > .05). Considering the stress index of both conditions, significantly higher values were measured in the TSST (M = −0.34, SD = 1.07; WG: M = −1.25, SD = 0.58; (t(25) = −3.90, p = .001, Cohen’s d = 1.06).
VAS: No significant difference between the WG (M = 61.30, SD = 10.42) and the TSST (M = 58.68, SD = 10.78) was detected (t(31) = 1.02, p = .315) in the extent of perceived stressfulness of the stressor.
STAI: A highly significant increase from pre to post was measured in the TSST (pre: M = 33.13, SD = 6.66; post: M = 43.91, SD = 10.69; (t(31) = −4.86, p = .001, Cohen’s d = 1.21) as well as in the WG (pre: M = 34.13, SD = 6.29; post: M = 41.09, SD = 8.26; (t(31) = −4.35, p = .001, Cohen’s d = 0.94) by examining the intensity of anxiety as an emotional state. However, both pre- and both post extents did not differ significantly from each other (pre: (t(31) = −0.92, p = .364); post: (t(31) = 1.52, p = .138).
Cross-stressor adaptation hypothesis
Dividing the individuals by their FFKA-activity group, neither in the cortisol (F(3.25, 47.09) = 0.98, p = .417) nor in the HRV (F(3.38, 49,06) = 0.398, p = .778) course a significant difference was detected between the activity groups during psychosocial stress. Even after splitting the participants via median split regarding the rel. VO2max, neither in the cortisol (F(1.65, 49.61) = 9.29, p = .588) nor in the HRV (F(1.76, 52.74) = 1.74, p = .189) course did the two groups differ in any significant way.
For the cortisol regeneration, no significant difference was detected between the three different activity groups classified through FFKA (F(2, 29) = 0.63, p = .539) as well as in HRV regeneration (F(2, 29) = 0.78, p = .469). Splitting the subjects by the measured relative VO2max at their median also did not lead to any significant differences in the ability for regeneration: Cortisol (t(30) = 0.98, p = .337) and HRV (t(30) = −0.27, p = .071).
Discussion
Previous studies have identified high intensity exercise as a potential way to increase stress parameters like cortisol but were not able to quantify their results or support the stress- generating effect using different parameters (Hill et al., Citation2008; McGuigan et al., Citation2004; Wahl et al., Citation2013). In this study, we used different kinds of stress parameters and had the opportunity of quantifying them by using two stressors without the limitations of previous investigations.
Cortisol measurements
It seems as if repeated physical stress activates the HPA-axis more than the psychosocial stressor. Our results are in line with Hill et al. (Citation2008), McGuigan et al. (Citation2004), Wahl et al., (Citation2013) and Wahl et al. (Citation2010) showing that next to psychosocial stress, HIIT should be seen as an effective stressor. While Wahl and colleagues (2013) used the same physical stressor, their baseline values were approximately twice as high as in the present study. This may be the result of repeated vein punctures due to the various blood samples taken (Smyth, Hucklebridge, Thorn, Evans, & Clow, Citation2013) as well as the omitted resting phase before the exercise intervention.
The WG-related cortisol response showed a significantly higher but delayed cortisol delta in comparison to the TSST (). A reason for this significance might be seen in the intense physical exhaustion and the associated energy deficit and metabolic response. Another possible reason for the different time-dependent peaks of both tasks (TSST at +10; WG at +20) might be seen in the fact that the intense part of the Wingate lasts approximately 10 minutes longer than the psychosocial stressor and that the number of intense intervals may affect the cortisol response (Dickerson & Kemeny, Citation2004). The differences in shorter-lasting stressors, however, contradict this hypothesis. The use of other stress inductions such as the dexamethasone-corticotrophin-releasing-hormone (DEX-CRH) test with an injection of the human corticotrophin-releasing hormone (CRH) led to a maximum cortisol value 60 minutes after injection (Kirschbaum et al., Citation1992; Petrowski, Wintermann, Kirschbaum, & Bornstein, Citation2012). A cold pressor test (CPT – brief injection), as well as a socially evaluated cold pressor test (SECPT – maximum length of 3 min), have their maximum earlier at 25 min after induction (Schwabe, Haddad, & Schachinger, Citation2008). Both facts challenge this hypothesis. Therefore, the afore-mentioned hypothesis of a comparable hormone increase could not be confirmed. The WG led to a delayed and higher peak with a persistent effect.
HRV measurements
The present results indicate that both stressors are capable of decreasing the HRV in a significant way. This is in line with the existing literature for the separate stressors (Petrowski et al., Citation2017; Sarmiento et al., Citation2013). Until now, a comparison of the two stressors has not been published.
By looking at the course of the TSST and WG, it is interesting that, even here, the WG seems to be more decisive in generating stress. In line with the delayed hormonal peak during the WG-course, the LF/HF-ratio also shows a more delayed peak in Wingate (cool-down-phase) than in TSST (arithmetic-phase). This indicates that the physical stressor has a stronger and more long-lasting effect on the autonomic system and the sympathovagal balance. A possible reason might be the way someone breathes during exercise which influences the heart rate variability (Murata, Citation1992). Next to the muscular and metabolic workload, the strong respiration during high intensity exercise may influence the HRV more than in TSST. Further research should include respiration measurements to highlight this aspect.
The hypothesized result concerning the HRV cannot be confirmed. Even though both conditions lead to a decrease in the HRV-, the impact of the physical stressor appears more dominant. This goes along with the amount of cortisol secretion measured. Our results show the strong stress-generating and long-lasting effect of the HIIT. The authors highly recommend the integration of this knowledge into (elite) sports and sports training systems, especially regarding regeneration phases after intense training sessions.
Subjective measurements
Looking at the subjective stress measurements, both interventions led to a comparable significant rise in the intensity of anxiety measured by the STAI, but the TSST showed significantly higher extent in the threat dimension, the primary appraisal as well as in the stress index of the PASA. It seems that the physical stress was evaluated much less harmful than the psychosocial stress – even though the objective parameters show a higher stress-generating effect by the HIIT. This discrepancy between perceived stress and increased stress parameters might result in a misjudgment of the effects of HIIT. Athletes may not pay attention to the burden of high intensity exercise and therefore also not to the need for regeneration.
Cross-stressor adaptation hypothesis
By testing the CSA-hypothesis, no significant cortisol or HRV differences between the three activity groups by FFKA (Klaperski et al., Citation2013; Rimmele et al., Citation2007, Citation2009) could be detected. The classification used in the literature is based on the answers given by the various participants. To avoid a discrepancy between the subjective value of the FFKA and the objective fitness level, the CSA-hypothesis was also tested with the individual relative VO2max measured by spirometry. Nonetheless, no significant difference was detected.
A potential reason for not reaching significance could be seen in the mean relative VO2max values of the two groups (untrained = 45.17 mL min−1 kg−1 vs. trained = 58.53 mL min−1 kg−1). According to Nunes et al., (Citation2005), both groups have good, respectively excellent performance levels. In addition, the homogeneity in the relative VO2max of the current sample led to small quartile clusters which do not allow for a statistical calculation. Regardless of the method, to differentiate between the subjects (using the relative VO2max or FFKA), a larger number of individuals and greater differences in their fitness status seem to be of relevance. Even when the negative delta was calculated to examine the ability for regeneration, no statistically significant difference could be found for the cortisol or the HRV-values. These results oppose the findings by Jackson and Dishman (Citation2006) for a better recovery of fit individuals after psychosocial stress.
Future studies should consider the critique for a heterogeneous way of CSA-hypothesis investigations (Jackson & Dishman, Citation2006). The authors advocate their chosen method of employing spirometry for determining the performance (Rimmele et al., Citation2007, Citation2009) and the TSST as well-estimated stressor. By way of the highly standardized investigation and the chosen methods, the hypothesized distinction cannot be confirmed.
Besides the beneficial effects of HIIT (Wahl et al. Citation2010a), this stimulus also highly increases the HPA axis activity and the amount of cortisol, which might catalyst the development of mental disorders such as depression (de Carvalho Tofoli, Von Werne Baes, Martins, & Juruena, Citation2011; Pariante & Lightman, Citation2008). Current research indicates that depression affects 6.7% of today’s general adult population (Wolanin, Gross, & Hong, Citation2015), whereby its prevalence in elite sport with 15.6% up to 21% is more than twice as high (Proctor & Boan-Lenzo, Citation2010; Yang et al., Citation2007). A possible reason for this difference may be seen in the chronically activated HPA axis through the repeated intensive training bouts such as HIIT (de Carvalho Tofoli et al., Citation2011). Additionally, overtraining which can be seen as the imbalance of physical exhaustion and recovery or rather stress and stress tolerance, seems to be a potential factor for the genesis of psychological disorders (Baumert et al., Citation2006; Ljungqvist et al., Citation2009). To prevent overtraining, chronic stress, or psychological disorders in (elite) sport, these results should be taken into consideration regarding training concepts. Thus, the implementation of sufficient regeneration phases is highly recommended.
Limitations
Besides the obvious highlights, there are limitations calling for future studies: the protocol of the Wingate should be modified regarding its use of the PASA. In the present study, the questionnaire was filled out between the second and the third load. With this timeline, the participants had already found out the specification of the physical stressor compared to the TSST timeline where the subjects fill out the PASA before the mock job interview starts. This might lead to a false low result during the physical stressor. Therefore, the results of the threat dimension needs to be relativized as well as for the stress index.
In this study, four WGs were used which led to a different timeline compared to the TSST. The effects of a WG-protocol with the same exposure time as the TSST needs to be investigated. Furthermore, in contrast to Wahl et al. (Citation2013), the authors refrained from verbal encouragement in this study to minimize the possible impact of strong verbal motivation. Moreover, the authors hypothesized that the specific requirements of the HIIT-load itself might cause psychological stress but that this interaction may be impossible to separate.
Informed consent
Informed consent was obtained from the individual participants included in the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Acknowledgments
The authors would like to thank all the participants of the study. A special thanks goes to Elisabeth Orrison for proofreading this paper.
Disclosure statement
No potential conflict of interest was reported by the authors.
Related Research Data
References
- Agelink, M.W., Malessa, R., Baumann, B., Majewski, T., Akila, F., Zeit, T., & Ziegler, D. (2001). Standardized tests of heart rate variability: Normal ranges obtained from 309 healthy humans, and effects of age, gender, and heart rate. Clinical Autonomic Research: Official Journal of the Clinical Autonomic Research Society, 11, 99–108. doi:10.1007/BF02322053
- Bar-Or, O. (1987). The Wingate Anaerobic Test. Sports Medicine, 4, 381–394. doi:10.2165/00007256-198704060-00001
- Baumert, M., Brechtel, L., Lock, J., Hermsdorf, M., Wolff, R., Baier, V., & Voss, A. (2006). Heart rate variability, blood pressure variability, and baroreflex sensitivity in overtrained athletes. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine, 16, 412–417. doi:10.1097/01.jsm.0000244610.34594.07
- Beck, A., & Beamesderfer, A. (1974). Assessment of Depression: The Depression Inventory. In P. Pichot & R. Oliver-Martin (Eds.), Psychological Measurements in Psychopharmacology (pp. 151–169). Basel: Karger Publishers.
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A Global measure of perceived stress. Journal of Health and Social Behavior, 24, 385. doi:10.2307/2136404
- Crews, D., & Landers, D. (1987). A meta-analytic review of aerobic fitness and reactivity to psychosocial stressors. Medicine & Science in Sports & Exercise, 19, 114–120. doi:10.1249/00005768-198710001-00004
- de Carvalho Tofoli, S.M., Von Werne Baes, C., Martins, C.M.S., & Juruena, M. (2011). Early life stress, HPA axis, and depression. Psychology & Neuroscience, 4, 229–234. doi:10.3922/j.psns.2011.2.008
- Derogatis, L. (1977). Administration, scoring, and procedures manual for the SCL-90-R. Baltimore: Clinical Psychometrics Research.
- Dickerson, S.S., & Kemeny, M.E. (2004). Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Psychological Bulletin, 130, 355–391. doi:10.1037/0033-2909.130.3.355
- Forcier, K., Stroud, L.R., Papandonatos, G.D., Hitsman, B., Reiches, M., Krishnamoorthy, J., & Niaura, R. (2006). Links between physical fitness and cardiovascular reactivity and recovery to psychological stressors: a meta-analysis. Health Psychology, 25, 723–739. doi:10.1037/0278-6133.25.6.723
- Frey, I., Berg, A., Grathwohl, D., & Keul, J. (1999). Freiburger fragebogen zur körperlichen aktivität- entwicklung, prüfung und anwendung. Sozial- Und Präventivmedizin SPM, 44, 55–64. doi:10.1007/BF01667127
- Gaab, J., Rohleder, N., Nater, U.M., & Ehlert, U. (2005). Psychological determinants of the cortisol stress response: The role of anticipatory cognitive appraisal. Psychoneuroendocrinology, 30, 599–610. doi:10.1016/j.psyneuen.2005.02.001
- Gillen, J.B., & Gibala, M.J. (2014). Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Applied Physiology, Nutrition, and Metabolism, 39, 409–412. doi:10.1139/apnm-2013-0187
- Gonzalez-Bono, E., Rohleder, N., Hellhammer, D.H., Salvador, A., & Kirschbaum, C. (2002). Glucose but not protein or fat load amplifies the cortisol response to psychosocial stress. Hormones and Behaviour, 41, 328–333. doi:10.1006/hbeh.2002.1766
- Hammerfald, K., Eberle, C., Grau, M., Kinsperger, A., Zimmermann, A., Ehlert, U., & Gaab, J. (2006). Persistent effects of cognitive-behavioral stress management on cortisol responses to acute stress in healthy subjects—A randomized controlled trial. Psychoneuroendocrinology, 31, 333–339. doi:10.1016/j.psyneuen.2005.08.007
- Hellhammer, D., Kudielka, B.M., Schommer, N.C., & Hellhammer, D.H. (2004). Acute HPA axis responses, heart rate, and mood changes to psychosocial stress (TSST) in humans at different times of day Acute HPA axis responses, heart rate, and mood changes to psychosocial stress (TSST) in humans at different times of day. Psychoneuroendocrinology, 29, 983–992. doi:10.1016/j.psyneuen.2003.08.009
- Hill, E.E., Zack, E., Battaglini, C., Viru, M., Viru, A., & Hackney, A.C. (2008). Exercise and circulating Cortisol levels: The intensity threshold effect. Journal of Endocrinological Investigation, 31, 587–591. doi:10.1007/BF03345606
- Jackson, E.M., & Dishman, R.K. (2006). Cardiorespiratory fitness and laboratory stress: A meta-regression analysis. Psychophysiology, 43, 57–72. doi:10.1111/j.1469-8986.2006.00373.x
- Kirschbaum, C., Pirke, K.M., & Hellhammer, D.H. (1993). The ’Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28, 76–81. doi:10.1159/000119004
- Kirschbaum, C., Wüst, S., Faig, H.G., & Hellhammer, D.H. (1992). Heritability of cortisol responses to human corticotropin-releasing hormone, ergometry, and psychological stress in humans. The Journal Of Clinical Endocrinology& Metabolism, 75, 1526–1530. doi:10.1210/jcem.75.6.1464659
- Kirschbaum, C., Wüst, S., & Hellhammer, D. (1992). Consistent sex differences in cortisol responses to psychological stress. Psychosomatic Medicine, 54, 648–657. doi:10.1097/00006842-199211000-00004
- Klaperski, S., von Dawans, B., Heinrichs, M., & Fuchs, R. (2013). Does the level of physical exercise affect physiological and psychological responses to psychosocial stress in women? Psychology of Sport and Exercise, 14, 266–274. doi:10.1016/j.psychsport.2012.11.003
- Kobasa, S.C., Maddi, S.R., & Puccetti, M.C. (1982). Personality and exercise as buffers in the stress-illness relationship. Journal of Behavioral Medicine, 5, 391–404. doi:10.1007/BF00845369
- Kudielka, B.M., Hellhammer, D.H., & Kirschbaum, C. (2007). Ten years of research with the Trier Social Stress Test - revisited. In Social neuroscience: Integrating biological and psychological explanations of social behavior (pp. 56–83). New York.
- Laux, L., Glanzmann, P., Schaffner, P., & Spielberger, C. (1981). The State-Trait Anxiety Inventory. Göttingen, Bern Hogrefe, 5. Retrieved from https://scholar.google.de/scholar?hl=de&q=Laux%2C+L.%2C+Glanzmann%2C+P.%2C+Schaffner%2C+P.%2C+%26+Spielberger%2C+D.+%281970%29.+Das+State-Trait-Angstinventar+%28STAI%29.+Göttingen%3A+Beltz.&btnG=&lr=
- Ljungqvist, A., Jenoure, P., Engebretsen, L., Alonso, J.M., Bahr, R., Clough, A., … Thill, C. (2009). The International Olympic Committee (IOC) Consensus Statement on periodic health evaluation of elite athletes March 2009. British Journal of Sports Medicine, 43, 631–643. doi:10.1136/bjsm.2009.064394
- McGuigan, M., Egan, A., & Foster, C. (2004). Salivary Cortisol Responses and Perceived Exertion during High Intensity and Low Intensity Bouts of Resistance Exercise. Journal of Sports Science and Medicine, 3, 8–15.
- Murata, A. (1992). Effects of respiration on heart-rate variability measures. Electronics and Communications in Japan (Part III: Fundamental Electronic Science), 75, 107–116. doi:10.1002/ecjc.4430750210
- Nunes, R., Pontes, G.F., Dantas, P.M., & Fernandes, F., J. (2005). Referencial table of cardiopulmonary fitness. Fitness & Performance Journal, 4, 27–33. https://doi.org/10.3900/fpj.4.1.27.e
- Pariante, C.M., & Lightman, S.L. (2008). The HPA axis in major depression: classical theories and new developments. Trends in Neurosciences, 31, 464–468. doi:10.1016/j.tins.2008.06.006
- Petrowski, K., Wichmann, S., Siepmann, T., Wintermann, G.-B., Bornstein, S.R., & Siepmann, M. (2017). Effects of mental stress induction on heart rate variability in patients with panic disorder. Applied Psychophysiology and Biofeedback, 42, 85–94. doi:10.1007/s10484-016-9346-9
- Petrowski, K., Wintermann, G.-B., Kirschbaum, C., & Bornstein, S.R. (2012). Dissociation between ACTH and cortisol response in DEX–CRH test in patients with panic disorder. Psychoneuroendocrinology, 37, 1199–1208. doi:10.1016/j.psyneuen.2011.12.013
- Petrowski, K., Wintermann, G.B., Schaarschmidt, M., Bornstein, S.R., & Kirschbaum, C. (2013). Blunted salivary and plasma cortisol response in patients with panic disorder under psychosocial stress. International Journal of Psychophysiology, 88, 35–39. doi:10.1016/j.ijpsycho.2013.01.002
- Proctor, S.L., & Boan-Lenzo, C. (2010). Prevalence of depressive symptoms in male intercollegiate student-athletes and nonathletes. Journal of Clinical Sport Psychology, 4, 204–220. doi:10.1123/jcsp.4.3.204
- Rimmele, U., Seiler, R., Marti, B., Wirtz, P.H., Ehlert, U., & Heinrichs, M. (2009). The level of physical activity affects adrenal and cardiovascular reactivity to psychosocial stress. Psychoneuroendocrinology, 34, 190–198. doi:10.1016/j.psyneuen.2008.08.023
- Rimmele, U., Zellweger, B.C., Marti, B., Seiler, R., Mohiyeddini, C., Ehlert, U., & Heinrichs, M. (2007). Trained men show lower cortisol, heart rate and psychological responses to psychosocial stress compared with untrained men. Psychoneuroendocrinology, 32, 627–635. doi:10.1016/j.psyneuen.2007.04.005
- Sarmiento, S., García-Manso, J.M., Martín-González, J.M., Vaamonde, D., Calderón, J., & Da Silva-Grigoletto, M.E. (2013). Heart rate variability during high-intensity exercise. Journal of Systems Science and Complexity, 26, 104–116. doi:10.1007/s11424-013-2287-y
- Schwabe, L., Haddad, L., & Schachinger, H. (2008). HPA axis activation by a socially evaluated cold-pressor test. Psychoneuroendocrinology, 33, 890–895. doi:10.1016/j.psyneuen.2008.03.001
- Selye, H. (1981). Geschichte und Grundzüge des Stresskonzepts. In J. Nitsch (Ed.), Stress: Theorien; Untersuchungen; Massnahmen (pp. 163–187). Bern: Huber.
- Smyth, N., Hucklebridge, F., Thorn, L., Evans, P., & Clow, A. (2013). Salivary cortisol as a biomarker in social science research. Psychoneuroendocrinology, 7, 605–625. doi:10.1111/spc3.12057
- Sothmann, M.S., Buckworth, J., Claytor, R.P., Cox, R.H., White-Welkley, J.E., & Dishman, R.K. (1996). Exercise training and the cross-stressor adaptation hypothesis. Exercise and Sport Sciences Reviews, 24, 267–287.
- Spieß, M., (2010). Der, U. M., Fehlenden Werten. In C., Wolf, H. & Best, (Eds.), Handbuch der sozialwissenschaftlichen Datenanalyse (pp. 117–142). VS Verlag für Sozialwissenschaften. doi:10.1007/978-3-531-92038-2_6
- Wahl, P., Hägele, M., Zinner, C., Bloch, W., & Mester, J. (2010a). High Intensity Training (HIT) für die verbesserung der ausdauerleistungsfähigkeit im leistungssport. Schweizerische Zeitschrift Fur Sportmedizin Und Sporttraumatologie, 58, 125–133. doi:10.1007/s10354-010-0857-3
- Wahl, P., Hägele, M., Zinner, C., Bloch, W., & Mester, J. (2010b). High Intensity Training (HIT) für die Verbesserung der Ausdauerleistungsfähigkeit von Normalpersonen und im Präventions- und Rehabilitationsbereich. Wiener Medizinische Wochenschrift, 160, 627–636. doi:10.1007/s10354-010-0857-3
- Wahl, P., Mathes, S., Köhler, K., Achtzehn, S., Bloch, W., & Mester, J. (2013). Acute metabolic, hormonal, and psychological responses to different endurance training protocols. Hormone and Metabolic Research, 45, 827–833. doi:10.1055/s-0033-1347242
- Wahl, P., Zinner, C., Achtzehn, S., Bloch, W., & Mester, J. (2010). Effect of high- and low-intensity exercise and metabolic acidosis on levels of GH, IGF-I, IGFBP-3 and cortisol. Growth Hormone and IGF Research, 20, 380–385. doi:10.1016/j.ghir.2010.08.001
- Walfish, S. (2006). A Review of Statistical Outlier Methods. Pharmaceutical Technology, 30, 1–5.
- Wolanin, A., Gross, M., & Hong, E. (2015). Depression in athletes: Prevalence and risk factors. Current Sports Medicine Reports, 14(1), 56–60. doi:10.1249/JSR.0000000000000123
- Yang, J., Peek-Asa, C., Corlette, J.D., Cheng, G., Foster, D.T., & Albright, J. (2007). Prevalence of and Risk Factors Associated With Symptoms of Depression in Competitive Collegiate Student Athletes. Clinical Journal of Sport Medicine, 17, 481–487. doi:10.1097/JSM.0b013e31815aed6b